

Full Length Research Article
Study on significant changes in calcium, phosphorus and thyroid hormones level in hypothyroidism patients
Nida Zahra1, Ahmad Ali2, Saima Kousar3, Arif Malik1, Ahmad Zaheer1, Imran Riaz Malik1,4*
Adv. life sci., vol. 8, no. 1, pp. 85-88, November 2020
*- Corresponding Author: Imran Riaz Malik (Email: imran.riaz@uos.edu.pk)
Authors' Affiliations
2. National Institute for Genomics and Advanced Biotechnology (NIGAB), National Agricultural Research Centre (NARC), Islamabad – Pakistan
3. Department of Psychology, University of Sargodha, University Road, Sargodha – Pakistan
4. Department of Biotechnology, University of Sargodha, University Road, Sargodha – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Thyroid hormones have a vital role in metabolism of lipids, cholesterol etc. They also have an important role in phosphorous and calcium homeostasis by their direct effect on bone turnover. The objective of present study was to find the significant differences of T3, T4, TSH, lipid profile (HDL, LDL, vLDL, TG, Cholesterol), electrolytes and minerals (sodium, potassium, chloride, phosphorus, calcium) between control group and hypothyroidism patients.
Methods: Blood samples were collected from 72 patients and 12 control after their consent. Serum was used to determine biochemical parameters using standard protocol. Data obtained were statistically analyzed using “t” student test.
Results: The level of TSH was significantly higher in female and male hypothyroidism patients (p < 0.01) as compared to control and it was inversely related to the level of T3 and T4. Patients with hypothyroidism have increased level of LFTs profile especially cholesterol and Triglycerides levels both in males and females. In hypothyroidism, the level of glomerulus filtrate rate decrease especially sodium level but thyroid hormonal disturbance does not affect serum electrolyte level. The serum phosphorus and calcium levels change significantly in thyroid disorder.
Conclusion: Hypothyroidism is associated with increased TSH level and decreased T3 and T4 levels but does not appear to be associated with abnormalities in lipid profile. The serum phosphorus and calcium levels change significantly in thyroid disorder, Treatments of its primary causes should be given and if it is possible minerals can be added to avoid further bone complications.
Keywords: Hypothyroid; T3; T4, TSH; Lipid profile; Mineral
Introduction![]()
Thyroid disorders prevail strongly in the South Asian community mainly due to iodine deficiency and goitrogen consumption. In Pakistan male thyroid disorders are more common than female [1]. Hypothyroidism results from beneath secretion of internal secretion from the endocrine. It’s 5-10 times a lot of common in females as compared to males [2]. The clinical presentation of glandular disease could vary from well to, rarely, with multisystem organ failure resulting in hypothyroidism coma [3]. Determining the precise incidence and prevalence rates for Hashimoto’s rubor has been tough as a result of variable expression of this sickness. Some studies estimate that the present prevalence rate within the United States ranges between 0.3%-1.2% [4]. Primary glandular disorder is indicated once hormone level is high >10mU/L with diminished T3 and T4 levels. Secondary glandular disorder is diagnosed once hormone level is low <0.4 mIU/L with diminished T3 and T4 levels whereas the diagnosis of subclinical glandular disorder is especially supported with increased hormone level between (4.5-10mU/L) with T4 and T3 inside the [5]. Lipoproteins profile is another fact affected in hypothyroidism [6]. Thyroid hormones play an important role in homeostasis of calcium and phosphorus levels by their direct action on bone turnover [7]. Study carried out by Suneel et and found that serum levels of calcium were significantly decreased in patients with hypothyroid (p<0.001) and phosphorus levels were significantly increased as compared to control [8]. Study carried out by Christopher Schwarza et al., and found that level of phosphate was higher with elevated TSH in patients as compared to control TSH. The level of serum calcium was significantly lower with high TSH than with control TSH (p<0.01). The level of calcium and phosphate was significantly correlate with TSH as p<0.0 [9].
Serum HDL were significantly lower in patients as compared to control as p<001. It was found that level of LDL, HDL, VLDL, LDL, triglycerides was significantly higher as compared to control [10]. Patients with clinical or unconcealed glandular disorder exhibit reduced free T4 estimates and inflated thyroid-stimulating hormone levels [11]. Varied morphological and physiological changes of the thyroid throughout the method of aging square measure well-known [12]. The objective of this study was to find the Pleiotropic effects of hypothyroidism and level of T3, T4, TSH, lipid profile, electrolytes and minerals in human serum of patients as compared to control group.
Methods![]()
Samples Collection: Blood samples were collected from 72 in vacutainer from patients and 12 control samples after their consent. Serum samples were used to determine the different biochemical parameters.
Determination of T3, T4 and TSH: Radioimmunoassay were carried out for the determination of T3 and T4 (IM1699 T3 RIA kit) and TSH (IM1699 TSH RIA kit) in human serum.
Biochemical analysis: A semi-automated clinical analyzer was used to estimate the biochemical parameters from serum containing HDL, LDL, TG, vLDL and cholesterol and results were compared between patients and in control. Its level was estimated using biochemical analyzer (Microlab 300). The concentration of Sodium, Calcium, and Potassium were also determined using standard methods.
Statistical Analysis: The data obtained from this study were analyzed by using Student “t” test to find out statistically significant differences between different variables.
Results![]()
In patients with hypothyroidism, there is an inverse relation between T3, T4 and TSH. The study compromised 84 subjects within the age limit of 10 to 80. Among 84 subjects, there were 45 females and 39 males. Statistical analysis was carried out using the SPSS software. The results were reported as mean ± S.D. student’s t-test was used to determine whether differences between means were significant.
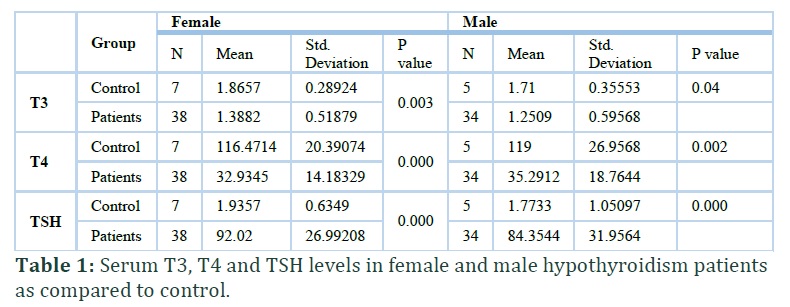
Comparison of T3, T4 and TSH in female patients with hypothyroidism and control: The results of the study showed that the mean values of T3 (1.3882± 0.51879 mIU/L) and T4 (32.9345±14.18329 mIU/L) decreases in female patients with hypothyroidism as compared to control T3 (1.8657±0.28924 mIU/L), control T4 (116.4714±20.39074 mIU/L), but the level of TSH increases as compared to control samples (92.02± 26.99208 VS 1.9357±0.6349) respectively (Table 1).
The mean values of T3 (1.2509± 0.59568 mIU/L) and T4 (35.2912±18.7644 mIU/L) decreases in male patients with hypothyroidism as compared to control T3 (1.71±0.35553 mIU/L) and control T4 (119 ±26.9568 mIU/L), but the level of TSH increases in patients samples as compared to control samples (84.3544 ± 31.9564 VS 1.7733±1.05097) as presented in Table 1.
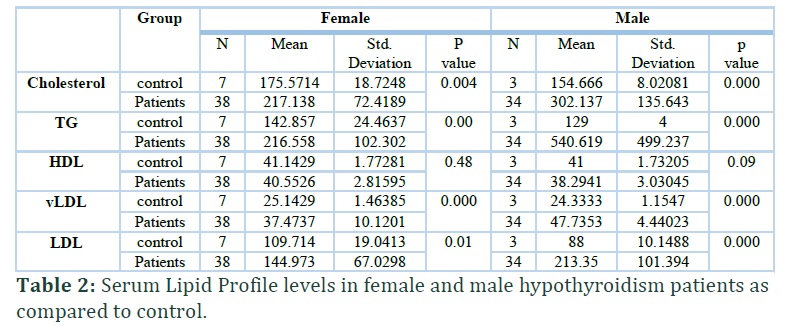
Serum Lipid Profile levels in female and male hypothyroidism patients as compared to control: Full serum lipid profile tests was conducted on 72 hypothyroidism patients. Table 2 shows that Patients with hypothyroidism have statistically increased level of LFTs profile especially cholesterol, Triglycerides levels, vLDL and HDL both in males and females except HDL which was statistically non-significant.
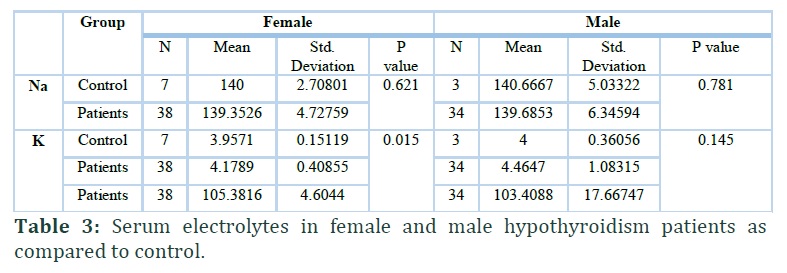
Serum Electrolytes in female and male hypothyroidism patients as compared to control: Patients with hypothyroidism has decreased sodium level of 139.3526 ± 4.72759 in females and 139.6853 ± 6.34594 in males as compared to control samples. The level of Potassium are also statistically significant at P<0.05 in female but results were non-significant in male when compared to control (Table 3).
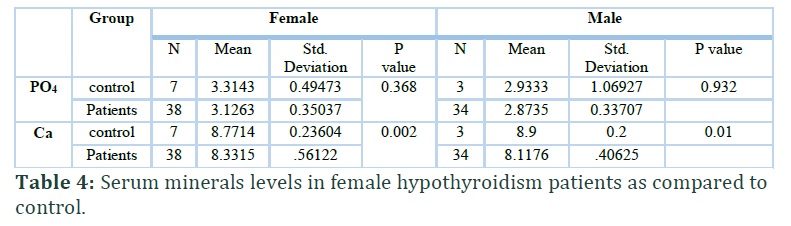
Serum minerals levels in female and male hypothyroidism patients as compared to control: Level of calcium and phosphorus were determined in the patients with hypothyroidism. The level of calcium decreases in female hypothyroid patients (3.1263± 0.56122) as compared to control (8.7714±0.23604) but the level of phosphorus (8.3316±0.35037) in female patients with hypothyroidism was increased than the control (3.3143± 0.49473) (Table 4). The same trends were observed in the male when calcium and phosphorus levels were determined in hypothyroidism patients. Results were statistically significant at p< 0.01.
Figures & Tables
Discussion![]()
The thyroid is amongst glands that store and release hormone into blood. Thyroid hormones then travel and affect the body cells. It is influenced by biochemical and other factors including sex, fruit, diet etc. of the person. During this study, different biochemical parameters were determined in order to find statistically differences between hypothyroidism patient and control group.
Result of thyroid hormone showed that decreased in the mean values of T3 and T4 whereas increased in TSH when compared female patients with control group. It was supported by the study as carried out by Mohamed in which the same results were observed that significant increased TSH levels (p=0.046) in patients while there was significant decrease in T3 (p=0.040) and T4 (0.029) levels when compared with Control group [13].
The level of T3 and T4 also decreased whereas increased in level of TSH in male patients with hypothyroidism as compared to control level of T3, T4 and TSH. Our findings are in strong agreement with the previous study carried out by Chuang in 1998 that TSH is inversely correlated with T3 and T4 levels hypothyroidism [14]. Serum TSH levels in patients (3.33 ± 0.78) were significantly higher (p < 0.001) as compared to control group (2.30 ± 0.91) and significantly lower levels of T4 (p < 0.001) in the patients of metabolic syndrome (117.45) than in controls [15].
Patients with hypothyroidism have statistically increased level of LFTs profile especially cholesteol, Triglycerides levels, vLDL and HDL both in males and females except HDL which was statistially non-significant. According to Gutch, the serum HDL was significantly lower (p < 0.001) in cases (41.28 ± 8.81) as compared to controls (54.00 ± 6.31). The serum LDL, VLDL, triglyceride levels and total cholesterol were significantly higher (p < 0.001) as compared to controls [10] and our study supported this.
Patients with hypothyroidism has decresead sodium level of 139.3526 ± 4.72759 in females and 139.6853 ± 6.34594 in males as compared to control samples which are in agreement with finding described by Hassan that the level of sodium was significantly decrease in hypothyroid patients as compared to control group [16].
Our Results shows that Potassium are statistically significant at P<0.05 in female but results were non-significant in male when compared to control. The level of electrolytes including potassium, sodium and chloride were reduced in hypothyroidism as compared to controls.
Level of calcium and Phophorus were determined in the patients with hypohyroidism. The level of calcium decreases in female hypothyroid patients but the level of phosphorus was increased than the control. Our outcomes are in agreement with the past examination directed by Shivaleela that the mean serum calcium levels were fundamentally lower in hypothyroidism patients (9.14 ± 0.51mg/dl, p<0.01) when contrasted with controls (9.41 ± 0.45mg/dl) 17]. The finding proposes that there is critical changes in the degrees of serum calcium and phosphorus in thyroid disorder that is significant reason for secondary osteoporosis and can be utilized as an index of bone desorption.
Hypothyroidism is associated with increased TSH level and decreased T3 and T4 levels but does not appear to be associated with abnormalities in lipid profile. The serum calcium and phosphorus levels are significantly altered in thyroid disorder, Treatments of primary cause and if necessary supplementation of minerals should be done in order to prevent further bone complications.
Author Contributions
All authors contributed equally in designing, conducting, compiling and drafting of this study.
It is declare by the authors that they have no conflict of interest about the research paper or any of its part.
References![]()
- Malik IR, Raza UA, Yasin M, Zaheer A, Malik A, Alam R. Study of oxidative stress parameters in patientns with hyperthyroidis. Electronic Journal of Biology, (2018); 14(4): 102-105.
- Becker DV, Bigos ST, Gaitan E. Optimal use of blood tests for assessment of thyroid function. Thyroid, (1993); 3: 353-354.
- Bensenor IM, Olmos RD, Lotufo PA. Hypothyroidism in the elderly: diagnosis and management. Clinical Interventions in Aging, (2012); 7: 97-111.
- Cappola R, Ladenson PW. Hypothyroidism and atherosclerosis. The Journal of Clinical Endocrinology and Metabolism, (2003); 6(88); 2438-2444.
- Chuang CC, Wang ST, Wang PW, Yu ML. Prevalence study of thyroid dysfunction in the elderly of Taiwan. Gerontology, 1998; 44(3);162-167.
- Cooper DS. Clinical Practice: Subclinical Hypothyroidism. The New England Journal of Medicine, (2001); 345(4); 260-265.
- Ashmaik AS, Gabra HM, Elzein AO, Shrif NEMA, Hassan EE. Asian Journal of Biomedical and Pharaceutical Sciences, (2013); 3(25): 21-26.
- Suneel B, Nagendra DR, Apama RR, Balalkrishna D, Naidu JN. Mineral Status I n Thyroid ( Hypo & Hyper). International Journal of Appliedd Biology and Pharmaceutical Technology, (2011); 2(4): 424-429.
- Schwarza C, Leichtle AB, Spiros A, George MF, Heins F, Aritmenis K, Gregor L. Thyroid function and serum electrolytes. Swiss Medical Weekly, (2012); 13669-142.
- Gutch M, Rungta S, Kumar S, Agarwal A, Bhattacharya A, Razi SM. Thyroid functions and serum lipid profile in metabolic syndrome. Biomedical journal, (2017); 40(3), 147-153.
- Hassan SH, Ali A, Ali JK. Assessment Levels of Some Electrolytes in Hypothyroidism Patients. International Journal of Pure and Applied Bioscience, (2019); 7(2); 10-14.
- Krishna MCS, Kumara HDS, Vishwanath HL. Study on the Electrolytes and Hypothyroidism – A Case Control Study. Biochemistry: an Indian journal, (2018); 12(2):131-134.
- Mohamed RJ. Relationship Between Disorder of Thyroid Gland and the levels of T3, T4 and TSH Hormones. Journal of Kerbala University, (2016); 14(2), 16-23.
- Shivaleela MB, Poornima RT, Jayaprakash Murthy DS. Serum calcium and phosphorous levels in thyroid dysfunction. Indian Journal of Fundamental and Applied Life Science, (2012); 2(2); 179-83.
- Staii A, Mirocha S, Todorova-Koteva K, Glinberg S, Jaume JC. Hashimoto thyroiditis is more frequent than expected when diagnosed by cytology which uncovers a pre-clinical state. Thyroid research, (2010); 3(1): 11
- Surks MI, Ortiz E, Daniels GH, Sawin CT, Cobin RH. Al Subclinical thyroid disease, scientific review and guidelines for diagnosis and management. The Journal of the American Medical Association, (2004); 291: 228-238.
- Vanderpump MP, Turnbridge WM. Epidemiology and prevention of clinical and subclinical hypothyroidism. Thyroid, (2002); 12: 839-47.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


