

Full Length Research Article
Public awareness of the coronary artery disease and its risk factors in the population of Hail region, Saudi Arabia: a cross-sectional study
S.M.A.Shahid1*, Tarig A.N Ginawi1, Mohd Adnan Kausar1, Mohammad Kuddus1, Fahaad S.H. Alenazi2 , Ahmed Hameed Alreshidi3 , Jaser Sultan Alshamari3, Dhari Abdulkarim Alquwaiay3, Wael Saleh Alanazi3, Abdulaziz Muflih Alghaithi3, Rian Mohamed Bnyan Al Amri3, Saleh Ali Saleh Alsanea3, Mohammed Rubayyi Alruwaytie3, Khalil Ibrahim Alanazi3, Hussam Salem Alshammari3, Mohd Saeed4
Adv. life sci., vol. 8, no. 1, pp. 89-92, November 2020
*- Corresponding Author: S.M.A.Shahid (Email: sm.shahid@uoh.edu.sa)
Authors' Affiliations
2. Department of Pharmacology, College of Medicine, University of Hail, P.O. Box 2440 – Saudi Arabia
3. Medical Student, College of Medicine, University of Hail, P.O. Box 2440 – Saudi Arabia
4. Department of Biology, College of Sciences, University of Hail, P.O. Box 2440 – Saudi Arabia
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Coronary Artery Disease (CAD) is a severe cardiovascular complication prevalent in the Kingdom of Saudi Arabia. The risk factors of this disease are so high that it became one of the major causes of mortality among middle-aged individuals. This study aimed to investigate the degree of awareness about risk factors for CAD among the Hail region population.
Methods: The study was carried out in the Hail region, Saudi Arabia, from April 2020 to May 2020. Data collected from five hundred and thirty-seven participants participated through an online survey. The process of selection of participants was through volunteer testing and an online review poll that was disseminated to them to complete. No limitations on age or sex were applied to the surveys.
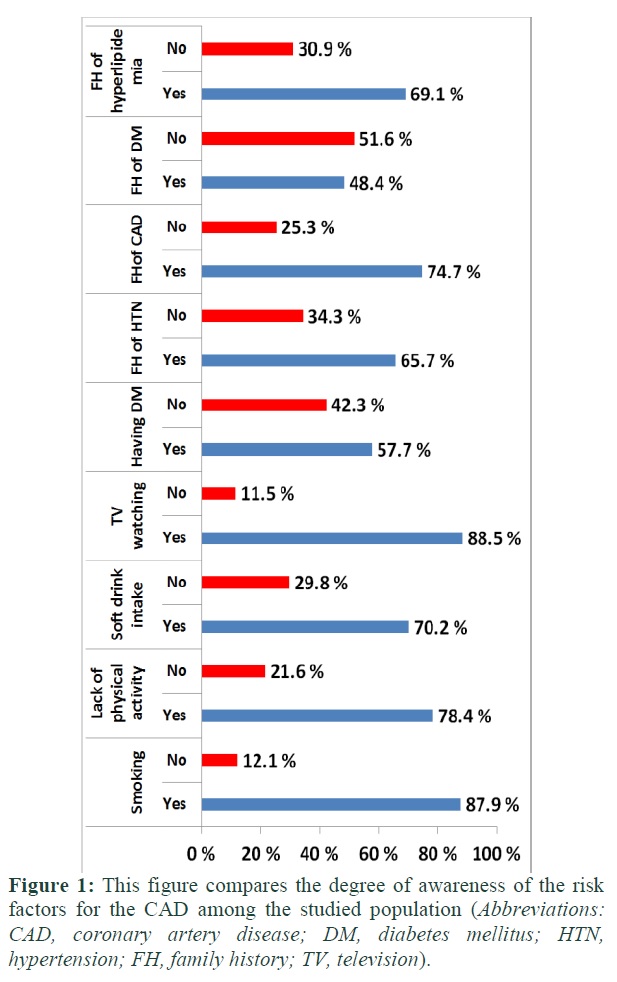
Results: Awareness of TV watching (88.5%), smoking (87.9%), lack of physical activities (78.4%) and family history of CAD (74.7%) as the leading cause of CAD has a notable higher percentage among the studied population whereas the family history of diabetes mellitus (51.6%), having diabetes mellitus (57.7%), family history of hypertension (65.7%) and family history of hyperlipidemia (69.1%) have the lowest percentages. Regarding the gender, the male participants have the poorest awareness degrees about risk factors for the CAD.
Conclusion: The study revealed that the family history of hyperlipidemia, Family history of DM, having DM and family history of hypertension have the poorest degrees of awareness of the risk factors for CAD among the studied population.
Keywords: Coronary artery disease; Risk factors; Awareness; Hail region
Introduction![]()
Cardiovascular diseases (CVD) adversely affects the human circulatory system, among all CVDs, coronary artery disease is most severe [1,2]. In developed countries, Coronary artery disease (CAD) is a genuine cardiovascular entanglement, which influences roughly 50% of moderately aged men and right around 33% of moderately aged ladies [3-7]. In spite of the fact that it still one of the main sources of death in grown-ups beyond 35 years old years, even with the remarkable decrease in coronary illness-related mortality [5]. In Saudi Arabia, there is an inadequate measure of information identified with the real prevalence of CAD. Notwithstanding, in 2004, a prevalence of 5.5% was accounted for among people somewhere in the range of 30 and 70 years [8]. CAD risk factors are well identified; hence, cardiovascular infractions can be prevented by taking effective measures [9]. CAD can be avoided by adopting a healthy lifestyle and preventing diseases such as Diabetes mellitus, hypertension, hypercholesteremia, obesity, psychological stress, and lack of physical activity) [10], which can pave the way towards CAD. However, old age, certain ethnicities, and family history cannot be avoided [11].
The greater part of the patients had, in any event, one uncontrolled hazard factor that mirrors a low degree of mindfulness about the ailment [12]. Generally, half of the patients had, in any event, three hazard factors. These three hazard factors are corpulence and hypertension were found in half of the patients, while dyslipidemia where found in seventy-five percent [13]. Mindfulness is known as earlier information on the status of cardiovascular hazard factors (CVRFs). An individual must see their wellbeing to be in danger or be vulnerable to hazard to make the preventive move, According to the Health Belief Model [14]. The consciousness of CAD hazard can urge the populace to change their everyday propensity with respect to the practice and a sound eating regimen and decline their opportunity of having a stroke or myocardial localized necrosis.
However, appropriate steps cannot be taken if people are unaware of the risk of CAD [15-17]. Awareness and education are essential to prevent and avoid the risk factors related to the prevalence of CAD [18,19]. For the prevention of the disease, knowledge and awareness about the risk factors for CAD are important, not only among health practitioners but also among the general population.
In Western nations, Coronary conduit artery disease (CAD) is the main source of death. Broad proof has demonstrated that the improvement of CAD can be forestalled by altering hazard factors [20]. The pervasiveness of CAD has been accounted for to go from 5.4% to 13.4% in the Middle Eastern regions. [21,22]. Anticipation is the foundation of endeavors to lessen CAD-related morbidity and mortality because up to date, even with the presence of profoundly compelling treatments for CAD, every one of them ought to be taken long-lasting, and a therapeutic operator stays subtle. Tight control of hazard factors is urgent for the counteraction of CAD. The point of the current work was examining the level of mindfulness about hazard factors for the CAD among the Hail area populace.
Methods![]()
Study design
This cross-sectional investigation was directed in the Hail Governorate of Saudi Arabia, between April and May 2020.
Participants
Using simple random sampling to assess the level of awareness toward CAD, 537 participants aged from 18 years and above were selected randomly from Hail.
Data Collection
The aim of the present work was to investigate the degree of awareness about risk factors for CAD among the Hail region population. Data were collected from a total of five hundred, and thirty-seven participants participated through an online survey. The process of selection of participants was through volunteer sampling and an online survey questionnaire, which was distributed to them to complete. No restrictions on age or gender were applied to the questionnaires. The survey was included s9 coronary artery disease (CAD) risk factors as follows: TV watching, lack of physical activity, smoking, soft drink intake, Having diabetes mellitus (DM), family history of DM, family history of hypertension (HTN), family history of CAD and family history of hyperlipidemia.
Statistical Analysis
Data management was done using the Statistical Package for Social Sciences (SPSS version 23). Data were represented as mean ± standard deviation and percentage.
Results![]()
The aim of present work was to investigate the degree of awareness about risk factors for the CAD among Hail region population, for that the data demographic and cross-sectional survey for the population has been collected as the following:
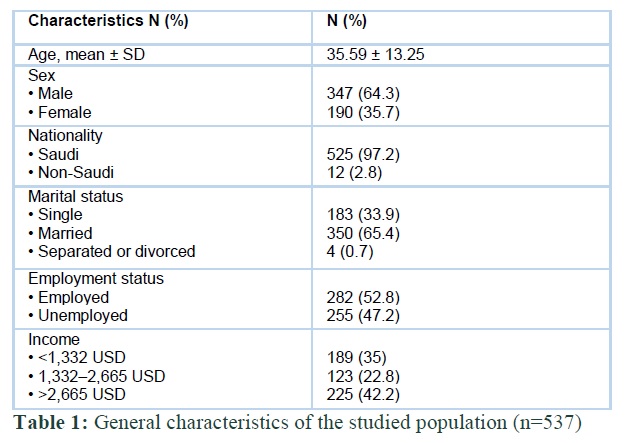
General characteristics of the studied population
The demographic characteristics of the 537 participants (Male = 347 64.3%) survey are shown in Table 1. The overall mean age was (35.59 ± 13.25 years) and the distribution of participants according to nationality Saudi / non-Saudi was 97.2% / 2.8%, employment status employed / unemployed was 52.8% / 47.2, marital status was 33.9 % single, 65.4% married, and 0.7% separated or divorced. For the participant's incomes, the salary amount was ranged between 1,332 – 2,665 USD.
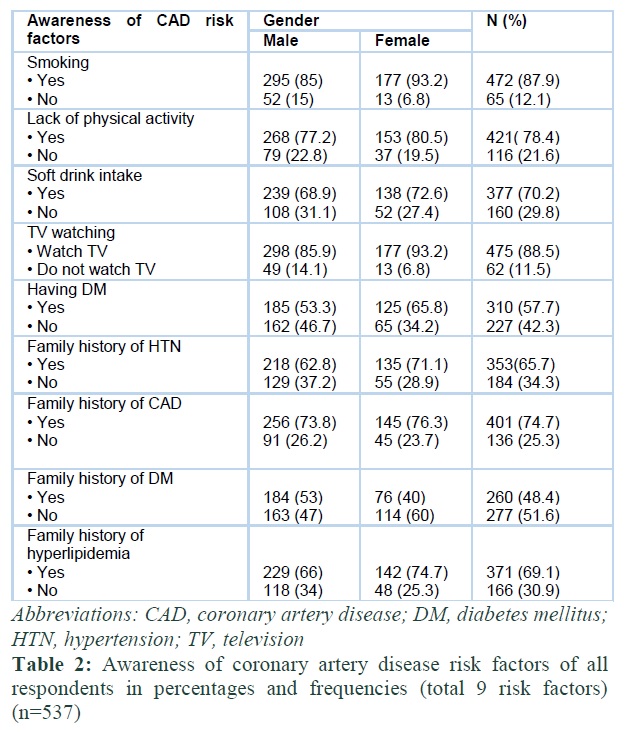
Awareness of risk factors for CAD
The degree of awareness about the CAD risk factors among the population of Hail region was shown in table 2 and figure 1. Awareness of TV watching (88.5%), smoking (87.9%), lack of physical activities (78.4%), and family history of CAD (74.7%) as the leading cause of CAD has a notable higher percentage among the studied population. In contrast, the family history of DM (51.6%), having DM (57.7%), a family history of HTN (65.7%), and a family history of hyperlipidemia (69.1%) have the lowest percentages. Regarding the gender, the male participants have the poorest awareness degrees about risk factors for the CAD (Table 2).
Figures & Tables
Discussion![]()
This was the first survey ever conducted for the Hail region population about the degree of awareness of the CAD and its risk factors. The study revealed that the poorest degrees of awareness of the risk factors for the CAD among the studied population were the family history of DM, having DM, family history of HTN, and family history of hyperlipidemia as follows 51.6, 57.7, 65.7 and 69.1 % respectively. However, our observation also confirmed by the finding of Kholoud (2018) who referred to the high percentage levels of heart diseases
(9%) among her studied population in Hail city that gives an alarm for taken more attention, and taking into account that CAD is the main leading cause of death among middle-aged individuals. On the other hand, we found that the male participants have the poorest awareness degrees about risk factors for the CAD.
The study revealed that the family history of hyperlipidemia, Family history of DM, having DM, and family history of hypertension have the poorest degrees of awareness of the risk factors for CAD among the studied population. We necessitate the need for a comprehensive awareness and screening program.
Author Contributions
S.M.A.S. Conceived and planned the experiments; T. A.N. G. Carried out the experiments and Data analysis; M. A. K. Planned and carried out the simulations; M. K. and F.S.H.A. Contributed to Questionnaire preparation; A. H. A., J.S.A, D.A.A.,W.S.A., R.M.A. , S.A.S.A., M.R.A.,K.I.A. H.S.A and A.M.A. Contributed to data collection; M. S. Contributed to the interpretation of the results.
The author(s) declare that they have no competing interests.
Ethical Consideration
Data collectors introduced the participants by explaining the benefits and aims of the study. Informed consent was obtained from all participants. Confidentiality and anonymity of data were maintained throughout the study.
Acknowledgment
The authors are indebted to Prof. Hussain Gadelkarim Ahmed for his help in the statistical analysis of the research data.
References![]()
- Al-Dosari ZF, Aldawsari AM, Almehyni AA, Alburayk AK, Hotan ASB, et al. Knowledge of coronary artery disease (CAD) risk factors and coronary intervention among university students in Saudi Arabia. International Journal of Medicine in Developing Countries. (2019); 3(6): 526-531.
- Nabi R, Alvi SS, Saeed M, Ahmad S, Khan MS. Glycation and HMG-CoA Reductase Inhibitors: Implication in Diabetes and Associated Complications. Current Diabetes Reviews, (2019); 15(3): 213-223.
- Sanchis-Gomar F, Perez-Quilis C, Leischik R, Lucia A. Epidemiology of coronary heart disease and acute coronary syndrome. Annals of Translational Medicine, (2016); 4(13): 256.
- Centers for Disease C, Prevention. Prevalence of coronary heart disease–United States, 2006-2010. Morbidity and Mortality Weekly Report, (2011); 60(40): 1377-1381.
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, et al. Heart disease and stroke statistics–2015 update: a report from the American Heart Association. Circulation, (2015); 131(4): e29-322.
- Berry JD, Dyer A, Cai X, Garside DB, Ning H, et al. Lifetime risks of cardiovascular disease. The New England Journal of Medicine, (2012); 366(4): 321-329.
- Ahmad S, Siddiqui Z, Rehman S, Khan MY, Khan H, et al. A Glycation Angle to Look into the Diabetic Vasculopathy: Cause and Cure. Current Vascular Pharmacology, (2017); 15(4): 352-364.
- Al-Nozha MM, Arafah MR, Al-Mazrou YY, Al-Maatouq MA, Khan NB, et al. Coronary artery disease in Saudi Arabia. Saudi Medical Journal, (2004); 25(9): 1165-1171.
- Sorrentino MJ. Cholesterol reduction to prevent CAD. What do the data show? Postgraduate Medical Journal, (2000); 108(7): 40-42, 45-46, 49-52.
- Hajar R. Risk Factors for Coronary Artery Disease: Historical Perspectives. Heart Views, (2017); 18(3): 109-114.
- Members: ATF, Perk J, De Backer G, Gohlke H, Graham I, et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012) The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). European heart journal, (2012); 33(13): 1635-1701.
- Traina MI, Almahmeed W, Edris A, Murat Tuzcu E. Coronary Heart Disease in the Middle East and North Africa: Current Status and Future Goals. Current Atherosclerosis Reports, (2017); 19(5): 24.
- Ahmed AM, Hersi A, Mashhoud W, Arafah MR, Abreu PC, et al. Cardiovascular risk factors burden in Saudi Arabia: The Africa Middle East Cardiovascular Epidemiological (ACE) study. Journal of the Saudi Heart Association, (2017); 29(4): 235-243.
- Jones CL, Jensen JD, Scherr CL, Brown NR, Christy K, et al. The Health Belief Model as an explanatory framework in communication research: exploring parallel, serial, and moderated mediation. Health Communication, (2015); 30(6): 566-576.
- Folsom AR, Yatsuya H, Nettleton JA, Lutsey PL, Cushman M, et al. Community prevalence of ideal cardiovascular health, by the American Heart Association definition, and relationship with cardiovascular disease incidence. Journal of the American College of Cardiology, (2011); 57(16): 1690-1696.
- Stampfer MJ, Hu FB, Manson JE, Rimm EB, Willett WC. Primary prevention of coronary heart disease in women through diet and lifestyle. The New England Journal of Medicine, (2000); 343(1): 16-22.
- Lloyd-Jones DM, Hong Y, Labarthe D, Mozaffarian D, Appel LJ, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association's strategic Impact Goal through 2020 and beyond. Circulation, (2010); 121(4): 586-613.
- Liu K, Cedres LB, Stamler J, Dyer A, Stamler R, et al. Relationship of education to major risk factors and death from coronary heart disease, cardiovascular diseases and all causes, Findings of three Chicago epidemiologic studies. Circulation, (1982); 66(6): 1308-1314.
- Pocock SJ, Shaper AG, Cook DG, Phillips AN, Walker M. Social class differences in ischaemic heart disease in British men. Lancet, (1987); 2(8552): 197-201.
- Mosca L, Ferris A, Fabunmi R, Robertson RM, American Heart A. Tracking women's awareness of heart disease: an American Heart Association national study. Circulation, (2004); 109(5): 573-579.
- Nsour M, Mahfoud Z, Kanaan MN, Balbeissi A. Prevalence and predictors of nonfatal myocardial infarction in Jordan. Eastern Mediterranean Health Journal, (2008); 14(4): 818-830.
- Zeidan RK, Farah R, Chahine MN, Asmar R, Hosseini H, et al. Prevalence and correlates of coronary heart disease: first population-based study in Lebanon. Vascular Health and Risk Management, (2016); 1275-84.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


