

Short Communication:
Characterization of antibiotic resistant gene in Staphylococcus aureus isolated from surgical wounds
Aisha Nawaz1, Abdul Razzaq2*, Sadia Ijaz3, Aisha Nawaz4, Arfan Ali5, Afshan kaleem1
Adv. life sci., vol. 3, no. 3, pp. 83-88, May 2016
*- Corresponding Author: Abdul Razzaq, (Email: biolformanite@gmail.com)
Authors' Affiliation
2- Institute of molecular biology and biotechnology, The University of Lahore – Pakistan
3- Main Diagnostic Laboratory, Mayo Hospital Lahore – Pakistan
4- Life sciences department, University of Central Punjab, Lahore – Pakistan
5- Institute of molecular biology and biotechnology, The University of Lahore – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: In the field of surgery wound infections have been a problem. Staphylococcus aureus, Escherichia coli, Proteus species, Klebsiella species, Streptococcus species, Enterobacter species, Pseudomonas species and species of staphylococci are frequently isolated from wound. This study was carried out to determine the prevalence of different pathogens in surgical wounds and their antimicrobial susceptibility patterns.
Methods: Pus swabs from each patient was collected aseptically, and inoculated on culture media. Isolates were characterized, identified, and their antibiotic susceptibility patterns were determined using the Kirby-Bauer diffusion method.
Results: Out of 300 surgical wound specimens analyzed, 208 samples were positive culture among which Staphylococcus aureus was most frequent pathogen with 103 (49.51%). The other 33 (15.86%) isolates were Pseudomonas aeruginosa followed by 27 (12.98%) isolates of Klebsiella 25 (12.01%) isolates of Proteus and 20 (9.61%). isolates of E.coli respectively. The antibiotic susceptibility of Staphylococcus aureus was checked.
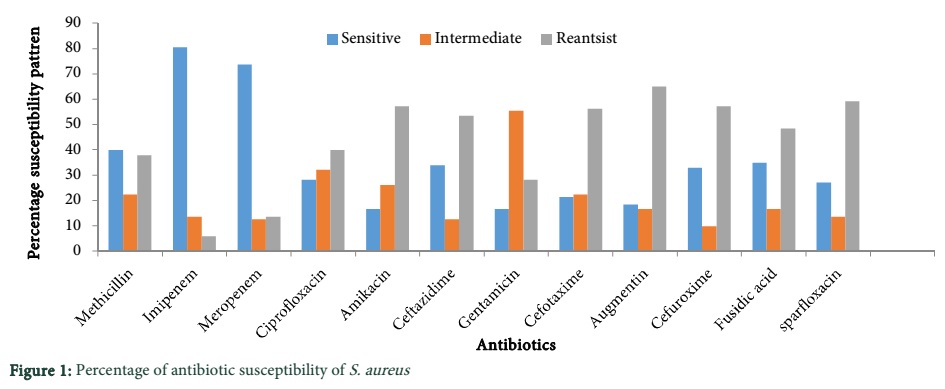
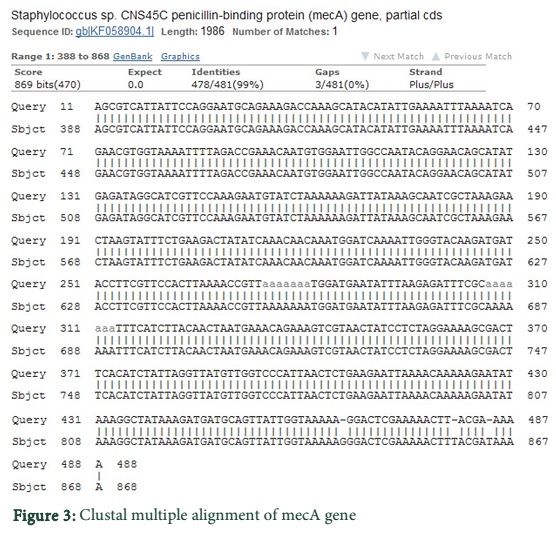
Conclusions: It was observed that 103 isolates of S. aureus were resistant to Augmentin 65.04% to Sparfloxacin 59.22% to Amikacin 57.28% to Cefuroxime 57.28% to cefotaxime 56.31% to Ceftazidime 53.39% to Fusidic acid 48.54% to Ciprofloxacin 39.80% to Methicillin 37.86% to Gentamicin 28.15% to Meropenem 13.59% to Imipenem 5.82%. PCR assay for the detection of clinically relevant antibiotic resistance gene of S. aureus was done. Fragments of mecA (encoding methicillin resistance) gene were amplified and commercially sequenced which showed insertion at three sites; 480-481: T, 484-485: T, 464-465: G.
Keywords: Antibiotic resistance genes, Staphylococcus aureus, surgical wounds, Imipenem
Introduction
A bodily injury caused by physical means with distraction of the continuity of structures is known as wound. Wounds consist of cuts, scratches scrapes and punctured skin. Wounds are a result of trauma or injury, surgical incisions, sutures, and stitches [1]. Microorganisms like viruses, prions, bacteria, and virods, and larger organisms such as macro parasites and fungi may cause infections in these wounds. Colonization of different pathogenic microbes within injured parts leads to interruption in cure of infected area. Immunity resistance of body as inadequate and do not have ability to manage with usual microbes development infected wounds be the outcome [2]. Exogenous and endogenous bacteria are the two major causes of surgical site post-operative wound infections and microorganisms are responsible for wound infections. One of the most frequent types of nosocomial infections in developing countries is surgical site infection (SSI). Interference with the skin barrier and the concentration of bacterial contamination of the wound at the time of surgery or afterward in wards during wound care is the reason of infection [3]. In the field of surgery wound infections have been a problem. Staphylococcus aureus, Escherichia coli, Proteus species, Klebsiella species, Streptococcus species, Enterobacter species, Pseudomonas species and species of staphylococci are frequently isolated from wound and within many developing countries ratio for nosocomial infections are particularly higher. A wound infection can arise up at any instance from two days after surgery until the wound has healed and an infection can occur several months after an operation very occasionally. Surgical wound infections are exceptional. Surgical wound infections are mostly limited to the skin, but can extend rarely to deeper tissues. The parts of the body that harbor lots of microorganisms are more prone towards infections after surgery [4]. In S. aureus antibiotic resistance gene is mecA gene which is responsible for most of the β-lactams antibiotics resistance including methicillin, its amplification and sequencing will provide insight to propose new synthetic drugs to manage treat acquired infections of S. aureus [5]. Detection of different clinically associated antibiotic resistant genes of S. aureus can be done with the help of multiplex polymerase chain reaction (PCR) assay. For the detection of antibiotic resistance profiles the multiplex PCR assay is a quick, easy and precise way and might be applied for the surveillance of increase in antibiotic resistance determinants in epidemiological studies and also for clinical diagnosis [6].
Methods
A total of 300 different samples of pus were collected from diverse wards of hospital and were evaluated for microbiological aspects as well as for antibiotic susceptibility pattern. Patients suffering from wound infections were provided with a questionnaire and all the concerned data was obtained which included gender, age, socio economic status, personal hygiene, wound type surgery source and previous history of disease. The data collected was used in this study after informed consent of the patients.
PCR amplification for mecA gene
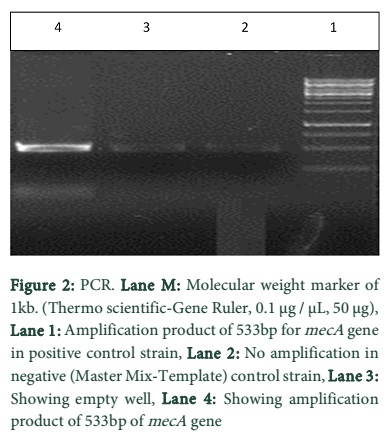
DNA was isolated from experimental samples through Sambrook’s protocol [7]. Bacterial genomic DNA (50 ng of genomic DNA) was added to PCR mixture consisting of 2 μL of concentrated reaction buffer (pH 8·3), with final concentrations of 2.5 μL each dNTP, 2.5 μL MgCl2, 0.75 μL of each mecA primer and 15.5 μL of water. This mixture was supplemented with 0.3 μL of Taq DNA polymerase. The final reaction volume for PCR was 25 μL. DNA amplification was carried out in an automated thermocycler [6]. Primers used for mecA gene amplification were 5′ -AAA ATC GAT GGT AAA GGT TGG C 3′ and 3′-AGT TCT GCA GTA CCG GAT TTG C 5′. After an initial denaturation step for 5 minutes at 95°C, 40 cycles of amplification were performed as follows: denaturation at 94°C for 30 seconds, annealing at 55°C for 30 seconds and DNA extension at 72°C for 90 seconds, followed by an additional cycle of 5 minutes at 72°C to complete partial polymerizations. Amplified products were analyzed using horizontal 1·2% agarose gel electrophoresis.
Results
Out of 300 samples of patients 208 were positive with growth of different isolates and 92 were negative. In the present study, different techniques for identification, isolation and biochemical characterization was employed to analyze the wound samples. The agents from the pus were isolated, identified analyzed and typed. Antibiogram of the isolated organisms were obtained by disc diffusion method.
The positive growth was shown by S. aureus, P. aeruginosa, Klebsiella, Proteus and E.coli. Of these 208 isolated organisms S. aureus were most frequent pathogen with 103 the next 33 isolates were of P. aeruginosa followed by 27 isolates of Klebsiella, 25 isolates of Proteus and 20 isolates of E.coli. Out of 208 positive cultures S. aureus was 49.51%, P. aeruginosa 15.86%, Klebsiella 12.98%, Proteus 12.01% and E.coli 9.61%.
Out of 103 isolates of S. aureus drug resistance pattern was observed and were found resistant to Augmentin 67 to Sparfloxacin 61 to Amikacin 59 to Cefuroxime 59 to Cefotaxime 58 to Ceftazidime 55 to Fusidic acid 50 to Ciprofloxacin 41 to Methicillin 39 to Gentamicin 29 to Meropenem 14 to Imipenem 06. It was observed that 103 isolates of S. aureus were resistant to Augmentin 65.04% to Sparfloxacin 59.22% to Amikacin 57.28% to Cefuroxime 57.28% to cefotaxime 56.31% to Ceftazidime 53.39% to Fusidic acid 48.54% to Ciprofloxacin 39.80% to Methicillin 37.86% to Gentamicin 28.15% to Meropenem 13.59% to Imipenem 5.82%. Methicillin was selected for this study because other lab data on other antibiotics for these organisms was not available.
Statistical analysis
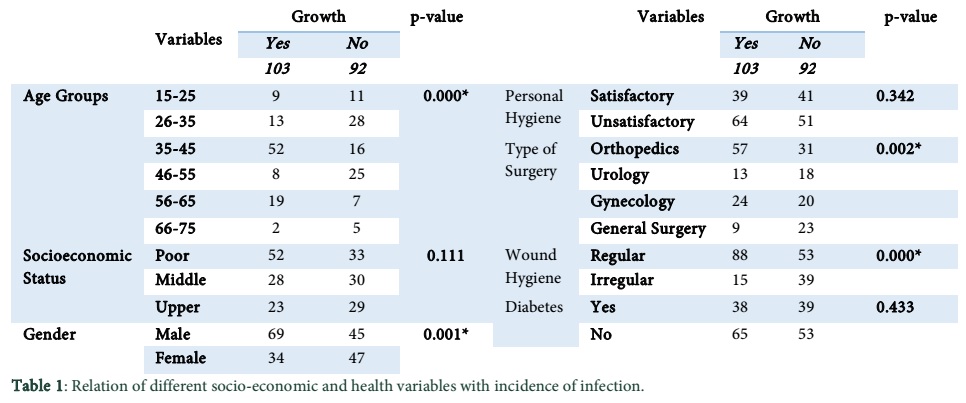
Age of patients was significantly associated with growth of S. aureus. i.e. (p-value=0.000) Among 103 patients in which S. aureus growth was detected 52 were in the group of 35-45 years respectively. Gender of patients, type of surgery and wound hygiene was significantly associated with growth of S. aureus.
Data and Tables
Discussion
This study was done to determine the division and passage rate of bacterial flora that might be a prospective risk of health within the facilities of hospital chiefly in the surgery units. Consequently, the facts present within this study will provide information of instant community health significance to practitioners in the choice of antimicrobial agents for the management of patients suffering from prophylaxis and surgical site infections. Bacteria isolated from the wound swabs of surgical site infections in this study were comparable to previous information by [4] and [8]. The bacterial isolates related to surgical infections were S. aureus, P. aeruginosa, Klebsiella species, Proteus species and Escherichia coli. This result was consistent with findings of [1,9,10]. Present study exposed that there were an increase percentage of males than females suffered from wound infection by S. aureus. this outcome was in accordance to the findings of [11].The rate of surgical infection was high in age group of 36-45 years with 50.48%.This is attributable to the information that the age range 36-45 years is thought to be energetic age group and these findings was near consistent with findings of [12]. Incidence of surgical wound infection with same age group was also reported [13]. It was observed that the rate of infection was very high in patients of poor economic status with 59.22% which indicated that they have reduced competent immune response to infections. During present study it was observed that presence of diabetes was 36.89% within the patients of surgical wounds and they are at high risk of delayed wound healing. All patients of diabetes had surgical wound infection in our study and no diabetic patient was observed who did not has wound infection these outcomes were consistent with findings of [1s4]. In present study 37.86% methicillin resistant S. aureus was observed which was in agreement to findings of [15] and [16]. In recent years a considerable raise in figure of wound infections because of methicillin resistant S. aureus has been determined in several reports [17,18]. Regarding antibiotic resistance it was observed that sparfloxacin showed resistance with 59.22% to Amikacin 57.28% to Cefuroxime 57.28% to cefotaxime 56.31% to Ceftazidime 53.39% to fusidic acid 48.54% to Ciprofloxacin 39.80% to Methicillin 37.86% to Gentamicin 28.15% to Meropenem 13.59% to Imipenem 5.82% .These findings was in agreement with findings of [19-21].
In the present study mecA was detected by PCR technique in which its amplification was done for the confirmation of isolates of S. aureus who are methicillin resistant and it was attained by disc diffusion method. The recovery rate of mecA gene was less due to storage of methicillin resistant isolate of S. aureus at low temperature which leads to the loss of mecA gene as found by [22]. This outcome was useful and employed for the managing bacterial strains of methicillin resistant S. aureus. Determination of mecA gene through PCR is a fast and consistent one step procedure for MRSA cultures identification and can be directly employed to clinical isolates. In present work mecA gene was determined by PCR with the help of 530 base pair primer and it is comparable to other findings [23-25].
Surgical site infections are a major cause of morbidity of post-operative surgical patient and in spite of using broad spectrum antibiotics including potent anti-staphylococcal drugs for perioperative prophylaxis, S. aureus remained most common cause of SSI. MRSA comprises a significant percentage among these isolates. Infection with MRSA is becoming endemic in hospitals worldwide. It enters healthcare facilities through infected or colonized patients and health care workers. Several studies all over the world have established that the early detection of methicillin resistance is very essential in the prognosis of infections which are caused by S. aureus as many of these infections are life threatening.
References
- Anguzu J, Olila D. Drug sensitivity patterns of bacterial isolates from septic post-operative wounds in a regional referral hospital in Uganda. African Health Sciences, (2007); 7(3): 148-154.
- Baker CC, Thomas AN, Trunkey DD. The role of emergency room thoracotomy in trauma. The Journal of Trauma and Acute Care Surgery, (1980); 20(10): 848-855.
- Pryor KO, Fahey III TJ, Lien CA, Goldstein PA. Surgical site infection and the routine use of perioperative hyperoxia in a general surgical population. JAMA: the journal of the American Medical Association, (2004); 291(1): 79-87.
- Biadglegne F, Abera B, Alem A, Anagaw B. Bacterial isolates from wound infection and their antimicrobial susceptibility pattern in Felege Hiwot Referral Hospital, North West Ethiopia. Ethiopian Journal of Health Sciences, (2009); 19: 173-177.
- Bode LG, Kluytmans JA, Wertheim HF, Bogaers D, Vandenbroucke-Grauls CM, Roosendaal R, Troelstra A, Box AT, Voss A, van der Tweel I. Preventing surgical-site infections in nasal carriers of Staphylococcus aureus. New England Journal of Medicine, (2010); 362(1): 9-17.
- Strommenger B, Kettlitz C, Werner G, Witte W. Multiplex PCR assay for simultaneous detection of nine clinically relevant antibiotic resistance genes in Staphylococcus aureus. Journal of Clinical Microbiology, (2003); 41(9):4089-4094.
- Sambrook J, Fritsch EF, Maniatis T. Molecular cloning. 1989; vol. 2: Cold spring harbor laboratory press New York.
- Mulu W, Kibru G, Beyene G, Damtie M. Postoperative Nosocomial Infections and Antimicrobial Resistance Pattern of Bacteria Isolates among Patients Admitted at Felege Hiwot Referral Hospital, Bahirdar, Ethiopia. Ethiopian Journal of Health Sciences, (2012); 22(1): 7-18.
- Endalafer N, Gebre-Selassie S, Kotiso B (2011). Nosocomial bacterial infections in a tertiary hospital in Ethiopia. Journal of Infection Prevention, 12(1):38-43.
- Oguntibeju OO. The biochemical, physiological and therapeutic roles of ascorbic acid. African Journal of Biotechnology, (2008); 7(25): 4700-4705.
- Fakoor M, Pipelzadeh MH. A study on the healing effect of honey on infected open fracture wounds. Pakistan Journal of Medical Sciences, (2007); 23(3): 327.
- Horiuchi A, Nakayama Y, Kajiyama M, Fujii H, Tanaka N. Nasopharyngeal decolonization of methicillin-resistant Staphylococcus aureus can reduce PEG peristomal wound infection. The American Journal of Gastroenterology, (2006); 101(2): 274-277.
- Al Saimary IEA. Antibiogram and multidrug resistance patterns of Staphylococcus aureus (MDRSA) associated with post operative wound infections in Basrah–Iraq. Medical Journal of Islamic World Academy of Sciences, (2012); 20(2): 57-66.
- Schimmel J, Horsting P, De Kleuver M, Wonders G, van Limbeek J. Risk factors for deep surgical site infections after spinal fusion. European Spine Journal, (2010); 19(10): 1711-1719.
- Kesah C, Ben Redjeb S, Odugbemi T, Boye CB, Dosso M, et al. Prevalence of methicillin‐resistant Staphylococcus aureus in eight African hospitals and Malta. Clinical Microbiology and Infection, (2003); 9(2): 153-156.
- Vandenesch F, Naimi T, Enright MC, Lina G, Nimmo GR, et al. Community-acquired methicillin-resistant Staphylococcus aureus carrying Panton-Valentine leukocidin genes: worldwide emergence. Emerging Infectious Diseases, (2003); 9(8): 978.
- Braun R, Hassler D. Methicillin-resistant Staphylococcus aureus (MRSA) infections spread in USA. Deutsche medizinische Wochenschrift, (2003); 128(16):855.
- Charbonneau P, Parienti J-J, Thibon P, Ramakers M, Daubin C, et al. Fluoroquinolone use and methicillin-resistant Staphylococcus aureus isolation rates in hospitalized patients: a quasi experimental study. Clinical Infectious Diseases, (2006); 42(6): 778-784.
- Soltani M, Sheikhzadeh N, Ebrahimzadeh-Mousavi H, Zargar A. Effects of Zataria multiflora essential oil on innate immune responses of common carp (Cyprinus carpio). Journal of Fisheries and Aquatic Science, (2010); 5(3): 191-199.
- Mohankumar A, Selvi ST. Antibiotic Pattern of Methicillin Resistant Staphylococcus aureus Isolated from Chronic Wound of Fisherman Community. International Journal of Microbiological Research, (2012): 3(2): 109-116.
- Naimi TS, LeDell KH, Como-Sabetti K, Borchardt SM, Boxrud DJ. Comparison of community-and health care–associated methicillin-resistant Staphylococcus aureus infection. JAMA: the Journal of the American Medical Association, (2003); 290(22):2976-2984.
- Van Griethuysen A, Van Loo I, Van Belkum A, Vandenbroucke-Grauls C, et al. Loss of the mecA gene during storage of methicillin-resistant Staphylococcus aureus strains. Journal of clinical microbiology, (2005); 43(3): 1361-1365.
- Corso A, Soloaga R, Faccone D, Gagetti P, Corbella S, et al. Improvement of a latex agglutination test for the evaluation of oxacillin resistance in coagulase-negative staphylococci. Diagnostic Microbiology and Infectious Disease, (2004); 50(3): 223-225.
- Hojo S, Fujita J, Negayama K, Ohnishi T, Xu G, et al. DNA fingerprinting by arbitrarily primed polymerase chain reaction (AP-PCR) for methicillin-resistant Staphylococcus aureus. Kansenshogaku zasshi. The Journal of the Japanese Association for Infectious Diseases, (1995); 69(5): 506.
- Skov R, Smyth R, Clausen M, Larsen A, Frimodt-Møller N, Olsson-Liljequist B, Kahlmeter G. Evaluation of a cefoxitin 30 µg disc on Iso-Sensitest agar for detection of methicillin-resistant Staphylococcus aureus. Journal of Antimicrobial Chemotherapy, (2003); 52(2): 204-207.


