

Full Length Research Article
Carotid artery Disease Assessed by Color Doppler Flow Imaging: Comparison Between Diabetic and Non-Diabetic Patients
Hamna Areej*, Syed Muhammad Yousaf Farooq, Naveed Asad, Mehreen Fatima, Areeba Mahmood, Ume Kalsoom Attique, M. Usama Tahir, Haq Nawaz Khan
Adv. life sci., vol. 10, no. 1, pp. 66-71, March 2023
*- Corresponding Author: Hamna Areej (Email: hamnaareej6@gmail.com)
Authors' Affiliations
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Carotid artery disease is most often seen in hypertensive patients and in patients with diabetes mellitus. More than 50% stenosis of extra cranial internal carotid arteries is linked with about 8–15% of ischemic strokes. The incidence of carotid artery stenosis (CAS) among diabetic patients is rising as compared to non-diabetic patients.
Methods: A cross-sectional study was performed on 120 patients, out of whom 60 were diabetic and 60 non-diabetics with clinically suspected carotid artery disease. The study was conducted at the university ultrasound clinic in Green Town by Doppler ultrasonography using the Toshiba XARIO XG, which features a linear probe of 5-7.5 MHz frequency. The data was analyzed with the help of SPSS version 25.0. Variables like age, gender, diabetes, and Intima-media thickness (IMT) were reported and the mean ± standard deviation of Pulsatility Index, Resistive Index, Peak Systolic Velocity, and End Diastolic Velocity were calculated with a significant p-value, which is less than 0.05. An independent t-test was applied to compare Doppler indices in diabetic and non-diabetic subjects.
Results: Data was collected from 120 patients. IMT of right and left carotid artery, PI and RI of right carotid were observed to be statistically significant in diabetic and non-diabetic.
Conclusions: This study concluded that there is a significant correlation found between carotid artery disease and diabetes. Through ultrasonography, the presence of plaque and stenosis was found in more diabetic patients than in non-diabetic patients.
Keywords: Ultrasonography; Carotid artery disease; Carotid artery stenosis; Carotid plaque; Vascular ultrasound; Diabetes
Introduction![]()
More than 50% stenosis of extra cranial internal carotid arteries is linked with about 8– 15% of ischemic strokes. Among diabetic patients, the incidence of carotid artery stenosis (CAS) is rising [1]. According to the Global Burden of Diseases, Injuries, and Risk Factors Study (2015), cardiovascular disease affected 422.7 million people and killed 17.9 million people worldwide in 2015, accounting for 31% of all global deaths. Annually, approximately 23.6 million people are expected to die from cardiovascular diseases by 2030 [2]. Any occlusion in the carotid arteries causes decreased blood supply to the brain, thus leading to significant permanent injury to the brain. Deposition of cholesterol or atherosclerosis causes narrowing of the carotid artery. The symptoms of carotid artery disease depend on the location of the blocked brain blood vessel. The symptoms of carotid artery disease include numbness in arms or legs; loss of vision in one eye; slurring of speech; and numbness on one side of the face [3]. With increasing age, the carotid arterial wall undergoes structural changes. The elasticity of the vessel decreases due to the assemblage of stiff substances like collagen and calcification. These changes are most often marked in hypertensive patients and in patients with renal failure [4]. Stroke occurs due to the occlusion of the main blood vessels. The non-modifiable risk factors that lead to stroke are age, family history, sex, and race. The modifiable risk factors include carotid stenosis, transient ischemic attack, cardiac disease, hypertension, diabetes mellitus, hyperlipidemia, alcohol abuse, physical inactivity, and cigarette smoking [5].
Carotid artery disease was found in diabetics with unstable and susceptible plaques, which might result in thrombo-embolism. Compared to non-diabetics, patients with diabetes mellitus had a larger carotid intima-media thickness (CIMT). A cluster of metabolic variables, such as insulin resistance, hyperlipidemia, obesity, and arterial hypertension, have a role in the etiology of carotid artery disease in people with type 2 diabetes [6]. Carotid artery stenosis (CAS) is becoming more common in diabetes patients. Diabetic people are three times more likely than non-diabetics to develop cardiovascular illnesses (CVD), such as coronary and carotid artery problems, and stroke [7]. The carotid bifurcation, which is typically affected by atherosclerosis and is a source of both transient ischemic events and strokes, is an important site to investigate [8]. Diabetes complications can be divided into three categories: metabolic, microangiopathic, and macroangiopathic problems. It was discovered that 20% of the patients experienced a stroke within a year, and 37% experienced a stroke within five years [9].
Doppler Ultrasonography (DU) is an accurate, well-recognized, and non-invasive method for evaluating carotid artery disease. Through this technique, various parameters like the presence of plaque, intima-media thickness (IMT), blood flow velocity, and arterial diameter are measured [10]. Intima media thickness (IMT) is considered an indicator of atherosclerotic changes in the vessel [11]. DU is used not only to determine the presence or absence of plaques, as well as the early and late manifestations of vascular disease in people with and without diabetes, but also to predict who is at risk of developing cardiovascular or cerebrovascular disease [12].
This study benefits from the discovery of a significant correlation between carotid artery disease and diabetics and non-diabetics. Only a few studies are published in the literature, most of which are done only on diabetics, but our main objective is to focus on both groups [diabetics and non-diabetics]. This study contributes to the early detection of plaque or stenosis in the carotid artery in diabetic patients and non-diabetic subjects.
Methods![]()
The study was performed at the university ultrasound clinic in Green Town from October 2021 to June 2022 for duration of 8 months. Sample size was calculated by the prevalence of carotid artery stenosis in diabetic patients. The prevalence was 10% and the sample size was 138. We collected 120 cases (60 diabetic and 60 nondiabetic) due to limited time duration. We considered any history of diabetes mellitus, hypertension, ischemic heart disease, and smoking. All patients clinically suspected of having carotid artery disease were included in this study. Males and females were included. Unwilling and non-cooperative patients were excluded from this study. A convenient sampling technique was preferred. All patients were examined by Doppler ultrasonography using the TOSHIBA XARIO XG, which features a linear probe of 5–7.5 MHz frequency. The data was analyzed with the help of SPSS version 25.0. The data was reported using descriptive statistics. The mean ± standard deviation of age, PI, RI, PSV, EDV, and IMT were calculated. An independent t-test was applied to compare Doppler indices in diabetic and non-diabetic subjects. The p-value is less than 0.05, which is significant [13].
Results![]()
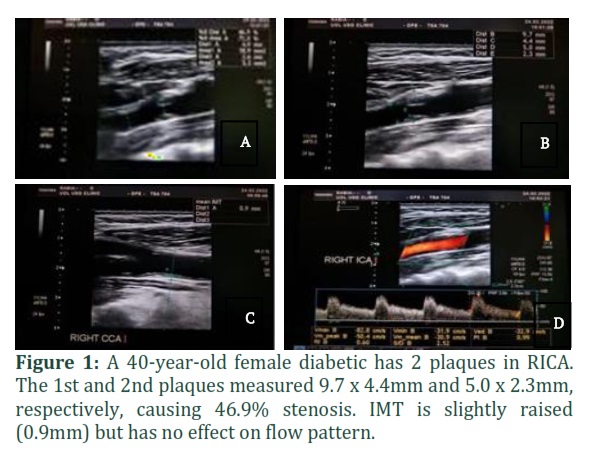
In this study, 120 patients at the University Ultrasound Clinic Green Town were enrolled. Patients were divided into 2 groups: Diabetic and non-diabetic. Minimum age of the patient was 13 and maximum was 80. The Mean of weight was = 68.21 ± 14.17. Out of 120 patients, females were 78 and males were 42. The diabetic group consisted of 60 patients (47 females and 13 males). The non-diabetic group consisted of 60 patients (31 females and 29 males). Risk factors learned from the patient's history were considered, and no laboratory tests were performed to look for additional risk factors. Ischemic heart disease, hypertension, and diabetes were observed in 14.2%, 60.0%, and 50% of patients, respectively. 18.3% were smokers. The percentage of diabetic patients with plaque was 13.3%, but there was no plaque in non-diabetic patients.
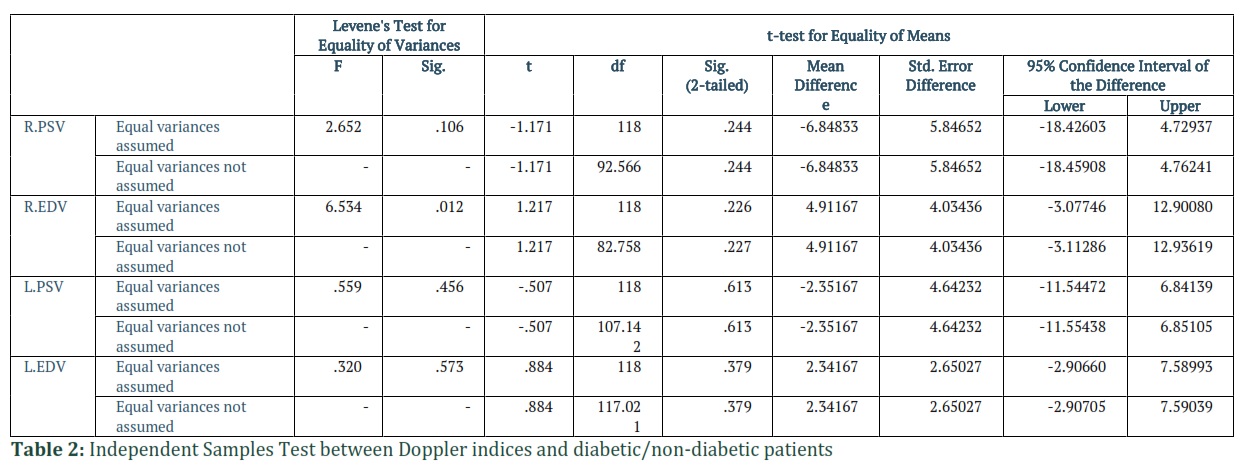
The mean and standard deviation of PSV of the right carotid artery were -71.41 ± 22.09 in non-diabetic patients while -64.56 ± 39.53 in diabetic respectively. The mean and standard deviation of EDV of the right carotid artery were -27.04 ± 13.02 in non- diabetic patients while -31.95 ± 28.41 in diabetic respectively. The mean and standard deviation of PSV of the left carotid artery were -67.10 ± 20.99 in non-diabetic patients while -64.75 ± 29.20 in diabetic respectively. In non-diabetic patients, the mean and standard deviation of EDV of the left carotid artery were -22.76 ± 13.84 while -25.10 ± 15.17 respectively (Table 1).
Right peak systolic velocity (R.PSV), Right end diastolic velocity (R.EDV), Left peak systolic velocity (L.PSV), Left end diastolic velocity (L.EDV) Mean peak systolic velocities of right and left carotid artery were compared in two groups (diabetic and non-diabetic). No statistically significant difference found between means of PSV of right carotid artery and left carotid artery in two groups as the mean difference between PSV of right and left carotid artery were -6.84 with p – value = 0.244 > = 0.05 and -2.35 with p – value = 0.613 > = 0.05 respectively. Mean end diastolic velocities of right and left carotid artery were compared in two groups (diabetic and non-diabetic). No statistically significant difference found between means of EDV of right carotid artery and left carotid artery in two groups as the mean difference between EDV of right and left carotid artery were 4.91 with p – value = 0.227 > = 0.05 and 2.34 with p – value = 0.379 > = 0.05 respectively (Table 2).
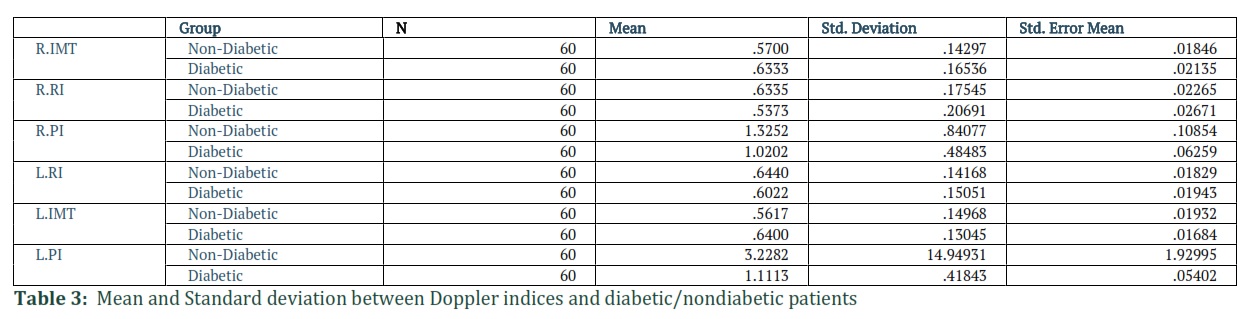
Mean and standard deviation of IMT of right carotid artery was 0.57 ± 0.14 in non-diabetic while 0.63 and 0.17 in diabetic patients respectively. Mean and standard deviation of RI of right carotid artery was 0.63 ± 0.18 in non-diabetic while 0.63 ± 0.18 in diabetic patients respectively. Mean and standard deviation of PI of right carotid artery was 1.33 ± 0.84 in non- diabetic while 1.02 ± 0.48 in diabetic patients respectively. Mean and standard deviation of IMT of left carotid artery was 0.56 ± 0.15 in non-diabetic while 0.64 ± 0.13 in diabetic patients respectively. Mean and standard deviation of RI of left carotid artery was 0.64 ± 0.14 in non-diabetic while 0.60 ± 0.15 in diabetic patients respectively. Mean and standard deviation of PI of left carotid artery was 3.22 ± 14.94 in non-diabetic while 1.11 ± 0.42 in diabetic patients respectively (Table 3).
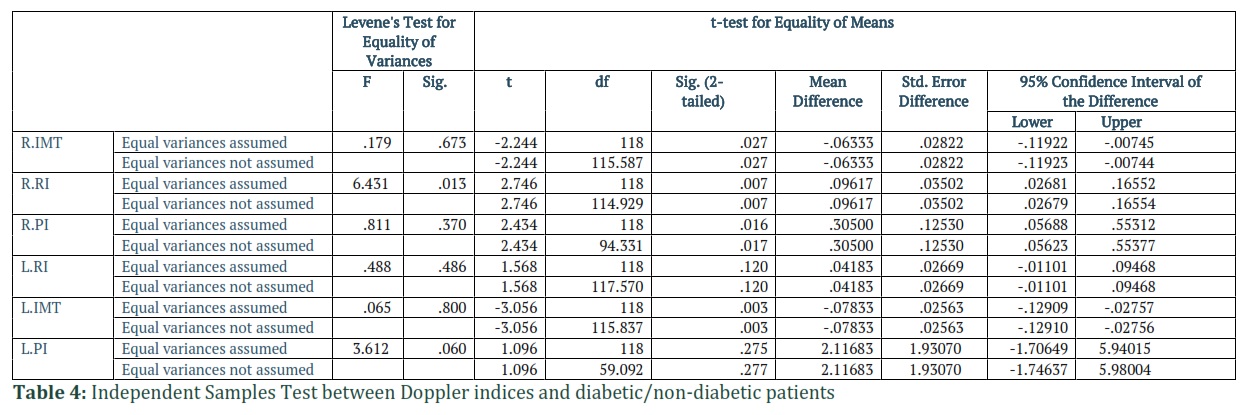
Right intima media thickness (R.IMT) ,Right resistive index (R.RI) , Right pulsatility index (R.PI) ,Left resistive index (L.RI) , Left intima media thickness (L.IMT) , Left pulsatility index (L.PI) IMT of right and left carotid artery was observed statistically significant in diabetic and non-diabetic as the mean difference between the right and left IMT was – 0.063 with p- value = 0.027 < µ=0.05 and – 0.078 with p–value =0.003 < 0.05.A statistically significant difference found between mean PI of carotid artery of right side as p- value=0.017 < 0.05. No statistically significant difference found between mean PI of carotid artery of left side as p-value =0.277 > 0.05.A statistically significant difference found between mean RI of carotid artery of right side as p-value=0.007 < 0.05. No statistically significant difference found between mean RI of carotid artery of left side as p-value =0.120 > 0.05 (Table 4).
Figures & Tables

Our objective was to assess carotid artery plaque or stenosis, which is a major cause of stroke and an early warning sign in both diabetic and non-diabetic patients. This is the only study conducted in Pakistan which explains the relation of Carotid artery disease in both diabetics and non-diabetics. This study emphasizes the importance of doppler ultrasonography in the evaluation of carotid artery stenosis.
We had two patient groups—60 diabetic and 60 non-diabetic—each with risk indicators that could be detected by Doppler ultrasound. Our results suggest that the main risk factors for carotid plaque or stenosis are diabetes, hypertension, smoking, and increasing age. In one of our literature studies, IMT has been described as an early signal for plaque formation in the carotid system, and it was proven to be a significant variable for carotid stenosis in our study [14], Age,
hypertension, diabetes, hyperlipidemia, and ischemic heart disease are some of the risk factors linked to carotid atherosclerosis [15]. In some studies, the location of plaque and the diameter of carotid arteries that can be affected by plaque have been different [16].
Risk variables, such as smoking and hypertension, were shown to be strongly related to carotid stenosis, as shown above in the analysis [17]. Hypertension was found to have a significant association with carotid atherosclerosis [18]. In most studies, it has a significant association with stroke, ischemic heart disease, peripheral vascular disease, cerebral infarction, and death [19, 20]. Only one study was found in our review that has shown a no association between hypertension and carotid stenosis [21].
Cigarette smoking has been found as a significant predictor for carotid stenosis in many studies [22]. In only 1 study, there was no link found between smoking and carotid stenosis [14]. Increasing age has been reported as a contributor to carotid artery stenosis in many studies [23].
Many studies have reported that males at all ages have a high prevalence of developing carotid atherosclerosis. However, postmenopausal females are also at high risk of developing carotid plaque [24]. Several studies have been reported that obesity (high BMI) may increase the risk of carotid atherosclerosis, which further acts as a greater risk factor for developing stroke and cerebrovascular disease [25, 26].
The right pulsatility index (PI) of ICA, which was found to be significantly associated with carotid artery stenosis in our study, has been found as a strong indicator for developing cerebrovascular and cardiovascular disease in various studies [27, 28]. The Right Resistive Index (RI) of ICA, which was found to be strongly correlated with carotid stenosis in our research, has been linked to carotid atherosclerosis and stroke [29, 30].
The most important variable that was discovered to be linked with carotid artery atherosclerosis was diabetes. Although it may not affect the development of atherosclerosis it acts as a risk element for atherosclerosis [25]. The pathophysiology of carotid atherosclerosis in diabetic patients depends upon multiple factors. The hallmark of diabetes is hyperglycemia. Hyperglycemia causes plenty of changes at the cellular level of vascular tissue that may help to speed up the atherosclerotic process. Diabetes causes cerebrovascular disease and cardiac embolism, which lead to stroke [31].
Diabetes was identified as a modifiable risk factor associated with high-grade carotid artery stenosis in a study by Baki Go ksan et al [14]. Doppler ultrasonography is a credible, precise, and noninvasive method for evaluating carotid artery stenosis that is widely available. DU should be the best option for the follow-up of patients with carotid atherosclerosis, especially those over 65 or those with other risk factors such as hypertension, diabetes, etc.
In conclusion, diabetes is considered as one of the most important risk factors that shows a significant association with carotid artery disease. The most common complication of carotid atherosclerosis is stroke. For the prevention of stroke, the main steps are early detection and management of diabetes and modifying other risk factors. Current study had some limitations. The sample size was limited and the results cannot be generalized on a larger population. Most of the participants were females.
Author Contributions
Samira Shokri: Data analysis
Kourosh Saki: Monitoring of research
Yeganeh mazaheri and Samira Shokri: Drafting
Gholamreza Jahed khaniki: Manuscript scanning
Samira Shokri: Data evaluation![]()
The authors declare that there is no conflict of interest.
![]()
References
- Paul J, Shaw K, Dasgupta S, Ghosh MK. Measurement of intima media thickness of carotid artery by B-mode ultrasound in healthy people of India and Bangladesh, and relation of age and sex with carotid artery intima media thickness: An observational study. Journal of cardiovascular disease research, (2012);2:128-131.
- Song P, Fang Z, Wang H, Cai Y, Rahimi K, Zhu Y, Fowkes FG, Fowkes FJ, Rudan I. Global and regional prevalence, burden, and risk factors for carotid atherosclerosis: a systematic review, meta-analysis, and modelling study. The Lancet Global Health, (2020);5:e721-e729.
- Sobieszczyk P, Beckman J. Carotid artery disease. Circulation, (2006);7:e244-e247.
- Rothwell PM. Carotid artery disease and the risk of ischemic stroke and coronary vascular events. Cerebrovascular Diseases, (2000);5:21-33.
- Shaikh NA, Bhatty S, Irfan M, Khatri G, Vaswani AS, Jakhrani N. Frequency, characteristics and risk factors of carotid artery stenosis in ischaemic stroke patients at Civil Hospital Karachi. JPMA, (2010);1:8-12.
- Bosevski M. Carotid artery disease in diabetic patients. Prilozi, (2014);1:53-63.
- Ali FS, Bader N, Zuberi BF, Banu S. Frequency of silent carotid artery stenosis in diabetics and its associated factors: An analysis in tertiary care hospital. Pakistan Journal of Medical Sciences, (2020);6:1270.
- De Weerd M, Greving JP, de Jong AW, Buskens E, Bots ML. Prevalence of asymptomatic carotid artery stenosis according to age and sex: systematic review and metaregression analysis. Stroke, (2009);4:1105-1113.
- Hussain MA, Bin-Ayeed SA, Saeed OQ, Verma S, Al-Omran M. Impact of diabetes on carotid artery revascularization. Journal of vascular surgery, (2016);4:1099-1107.
- Kim GH, Youn HJ. Is carotid artery ultrasound still useful method for evaluation of atherosclerosis?. Korean circulation journal, (2017);1:1-8.
- Willeit P, Tschiderer L, Allara E, Reuber K, Seekircher L, Gao LU, Liao X, Lonn E, Gerstein HC, Yusuf S, Brouwers FP. Carotid intima-media thickness progression as surrogate marker for cardiovascular risk: meta-analysis of 119 clinical trials involving 100 667 patients. Circulation, (2020);7:621-642.
- Parikh A, Daneman D. Is carotid ultrasound a useful tool in assessing cardiovascular disease in individuals with diabetes?. Diabetes technology & therapeutics, (2004);1:65-69.
- De Angelis M, Scrucca L, Leandri M, Mincigrucci S, Bistoni S, Bovi M, Calabrese G, Pippi R, Parretti D, Grilli P, Colorio P. Prevalence of carotid stenosis in type 2 diabetic patients asymptomatic for cerebrovascular disease. Diabetes, nutrition & metabolism, (2003);3:1011-1016.
- Göksan B, Erkol G, Bozluolcay M, Ince B. Diabetes as a determinant of high-grade carotid artery stenosis: evaluation of 1,058 cases by Doppler sonography. Journal of Stroke and Cerebrovascular Diseases, (2001);6:252-256.
- Anand SS, Yusuf S, Vuksan V, Devanesen S, Teo KK, Montague PA, Kelemen L, Yi C, Lonn E, Gerstein H, Hegele RA. Differences in risk factors, atherosclerosis, and cardiovascular disease between ethnic groups in Canada: the Study of Health Assessment and Risk in Ethnic groups (SHARE). The lancet, (2000);9226:279-284.
- Sacco RL, Kargman DE, Gu Q, Zamanillo MC. Race-ethnicity and determinants of intracranial atherosclerotic cerebral infarction: the Northern Manhattan Stroke Study. Stroke, (1995);1:14-20.
- Wagenknecht LE, D’Agostino Jr R, Savage PJ, O’Leary DH, Saad MF, Haffner SM. Duration of diabetes and carotid wall thickness: the Insulin Resistance Atherosclerosis Study (IRAS). Stroke, (1997);5:999-1005.
- Shah Ebrahim DM, Papacosta O, Whincup P, Wannamethee G, Walker M, Nicolaides AN, Dhanjil S, Griffin M, Belcaro G, Rumley A, Lowe GD. Carotid plaque, intima media thickness, cardiovascular risk factors, and prevalent cardiovascular disease in men and women. Arteriosclerosis, Thrombosis, and Vascular Biology, (2005);7:1482–1488.
- Sutton-Tyrrell K, Alcorn HG, Wolfson Jr S, Kelsey SF, Kuller LH. Predictors of carotid stenosis in older adults with and without isolated systolic hypertension. Stroke, (1993);3:355-3561.
- Crouse JR, Goldbourt U, Evans G, Pinsky J, Sharrett AR, Sorlie P, Riley W, Heiss G. Risk factors and segment-specific carotid arterial enlargement in the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke, (1996);1:69-75.
- Mast H, Thompson JL, Lin IF, Hofmeister C, Hartmann A, Marx P, Mohr JP, Sacco RL. Cigarette smoking as a determinant of high-grade carotid artery stenosis in Hispanic, black, and white patients with stroke or transient ischemic attack. Stroke, (1998);5:908-912.
- Dempsey RJ, Moore RW. Amount of smoking independently predicts carotid artery atherosclerosis severity. Stroke, (1992);5:693-696.
- Kawamoto R, Tomita H, Oka Y, Ohtsuka N. Association between risk factors and carotid enlargement. Internal medicine, (2006);8:503-509.
- Baldassarre D, Amato M, Bondioli A, Sirtori CR, Tremoli E. Carotid artery intima-media thickness measured by ultrasonography in normal clinical practice correlates well with atherosclerosis risk factors. Stroke, (2000);10:2426-2430.
- Su TC, Chien KL, Jeng JS, Chen MF, Hsu HC, Torng PL, Sung FC, Lee YT. Age-and gender- associated determinants of carotid intima-media thickness: a community-based study. Journal of atherosclerosis and thrombosis, (2012);9:872-880.
- De Michele M, Panico S, Iannuzzi A, Celentano E, Ciardullo AV, Galasso R, Sacchetti L, Zarrilli F, Bond MG, Rubba P. Association of obesity and central fat distribution with carotid artery wall thickening in middle-aged women. Stroke, (2002);12:2923-2928.
- Oughton JA, Rose S, Galloway G, Khoo SK, O'Neill S, Coulthard A. Carotid ultrasound pulsatility indices and cardiovascular risk in Australian women. Journal of medical imaging and radiation oncology,(2015);1:20-15.
- Hitomi Y, Masaki N, Ishinoda Y, Kagami K, Yasuda R, Toya T, Namba T, Nagatomo Y, Takase B, Adachi T. Effectiveness of pulsatility index of carotid Doppler ultrasonography to predict cardiovascular events. Journal of Medical Ultrasonics, (2022);1:95-103.
- Frauchiger B, Schmid HP, Roedel C, Moosmann P, Staub D. Comparison of carotid arterial resistive indices with intima-media thickness as sonographic markers of atherosclerosis. Stroke, (2001);4:836-841.
- Bai CH, Chen JR, Chiu HC, Pan WH. Lower blood flow velocity, higher resistance index, and larger diameter of extracranial carotid arteries are associated with ischemic stroke independently of carotid atherosclerosis and cardiovascular risk factors. Journal of Clinical Ultrasound, (2007);6:322-330.
- Chait A, Bornfeldt KE. Diabetes and atherosclerosis: is there a role for hyperglycemia?. Journal of lipid research, (2009);1:S335-S339.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


