

Full Length Research Article
Evaluation of Antibiotics Pattern of Extended Spectrum Beta-Lactamase Producing Multi-Drug Resistant Pseudomonas aeruginosa
Anees Muhammad1, Ihsan Ali2, Muhammad Owais1, Sadiq Noor Khan2, Irfan Qadir Afridi3, Nasir Ali1*
Adv. life sci., vol. 7, no. 3, pp. 146-150, May 2020
*- Corresponding Author: Nasir Ali (Email: nasirimbb@gmail.com)
Authors' Affiliations
2. Department of Medical Laboratory Technology, Faculty of Basic & Applied Sciences, The University of Haripur, KPK – Pakistan
3. Khyber Teaching Hospital, Medical Teaching Institution, Peshawar – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Pseudomonas aeruginosa (Ps. aeruginosa) is considered as an opportunistic pathogen and the leading cause of morbidity and mortality in immunocompromised individuals. Globally, approximately 10-15% of the nosocomial infections are caused by Ps. aeruginosa. The Ps. aeruginosa can acquire resistance against broad-spectrum antibiotics. According to recent studies increased mortality has been observed due to infection with extended-spectrum-beta-lactamase (ESBL) producing Ps. aeruginosa strains. This study was designed to determined antibiogram of ESBL producing multi-drug resistant Ps. aeruginosa in Khyber Pakhtunkhwa.
Methods: The clinical confirmed Ps. aeruginosa samples were collected according to the standard protocol, at Khyber Teaching Hospital (KTH), Peshawar. All collected samples were sub- cultured on appropriate culture media. After isolation and identification, the antibiotics susceptibility testing was performed. The detection of ESBL was carried out by the double-disc diffusion method. Carbapenemase-producing bacteria was confirmed by the modified Hodge test. Descriptive analysis was performed for statistical analysis of collected data.
Results: A total of one hundred and sixty-two (n=162) Ps. aeruginosa confirmed isolates were collected, in which 59.3% were male and 40.7% were from female patients. The percentages of ESBL and carbapenemase producing Ps. aeruginosa isolates were 5.5% and 23.5%, respectively. The multidrug resistance was observed against 27.2% isolates. Among tested antibiotics highest percentages of resistance was observed against ciprofloxacin (43%) and ceftazidime (39.5%).
Conclusion: We observed highest level of drug resistance in Ps. aeruginosa clinical isolates against tested antibiotics and majority of the isolates were Multi-drug resistant (MDR).
Keywords: Pseudomonas; Multi-Drug Resistant; Extended Spectrum Beta Lactamases; Antibiotics Susceptibility
Introduction![]()
Pseudomonas aeruginosa (Ps. aeruginosa) is a gram-negative, rod shaped, non-lactose fermenter and opportunistic pathogen. As an opportunistic pathogen it is considered as a leading cause of morbidity and mortality [1]. It causes both hospital and community-acquired infections [2]. Worldwide approximately 10-15% of the nosocomial infections are caused by Ps. aeruginosa [3]. Various virulence factors that contribute in its pathogenesis are endotoxins, exotoxins, ability to produce biofilm and different enzymes [4]. Usually, for the treatment of Ps. aeruginosa infections broad spectrum antibiotics such as carbapenems, extended-spectrum cephalosporin, anti-pseudomonal penicillin, and polymyxin B/colistin are used [5]. With the passage of time theses antibiotics acquired resistance due to over use or misuse of these antimicrobial agents [3]. Other factors that contribute in its increase resistance are production of beta-lactamase enzymes such as extended spectrum beta lactamases (ESBLs) and metallo-beta-lactamases (MBLs), target site modification, efflux pump and biofilm formation [6]. The Ps. aeruginosa acquire resistance by intrinsic as well as extrinsic mechanism [7]. As a result increase in morbidity and mortality have been observed from the infections of multi drug resistant (MDR) Ps. aeruginosa [8].
Globally, the prevalence of ESBL and carbapenemase producing Ps. aeruginosa have been reported [9]. The infections caused by MDR Ps. aeruginosa are difficult to treat. It is important to periodically check the antibiotic susceptibility patron of important clinical pathogens that will improve empirical treatment of clinical infections. Therefore, this study was conducted to evaluate the antibiotic susceptibility profile and phenotypic detection of ESBL and carbapenemase enzyme among clinical isolates of Ps. aeruginosa.
Methods![]()
This study was carried out in Khyber Teaching Hospital, Peshawar from February to September 2019. A total of one hundred and sixty-two (n=162) Ps. aeruginosa confirmed samples were collected. The Ps. aeruginosa strains were isolated from blood, bone marrow, fluids, pus, sputum, tissue, urine, and wound etc. The collected strains were sub-cultured on Blood agar and MacConkey agar (OXIDE England) and incubated overnight. The isolated strains were confirmed by standard microbiological procedures such as colony morphology, Gram staining, and biochemical testing.
The antibiotic susceptibility testing was carried out by Kirby-Bauer disc diffusion method as per CLSI, 2018 recommended guidelines [10]. The antibiotic discs and concentrations used were as follows; ciprofloxacin (5μg), gentamicin (10μg), imipenem (10μg), sulzone (100µg), meropenem (10μg), ceftazidime (30μg), tazocin (100µg), amikacin (30μg) and polymyxin B/colistin (10µg). The bacterial suspension was prepared in a sterile normal saline solution and compared with 0.5 McFarland’s turbidity standard. The tested antibiotic discs were placed on Muller Hinton agar (OXIDE England) plate and overnight incubated at 37C. The zone size interpretation was carried out as per CLSI guidelines 2018 [10]. The Ps. aeruginosa ATCC 27853 reference strain was used as quality control. The imipenem resistant strains were tested for carbapenemase production by modified Hodge test [11]. ESBL detection was carried out by double disc synergy method. The disc used were amoxicillin clavulanic acid, cefotaxime and ceftazidime [12].
All the data were analyzed through statistical package for social science software version 21. The descriptive analysis (percentage and number) were performed for collected data.
Results![]()
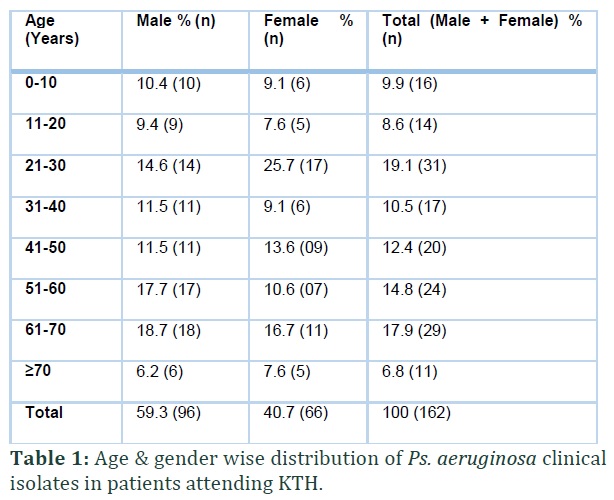
A total of one hundred and sixty-two (n=162) confirmed isolates of Ps. aeruginosa were collected in which 59.3% were from male and 40.7% were from female patients. In this study, age wise the patients were categorized into eight groups (Table no.1). Majority of the Ps. aeruginosa were recovered from the age grouped between 21-30 years.
The strains of Ps. aeruginosa were collected from nine different clinical samples (Shown in table no. 2), which includes; Urine 34.0% (n=55), Pus 30.2% (n=49), Sputum 24.1% (n=39), Wound 04.3% (n=07), Tissue 1.2% (n=2), Blood 2.5% (n=4), Bone marrow 1.9% (n=3), Fluid 1.2% (n=2) and CSF 0.6% (n=1). The highest number of specimens were collected from urine samples. All the isolates (n=162) were tested for the antibiogram against commonly prescribed antibiotics used in our locality and overall MDR has been observed as shown in table no 3.
Among the tested isolates 27.16% isolates were MDR (The isolates showed resistance to at least one antibiotic in three or more antimicrobial classes were classified as Multidrug resistant Ps. aeruginosa). Overall, 23.4% and 5.5% of the isolates were carbapenemase and ESBL producers respectively.
Figures & Tables



Discussion![]()
The Ps. aeruginosa is a non-fermenting multidrug resistant pathogen and the main cause of hospital and community-acquired infections [13]. The prevalence of resistant strains varies in different regions. In this study, the increase prevalence of Ps. aeruginosa infection was recorded in patients with age group of 21-30 years (19.1%), followed by 61-70 years (17.9%). A study conducted at Peshawar in 2017, revealed that age group 41-61 years have a high prevalence (36.6%) of Ps. aeruginosa infection, which are not in consistence with the current study [14]. The possible reason that caused difference could be origin of bacterial isolation.
A study conducted at Karachi, Pakistan, showed that infection caused by Ps. aeruginosa is more prevalent in females (64.71%) than in men (35.29%) [15]. Comparatively we observed low prevalence among females. In our study, the resistance against Ciprofloxacin, Gentamicin, Imipenem, Suzlon, Meropenem, Ceftazidime, Tazocin, Amikacin and Colistin were 43%, 35.2%, 32.7%, 32.7%, 33.3%, 39.5%, 35.2%, 34%, and 16%, respectively. A study conducted in 2009 at North West region of Pakistan, showed resistance against Amikacin (70%), Gentamicin (25%), and Ciprofloxacin (49%) [16]. In correlation to this study, the resistance against Amikacin is less. Another study carried out at Burn Center Islamabad in 2015, reported resistance to Tazocin (Piperacillin and Tazobactam) 80.55%, Imipenem (63.88%), Ciprofloxacin (44.44%), Polymyxin/colistin (36.11%), Suzlon (Cefoperazone and Sulbactam) 30.55%, ceftazidime (11.11%) and Amikacin (8.33%) [17]. We observed a low level of resistance against Amikacin and Ceftazidime. The reported resistance in another study were as follows; Ciprofloxacin (60%), Cefepime (57%), Levofloxacin (56%), Ceftazidime (53.9%), Amikacin (53%), Gentamicin (51%) and Tazobactum/Piperacillin 81(37.9%) [16].
The reported frequency of carbapenemase and ESBL producer from Lahore was 3.4% and 12.5% respectively, and all the strains were multidrug-resistant [18]. Our results of ESBL are in consistence with the previous report whereas a slight increase have been observed in case of carbapenemase. The frequency of MDR-ESBL and MDR-carbapenemase were almost similar with the results of the previous study. Ullah et.al. at Peshawar in 2014 reported the frequency of MDR 2.75% (n=102/3700) [19].
Conclusively, we identified Ps. aeruginosa clinical isolates from a tertiary care hospital. Majority of the studied isolates were ESBL producers and MDR. This increase prevalence of MDR will lead to treatment failure of infection caused these strains. This study recommends development of alternative treatment regimen. Furthermore, periodical surveillance and observation of resistance to antimicrobial agents at local and national level will be better for management of bacterial infections and for effective empirical therapy.
Acknowledgment
We are thankful to the Laboratory staff of Khyber Teaching Hospital, Peshawar for their support and help during sample collection and processing.
Funding
This study was funded by the HEC Startup Research Grant (Project no: 2418) titled "Isolation and molecular characterization of drug-resistant Pseudomonas aeruginosa strains from hospitalized patients”.
Conceived and designed the experiments: Anees Muhammad, Ihsan Ali, Muhammad Owais
Performed the experiments: Anees Muhammad, Sadiq Noor Khan, Irfan Qadir Afridi
Analyzed the data: Anees Muhammad, Muhammad Owais and Nasir Ali
Contributed materials/ analysis/ tools: Ihsan Ali, Sadiq Noor Khan and Nasir Ali
Wrote the paper: Ihsan Ali, Muhammad Owais, Irfan Qadir Afridi and Nasir Ali
Critical Review: Ihsan Ali, Sadiq Noor Khan, Irfan Qadir Afridi and Nasir Ali
All the authors declare that they have no competing interest that can negatively affect the current study.
References![]()
- Pang Z, Raudonis R, Glick BR, Lin T-J, Cheng Z. Antibiotic resistance in Pseudomonas aeruginosa: mechanisms and alternative therapeutic strategies. Biotechnology advances, (2019); 37(1): 177-192.
- Gellatly SL, Hancock RE. Pseudomonas aeruginosa: new insights into pathogenesis and host defenses. Pathogens and disease, (2013); 67(3): 159-173.
- Yayan J, Ghebremedhin B, Rasche K. Antibiotic resistance of Pseudomonas aeruginosa in pneumonia at a single university hospital center in Germany over a 10-year period. Plos one, (2015); 10(10): :e0139836.
- Sonbol FI, Khalil MAEF, Mohamed AB, Ali SS. Correlation between antibiotic resistance and virulence ofPseudomonas aeruginosa clinical isolates. Turkish journal of medical sciences, (2015); 45(3): 568-577.
- Bassetti M, Vena A, Croxatto A, Righi E, Guery B. How to manage Pseudomonas aeruginosa infections. Drugs in context, (2018); 72: 125-27.
- Lister PD, Wolter DJ, Hanson ND. Antibacterial-resistant Pseudomonas aeruginosa: clinical impact and complex regulation of chromosomally encoded resistance mechanisms. Clinical microbiology reviews, (2009); 22(4): 582-610.
- Dash M, Padhi S, Narasimham MV, Pattnaik S. Antimicrobial resistance pattern of Pseudomonas aeruginosa isolated from various clinical samples in a tertiary care hospital, South Odisha, India. Saudi Journal for Health Sciences, (2014); 3(1): 15.
- Ali Z, Mumtaz N, Naz SA, Jabeen N, Shafique M. Multi-drug resistant Pseudomonas aeruginosa: a threat of nosocomial infections in tertiary care hospitals. JPMA, (2015); 65(12): 12-16.
- Chen Z, Niu H, Chen G, Li M, Li M, et al. Prevalence of ESBLs-producing Pseudomonas aeruginosa isolates from different wards in a Chinese teaching hospital. International journal of clinical and experimental medicine, (2015); 8(10): 19400.
- Institute CaLS. Performance Standards for Antimicrobial Susceptibility Testing. CLSI, (2018); M100, 28th ed.
- Amjad A, Mirza IA, Abbasi S, Farwa U, Malik N, et al. Modified Hodge test: A simple and effective test for detection of carbapenemase production. Iranian journal of microbiology, (2011); 3(4): 189-193.
- Laudy AE, Rog P, Smolińska-Król K, Ćmiel M, Słoczyńska A, et al. Prevalence of ESBL-producing Pseudomonas aeruginosa isolates in Warsaw, Poland, detected by various phenotypic and genotypic methods. PloS one, (2017); 12(6): e0180121
- Senthamarai S. Resistance pattern of Pseudomonas aeruginosa in a tertiary care hospital of Kanchipuram, Tamilnadu, India. Journal of clinical and diagnostic research: JCDR, (2014); 8(5): DC30.
- Samad A, Ahmed T, Rahim A, Khalil A, Ali I. Antimicrobial susceptibility patterns of clinical isolates of Pseudomonas aeruginosa isolated from patients of respiratory tract infections in a Tertiary Care Hospital, Peshawar. Pakistan journal of medical sciences, (2017); 33(3): 670-674.
- Shah DA, Wasim S, Abdullah FE. Antibiotic resistance pattern of Pseudomonas aeruginosa isolated from urine samples of Urinary Tract Infections patients in Karachi, Pakistan. Pakistan journal of medical sciences, (2015); 31(2): 341-345.
- Ullah F, Malik SA, Ahmed J. Antimicrobial susceptibility and ESBL prevalence in Pseudomonas aeruginosa isolated from burn patients in the North West of Pakistan. Burns, (2009); 35(7): 1020-1025.
- Saaiq M, Ahmad S, Zaib MS. Burn wound infections and antibiotic susceptibility patterns at Pakistan Institute of Medical Sciences, Islamabad, Pakistan. World journal of plastic surgery, (2015); 4(1): 9-15.
- Aneela S, Abrar S, Saeed M, Hussain S, Hannan A, et al. Distribution of Extended-spectrum β-lactamase and Metallo-β-lactamase-producing Pseudomonas aeruginosa in Tertiary Care Hospitals of Lahore, Pakistan. Journal of Islamabad Medical & Dental College, (2019); 8(1): 23-28.
- Ullah W, Qasim M, Rahman H, Bari F, Khan S, et al. Multi drug resistant Pseudomonas aeruginosa: Pathogen burden and associated antibiogram in a tertiary care hospital of Pakistan. Microbial pathogenesis, (2016); 97: 209-212.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


