

Short Communication
Identification and Antimicrobial Susceptibility Profile of Bacterial Pathogens Isolated From Wound Infections in a Teaching Hospital, Peshawar, Pakistan
Ibrar Khan1*, Naveed Sarwar1, Bashir Ahmad1, Sadiq Azam1, Noor Rehman1,2
Adv. life sci., vol. 5, no. 1, pp. 08-12, November 2017
*- Corresponding Author: Ibrar Khan (Email: Ibrarkhan1984@upesh.edu.pk)
Authors' Affiliations
2- Microbiology Laboratory, Khyber Teaching Hospital, Peshawar, Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The resistance profile of bacteria causing wound infections may vary from time to time in a given geographical location. The key objective of this study was to determine the prevalent aerobic and or facultative anaerobic bacterial types and their antibiogram to commonly prescribed antibiotics.
Methods: Pus, drainage or wound swabs from various body parts of 200 patients were aseptically collected from Khyber Teaching Hospital (KTH) and processed by standard microbiological techniques for identification of bacterial isolates and later antimicrobial susceptibility profile was determined as per Clinical and Laboratory Standard Institute (CLSI) guidelines by using Kirby-Bauer method.
Results: Out of 200 clinical wound specimens processed, Staphylococcus aureus was the most common bacterial pathogen isolated (n=100, 50%), followed by Escherichia coli (n=45, 22.5%), Pseudomonas aeruginosa (n=35, 17.5%), Enterobacter species (n=14, 7%), Proteus species (n=5, 2.5%) and Morganella species (n=1, 0.5%). Staphylococcus aureus (n=100) showed highest resistance to amoxicillin (82%), followed by ofloxacin (80%), sparfloxacin (78%), ciprofloxacin (71%), levofloxacin (46%) and Gentamicin (34%). Out of 100 S. aureus isolates methicillin and vancomycin resistance was found to be in 1.5 and 2% of the isolates, respectively. Among Gram negative isolates (n=100) the vast majority were resistant to augmentin, followed by cephalosporins, quinolones and almost fairly susceptible to carbapenems, cefoperazone + sulbactam and aminoglycosides.
Conclusion: There is a need for judicious use of antibiotics in clinical setup. The periodic monitoring of bacterial pathogens and their susceptibility profile is very helpful in understanding the resistance phenotypes in a given area which ultimately help physicians in selecting suitable empirical therapy.
Key words: Staphylococcus aureus, Gram negative rods, Antibiotics
Introduction
The human skin is a primary defense organ that prevents infection by forming an effective barrier that keeps the underlying tissue intact [1]. Loss of skin integrity or wound formation exposes the subcutaneous tissue that provides a moist, nutritious environment, facilitating microbial colonization and proliferation. As wound colonization is poly microbial with, potentially pathogenic microorganisms, thus any wound is at some risk of getting infected [2]. In addition to the skin and soft tissue infections that occur mainly due to a break in the surface of the skin, wound infections can also occur as complications of surgery, trauma, bites or diseases that disrupt the skin. Considering that cutaneous barrier is disrupted by every incision on the skin, microbial contamination is, thus, unavoidable, despite the best preparation of the skin prior to an incision [3]. Further, even though a burn site is relatively sterile for the first 24 hours, wound colonization by Gram-negative bacteria is common afterwards [4]. Such infections are a major obstacle to healing and can negatively impact the patient’s quality of life and cure rate of the wounds. Infected wounds are generally odorous, hypersensitive and more painful, and result in greater patient discomfort [5].
The most common bacteria associated with wound infection include S. aureus and Pseudomonas aeruginosa, which together account for 20-40% of all nosocomial, post-surgery and burn infections. Other pathogens, such as Enterococci and Enteriobacteria have also been implicated, especially after abdominal surgery in immune-compromised patients [6]. Antibiotic resistance, with the aforementioned risks associated, makes wound infections a complicated problem. The major factors responsible for antimicrobial resistance include changes in microbial ecology, genetics and the non-selective use of antimicrobial agents. Medically relevant examples of antimicrobial resistance are; Methicillin Resistant S. aureus (MRSA), Vancomycin resistant Enterococci (VRE) and Multi-drugs resistant tuberculosis (MDR-TB) [7].
Given the need for rapidly and effectively treating wound infections, the current study aimed to identify pathogenic bacteria present in wound infections and determine their antimicrobial susceptibility pattern.
Methods
Study area, sample size and selection criteria
A prospective study during June-August 2014 was conducted at the Khyber Teaching Hospital (KTH) in Peshawar, Pakistan. A total of 200Pus, drainage or wound swabs were collected from infected wounds in patients who had either undergone surgery or from patients with burn or traumatic injuries. Samples were obtained from both outpatient and inpatients admitted to various wards of the hospital. The study objectives and research methods were explained to the patients and informed consent was obtained from all participants, prior to the sample collection, after taking proper approval from ethical committee.
Inclusion and exclusion criteria
All bacteria were isolated from the pus samples obtained from wounds that were either painful or with discharge, swelling and a foul smell. However, patients who had other known infections, such as parasitic or fungal infection, or on an antibiotic treatment, were excluded from the study.
Sampling procedure
All the specimens were aseptically collected using a sterile cotton swab and transported in Amies transport media to the microbiology laboratory. Care was taken to ensure that the samples were not contaminated with surrounding skin commensals. The swabs were subsequently analyzed at the Microbiology section of the Pathology Department of the hospital.
Isolation and identification of bacteria
The collected specimens were streaked on to sterile MacConkey and blood agar (Oxoid Ltd, Bashingstore, Hampire, UK) plates and incubated for 24-48 hours at 37°C. Preliminary identification of bacteria was performed based colony characteristics; Lactose fermenters and Non lactose fermenters on MacConkey agar, hemolysis on blood agar, changes in physical appearance in differential media and biochemical tests like catalase, coagulase, oxidase. Gram-positive Cocci (GPC) were identified based on Gram reaction, coagulase, catalase and DNase activity. Gram-negative bacilli (GNR) were identified using the citrate, urease, oxidase and Triple Sugar Iron (TSI) tests [8].
The following criteria were used for the identification of pure isolates of GPC and GNR. Gram positive Cocci with positive coagulase, catalase and DNase activity were identified as S. aureus while Cefoxitin disc was used to identify MRSA, as it is resistant to this antibiotic. Gram-negative bacilli with negative citrate, urease and oxidase activity but positive TSI activity with; yellow slope (acidic reaction) and yellow butt (acidic reaction) were identified as E. coli. Gram-negative bacilli that were citrate and oxidase positive, urease negative but with an alkaline TSI reaction (red slope and red butt) were identified as Pseudomonas species. Enterobacter species were identified as GNR that were citrate positive, urease and oxidase negative but with an acidic TSI reaction (yellow slope and yellow butt). Proteus species were identified as GNR that were citrate and urease positive but oxidase negative with an acidic TSI reaction (yellow slope and yellow butt), along with H2S production. Morganella species were identified as GNR that were urease positive, citrate and oxidase negative but an alkaline (red slope) and acidic (yellow butt) TSI reaction [8].
Antibiotic susceptibility testing
Antimicrobial susceptibility testing was performed by Kirby-Bauer disk diffusion technique according to criteria set by CLSI 2013, after identification of the isolates. Pure colonies of the test organism were suspended in a sterile nutrient broth and a uniform lawn was made on the surface of Mueller Hinton agar (MHA) plates. Antibiotic impregnated paper discs, with known antibiotic concentration, were then introduced on the MHA plates and incubated for 24 hours at 37°C. The diameter of the zone of inhibition around the impregnated discs was measured to the nearest millimeter, and this was used to classify the isolates as Susceptible, Intermediate or Resistant (SIR) based on standard criteria issued by the CLSI [8].
The antibiotics used on Gram positive bacteria were; amoxicillin (AMP), ofloxacin (OFX), sparfloxacin (SPX), ciprofloxacin(CIP), levofloxacin (LEV), gentamycin (CN), tygacil (TGC), linezolid (LZN), sulzone (SCF), Oxacillin (OX), vancomycin (VA), fusidic acid (FA), clarithromycin (CLR), erythromycin (E), cefoxintin (FOX), amikacin (AK), cefaclor (CEF) and cephradine (CE)while those used on Gram negative bacteria were; augmentin (AMC), OFX, SPX, CIP, CN, meronem (MEM), imipenem (IPM), SCF, ceftriaxone(CTX), ceftazidime (CAZ), cefoperazone (CFP), moxifloxacin (MXF), E, cefaxime (CFM), amikacin (AK), cefipime (CFP) and aztreonam (ATM).
Results
A total of 200 samples were collected from patients suspected of having wound infections. Out of the 200 patients included in this study, 118 (59%) were males and 82 (41%) were females (07-74 years).
Out of the 200 samples, 100(50%) samples were positive for S. aureus, 03 (1.5%) were positive for MRSA, 04 (2%) were positive for vancomycin resistant S. aureus, while 45 (22.5%) were positive for E.coli, 35 (17.5%) were positive for Pseudomonas spp, 14 (7%) were positive for Enterobacter spp., 05 (2.5%) were positive for Proteus species and only one sample (0.5%) was positive for Morganella.
A total of 18 antibiotics were selected and tested for resistance in Gram-positive bacteria. The sensitivity of these bacteria to the antibiotics used varied, depending on the species and majority of the isolates showed multi drug resistance (resistance to three or more classes of antibiotics). Isolates of S. aureus were resistant to amoxicillin (82%), Ofloxacin (80%), sparfloxacin (78%), ciprofloxacin (71%), levofloxacin (46%) and gentamycin (36%). All isolates were completely sensitive to tygacil and linezolid, and showed low resistance to sulzone (2%), Oxacillin (3%), vancomycin (4%), fusidic acid (5%), clarithromycin (7%), erythromycin (8%), cefoxintin (9%), amikacin (15%), cefaclor (15%) and cephradine (19%).
Similarly, 18 antibiotics were tested on Gram-negative bacteria and majority of the isolates showed multi drug resistance. E. coli isolates were resistant to erythromycin (88.8%), moxifloxacin (73.3%), cefaxime (73%), ceftazidime (66.6%), ofloxacin (62.2%), ciprofloxacin (57.7%), sparfloxacin (51.1%), aztreonam (44.4%), augmentin (37.7%) and cefipime (37.7%). All isolates were 100% sensitive to meronem, sulzone and imipenem and showed low resistance to amikacin (6.6%), gentamycin (22.2%) and ceftriaxone (31.1%). Isolates of P. aeruginosa showed resistance to cefaxime (70%), erythromycin (64.7%), augmentin (60%), ofloxacin (41%), moxifloxacin (37.1%), ciprofloxacin (37.1%), gentamycin (37.1%) and sparfloxacin (34.2%). All the isolates showed low resistance to meronem and imipenem (5%), sulzone (2.8%), cefoperazone and aztreonam (11.4%), cefipime (14.2%), ceftriaxone (20%), amikacin (22.8%) and ceftazidime (25%). Isolates of Enterobacter spp were resistant to cefoperazone (92.8%), erythromycin (92%), cefaxime and augmentin (85%), Ofloxacin, moxifloxacin and sparfloxacin (78%), ceftriaxone (71.1%), ceftazidime (71%), aztreonam (50%), amikacin (42.8%) and gentamycin (42%). All isolates of this specie were completely sensitive to meronem and imipenem and showed low resistance to sulzone (7.1%) and ciprofloxacin (14%). Isolates of Proteus spp were completely resistant (100%) to cefaxime, erythromycin, augmentin, ceftriaxone and ceftazidime and resistance to gentamycin and Cefepime was 80% while to aztreonam, it was 60%. All Proteus spp. isolates were completely sensitive to moxifloxacin, sulzone and amikacin and showed low resistance to ofloxacin, ciprofloxacin, meronem, imipenem, cefoperazone and sparfloxacin. The Morganella isolate was resistant to all antibiotics except aztreonam, amikacin and gentamycin.
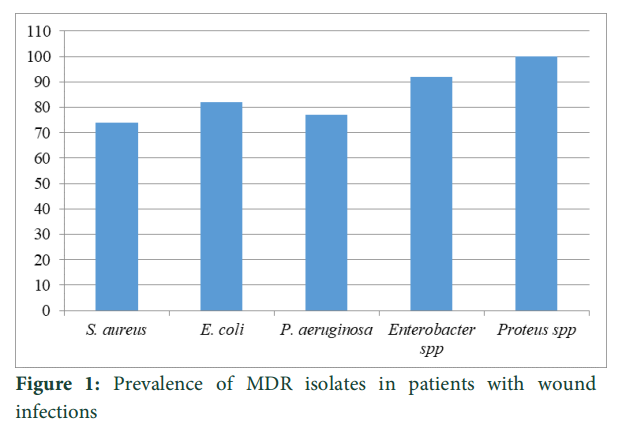
Multi- drug resistance (MDR) was found in both the Gram positive and Gram negative isolates with 74% of the Gram positive bacterial isolates being MDR. Similarly, the Gram-negative bacterial isolates were resistant to between two and seven classes of antimicrobial tested with 82% of the E.coliisolates,77.1% of Pseudomonas spp. Isolates, 92% of Enterobacter spp. isolates and 100% of Proteus spp. Isolates showing MDR pattern (Figure 1).
Figure
Discussion
This study aimed to ascertain the type and antibiotic resistance pattern of pathogenic bacteria present in wound infections among patients in the KTH, Peshawar. The incidence of wound infection was higher in males (59%) than in females (41%) which could be explained by the fact that men included in the study were involved in professions such as agriculture, construction, transportation and industry, making them more vulnerable to trauma and injury. S. aureus and E. coli were the most frequently isolated bacteria from the infected wounds and our data confirm similar findings in previous studies [9-11]. The high prevalence of S. aureus infection could be due to environmental contamination or due to like contamination of surgical instruments; thus when the natural skin barrier is broken or damaged, the bacteria easily find their way into the wounds.The overall resistance of the isolates to multiple antibiotics was 85%, and concurs with data in other reports from different parts of the world [11,12].
The susceptibility of S. aureus to eighteen antibiotics as determined by disc diffusion method, showed that S. aureus was highly resistant to a broad spectrum of antibiotics including AMC, OFX, SPX, CIP, LEV and CN but alsohighly sensitive to TGC,LZN, SCF, OX, VA,FA, CLR, E, FOX, AK, CEF and CE.
Compared to previous reports on antibiotic susceptibly and resistance pattern of S. aureus, the isolates obtained in our study showed reduced sensitivity to certain antibiotics such as: LEV (54% vs60.42%) [13], VA (96% vs 100%), AK (85% vs 100%) CIP (29% vs 96%), CN (66% vs 96%to 100%) [13], OFX (20% vs 70%) [14] and higher sensitivity to other antibiotics such as OX (97% vs.70.83%). The resistance of S. aureus to VA was found to be 2% and this incidence of VRSA is lower compared to another study from India [15].
Similar to S. aureus, we found that antibiotic susceptibility and resistance patterns of E. coli were different from those reported previously. Specifically, the E. coli isolates from our study showed reduced sensitivity to CIP (57% vs 62.07%), CAZ (33.4% vs 27.59%) [15], but increased sensitivity to AK (93.4% vs 71.42%), CN (77.8% vs 69.04%) and IPM (100% vs 96.42%) [14]. Analogous differences in the susceptibly pattern of P. aeruginosa isolates were also observed, with these bacteria showing higher resistance to CIP (62.9% vs 83.78%)[11], but higher sensitivity to MEM (95% vs 51.35%)[15], CAZ (75% vs 45.95%)[11], AK (77.2 vs 72.5%), ATM (88.6 vs 40%), CN (62.9% vs 41.25%) and IPM (95% vs 90%)[14].The Proteus spp. Isolates from our study have showed reduced sensitivity to CIP (80% vs 83%),CN (20% vs 74%)[13],AK (100% vs 73.33%), IPM (89% vs 100%) and CAZ (0 % vs 30%)[16] but were more resistant to CRO (100% vs 65%) compared to Proteus spp. isolates at the Jimma University Specialized Hospital, South-West Ethiopia [16].
Conflict of Interest
The authors declare no conflict of interest.
References
- Ndip RN, Malange Takang AE, Echakachi CM, Malongue A, Akoachere JF, et al. In-vitro antimicrobial activity of selected honeys on clinical isolates of Helicobacter pylori. African Health Sciences, (2007); 7(4): 228-232.
- Dai T, Huang YY, Sharma SK, Hashmi JT, Kurup DB, et al. Topical antimicrobials for burn wound infections. Recent Patents on Anti-Infective Drug Discovery, (2010); 5(2): 124-151.
- Cochran A, Morris SE, Edelman LS, Saffle JR. Systemic Candida infection in burn patients: a case-control study of management patterns and outcomes. Surgical Infections (Larchmt), (2002); 3(4): 367-374.
- Howard RJ. Host defense against infection–part 1. Current Problems in Surgery, (1980); 17(5): 267-316.
- Pruitt BA, Jr., McManus AT, Kim SH, Goodwin CW. Burn wound infections: current status. World Journal of Surgery, (1998); 22(2): 135-145.
- Kotz P, Fisher J, McCluskey P, Hartwell SD, Dharma H. Use of a new silver barrier dressing, ALLEVYN Ag in exuding chronic wounds. International Wound Journal, (2009); 6(3): 186-194.
- Al-Waili N, Salom K, Al-Ghamdi AA. Honey for wound healing, ulcers, and burns; data supporting its use in clinical practice. Scientific World Journal, (2011); 11766-787.
- Wkler Mathew A CFR, Bush Karen, Dudley Michael N, Etiopoule Georage , M HDJ. Clinical and laboratory standard institute. (2005); 10th ed.
- Zhanel GG, DeCorby M, Laing N, Weshnoweski B, Vashisht R, et al. Antimicrobial-resistant pathogens in intensive care units in Canada: results of the Canadian National Intensive Care Unit (CAN-ICU) study, 2005-2006. Antimicrobial Agents and Chemotherapy, (2008); 52(4): 1430-1437.
- Weber SG, Miller RR, Perencevich EN, Tolentino J, Meltzer D, et al. Prevalence of antimicrobial-resistant bacteria isolated from older versus younger hospitalized adults: results of a two-centre study. Journal of Antimicrobial Chemotherapy, (2009); 64(6): 1291-1298.
- Schmitz FJ, Fluit AC, Gondolf M, Beyrau R, Lindenlauf E, et al. The prevalence of aminoglycoside resistance and corresponding resistance genes in clinical isolates of staphylococci from 19 European hospitals. Journal of Antimicrobial Chemotherapy, (1999); 43(2): 253-259.
- Mulu A, Moges F, Tessema B, Kassu A. Pattern and multiple drug resistance of bacterial pathogens isolated from wound infection at University of Gondar Teaching Hospital, Northwest Ethiopia. Ethiopian Medical Journal, (2006); 44(2): 125-131.
- Goswami NN, Trivedi HR, Goswami AP, Patel TK, Tripathi CB. Antibiotic sensitivity profile of bacterial pathogens in postoperative wound infections at a tertiary care hospital in Gujarat, India. Journal of Pharmacology and Pharmacotherapeutics, (2011); 2(3): 158-164.
- Mama M, Abdissa A, Sewunet T. Antimicrobial susceptibility pattern of bacterial isolates from wound infection and their sensitivity to alternative topical agents at Jimma University Specialized Hospital, South-West Ethiopia. Annals of Clinical Microbiology and Antimicrobials, (2014); 1314.
- Bayram Y, Parlak M, Aypak C, Bayram I. Three-year review of bacteriological profile and antibiogram of burn wound isolates in Van, Turkey. International Journal of Medical Sciences (2013); 10(1): 19-23.
- Kranthi K RR, Manasa D, Ganapathi S. . A study on bacterial pathogens in wound infections at Ganni Subba Lakshmi Medical College. . International Journal of Health Sciences and Research (2013); 344-50.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0/


