

![]()
Microbial profiling and risk factors assessment for Otitis Media and Otitis Externa
Tayyaba Ijaz1, Aftab Ahmad Anjum2, Sana Aslam1,Sarwat Ali Raja2, Abdul Rehman Khawaja3, Saadia Ijaz1
Adv. life sci., vol. 1, no. 4, pp. 191-196, August 2014
*Corresponding Author: Tayyaba Ijaz (Email: tayyabalhr@yahoo.com)
Author Affiliations
2- University of Vet & Animal Sciences, Lahore – Pakistan
3- Allama Iqbal Medical College, Lahore – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Otitis media and otitis externa are common otological manifestations in all generations especially in children. There is lack of accurate identification of the causative agent and thus poor diagnosis for such infections. Therefore, it leads to permanent anatomical disabilities including poor speech and defects in balancing and hearing. The study was conducted to isolate, characterize and identify the microbes causing otitis media and otitis externa.
Methods: A total of 250 patients having otitis media and otitis externa were enrolled in the study from March 2011 to October 2011. All patients were examined through clinical examination and detailed history was collected. Pus samples from the discharging ears were plated on MacConkey’s, Chocolate and Blood agar for 24 to 48 hours. Isolates were identified on the basis of morphology, staining reactions and various biochemical tests.
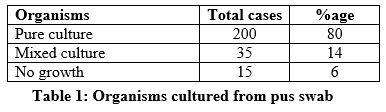
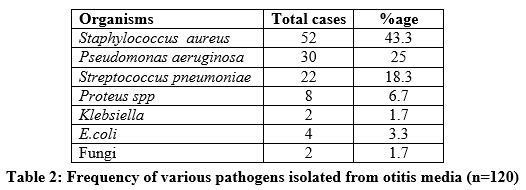
Results: In this study, only 6% cases yielded no growth, 14% yielded mixed cultures while 80% cases yielded pure cultures. The presumptive diagnosis for ear swabbing was otitis media (76%) and otitis externa (24%). The most common bacterial isolates obtained were Staphylococcus aureus (43.3%) followed by Pseudomonas aeruginosa (25%) in the diagnosed cases of otitis media. While for the cases of otitis externa, Pseudomonas aeruginosa was the predominant organism with 52.2%. Infection of otitis media was most common among children and the persons having low socioeconomic conditions.
Conclusion: Pseudomonas aeruginosa was identified as the principal pathogen followed by Staphylococcus aureus. To circumvent the painful effects of acute and chronic ear infections, an accurate microbial profiling may play pivotal role.
Key words: Otitis media, Otitis externa, Pathogens, Prevalence, Eustachian tube
Introduction
Otitis media and otitis externa infection is a frequent problem in the tropics. Relatively higher numbers of ear infections occur in children with 2 years of age. For instance, in America alone, children of mentioned age have 9.1 million episodes of otitis media in a year. While, annual incidence rate for otitis externa is 8.1/1000 which increases in summer season. These infections may arise from the external auditory meatus in otitis externa, or from the middle ear cavity in otitis media [1]. Otitis media is the infection of middle ear. It is caused by resident bacterial pathogens and usually results in severe respiratory infection [2-4].
Complications for otitis media vary depending on the level of severity and duration of the infection in relationship to the associated microorganisms. There are two types of otitis media, acute otitis media (AOM) and chronic suppurative otitis media (CSOM) [1,5]. The organisms often isolated in cases of acute otitis media are: Haemolytic Streptococci, Staphylococci, Haemophilus or Pneumococci while gram negative bacilli are commonly associated with chronic otitis media particularly Pseudomonas and Proteus sp. [6,7].
Acute otitis media (AOM) can cause inflammation and pain that leads to insomnia, unusual irritability, loss of balance, ear drum perforations, draining of fluid in the ear, brain abscess and vomiting. If a severe infection is not cured in time it may leads to death [8]. Otitis media infection may spread to the middle ear through the route of Eustachian tube. The causes of infection in such cases are nasopharyngeal diseases [9]. The risk factors of otitis media include allergies, exposure to smoke, cigarette and respiratory infections [10].
Otitis externa or swimmer’s ear is an inflammation of the ear canal and outer ear. Otitis Externa is more prevalent in teenagers with occasional association to otitis media or respiratory tract viral infections [11]. The symptoms include inflammation of the pinna, characterized by pruritus, pain, foul-smelling discharge, reduced hearing, and vertigo. The most common organism reported in otitis externa is the Pseudomonas sp., while others are Staphylococcus, Streptococcus and fungi. In malignant otitis externa, the bacterial infection can affects the deeper underlying soft tissues of ear and destroy the temporal bone.
Several errors including bias on the part of parents, physicians in using antibiotics can lead to the over-diagnosis of otitis media and otitis externa. Finally, inappropriate antibiotic treatment of the condition encourages the emergence of multidrug-resistant strains of bacterial pathogens.
Methods
A total of two hundred and fifty (250) patients suffering from various ear infections visiting ENT Out Patient Department at Mayo Hospital (Lahore), Pakistan were selected for the study during a period of eight months (March – October, 2011). Purulent materials were collected with sterile swab sticks and transported to the Microbiology Laboratory where they were processed immediately. These samples were cultured on MacConkey agar, blood agar and chocolate agar plates by streaking method. The cultured plates were then incubated at 37°C in an incubator for 24 hours (hours). The colonies were further sub cultured on nutrient agar s to obtain pure colonies. Isolated bacteria were characterized on the basis of colony morphology, growth characteristics and standard biochemical tests. Various associated risk factors were also analyzed using a questionnaire filled by the patients.
Results
Out of two hundred and fifty (250) patients, 62 (24.8%) were male patients, 87 (34.8%) female while 101 (40.4%) were children. In socioeconomic grouping 4% patients were from the upper, 20% from the middle and 76% from the lower group (Figure 1 & 2). Otitis media was more prevalent among children of less than 10 years of age (40%) and 60% of these children were bottle fed or had sore throat infection. In the case of otitis externa, 45.8% (the highest) infected people were predominantly from the age group of 21-30 years. In our study, there was absence of growth in 6% cases, 14% yielded mixed cultures while 80% cases yielded pure cultures (Table 1). The results from the biochemical and morphological characterization of the bacterial isolates from the otitis media samples revealed that the most common bacterial isolates were Staphylococcus aureus (43.3%), Pseudomonas aeruginosa (25%), Streptococcus sp. (18.3%) followed by Proteus sp. (6.7%), Klebsiella (1.7%), Escherichia coli (3.3%) and fungi (1.7%) (Table 2). In the case of otitis externa, the pure cultures yielded P. aeruginosa in 52.5% of the cases, S. aureus in 21.2%, Streptococcus pneumonia in 10%, E. coli in 5%, Proteus sp. in 7.5% and fungi in 3.8% of the cases (Table 3).
A strong association was found between Socio economic status, visiting untrained practitioners, using objects and swimming with the Otitis (p< 0.05).
Data & Tables
Discussion
Ear diseases have plagued humanity even before the modern history started. These diseases even today, lead to a wide variety of complications. Various complications associated with Otitis media such as irreversible local destruction of middle ear structures, facial palsy, serious intracranial and extracranial complications are among the most common conditions seen by the otologists, paediatricians and the general practitioners [12].
In our study, the prevalence of otitis media was found to be greater among children of less than 10 years age and those who were bottle fed. This might be due to the reason that the susceptibility of the children to otitis media is traceable to their immune system and to the particular constitution (shorter and straight/horizontal) Eustachian tube. These observations are in concordance with the reports of Klien and Howard et al., [5,13]. So, with the decline of breast feeding and with the increase of environmental exposures, the increased risk for otitis media episodes during the first 2 years of life was identified.
The role of occupational status in relevance to certain risk factors of otitis media was also studied. In developing countries like Pakistan, socio-economic status of large population is low. Moreover, inappropriate safety precautions at industrial work place produce otitis media and certain allergies among laborers. . Frequency of otitis media was found to be 60% in children having sore throat infection. Other researchers recorded similar results and concluded that otitis media with hearing loss is common in children having recurrent upper respiratory tract infection [14].
Otitis externa was common among teenagers because swimming in polluted water was the most common way to contract swimmer’s ear disease [11]. The pathological investigation of otitis media revealed that S. aureus was more frequently isolated (43.3%) and was recovered mostly from the individuals who were habitual of using wooden sticks, matchsticks, keys, hair pin and those who visited untrained practitioners for the purposes of ear cleaning. It can be observed in the results that S. aureus was an opportunistic pathogen This is in accordance with other studies conducted to check an outbreak of otitis externa and its bacteriological investigation [15-17].
In this study, P. aeroginosa was found the more prominent causative agent of otitis externa followed by Staphylococcus sp. The reason probably lies in the fact that the epithelium of the ear canal absorbs moisture from the environment, and in this situation maceration may occur in the ear canal leading to invasion of skin organisms and opportunistic gram-negative pathogens such as P. aeruginosa. Similar findings were reported by some other researchers [18,19].
Conclusively, S. aureus was found as the most common pathogen followed by P. aeruginosa isolated from otitis media. While in case of otitis externa, P. aeruginosa was the highest in peak as compared to other pathogens. There has been a dramatic increase in the number of consultations to the pediatricians for otitis, therefore, efforts should be made to reduce the factors militating its occurrence in the community.
References
- Oni A, Nwaorgu O, Bakare R, Ogunkunle M, Toki R. The discharging ears in Adults in Ibadan, Nigeria causative agents and antimicrobial sensitivity pattern. African Journal of Clinical and Experimental Microbiology, (2002); 3(1): 3-5.
- Celin B, Collins J, Yilmaz M. Tackling Otitis Media in Adults. Journal of Emerging Medicine, (1992); 1567-68.
- Isah K, Abubakar T. Chronic suppurative otitis media. A clinical profile in Sokoto Sahel. Med J, (2003); 6(3): 75-78.
- Dubey SP, Larawin V. Complications of chronic suppurative otitis media and their management. The laryngoscope, (2007); 117(2): 264-267.
- Klein JO. Otitis media. Clinical infectious diseases, (1994); 823-832.
- Jokipii AM, Karma P, Ojala K, Jokipii L. Anaerobic bacteria in chronic otitis media. Archives of otolaryngology, (1977); 103(5): 278-280.
- Riding KH, Bluestone CD, Michaels RH, Cantekin EI, Doyle WJ, et al. Microbiology of recurrent and chronic otitis media with effusion. The Journal of pediatrics, (1978); 93(5): 739-743.
- Arroll B. Antibiotics for upper respiratory tract infections: an overview of Cochrane reviews. Respiratory medicine, (2005); 99(3): 255-261.
- Eskola J, Kilpi T, Palmu A, Jokinen J, Eerola M, et al. Efficacy of a pneumococcal conjugate vaccine against acute otitis media. New England Journal of Medicine, (2001); 344(6): 403-409.
- Froom J, Culpepper L, Green LA, de Melker RA, Grob P, et al. A cross-national study of acute otitis media: risk factors, severity, and treatment at initial visit. Report from the International Primary Care Network (IPCN) and the Ambulatory Sentinel Practice Network (ASPN). The Journal of the American Board of Family Practice, (2001); 14(6): 406-417.
- McCoy SI, Zell ER, Besser RE. Antimicrobial prescribing for otitis externa in children. The Pediatric infectious disease journal, (2004); 23(2): 181-183.
- Jang C, Park S. Emergence of ciprofloxacin‐resistant pseudomonas in chronic suppurative otitis media. Clinical Otolaryngology & Allied Sciences, (2004); 29(4): 321-323.
- Duffy LC, Faden H, Wasielewski R, Wolf J, Krystofik D. Exclusive breastfeeding protects against bacterial colonization and day care exposure to otitis media. Pediatrics, (1997); 100(4): e7-e7.
- Raza M, Jalil J, Shafique M, Ghafoor T. Frequency of Otitis Media with Effusion in recurrent upper respiratory tract infection in children. J Coll Physician Surg Pak, (2008); 18(4): 226-229.
- Ahmed S, Iqbal M, Hassan Z, Khurshid T, Ali L, et al. Spectrum and bacterial isolates in chronic suppurative otitis media in Khuzdar. Pak J Otolaryngol, (2006); 2234-36.
- Ahmed B, Hydri AS, Ejaz A, Farooq S, Zaidi S, et al. Microbiology of ear discharge in Quetta. Journal of the College of Physicians and Surgeons–Pakistan: JCPSP, (2005); 15(9): 583.
- Yeo SG, Park DC, Hong SM, Cha CI, Kim MG. Bacteriology of chronic suppurative otitis media-a multicenter study. Acta oto-laryngologica, (2007); 127(10): 1062-1067.
- Kuczkowski J, Samet A, Brzoznowski W. [Bacteriologic evaluation of otitis externa and chronic otitis media]. Otolaryngologia polska The Polish otolaryngology, (1999); 54(5): 551-556.
- Van Asperen IA, De Rover CM, Schijven JF, Oetomo SB, Schellekens JF, et al. Risk of otitis externa after swimming in recreational fresh water lakes containing Pseudomonas aeruginosa. Bmj, (1995); 311(7017): 1407-1410.


