

![]()
Status of oxidative stress in breast cancer patients in Pakistani population
Sara Javed, Muhammad Ali, Fatima Ali, Sanam Saiqa Anwar, Nadia Wajid*
Adv. life sci., vol. 2, no. 3, pp. 115-118, May 2015
*- Corresponding Author: Nadia Wajid (Email: Nadia.wajid@imbb.uol.edu.pk)
Author Affiliations[Date Received: 12/07/2014; Date Revised: 11/05/2015; Date Published Online: 25/05/2015]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Breast cancer is a major risk factor to the health of women around the globe and every year more than one million women are diagnosed with it. Pakistan is considered on the highest risk of breast cancer among Asian countries. One of the major reasons associated with higher incidence rate is oxidative stress condition in Pakistani women. The aim of this study was to analyze oxidative stress in patients with breast cancer in local population.
Methods: Activity of antioxidant enzymes i.e. superoxide dismutase (SOD) and catalase, level of reduced glutathione (GSH) were measured in the blood samples of breast cancer patients. To emphasize the results and the extent of lipid peroxidation in terms of malonyl dialdehyde (MDA) level were also evaluated. All the activities from cancer patients were compared with those of healthy people taken as control.
Results: The levels of GSH and MDA were found higher in the patients as compared to control group. While, activity of SOD and catalase enzymes was low in the diseased group.
Conclusion: Our study shows a significant oxidative stress in breast cancer patients in local population.
Key words: Breast cancer, Oxidative stress, Lipid peroxidation, Antioxidants, Reactive Oxygen Species
Introduction
Worldwide, breast cancer is one of the most prevalent cancers amongst females [1]. Breast cancer is actually the malignant tumor which develops from cells present within the breast. It mostly begins in the ducts of the breast and sometimes in the lobules and rarely in the stromal tissues such as fatty and fibrous connective tissue [2].
Oxidative stress is caused by high production of reactive oxygen species (ROS) or low antioxidant defense system [3,4]. Experimental documentation revealed that the ROS take part in the pathogenesis of breast cancer. Free radicals actively serve in cell proliferation and cause serious harm to membrane, mitochondria and macromolecules along with proteins, lipids and DNA. This damage to cell and cell organelles serve as a signal to initiate an inflammatory response and thus disease progression is stimulated. Enhanced oxidative stress in the tissues of breast tumor was reported in comparison to non-malignant tissues [5-7]. Additionally, growing evidences also suggest that oxidative stress leads to the neoplastic progressiveness and metastasis [8]. Therefore, investigating oxidative stress at early stages in the patients can help clinicians to design efficient therapies [9].
An essential antioxidant enzyme superoxide dismutase (SOD) decays the harmful superoxide anions into hydrogen peroxide and provides protection against free radicals. Extravagant buildup of superoxide anions leads to elevated free radical mediated injury causing reduction of SOD activity. Glutathione (GSH) is another antioxidant which behaves like a reducing agent. It converts hydrogen peroxide into water and alters lipid peroxidation products into their corresponding alcohols and hence mediates protective action [10]. Catalase, another antioxidant enzyme is responsible for conversion of hydrogen peroxide to oxygen and water [11]. Malonyl dialdehyde (MDA) is a type of ROS produced as a result of lipid peroxidation. Oxidative stress is the source of inflammation in breast cancer patients.
The present study aims to evaluate the status of free radical species as well as antioxidant enzymes in breast cancer patients.
Methods
Collection of Cancer Plasma
The Blood samples of 100 female Breast Cancer patients without any therapeutic intervention and 100 normal females were taken with informed consent from INMOL (Institute of Nuclear Medicine and Oncology) hospital, Lahore. A total of 2-3 ml blood was collected from each patient into EDTA vial and plasma was isolated. Randomly samples from 10 patients were pooled and passed through syringe filter (0.22 µm) and stored at -20˚C.
Estimation of GSH
Amount of reduced GSH in plasma was estimated using method of Wajid et al [12]. Briefly, 0.5 ml plasma from both groups was added in a tube along with 2.0 ml disodium hydrogen phosphate buffer (0.3 M) and 0.25 ml 5,5'-dithiobis-(2-nitrobenzoic acid) or DTNB (0.001 M) (Invitrogen Inc., USA). Mixture was incubated for 15 minutes and absorbance was measured at 412 nm.
Estimation of SOD Activity
SOD activity was assessed by the method of Wajid et al [12]. Briefly, 0.1 ml plasma was mixed with 1.2 ml sodium pyrophosphate buffer (52 mM, pH 8.3), 0.1 ml phenazine methosulphate (PMS) (186 µM) (Santa Cruz Biotechnology, USA), 0.3 ml nitroblue tetrazolium (NBT) (300 µM) (Invitrogen Inc., USA) and reaction was started by addition of 0.2 ml nicotinamide adenine dinucleotide (NADH) (750 µM) (Santa Cruz Biotechnology, USA). After incubation at 30°C for 90 seconds, reaction was stopped by the addition of 0.1 ml glacial acetic acid. Reaction mixture was stirred vigorously with 4.0 ml n-Butanol. Mixture was incubated for 10 minutes and centrifuged at 2000 rpm for 5 minutes. Upper butanol layer was taken and its absorbance was recorded at 560 nm.
Estimation of Catalase Activity
Activity of catalase was monitored by using method described by Wajid et al [12]. 0.1 ml plasma was taken and mixed with 1.0 ml phosphate buffer (10 mM, pH 7.0) and 0.4 ml H2O2 (0.2 M) (Sigma Aldrich, USA). Reaction was stopped by adding 2.0 ml dichromate acetic acid reagent. Samples were incubated for 10 minutes in a boiling water bath, cooled and absorbance was measured at 530 nm.
Estimation of MDA Level
Level of MDA, a free radical species was evaluated by measuring thiobarbituric acid reactive substances via method of Wajid et al [12]. For this, 0.2 ml cell culture medium was added to 0.2 ml sodium dodecyl sulfate (SDS) (8.1%), 1.5 ml thiobarbituric acid (TBA) (0.8%), 1.5 ml acetic Acid (20%, pH 3.5) and volume was made up to 4.0 ml with distilled water and incubated at 90˚C for 60 minutes. After cooling, 1.0 ml distilled water, 5.0 ml n-butanol-pyridine mixture (15:1) was added and the mixture was shaken vigorously and centrifuged at 4000 g for 10 minutes. Upper n-butanol layer was taken and its absorbance was measured at 532 nm.
Statistical Analysis
All the trials were performed in triplicates. Statistical tests and graphical representations were performed using GraphPad Prism 5 software (GraphPad, San Diego, CA). Data is presented as mean ± standard deviation. Unpaired student T tests were performed for comparison between two group’s data. The statistical significance was set at P<0.05.
Results
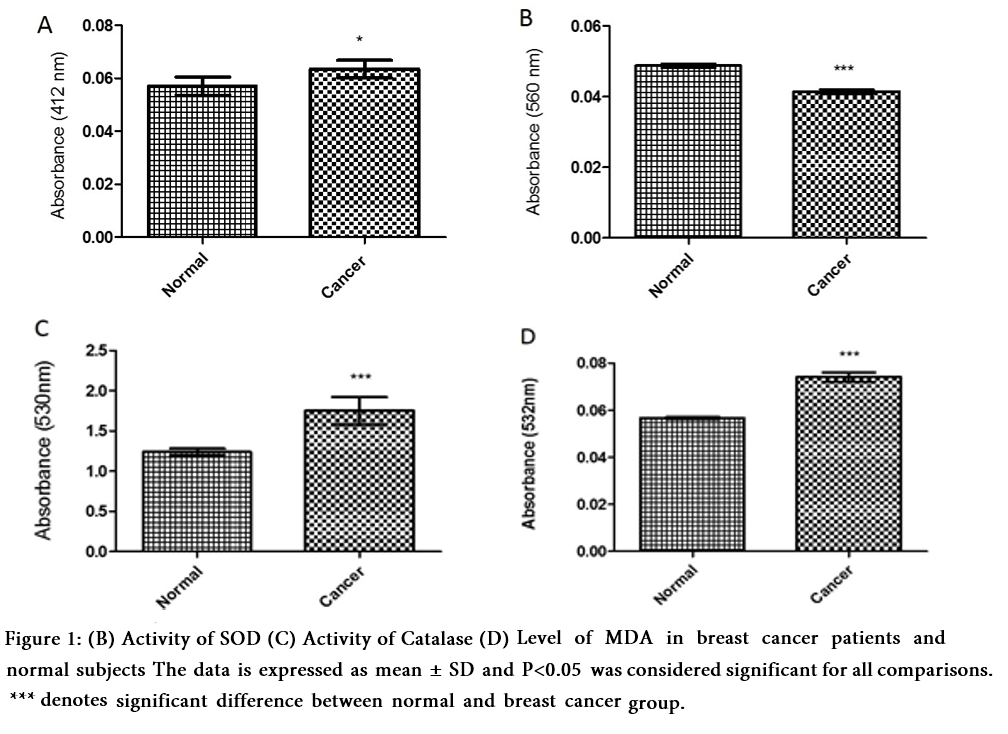
The current study was conducted to assess GSH and MDA levels and activities of SOD and catalase in plasma samples to evaluate oxidative stress in patients with breast cancer. It was observed that breast cancer patients have a significant increase in GSH levels in comparison to healthy individuals. Activity of SOD and catalase was significantly decreased in case of breast cancer, whereas a significant rise in MDA level was observed in breast cancer patients compared to normal individuals (Fig. 1).
Discussion
Breast cancer is one of the leading causes of deaths in females around the globe [1]. ROS are generated in cancer conditions [13] which promote DNA damage [5]. Present study describes the status of antioxidant enzymes as well as free radicals in breast cancer patients in Pakistani population.
GSH exhibit multidirectional role in cellular processes including cell growth, apoptosis, defense against oxidative stress as well as in chemo resistance and progression of cancer. A decrease in GSH level in general is an indication of oxidative stress but on other hand a rise in its level supports metastatic invasions of cancer [14]. In breast cancer patients, GSH was found to be elevated in some cases [15] while it was reduced in others [9,13,16]. A significantly increased level of GSH was observed in breast cancer patients (Fig. 1 A) in the present study. SOD is an important antioxidant enzyme and its activity was found to be reduced in breast cancer patients in our study (Fig. 1 B). This data is in accordance with the study of Negahdar et al [17] and Mahajan et al [9].
It has been reported that activity of catalase is significantly reduced in breast carcinoma [13]. Our study supports the previous data and catalase activity was found to be significantly reduced in breast cancer patients as compared to healthy controls (Fig. 1 C). The presence of MDA indicates lipid peroxidation which remains higher in breast cancer [13,18]. Our study confirms the data and MDA level was significantly higher in breast cancer patients (Fig. 1D).
Hence, t study demonstrated increased production of ROS and decreased activity of antioxidants indicating a significant oxidative stress in breast cancer patients of Pakistani population. It is suggested to clinicians to consider these parameters carefully before recommending any therapy for the patients.
Acknowledgements
Authors are thankful to The University of Lahore for financial support and INMOL Hospital for providing support in sample collection.
Conflict of interest
Authors declare no conflict of interest.
References
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA: A Cancer Journal for Clinicians, (2014); 64(1): 9-29.
- Benson JR, Jatoi I, Keisch M, Esteva FJ, Makris A, et al. Early breast cancer. The Lancet, (2009); 373(9673): 1463-1479.
- Cindrova-Davies T, Yung H-W, Johns J, Spasic-Boskovic O, Korolchuk S, et al. Oxidative stress, gene expression, and protein changes induced in the human placenta during labor. The American Journal of Pathology, (2007); 171(4): 1168-1179.
- Ruder EH, Hartman TJ, Goldman MB. Impact of oxidative stress on female fertility. Current Opinion in Obstetrics & Gynecology, (2009); 21(3): 219.
- Tas F, Hansel H, Belce A, Ilvan S, Argon A, et al. Oxidative stress in breast cancer. Medical Oncology, (2005); 22(1): 11-15.
- Rockenbach G, Di Pietro P, Ambrosi C, Boaventura B, Vieira F, et al. Dietary intake and oxidative stress in breast cancer: before and after treatments. Nutrición Hospitalaria, (2011); 26(4): 737-744.
- Tesarova P, Kalousová M, Trnková B, Soukupová J, Argalásová S, et al. Carbonyl and oxidative stress in patients with breast cancer–is there a relation to the stage of the disease? Neoplasma, (2006); 54(3): 219-224.
- Sotgia F, Martinez-Outschoorn UE, Lisanti MP. Mitochondrial oxidative stress drives tumor progression and metastasis: should we use antioxidants as a key component of cancer treatment and prevention? BMC Medicine, (2011); 9(1): 62.
- Mahajan M, Tiwari N, Sharma R, Kaur S, Singh N. Oxidative Stress and Its Relationship With Adenosine Deaminase Activity in Various Stages of Breast Cancer. Indian Journal of Clinical Biochemistry, (2013); 28(1): 51-54.
- Klaunig JE, Kamendulis LM, Hocevar BA. Oxidative stress and oxidative damage in carcinogenesis. Toxicologic pathology, (2010); 38(1): 96-109.
- Weydert CJ, Cullen JJ. Measurement of superoxide dismutase, catalase and glutathione peroxidase in cultured cells and tissue. Nature Protocols, (2010); 5(1): 51-66.
- Wajid N, Naseem R, Anwar SS, Awan SJ, Ali M, et al. The effect of gestational diabetes on proliferation capacity and viability of human umbilical cord-derived stromal cells. Cell and Tissue Banking, (2014); 1-9.
- Amin KA, Mohamed BM, El-Wakil MAM, Ibrahem SO. Impact of breast cancer and combination chemotherapy on oxidative stress, hepatic and cardiac markers. Journal of Breast Cancer, (2012); 15(3): 306-312.
- Traverso N, Ricciarelli R, Nitti M, Marengo B, Furfaro AL, et al. Role of glutathione in cancer progression and chemoresistance. Oxidative medicine and cellular longevity, (2013); 2013.
- Ghalia AHA, Fouad IM. Glutathione and its metabolizing enzymes in patients with different benign and malignant diseases. Clinical Biochemistry, (2000); 33(8): 657-662.
- Kumaraguruparan R, Subapriya R, Kabalimoorthy J, Nagini S. Antioxidant profile in the circulation of patients with fibroadenoma and adenocarcinoma of the breast. Clinical Biochemistry, (2002); 35(4): 275-279.
- Negahdar M, Djalali M, Abtahi H, Sadeghi M, Aghvami T, et al. Blood superoxide dismutase and catalase activities in women affected with breast cancer. Iranian Journal of Public Health, (2005); 34(3): 39-43.
- Guo C-H, Hsia S, Chen P-C. Distribution of selenium and oxidative stress in breast tumor-bearing mice. Nutrients, (2013); 5(2): 594-607.