

![]()
Clinical effectiveness of Carbimazole and Propylthiouracil for Hyperthyroidism in Patients of Punjab, Pakistan
Maria Fareed Siddiqui*1, Sidra Hasnain2, Zahra Batool3, MH Qazi1, Muhammad Imtiaz3, Ismat Fatima4, Rabail Alam3
Adv. life sci., vol. 2, no. 1, pp. 10-15, November 2014
*- Corresponding Author: Maria Fareed Siddiqui (Email: maria.pharmacist@gmail.com)
Author Affiliations
2- Department of Pharmaceutical Sciences, Superior University, Lahore- Pakistan
3- Institute of Molecular Biology and Biotechnology, University of Lahore, Lahore- Pakistan
4- Centre for Nuclear Medicine, Mayo Hospital, Lahore- Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The primary objective of any drug for hyperthyroidism is to control clinical manifestations and maintenance of normal levels of hormonal concentrations. It also targets to prevent the recurrence of disease along with minimizing associated risk factors. In this study, effectiveness of oral anti thyroid agents was checked to normalize altered levels of thyroid hormones due to hyperthyroidism.
Methods: The study was comprised of 40 subjects of whom 30 were experiencing hyperthyroidism and were administered anti-hyperthyroid drugs. 10 patients of hyperthyroidism were not taking any medication. Standard dose regimens of carbimazole and propylthiouracil were employed for all 30 hyperthyroid patients under closed monitoring. Physical as well as biochemical analyses of all subjects were done and thyroid profiling was performed for measuring levels of free thyroxine (fT4), free triiodothyronine (fT3), thyroid stimulating hormone (TSH) and antibodies against thyroglobulin (Tg).
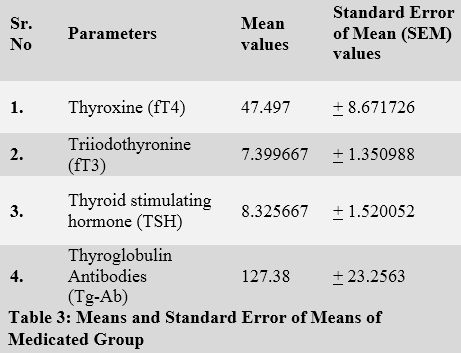
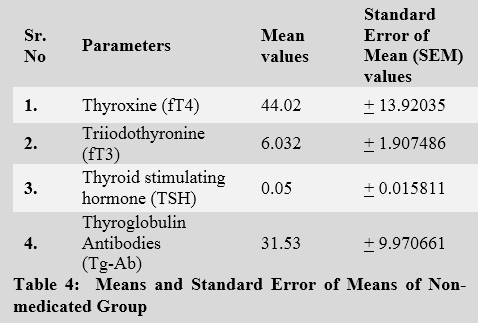
Results: Thyroid profiles of medicated hyperthyroid patients were compared with the profiles of non-medicated group. Statistical analysis appeared with non-significant values for all four parameters.
Conclusion: No significant difference was found between medicated and non-medicated groups. We recommend that combinatorial drugs and new derivatives with better efficacy and fewer side effects should be employed to treat hyperthyroidism.
Key words: Carbimazole, Propylthiouracil, Hyperthyroidism, Thyroid stimulating hormone, Thyroxine, Triiodothyronine
Introduction
Thyroid gland is one of the major endocrine gland involved in synthesis of three hormones triiodothyronine (T3), thyroxine (T4) and calcitonin [1]. These hormones are synthesized by a glycoprotein, thyroglobulin (Tg) produced in follicular colloid of thyroid cells upon stimulation by thyroid stimulating hormone (TSH) [4]. Various biological procedures such as growth, development, reproduction, metabolism, nervous system maturation and muscle functions are regulated by thyroid hormones and variations in these hormones lead towards mild to severe ailment [2]. Complications that are usually observed in Hyperthyroidism are Tachycardia, hypotension, diarrhea, sepsis, trauma, acute renal failure, lactic acidosis, cardiac dysrhythmia and thyroid storm in most severe cases [3]. Tg also serves as a sensitive marker to monitor recurrence of hyperthyroidism disease due to variation of its levels in thyroid disorders [5].
In case of autoimmune hyperthyroidism or hypothyroidism, antibodies against Tg are present and cancerous states of thyroid gland such as follicular and papillary cancers as well as certain concurrent diseases like type 1 diabetes, rheumatoid arthritis and pernicious anemia are also evaluated by estimating antibodies against Tg. Antibodies against thyroglobulin may also be present in patients with Hashimoto’s thyroiditis, myxedema, hypothyroidism, thyrotoxicosis, Graves’ disease, and simple goiters are not expressed when thyroglobulin serve as tumor marker [6]. If circulating levels of thyroid hormone are decreased then levels of thyroid stimulating hormone will be increased as it has been seen in certain thyroid disorders, so TSH is another marker to evaluate thyroid status [7]. In hyperthyroidism, TSH (thyroid stimulating hormone) receptor antibodies and Tg-Ab are responsible for autoimmune response of this disease and it is 4-7 times more common in females than males [8]. It occurs at any intervals of life mostly in 3rd and 4th intervals [9].
It has been well reported that certain environmental factors are there which are grossly responsible for the probability of cancer and interruption in immune system of thyroid gland and these are; iodine intake, atomic radiations and therapeutic applications [10]. All of these players markedly change levels and functions of thyroid markers and effectiveness of drugs used in hyperthyroidism lies in reversing these abnormal parameters.
For coping up with these hazardous and chief factors in order to reduce associated thyroid disorders, anti- thyroid medications are recommended to minimize reappearance of ailment as well improving patient’s quality of life. Hypo and hyperthyroidism patients should receive treatment that may keep their hormone levels at normal state. Hyperthyroidism patients are critical, they must be treated by a specialist whereas hypothyroid patients can be treated or diagnosed by general practitioners. In the battle against thyroid disorders many efforts have been done on thyroid drugs for identifying promising outcomes. First line of treatment in hyperthyroidism is drug therapy or radioactive iodine but in critical conditions surgery may be done [11].
Anti thyroids are the first choices of treatment in clinical settings and are source for cure of disease in 40% of hyperthyroidism patients. Radioactive iodine is given to those patients who previously relapse from anti thyroid drugs but also can be given initially if patients have toxic nodule or multi-nodular goiter because anti thyroids do not relieve this goiter formation.
The primary anti thyroid drugs prescribed in Pakistan to treat hyperthyroidism are; carbimazole and propylthiouracil. These drugs have also been proven to be used for patients to prepare them for radioactive iodine therapy or surgery.
CARBIMAZOLE
Carbimazole is commonly used in the treatment of hyperthyroidism. It efficiently reduces the mass of thyroid hormones synthesized by the thyroid gland. It is administered in the form of high initial dose before surgery or administration of radioactive iodine. Possible side effects are nausea, headache, joint pain, gastrointestinal problem, skin rash, itching, hair loss, urticaria, bone marrow problems and muscle pain [12].
PROPYLTHIOURACIL
Propylthiouracil was published by FDA (food and drug administration) in 2009 for liver failure and hyperthyroidism. It inhibits the conversion of T4 to T3. It is given 2-3 times a day because of its short acting lifespan and lowers down thyroid hormone levels [13]. Propylthiouracil is the drug of choice for pregnant women because it has a lower risk of birth defects [14]. Major side effects are agranulocytosis, aplastic anemia, hepatitis, acute renal failure, nausea, urticaria, jaundice and leukopenia.
Methods
The study included 40 patients who were experiencing hyperthyroidism and they appeared with positive symptoms for thyrotoxicosis. Patients were divided into two groups. Group I was comprised of 30 patients who were taking two anti-thyroid drugs; carbimazole and propylthiouracil as primary treatment. 10 patients were included in Group II and they were not using any medicine.
Patients were recruited from Centre of Nuclear Medicine (CENUM), Mayo Hospital, Lahore, and, selection was made after taking complete history and medical as well as physical examinations were also done before sampling of patients. The hormonal statuses of patients were evaluated by using ELISA kits of Monobind Company for fT3 and fT4 with catalogue numbers: T3 eia1k-314 and T4 eia2k-314 respectively. TSH and Tg-Ab were estimated through ELISA kits of Generic Assay GmbH Company with catalogue numbers 109570-14 and 119570-14 respectively.
Patients were recruited after signing consent forms and those with any concomitant disorder were strongly restricted in the study. In our community hospitals, carbimazole is the major drug which is used to treat hyperthyroidism owing to its reported efficacy over propylthiouracil and lesser side effects [15].
In group I, 20 patients were prescribed carbimazole while 10 were on propylthiouracil therapy. Standard dosage regimens i.e., 15-40 mg /day and 200-400 mg/ day of carbimazole and propylthiouracil respectively were employed for medicated group.
Sampling of group I was done at the end of third month of therapy at fasting state and drug treatment was not stopped in them, while sampling of group II was done before initiation of therapy.
Results
All the results are given in tables and figures, below.
Tables & Figures
Figure 1 Table 1 Table 2 Table 3 Table 4
Discussion
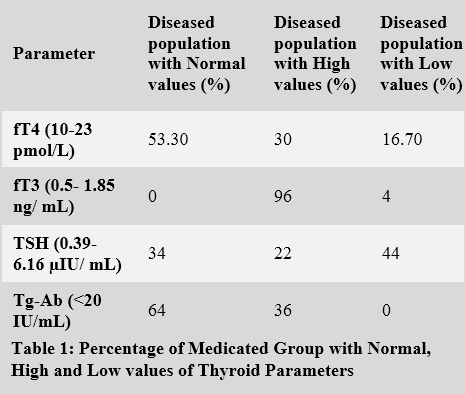
We examined effects of anti-thyroid drugs on thyroid parameters i.e. fT3, fT4, TSH and Tg-Ab in hyperthyroidism patients of Pakistani population. A total of 53.3 % population appeared with normal levels of fT4 while populations with the normal fT3, TSH and Tg-Ab were 0%, 34% and 64% respectively. Percentages of patients with higher values were 30, 96, 22 and 36 for fT4, fT3, TSH and Tg-Ab. Neither of the drugs proved to be completely effective in normalizing all altered thyroid parameters associated with hyperthyroidism.
Both of the drugs i.e. propylthiouracil and carbimazole did not prove any significant effect on thyroid markers. Results are comparable with the study done by Mary H. Samuels in 2001 in which it was concluded that anti thyroid drugs in hyperthyroidism are effective but are not responsible for the successful treatment of this disease [16].
Recently improved efficacy of carbimazole over propylthiouracil has been discussed by Douglas Ross et al. in 2011 which proves that carbimazole is more effective than propylthiouracil in some degree of effectiveness as it lowers down the levels of thyroid hormones more quickly than propylthiouracil and has less side effects and mostly given before radioiodine treatment. Furthermore, it is considered as a drug of choice for hyperthyroidism. There are reports regarding its efficacy which strongly prove that, even in prolonged usage, long term remission rate is less than 50% [17].
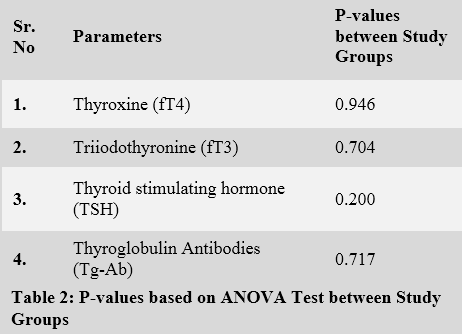
According to our study fT3 and fT4 are non-significant in medicated hyperthyroid cases when compared with non-medicated group with p-values i.e., 0.946 and 0.704 respectively and these non-significances were also seen in study done by Mary Shomon [18]. Several studies have been stated that TSH is an ideal investigation in estimation of thyroid disorder. No difference found between TSH levels of medicated and non-medicated groups as we can see from the p-value of 0.200.
The levels of antibodies against thyroglobulin were also appeared insignificant between medicated and non-medicated groups with p-value 0.717, again showing the inefficacy of both drugs in normalizing disturbed levels of thyroid marker.
The variations in the values of TFTs even after the use of propylthiouracil and carbimazole lead to the conclusion that block regimens must be used to achieve euthyroid status. This may be supported by the studies of Vanderpump MPJ in 1996, and Weetman AP in 2001, concluding that by acquiring dose adjustment in doses of carbimazole for blocking thyroid function and thyroxine for the replacement of thyroid hormones will be more beneficial and smooth in controlling biochemical pathology of hyperthyroidism [19,20].
Propylthiouracil and carbimazole also have been reported to reduce the effectiveness of radioiodine therapy in patients with Grave’s disease as reported by Roberto B. Santos et al in 2004. They examined 100 patients with Grave’s disease of different age, gender, anti-thyroid drug pretreatment duration, goiter size, thyroid hormones T3, T4, fT4 and anti thyroid antibodies who took radioiodine treatment in different month intervals. These patients were withdrawn from anti thyroids before 15 days of radioiodine treatment. They resulted out that there are more chances of failure of iodine 131 therapies in those who took propylthiouracil before therapy rather than those who took methimazole [21].
Siersbaek et al, in 1978 estimated extra thyroidal effects of anti-thyroids on serum levels of thyroid hormones T3, T4, reverse T3 and TRH. They took 19 patients who were having severe hyperthyroidism and treated with fT4. Serum T3 levels decreased during administration of propylthiouracil but reciprocal increase in rT3 was seen. There were no considerable changes in serum T4 and TSH. Furthermore, carbimazole did not affected by any of the parameters studied above [22].
Recently, in 2011, Luigi Bartalena et al. explained the effectiveness of methimazole in hyperthyroidism. Methimazole is more effective than propylthiouracil because it has fewer side effects than the second one. Propylthiouracil is only effective for pregnant women. In case of toxic multi-nodular goiter and toxic adenoma, methimazole can be given before surgery. Major side effects are agranulocytosis, severe hepatotoxicity and vasculitis [23].
Conclusion and Future Perspectives
In light of our findings, physicians are suggested to prescribe block regimen and focus should be put on new derivatives with greater efficacy and fewer side effects in our community hospitals for decreasing severity of pathology. Moreover the combinatorial use of triiodothyronine along with thyroxine should be exploited for better results and these results may be validated using a bigger set of data.
References
- Wirth EK, Sheu S-Y, Chiu-Ugalde J, Sapin R, Klein MO, et al. Monocarboxylate transporter 8 deficiency: altered thyroid morphology and persistent high triiodothyronine/thyroxine ratio after thyroidectomy. European Journal of Endocrinology, (2011); 165(4): 555-561.
- Malandrino P, Latina A, Marescalco S, Spadaro A, Regalbuto C, et al. Risk-adapted management of differentiated thyroid cancer assessed by a sensitive measurement of basal serum thyroglobulin. The Journal of Clinical Endocrinology & Metabolism, (2011); 96(6): 1703-1709.
- Garber JR, Cobin RH, Gharib H, Hennessey JV, Klein I, et al. Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Endocrine Practice, (2012); 18(6): 988-1028.
- Spencer CA, LoPresti JS. Technology Insight: measuring thyroglobulin and thyroglobulin autoantibody in patients with differentiated thyroid cancer. Nature Clinical Practice Endocrinology & Metabolism, (2008); 4(4): 223-233.
- Iervasi A, Iervasi G, Bottoni A, Boni G, Annicchiarico C, et al. Diagnostic performance of a new highly sensitive thyroglobulin immunoassay. Journal of endocrinology, (2004); 182(2): 287-294.
- Harish K. Thyroglobulin: current status in differentiated thyroid carcinoma (review). Endocrine regulations, (2006); 40(2): 53-67.
- De Escobar GM, Obregón MJ, Del Rey FE. Role of thyroid hormone during early brain development. European Journal of Endocrinology, (2004); 151(Suppl 3): U25-U37.
- Tallstedt L, Lundell G, Tørring O, Wallin G, Ljunggren J-G, et al. Occurrence of ophthalmopathy after treatment for Graves' hyperthyroidism. New England Journal of Medicine, (1992); 326(26): 1733-1738.
- Pinto A, Glick M. Management of patients with thyroid disease: oral health considerations. Journal of the American Dental Association (1939), (2002); 133(7): 849-858.
- Feldt-Rasmussen U, Rasmussen AK. Autoimmunity in differentiated thyroid cancer: significance and related clinical problems. Hormones, (2010); 9(2): 109-117.
- Abraham P, Avenell A, Watson WA, Park CM, Bevan JS. Antithyroid drug regimen for treating Graves’ hyperthyroidism. Cochrane Database Syst Rev, (2005); 18(2).
- Uduak O, Ani EJ, Etoh E, Macstephen AO. Comparative effect of Citrus sinensis and carbimazole on serum T 4, T 3 and TSH levels. Nigerian Medical Journal, (2014); 55(3): 230.
- Vitti P, Rago T, Chiovato L, Pallini S, Santini F, et al. Clinical features of patients with Graves' disease undergoing remission after antithyroid drug treatment. Thyroid, (1997); 7(3): 369-375.
- Cooper DS. Antithyroid drugs. New England Journal of Medicine, (2005); 352(9): 905-917.
- Warnock AL, Cooper DS, Burch HB. Life-Threatening Thyrotoxicosis: Thyroid Storm and Adverse Effects of Antithyroid Drugs. Congestive heart failure, (2014); 130(139): 20.
- Samuels MH. The Use of Tests for the Diagnosis and Monitoring of Thyroid Disease. Lab Medicine, (2001); 32(5): 257-259.
- Ross DS. Radioiodine therapy for hyperthyroidism. New England Journal of Medicine, (2011); 364(6): 542-550.
- Shomon M (2000) Living well with hypothyroidism. New York, Avon Books.
- Vanderpump M, Ahlquist J, Franklyn J, Clayton R. Consensus statement for good practice and audit measures in the management of hypothyroidism and hyperthyroidism. The Research Unit of the Royal College of Physicians of London, the Endocrinology and Diabetes Committee of the Royal College of Physicians of London, and the Society for Endocrinology. BMJ: British Medical Journal, (1996); 313(7056): 539.
- Ajjan RA, Weetman AP. Medical management of hyperthyroidism. European Endocrine Disease, (2007); 177-80.
- Santos RB, Romaldini JH, Ward LS. Propylthiouracil reduces the effectiveness of radioiodine treatment in hyperthyroid patients with Graves' disease. Thyroid, (2004); 14(7): 525-530.
- Siersbaek-Nielsen K, Kirkegaard C, Rogowski P, Faber J, Lumholtz B, et al. Extrathyroidal effects of propylthiouracil and carbimazole on serum T4, T3, reverse T3 and TRH-induced TSH-release in man. Acta endocrinologica, (1978); 87(1): 80-87.
- Marcocci C, Kahaly GJ, Krassas GE, Bartalena L, Prummel M, et al. Selenium and the course of mild Graves' orbitopathy. New England Journal of Medicine, (2011); 364(20): 1920-1931.


