

Review Article
Viral outbreaks: A real threat to the world
Muhammad Asif1, Shah Nawaz2, Zeeshan Ahmad Bhutta3*, Muhammad Fakhar-e-Alam Kulyar4, Muhmmad Rashid5, Shafqat Shabir6, Muhammad Kashif Khan7, Muhammad Muaaz Qadir8
Adv. life sci., vol. 8, no. 1, pp. 08-19, November 2020
*- Corresponding Authors: Zeeshan Ahmad Bhutta (Email: doctorzeeshan94@gmail.com)
Authors' Affiliations
2. Department of Pathology, University of Agriculture, Faisalabad – Pakistan
3. The Royal (Dick) School of Veterinary Studies, University of Edinburgh – United Kingdom
4. College of Veterinary Medicine, Huazhong Agricultural University, Wuhan, 430070 – PR China
5. Independent Medical College, Faisalabad – Pakistan
6. Department of Parasitology, University of Veterinary and Animal Sciences, Lahore – Pakistan
7. Department of Pathology, University of Agriculture, Peshawar – Pakistan
8. Faculty of Veterinary and Animal Sciences, The Islamia University of Bahawalpur – Pakistan
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
Global public health is facing significant challenges in terms of emerging and re-emerging pathogens. The world is facing a new public health crisis emergence and spread of Coronaviruses outbreaks especially COVID-19 after nine deadliest viral outbreaks including Marburg virus, Ebola virus, Rabies, HIV, Smallpox, Hantavirus, Influenza, Dengue and Rotavirus. Coronaviruses (enveloped non-segmented positive-sense RNA viruses) belong to the Coronaviridae family, broadly distributed in humans as well as in other mammals. In December 2019, the COVID-19 outbreak was reported in the Wuhan, Hubei province of China. WHO confirmed that COVID-19 is associated with Huanan seafood (Wuhan). COVID-19 virus outbreak is more dangerous than its ancestors MERS-CoV and SARS-CoV. Although the case fatality rate is lower, it has alarmed the world because of its rapid spread during this era of the modern world where the whole world is connected through different channels of trade. As the world is already facing economic challenges, underdeveloped countries are not capable of facing such challenges, and this outbreak may become worse than ever before.
Keywords: Coronaviruses; COVID-19; Marburg virus; Ebola virus; Rabies; HIV; Smallpox; Hantavirus; Influenza; Dengue; Rotavirus
Introduction![]()
Outbreaks are usually defined as cases of illnesses that occur in the community more frequently than usual. Number of cases showing outbreak occurrence depends upon the size and type of the population exposed to the infectious agent. Viruses are known as major causes of the outbreak of foodborne diseases [1]. Emerging infectious diseases are the most significant health challenge of the 21st century. Among these, the zoonotic viruses which originate from the reservoir host and transfer to humans and causes the disease syndrome of different form and severity. Depending on the capability of the emerging virus to transmit in the human population, causes individual or some sporadic cases which results into localized outbreak or, in worst condition large epidemic or a global pandemic. Such type of various emergence events occurs in the last two decades. They include the viruses that are not previously encountered like coronaviruses, severe acute respiratory syndrome (SARS), Middle East Respiratory Syndrome (MERS) and familiar enemy which have reappeared and causes outbreaks like Ebola virus outbreaks [2]. Emerging viruses had the capability to cause significant mortality, morbidity and economic burdens for humans. This review aims for the better understanding of the risks and impact of these viral outbreaks (coronaviruses, COVID-19, Marburg virus, Ebola virus, Rabies, HIV, Smallpox, Hantavirus, Influenza, Dengue, Rotavirus) on humans at global level mainly focusing on recent COVID-19 pandemic which showed inimitable impact all over the world.
Methods![]()
Literature Search strategy and selection criteria
A systemic search was carried from PubMed, Google Scholar, Google Web Browser and World health organization reports, by using keywords viral outbreaks, coronaviruses, COVID-19, Marburg virus, Ebola virus, Rabies, HIV, Smallpox, Hantavirus, Influenza, Dengue, Rotavirus. According to the particular contents, further literature was screened mainly on the basis that when first outbreak of these viruses was reported, total number of cases and deaths reported in first outbreak. Transmission and economic losses were also reviewed. In this study, 126 published articles including World Health Organization (WHO) reports were selected to do a comprehensive review.
Discussion![]()
Corona Viruses
Novel Corona Virus (COVID-19)
The world is facing a new public health crisis emergence and spread of COVID-19 (coronavirus disease caused by 2019-nCoV). Coronaviruses (enveloped non-segmented positive-sense RNA viruses) belong to the Coronaviridae family, broadly distributed in humans as well as in other mammals [3]. In December 2019 COVID-19 outbreak was reported in the Wuhan province of China [4], which is subsequently prevalent worldwide. Initially, series of pneumonia cases of unknown cause was reported in Wuhan, China, WHO named this virus 2019-nCoV (2019 novel Coronavirus) on 12th January 2020, later world health organization named this disease COVID-19 (coronavirus disease caused by 2019-nCoV) officially on 11th February 2020 [5]. WHO confirmed that the COVID-19 outbreak was associated with the Huanan South China Seafood Marketplace [6]. The novel coronavirus (COVID-19) is spreading rapidly from Wuhan to the rest of the world [7]. Internationally public health emergency declared by WHO on 30 January 2020, after the emergence of SARS-CoV (severe acute respiratory syndrome coronavirus) and MERS-CoV (Middle East respiratory syndrome coronavirus) in 2002 and 2012 respectively, marked the 3rd introduction of coronavirus into humans which is highly pathogenic in this 21st century [8]. The genome of the COVID-19 was published for the first time on 10 January 2020 by a research team working under Prof. Yong-Zhen Zhang [6]. The National Health Commission of China officially announced to include COVID-19 into the management of class B legal infectious [6]. This virus (COVID-19) originates from bats while its intermediate host is pangolins, humans are terminal hosts [9], transmitted into humans [10], animals to humans [11], it transmits through respiratory droplets by coughing or sneezing. The reproduction number of COVID-19 is 2.2. Generally, COVID19 is an infectious disease with a 2% case fatality rate [12]. Pathologically COVID19 features show great resemblance to the SARS-CoV and MERS-CoV pathological features [13]. The novel coronavirus (COVID-19) spreads faster than SARS-CoV and MERS-CoV, but low case fatality rate [14]. The transmissibility level of the COVID-19 is higher than SARS-CoV (severe acute respiratory syndrome). A severe onset of a disease may result in death because of massive alveolar damage in the lungs and progressive failure of the respiratory system [15]. Symptoms that are reported in case of COVID-19 include fever, dyspnea, cough, hemoptysis, fatigue, diarrhoea, pneumonia and headache [16]. Lymphopenia is common in COVID-19 patients, and it may be the critical factor associated with mortality and severity of disease [12].
Total confirmed cases of COVID-19 were 93091 (04 March 2020) which increases to 972303 (3 April 2020). On average, 28361 cases rise daily. At the same time, total confirmed cases of COVID-19 were 3198 (04 March 2020) which grows to 50321 (3 April 2020). On average 1590 daily deaths were being reported (Figure 1).
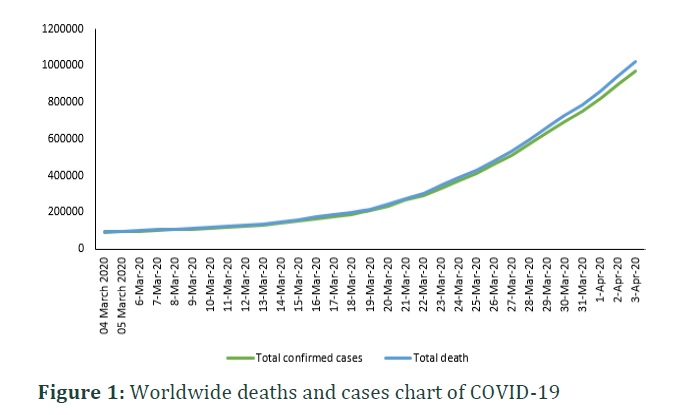
As the number of cases increases daily deaths also increasing day by day, it indicates that the situation may be worsened in the future.
Transmission
This virus (2019-nCoV) originates from bats while its intermediate host is pangolins, humans are terminal hosts [9], transmitted into humans [10], animals to humans [11], it transmits through respiratory droplets by coughing or sneezing. The reproduction number of COVID-19 is 2.2. Generally, COVID19 infection is an acute disease with a 2% case fatality rate [12]. Pathologically COVID19 features show a remarkable resemblance to the SARS-CoV and MERS-CoV pathological features [13]. The novel coronavirus (2019-nCoV) spreads faster than SARS-CoV and MERS-CoV, but low case fatality rate [14]. The transmissibility level of the COVID-19 is higher than SARS-CoV (severe acute respiratory syndrome). A severe onset of a disease may result in death because of massive alveolar damage in the lungs and progressive failure of the respiratory system [15]. Symptoms that are reported in case of COVID-19 include fever, dyspnea, cough, hemoptysis, fatigue, diarrhoea, pneumonia and headache [16]. Lymphopenia is common in COVID-19 patients, and it may be the critical factor associated with mortality and severity of disease [12].
MERS-CoV and SARS-CoV
Global public health is facing significant challenges in terms of emerging and re-emerging pathogens[17]. Coronaviruses, the enveloped RNA viruses, have a wide range of distribution among humans, birds, and other mammals leading to respiratory, hepatic, enteric, and neurological infections [18]. Due to wide distribution, high prevalence of coronaviruses, more genetic diversity, recombination of genomes, and enhancing animal-human interaction, novel coronaviruses may emerge or re-emerge periodically. It is more dangerous because of the zoonotic importance, trans-species infections, and occasionally spillover events [19]. The name coronavirus is derived after the crown-like spikes on the surface of the virus, these also resemble the corona of the sun, the diameter of the virus ranges between 60-140 nm. Distinctive spikes on the surface give them a typical appearance, the diameter of coronavirus spikes varies from 9-12 nm [18]. The genome organization of all coronaviruses is similar, while gene replicates circumscribe the 5ʹ sixty percent of the genome and is made up of two open reading frames (ORFs). These frames are ‘ORF1a’ and ‘ORF1b’ which are encoded for non-structural proteins, could be up to 16. On the 3ʹ end, the structural gene region covers one-third of the genome, structural protein genes are encoded from 5ʹ to 3ʹ as a spike, envelop, membrane, and nucleocapsid, respectively. Open reading frames are also nurtured by structural gene regions and are intermixed along with the coding genes of the structural proteins. Each coronavirus species has a distinct sequence and number of ORFs [20].
In the previous two decades, two species of coronaviruses have crossed the species barrier, leading to the acute and lethal infection to humans, SARS-CoV, and MERS-CoV in 2002 and 2012, respectively [21]. The case fatality rate of SARS-CoV and MERS-CoV was noted comparatively higher than that of other common respiratory viral infections, 10 and up to 50%, respectively [22].
MERS-CoV was first identified and reported to WHO in September 2012 [21]. The first human with the infection of “MERS-CoV” (Middle East Respiratory Syndrome) appears in Saudi Arabia during June 2012. The one was an old man of 60 years. He visited the hospital owing to pneumonia, while later, it was known to develop renal failure [23].
The latent period of middle east respiratory syndrome coronavirus is two to fourteen days, with a median of 5.4 days. It takes four days from the disease development and patients admission, the period when people die due to disease. It takes 11.5 days [24]. Flue like symptom is observed in the first stage, including arthralgia, myalgia, fever, chilling, and coughing followed by the respiratory difficulty, which is quickly progressed to pneumonia [25]. The complaint of thirty percent of patients was to have bowel symptoms, including vomiting and diarrhea [26].
Natural reservoirs of the “MERS-CoV” and SARS-like coronaviruses are Bats. However, there is a shred of evidence about a small number of camels found positive (positive nasal swabs by rtPCR) and the presence of antibodies against middle east respiratory syndrome coronaviruses. The route of transmission and the intermediate animal source remains uncertain among sporadic primary cases. Severe respiratory failure may occur due to both middle east respiratory syndrome viruses and SARS-CoV, which also causes extrapulmonary features like diarrhea, while mild and asymptomatic cases also present in both conditions. In contrast with SARS-CoV and patients with middle east respiratory syndrome, coronaviruses are older and male predominance more comorbid illness and comparatively lower transmission potential regarding humans to humans. Although viral kinetics of the middle east respiratory syndrome Coronaviruses remains unknown and nosocomial infection of MERS-CoV occurs early within 1st week of illness, while SARS-CoV in 2nd week of illness when the viral load peaks on in the upper airway of the patients on 10th day of the illness. It is suggested by the in-vitro data that interferons with or without the mycophenolic acid and ribavirin may inhibit middle east respiratory syndrome Coronaviruses, while interferons and protease inhibitors also have inhibitory activity against the SARS-CoV [23].
Globally 887 cases of middle east respiratory syndrome Corona Viruses infection confirmed by the laboratory were reported since 30 September 2014, and 352 patients have died with 39.7% case fatality rate, 97.5% cases were present in the Middle East including Saudi Arabia, Iran, Lebanon, Jordan, Yemen, Oman, Egypt, United Arab Emirates, Kuwait, and Qatar, among this 85.0% was reported in Saudi Arabia [27]. To closely monitor the “MERS-CoV” infections globally and to understand the risks regarding public health in a better way, CDC is working with WHO and other partners.
WHO confirmed the 956 cases (laboratory-confirmed cases) of Middle East respiratory syndrome Corona Viruses (MERS-CoV) with at least 351 casualties since 23rd of January, 2015. All the reported cases were linked directly or indirectly through traveling or residential history to the 9 countries, including Saudi Arabia, Iran, Lebanon, Jordan, Yemen, Oman, Egypt, United Arab Emirates, Kuwait, and Qatar. Two patients were found positive to MERS-CoV infection since May 2014 in the United States, each of them showed a history of fever and one or more respiratory signs after their recent travel from Saudi Arabia. No further case of Middle East respiratory syndrome Corona Viruses infection was reported despite the nationwide surveillance and also the testing of 514 patients from the 45 states of the United States. The majority of the cases 504 out of 956 MERS-CoV occurred during the month of March-May.
However, WHO received the cases MERS-CoV infection mostly from Saudi Arabia from 1st august, 2014, through 23 January 2015, world health organization confirmed 102 cases out of these 97 cases occurred in the persons who were resident in Saudi Arabia, including three traveling histories of cases reported by Jordan, Austria and Turkey, two cases were reported from Qatar and three cases were reported from Oman [28].
Transmission
Primarily severe acute respiratory syndrome is transmitted through contact or large respiratory droplets [29], limited airborne transmission [30]. No evidence of perinatal SARS infection among infants born to mothers who developed SARS infection during pregnancy [31]. MERS-CoV infection suggests zoonotic transmission [32]. Secondary transmission (human to human) [24]. Bats may be the ancestors of coronavirus [33]. MERS-CoV causes a zoonotic infection, infects dromedary camels, and can be transmitted to humans through close contact [34]. SARS-CoV and MERS-CoV can be transmitted through symptomatic patients, not from asymptomatic or patients with no specific signs [35]. SARS-CoV was transmitted to humans from exotic animals in wet markets, while MERS-CoV is transmitted to humans from camels [36]. human hosts from Zoonotic reservoirs such as bats, raccoon dogs and Himalayan palm civets transmits SARS-CoV into human host [37]. Risk of transmission of MERS-CoV infections is high in the health care workers who are in close contact with the patients and handling the biological materials such as faeces, blood, sputum, urine, and respiratory secretions[38]. 5% rate of secondary transmission of MERS-CoV infections is reported [39]; it can also be transmitted from human to human [40].
Marburg virus
In 1967, filovirus hemorrhagic fever first appeared in Germany and the former Yugoslavia. Marburg virus (MARV), the pathogen identified in this outbreak, is one of the deadliest pathogens in humans. [41]. The Ebola virus (EBOV) (organization, 1978) belongs to a well-known family and first appeared in Africa in 1976. Shortly afterwards, Marburg and Ebola viruses were classified as a newly formed family called Filoviridae. It is called because of its characteristic filament structure (filum is Latin means thread). Between 1975 and 1985, MARV on the African continent caused only one outbreak, affecting a small number of people.
Because the case fatality rates associated with MVD were lower than 90% of the catastrophic outbreaks associated with EBOV, the threat of MARV has not been considered for a long time. MARV reemerged between 1998 and 2000. Two major outbreaks: Democratic Republic of the Congo (DRC), 2004-2005 [42], and First time in Angola in West Africa [43]. A total number of cases more than four hundred with high case fatality rates >80% in DRC and up to 90% in Angola depicts that MARV was a major public health threat like EBOV [44].
According to the World Health Organization (WHO), the mortality rate at the first outbreak was 25%, compared to the Democratic Republic of the Congo between 1998 and 2000 and more than 80% in Angola in 2005.
Transmission
Filoviruses categorized as the deadliest zoonotic viruses known to infect human beings [45]. Marburg virus infects humans sporadically [46]. There is no evidence of transmission by asymptomatic patients. The chance of transmission without direct physical contact is very low but not zero [47]. Risks of transmission increase dramatically by visiting and caring for filovirus cases in hospitals. Earlier hospitalization and longer stay providing isolation and protection can shorten the periods of filovirus outbreaks [47], can transmit human to human [48]. Possible sexual transmission of Marburg Virus has been reported [49]. Infection can be transmitted due to funeral related events [50].
Ebola virus
The first Ebola outbreak in Sudan and the Democratic Republic of the Congo in 1976 was stuck in humans [51]. The Ebola outbreak in West Africa was the 25th known outbreak since 1976, but radically different from all previous cases [52]. Transmission of the Ebola virus occurs via body fluids or tissues of infected individuals. According to Milberger, the deadlines of known strains varies widely. Ebola Reston is a nonpathogenic strain. As of 31 March 2020, a total of 3453 EVD (Ebola virus disease) cases were reported from 29 health zones including 3310 confirmed and 143 probable cases, of which 2273 cases died (overall case fatality ratio 66%). Of the total confirmed and probable cases, 56% (1935) were female, 28% (979) were children aged less than 18 years, and 5% (171) were healthcare workers.
Transmission
The Ebola virus outbreaks were associated with bush meat and fruit bats handling [46]. Filovirus infection is primarily transmitted through close contact or later stages of illness[47], infected patients, body secretions including sweat and breast milk, and excretions including semen, vomit, stool, urine [53], broken skin, mucous membrane, contaminated syringes [47], transmits to human by the freshly killed bats consumption [54], hunting and butchering of monkeys, chimpanzees, duikers and gorillas for food [55]. Isolation of the Ebola virus 82 days and detection of viral RNA 101 days after the onset of symptoms has been reported [56]. There is evidence of sexual transmission and persistence of infective Ebola virus in semen for 179 days or more after the onset of Ebola virus disease (EVD) [57]. Ebola Virus survivors should avoid unsafe sex until more information about the shedding of the infectious virus through body fluids is known. A male survivor should use condemn every time for safe sex (oral, vagina, anal) [58]. There is circumstantial evidence of aerosol transmission during EBOV outbreak (1995) in the democratic republic of Congo that has been reported [59].
Rabies virus
Rabies (acute encephalitis) caused by Lyssavirus of Rhabdoviridae family, rarely infects human, transmits from an organ donor to multiple recipients [60]. Lyssavirus is one of the seven genera of the family Rhabdoviridae family, order Mononegavirale. It comprises of RABV; genotype 1 (classical rabies virus), LBV; genotype 2 (Lagos bat virus), MKV; genotype 3 (Mokola virus), DV; genotype 4 (Duvenhage virus), EBLV-1; genotype 5 (European bat lyssavirus 1), EBLV-2; genotype 6 (European bat lyssavirus 2), and ABLV; genotype 7 (Australian bat lyssavirus). Four additional viruses are also isolated from insectivorous bats and proposed as new members of the Lyssavirus genus: Aravan virus, Khujand virus, Irkut virus, and West Caucasian bat virus [61].
Transmission
Non-bite transmission is very rare, and aerosol transmission has never been well documented [62]. 99% of humans death due to rabies occurs due to domestic dog [63], infected peoples (secretions) may be a potential risk [64]. The virus is inoculated by the biting of rabid animals (virus-laden saliva) into muscles subcutaneous tissues [65], through wounds, direct contact with the mucosal surface and it cannot cross intact skin. Risk of rabies infection by a bite is 5%-80% which is at least 50 times greater than that by a scratch 0.1%-1%, Mortality after untreated bites by rabid dogs ranges from 38% to 57% [66]. Bat virus might be more infectious than dogs [67].
The rabies vaccine was introduced in the 1920s because of its use in domestic animals number of cases was exceedingly reduced in developed countries, but it remained a significant issue in African and some Asian countries. This was the first outbreak of rabies transmitted by vampire bats in Brazil, where the rabies virus was isolated from humans and bats [68]. Bats have spread rabies outbreaks in several remote locations in Peru [69], Venezuela [70], and Brazil [71].
HIV (Human immunodeficiency virus)
Human immunodeficiency virus (HIV-1) belongs to the retroviridae family and is a causative agent of acquired immunodeficiency syndrome, more than 30 antiviral drugs have been invented [72]. These antiviral drugs help infected patients with HIV to live even for years. But the destruction of this disease being continued in middle and low-income countries in which more than 90% of new cases of HIV occur. According to WHO, 5% of the population of African countries is HIV-positive. HIV infection was diagnosed in 135 patients out of 4200 papulation on April 21st by ISDH (Indiana State Department of Health), out of them, 129 were confirmed positive while 6 cases were preliminary positive with rapid HIV testing and their confirmatory testing was pending. Confirmed (135) patients range between 18-57 years of age with 35 years mean and 32 years of the median. The percentage of male patients (55%) was higher than that of female, and no infant was declared as HIV positive. Antiretroviral therapy was recommended for pregnant HIV women patients during pregnancy. Out of all the confirmed cases, 80% were those having injection drug use (IDU) history, only 3% with no IDU while remaining have unknown IDU status.
Transmission
The process of HIV transmission, establishment, and dissemination remains unclear in human beings for thirty years after its discovery [73]. The gender relatedness of women makes them at high risk directly or indirectly to HIV. The statistical analysis of HIV depicts an alarming situation. According to a survey of the World Health Organization up to 10 million people were infected in jolly 1990 round the globe[74]. People who are infected with HIV are often held responsible for their condition. Because HIV is infected with behaviours that people think they can avoid: unsafe sex and irrational drug use [75]. The stigma of AIDS is also closely linked to other stigma related to dangerous behaviours, such as sexual temptation, homosexuality, intercourse, and drug use. HIV-infected people with sexual and narcotic effects have the greatest side effects compared to people infected with blood transfusions [76].
Smallpox
Natural pox is the main biological, social, and spatial factor that affects the spread of disease in modern populations, and it has been largely elucidated based on historical research before the disease was eliminated in 1979 [77]. Even after the eradication of smallpox, it is a continuous risk for humanity until laboratory stocks of virus vanished [78]. Some Preliminary reports that the outbreak of smallpox in the former Soviet Union in 1971 was triggered by field trials with secret biological weapons led to intense debate and several uncomfortable steps among a small group of bioterrorism experts. Outbreaks indicate that a natural smallpox aerosol attack could indeed be fatal, suggesting that the Soviet Union turned the extremely deadly effects of natural smallpox into a weapon [79]. Contingency arranging for the plausible intentional reintroduction of natural smallpox has been a priority for many national health authorities in recent years [80].
Tracked vaccination policy has been integrated into a natural smallpox transmission model to approximate the number of suspected cases and deaths from agglomeration attacks. If we compare the results from the time the seizures were detected with mass vaccination, we see that mass vaccination leads to far fewer deaths and much faster epidemic eradication for a variety of diseases and intervention guidelines. Mass vaccinations, including those considered the most likely, also go beyond current policies and begin tracking vaccinations and switch to mass vaccination only when needed [81].
World Health Assembly proclaimed the globe free from smallpox in 1980. But before the eradication of disease, it makes several attacks on humans over thousands of years, and smallpox killed humans with a 33% case fatality rate, those who survived have to suffer scars and blindness permanently. Non-European populations have a higher mortality rate, and the virus is little exposed until tourists bring it to the region. For example, according to an estimation, the death of 90% American native population from smallpox occurred due to European researchers. Three hundred million people were died by smallpox only in the 20th century. Smallpox was a massive burden on the earth, not only because of mortality but also scars and blindness, which stimulate a campaign for its eradication from the earth.
Transmission
First outbreak of smallpox in Bradford was reported in 1942 [82] and 1962 in Edinburgh. The initial reproduction rate of smallpox is 2 [83], which is reported different in other breaks. Before the eradication of smallpox, it was a directly transmitted respiratory disease caused by the variola viruses, the mortality rate in 1974 was 26.5% among the unvaccinated in India [80]. Variola aerosols produced a disease that simulated human smallpox [84]. Transmission throughv casual contact is very rare [85].
Hantavirus
This virus belongs to the family Bunyaviridae and is nurture from martyred rodents. Infected rodents are reservoir host, and they excrete viruses through body secretions and excretions like saliva, urine, and faeces. Deer mouse (Peromyscus maniculatus) is a reservoir host for Sin Nombre orthohantavirus [86]. A zoonotic disease which is rodent born, Hantavirus cardiorespiratory syndrome (HCPS) is an endemic disease of America and confined there for several decades. According to a hypothesis, precipitation was increased due to El Nino southern oscillation providing a favourable environment that allowed a rise in rodent’s population, increasing its risk of zoonotic transmission in 1991-1992. This transmission possibly results in the HCPS outbreak between 1993-1994 at each corner of the southwestern United States [87]. A total of 52 patients were affected by HCPS in the 1993 outbreak that was continued up to 1994. These cases were reported sporadically in a four-cornered state and elsewhere in the USA. An average of four cases were reported annually from 1995-1997 in the United States [87].
Ample attention was gained by HPSC first time in the United States when a young man with his fiancée was died within a few days due to breathing shortness, from a four-cornered area in 1993. Few months after the death of a young man Hantavirus was isolated from deer mouse from the house of that affected person by health authorities. According to the reports of the Center for Disease Control and Prevention total of 600 people were affected by HPS in the U.S and out of the 216 were died with a 36% case fatality rate. According to the Federal Infection Protection Act in Germany, Hantavirus clinical cases have been reported since 2001 majorly due to the Puumala virus (PUUV) along with two other viruses, Dobrava-Belgrade and Tula [88].
On average, 220 cases of HPSC were reported each year from 2001-2006 with the highest 448 patients in 2005 [89]. While 1687 cases were confirmed in 2007 [89]. Droppings from infected mice are the main source of infection, from which infection spreads person to person. There was a previous outbreak of Hantavirus during the Korean War in the 1950s, reported in the review paper of journal Clinical Microbiology 2010. In this outbreak, 3000 soldiers were infected, and 360 have died with a 12% case fatality rate. At that time Hantavirus was a novel infection for U.S researchers, later on, its relation with deer mice was determined by Navajo medical traditions by detecting a similar disease.
Transmission
In 1993 Hantavirus pulmonary syndrome was recognized in united states for the first time it is a rodent-borne zoonosis [90]. Person to person of Hantavirus is reported [91]. Direct contact is not necessary for the transmission of Hantavirus between the rodents or rodents and humans, it can also be transmitted horizontally. Transmission rate becomes least dependent on the host density while increases the persistence in host population in case of indirect transmission [92].
Influenza Virus
Periodic and frequent epidemics caused by the Influenza virus is a major health issue. In 1918, 1957, 1968, 1977 pandemics of swine influenza, Asian influenza, Hong Kong influenza, Russian influenza occurred due to the type A antigenic variation of influenza virus. Due to minor antigenic variation in the strains of pandemics frequent epidemics may occur. Type A (H1N1) and A (H3N2) strains with minor antigenic variation and type B influenza virus is currently circulating worldwide causing frequent epidemics. Influenza virus belongs to Orthomyxoviridae family, having medium size 80–120 nm and three immunologic types: A, B, and C. Type A virus which is a major cause of disease outbreak (epidemics, pandemics) show antigenic variation continuously [93].
According to the WHO's, more than 500,000 people around the world die from the disease during a typical season of flu. Occasionally, however, a new strain of influenza appears, and a pandemic spreads the disease faster, often leading to higher mortality percentages. The most lethal pandemic influenza called Spanish flu that began in the 2nd decade of the 20th century and affected the 40% population worldwide. According to estimation, 50 million people have died during this outbreak.
Transmission
Influenza viruses can be transmitted through aerosols, large droplets, or direct contact with secretions (or fomites), aerosol transmission [94]. Large-droplets are the predominant mode of transmission of influenza virus infection [95], Coughing or sneezing [96].
Dengue virus
Dengue is a mosquito born emerging viral infection which is life threatening. There are four serotypes of Dengue virus including DENV-1, DENV-2, DENV-3 and DENV-4. Approximately 96 million clinical cases of dengue cases occur per annum throughout the world [97]. The first outbreak of the Dengue virus appeared in Thailand, and the Philippine in the 1950s then spread to the tropical and sub-tropical regions of the world. Global warming is enhancing the risk of disease transmission with carrier mosquitoes. Currently, the Dengue virus is endemic in the world’s 40% population area. The disease caused by this virus called ‘dengue hemorrhagic fever’ having some similarity with Ebola virus infection. Its mortality rate is 2.5%, slightly lower than some other deadly viral infections, but it could rise to 20% if left untreated. “Dengue is a real threat for humanity, and we have to take some practical steps against it,” Muhlberger said. Till now, there is no vaccine against this disease, some positive clinical results have obtained by French drug maker Sanofi.
Transmission
Dengue is a mosquito-borne viral infection [98], caused by four virus serotypes (DENV-1, -2, -3, and -4), primarily transmitted by day-biting of Aedes aegypti [99], having a short flight range [100, 101]. The dengue virus transmission is sensitive with seasonal variation as temperature changes affect the transmission of vector-borne viral disease and epidemic potential by the vector’s reproductive rate, length of EIP (the extrinsic incubation period), and biting rate [102]. Dengue virus can be transmitted without vector mosquito, needle stick injuries, vertical transmission, intrapartum, bone marrow transplantation and blood transfusion [103]. It is highly anthropophilic and breeds in water storage drums, bottles, buckets, discarded waste items, and over headed tanks [104]. Dengue is of particular importance in Asia [105]. Virus transmission increases with the increase of human population density. In cities, the movement of viraemic persons is a more important means of transporting dengue viruses as compared to the movement of Ae. aegypti mosquitoes [101].
Rotavirus
Rotavirus is a non-enveloped double-strand RNA virus. 114 million cases of rotavirus infection and more than 200000 deaths of children were reported worldwide in 2003 [106]. According to an estimation, 138 million cases and 215000 deaths annually were reported in children of age less than five years, in developing as well as in developed countries mainly in Asia and sub-Saharan Africa [107]. According to Rotavirus surveillance data (2008-2018) 40.78% children out of all diarrheal disease, children was infected with Rotavirus infection in Southeast Asia [108].
Rotavirus, another deadly viral threat mainly for children, one of the most leading causes of severe diarrhoea in young ones. Its transmission occurs through feco-oral route. Although two types of vaccines are available against this disease but the death of affected children occurs in developing countries due to a lack of rehydration facilities. But its mortality rate is very low in the developed world due to better treatment.
Rotavirus outbreak in 2008, up to half a million children were died worldwide, according to the World Health Organization. But a sudden decline in mortality rate has been reported in countries, where proper vaccination against rotavirus was done.
Transmission
Rotavirus can be transmitted through feco-oral route, and it can also be transmitted through direct contact with the contaminated surfaces, respiratory spread, contaminated hands. Other gastrointestinal infectious agents are transmitted through fecal-oral route, food may transmit such type of pathogen irrespective to this rotavirus spread in all home or day care centre not only the areas which are contaminated with stool [109]. A children with Rotavirus infection can excrete 100 billion virus particles in 1 g of stool. [110]. In hospitals rotavirus can be transmitted through aerosol transmission, and is detected in the respiratory secretions of some patients[111]. Investigators have found rotavirus on hand washing areas, faucet, toys, food preparation areas, diaper disposal containers and diaper changing areas [112]. It is also reported that asymptomatic patients can also transmit or shed Rotaviruses [113].
Economic impact
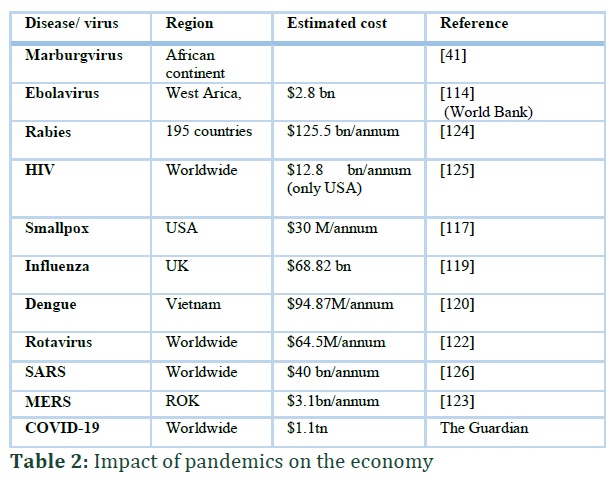
The outbreak of Ebola virus initially reported in Guinea in 2014 than spread to other West African nations like Liberia, Sierra Leone, and Guinea. The case fatality rate of this lethal virus was its major scare, 42-66% (World Health Organization, 2014). Due to high fatality and transmission rates, the borders of affected countries were sealed in July 2014, resulted in a negative impact on the economy. Agriculture and mining sectors are major contributors to GDP, 25% and 17% respectively in West African countries, and their production was slumped from 30-60% due to viral outbreaks [114].
According to an estimation, a total of $2.8 billion shrinkages in the economy of West African countries was produced because of the Ebolavirus outbreak in 2014 (World Bank).
Rabies is another disease of economic and public health significance around the globe. Its economic loses are more in developing and underdeveloped countries. Major economic losses are divided into three categories, i.e. direct losses, indirect and DALYs (disability-adjusted life years). DALYs loses are because of dog bites ($1.8 M) while their cumulative effect on vaccination, testing, and other effects on livestock and pets makes $5.5 billion per year[115]. Human mortality risk associated cost is a major burden on the global economy comprises of $1.2billion per year [114].
Human immunodeficiency syndrome virus (HIV) is a contagious and lethal virus throughout the world. It has diverse effects on the economy, according to a study there will be 0.56-1.08% drop in GDP of 30 African countries from 1990 to 2025[116]. In the United States, its economic impact is more scare, antiretroviral therapy against HIV costs $256 billion at the present level for previous years. This huge treatment cost reveals its economic importance [116]. Smallpox, a zoonotic disease of agricultural importance also played a diverse role against an economy in the history of mankind, its complete eradication costs $300 million in 10 years duration [117].
In the 20th century, there were three major pandemic outbreaks of Influenza (1918, 1957 and 1968)[118]. Its economic impact on the low fatality scenario was $68.2 billion while $88.9 billion for a high fatality scenario only in the United Kingdom [119]. The 21st century has seen a modified form of Influenza A subtype H1N1 severe acute respiratory syndrome (SARS) in 2003 and H5N1 (bird flu) in 2009.
Dengue is a mosquito-borne pandemic occurring in more than 100 countries all over the world. Its economic impact can be estimated that it costs $94.8 million per year only in Vietnam [120] and $169 million over 10 years between 2000-2015 in Brazil [121].
Diseases of GIT remains fifth and 2nd major cause of mortality and morbidity respectively in children’s of less than 5 years around the globe, rotavirus (norovirus) is one of them [122]. Globally, a total of 64.5 billion per year economic impact of norovirus, 4.2 billion covers direct health system cost while 60.3 billion is a societal cost [122].
The Middle East respiratory syndrome (MERS) outbreak in 2015 caused a total of $3.1 billion loss to the economy of Republic of Korea which indicates that public health emergencies due to outbreaks of contagious diseases may cause significant losses to the economies of affected countries [123]. COVID-19 may prove highly contagious economically as it is medically. The economic impact of this pandemic virus is far more than any previous outbreak. Its economic disruption is because of travel restrictions, factories closure, quarantines, and most effectively lockdown along with the direct impact on human health (economic in Time of COVID-19). According to an estimation, the global workforce may lose $3.4 trillion in 2020 because of the COVID-19 outbreak (International labor organization) (Figure 2).
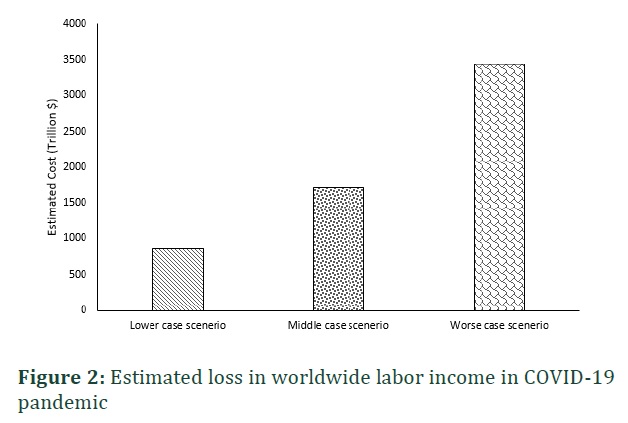
According to an estimation, $2.8 billion shrinkages in the economy of West African countries due to Ebolavirus outbreak in 2014, Rabies vaccination, testing, and other effects on livestock and pets makes loss of $5.5 billion annually, Human mortality risk associated cost is a major burden on the global economy is $1.2billion/ annum due to rabies. All viral outbreaks, including Marburg virus, HIV, Smallpox, Hantavirus, Influenza, Dengue, Rotavirus causes major loss of global economy. The global workforce may lose $3.4 trillion in 2020 due to COVD-19 pandemic. COVID-19 disease is a potentially fatal disease of global health concern that can be transmitted easily through aerosol transmission, direct contact, human to human and through secretions. Transmission of COVID-19 virus through asymptomatic patient is also a major threat. The COVID-19 pandemic showed us the immense economic cost of slowing down global trade, particularly shipping. It also reveals how dependent on the global supply chain we are, even for medical supplies such as masks and test materials. Due to the easy transmission of viral infection and fast spreading capability and high pathogenicity, viral outbreaks are the major threat for the modern world. The cases of COVID-19 are increasing day by day and a great threat to the world economy. Underdeveloped countries having inadequate healthcare facilities are going to be destroyed. Trade has stopped all over the world, implementation of curfew and lockdown in most of the countries indicates that despite having low case fatality rate, coronavirus (COVID-19) outbreak is going to be worse than ever before.
Future research should focus on the prevention of transmission of viruses rather than finding the cure of the disease or making an effective vaccine because the cost of vaccine and treatment results in an economic burden on the state. This could only be achieved by adopting the One Health approach. It is an integrated approach that enables workers of human health, animal health and plant to work mutually to achieve this goal.
Muhammad Asif: Conceptualization, Writing- Original draft preparation
Shah Nawaz: Conceptualization, Writing- Original draft preparation
Zeeshan Ahmad Bhutta: Visualization, Writing, Original draft preparation
Muhammad Fakhar-e-Alam Kulyar: Resources, Writing, Original draft preparation
Muhammad Rashid: Supervision, Writing, Reviewing and Editing
Shafqat Shabir: Project administration, Writing, Reviewing and Editing
Muhammad Kashif Khan: Writing, Reviewing and Editing
Muaaz Qadir: Writing, Reviewing and Editing
The author declares no conflict of interest.
References ![]()
- Bellou M, Kokkinos P, Vantarakis A. Shellfish-borne viral outbreaks: a systematic review. Food and Environmental Virologyl, (2013); 5(1): 13-23.
- Grubaugh ND, Ladner JT, Lemey P, Pybus OG, Rambaut A, et al. Tracking virus outbreaks in the twenty-first century. Nature Microbiology, (2019); 4(1): 10-19.
- Astuti I, Ysrafil. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): An overview of viral structure and host response. Diabetes & metabolic syndrome, (2020); 14(4): 407-412.
- Huang C, Wang Y, Li X, Ren L, Zhao J, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet, (2020); 395(10223): 497-506.
- Sun P, Lu X, Xu C, Sun W, Pan B. Understanding of COVID‐19 based on current evidence. Journal of medical virology, (2020); 92(6): 548-51.
- Adhikari SP, Meng S, Wu Y-J, Mao Y-P, Ye R-X, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infectious Diseases of Poverty, (2020); 9(1): 1-12.
- Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. The Lancet, (2020); 395(10223): 470-473.
- Guo YR, Cao QD, Hong ZS, Tan YY, Chen SD, et al. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak – an update on the status. Military Medical Research, (2020); 7(1): 11.
- Hassan SA, Sheikh FN, Jamal S, Ezeh JK, Akhtar A. Coronavirus (COVID-19): A Review of Clinical Features, Diagnosis, and Treatment. Cureus, (2020); 12(3): 1-7.
- Singhal T. A Review of Coronavirus Disease-2019 (COVID-19). The Indian Journal of Pediatrics, (2020); 87(4): 281-286.
- Cascella M, Rajnik M, Cuomo A, Dulebohn SC, Di Napoli R (2020) Features, Evaluation and Treatment Coronavirus (COVID-19). StatPearls [Internet]: StatPearls Publishing.
- Chan JF-W, Yuan S, Kok K-H, To KK-W, Chu H, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. The Lancet, (2020); 395(10223): 514-523.
- Ding Y, Wang H, Shen H, Li Z, Geng J, et al. The clinical pathology of severe acute respiratory syndrome (SARS): a report from China. The Journal of Pathology: A Journal of the Pathological Society of Great Britain and Ireland, (2003); 200(3): 282-289.
- Singhal T. A Review of Coronavirus Disease-2019 (COVID-19). The Indian Journal of Pediatrics, (2020); 1-6.
- Xu Z, Shi L, Wang Y, Zhang J, Huang L, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. The Lancet respiratory medicine, (2020); 8(4):420-422.
- Adhikari SP, Meng S, Wu YJ, Mao YP, Ye RX, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infectious Diseases of Poverty, (2020); 9(1): 29.
- Gao GF. From “A” IV to “Z” IKV: attacks from emerging and reemerging pathogens. Cell, (2018); 172(6): 1157-1159.
- Zhu N, Zhang D, Wang W, Li X, Yang B, et al. A novel coronavirus from patients with pneumonia in China, 2019. New England Journal of Medicine, (2020); 382: 727-733.
- Cui J, Li F, Shi Z-L. Origin and evolution of pathogenic coronaviruses. Nature reviews Microbiology, (2019); 17(3): 181-192.
- Brian D, Baric R (2005) Coronavirus genome structure and replication. Coronavirus replication and reverse genetics: Springer. pp. 1-30.
- Zaki AM, Van Boheemen S, Bestebroer TM, Osterhaus AD, Fouchier RA. Isolation of a novel coronavirus from a man with pneumonia in Saudi Arabia. New England Journal of Medicine, (2012); 367(19): 1814-1820.
- Mizumoto K, Saitoh M, Chowell G, Miyamatsu Y, Nishiura H. Estimating the risk of Middle East respiratory syndrome (MERS) death during the course of the outbreak in the Republic of Korea, 2015. International Journal of Infectious Diseases, (2015); 397-9.
- Hui DS, Memish ZA, Zumla A. Severe acute respiratory syndrome vs. the Middle East respiratory syndrome. Current opinion in pulmonary medicine, (2014); 20(3): 233-241.
- Assiri A, McGeer A, Perl TM, Price CS, Al Rabeeah AA, et al. Hospital outbreak of Middle East respiratory syndrome coronavirus. New England Journal of Medicine, (2013); 369(5): 407-416.
- Haagmans BL, Al Dhahiry SH, Reusken CB, Raj VS, Galiano M, et al. Middle East respiratory syndrome coronavirus in dromedary camels: an outbreak investigation. The Lancet infectious diseases, (2014); 14(2): 140-145.
- Sha J, Li Y, Chen X, Hu Y, Ren Y, et al. Fatality risks for nosocomial outbreaks of Middle East respiratory syndrome coronavirus in the Middle East and South Korea. Archives of virology, (2017); 162(1): 33-44.
- Petersen E, Pollack MM, Madoff LC. Health-care associate transmission of Middle East respiratory syndrome corona virus, MERS-CoV, in the Kingdom of Saudi Arabia. International Journal of Infectious Diseases, (2014); 29: 299-300.
- Rha B, Rudd J, Feikin D, Watson J, Curns AT, et al. Update on the epidemiology of Middle East respiratory syndrome coronavirus (MERS-CoV) infection, and guidance for the public, clinicians, and public health authorities—January 2015. MMWR Morbidity and mortality weekly report, (2015); 64(3): 61.
- Poutanen SM, Low DE, Henry B, Finkelstein S, Rose D, et al. Identification of severe acute respiratory syndrome in Canada. New England Journal of Medicine, (2003); 348(20): 1995-2005.
- Ofner M, Lem M, Sarwal S, Vearncombe M, Simor A. Cluster of severe acute respiratory syndrome cases among protected health care workers-Toronto, April 2003. Canada communicable disease report= Releve des maladies transmissibles au Canada, (2003); 29(11): 93-97.
- Wong SF, Chow KM, Leung TN, Ng WF, Ng TK, et al. Pregnancy and perinatal outcomes of women with severe acute respiratory syndrome. American journal of obstetrics and gynecology, (2004); 191(1): 292-297.
- Perera R, Wang P, Gomaa M, El-Shesheny R, Kandeil A, et al. Seroepidemiology for MERS coronavirus using microneutralization and pseudoparticle virus neutralization assays reveal a high prevalence of antibody in dromedary camels in Egypt, June 2013. Eurosurveillance, (2013); 18(36): 20574.
- Cotten M, Lam TT, Watson SJ, Palser AL, Petrova V, et al. Full-genome deep sequencing and phylogenetic analysis of novel human betacoronavirus. Emerging infectious diseases, (2013); 19(5): 736.
- Azhar EI, El-Kafrawy SA, Farraj SA, Hassan AM, Al-Saeed MS, et al. Evidence for camel-to-human transmission of MERS coronavirus. New England Journal of Medicine, (2014); 370(26): 2499-2505.
- Perlman S. Another decade, another coronavirus. New England Journal of Medicine, (2020); 382: 760-762.
- Sabir JS, Lam TT-Y, Ahmed MM, Li L, Shen Y, et al. Co-circulation of three camel coronavirus species and recombination of MERS-CoVs in Saudi Arabia. Science, (2016); 351(6268): 81-84.
- Graham RL, Baric RS. Recombination, reservoirs, and the modular spike: mechanisms of coronavirus cross-species transmission. Journal of virology, (2010); 84(7): 3134-3146.
- Memish ZA, Zumla AI, Assiri A. Middle East respiratory syndrome coronavirus infections in health care workers. New England Journal of Medicine, (2013); 369(9): 884-886.
- Drosten C, Meyer B, Müller MA, Corman VM, Al-Masri M, et al. Transmission of MERS-coronavirus in household contacts. New England Journal of Medicine, (2014); 371(9): 828-835.
- team HPAUNCI. Evidence of person-to-person transmission within a family cluster of novel coronavirus infections, United Kingdom, February 2013. Euro surveillance: bulletin Européen sur les maladies transmissibles= European communicable disease bulletin, (2013); 18(11): 20427.
- Brauburger K, Hume AJ, Mühlberger E, Olejnik J. Forty-five years of Marburg virus research. Viruses, (2012); 4(10): 1878-1927.
- Bausch DG, Nichol ST, Muyembe-Tamfum JJ, Borchert M, Rollin PE, et al. Marburg hemorrhagic fever associated with multiple genetic lineages of virus. New England Journal of Medicine, (2006); 355(9): 909-919.
- Towner JS, Khristova ML, Sealy TK, Vincent MJ, Erickson BR, et al. Marburgvirus genomics and association with a large hemorrhagic fever outbreak in Angola. Journal of virology, (2006); 80(13): 6497-6516.
- Slenczka W, Klenk HD. Forty years of marburg virus. The Journal of infectious diseases, (2007); 196(Supplement_2): S131-S135.
- Martina BE, Osterhaus AD. “Filoviruses”: a real pandemic threat? EMBO molecular medicine, (2009); 1(1): 10-18.
- Mekibib B, Ariën KK. Aerosol transmission of filoviruses. Viruses, (2016); 8(5): 148.
- Brainard J, Hooper L, Pond K, Edmunds K, Hunter PR. Risk factors for transmission of Ebola or Marburg virus disease: a systematic review and meta-analysis. International journal of epidemiology, (2016); 45(1): 102-116.
- Park DJ, Dudas G, Wohl S, Goba A, Whitmer SL, et al. Ebola virus epidemiology, transmission, and evolution during seven months in Sierra Leone. Cell, (2015); 161(7): 1516-1526.
- Martini G, Schmidt H. Spermatogenic transmission of the" Marburg virus".(Causes of" Marburg simian disease"). Klinische Wochenschrift, (1968); 46(7): 398.
- Legrand J, Grais RF, Boelle P-Y, Valleron A-J, Flahault A. Understanding the dynamics of Ebola epidemics. Epidemiology & Infection, (2007); 135(4): 610-621.
- Leroy EM, Kumulungui B, Pourrut X, Rouquet P, Hassanin A, et al. Fruit bats as reservoirs of Ebola virus. Nature, (2005); 438(7068): 575-576.
- Piot P, Muyembe J-J, Edmunds WJ. Ebola in west Africa: from disease outbreak to humanitarian crisis. The Lancet Infectious Diseases, (2014); 14(11): 1034-1035.
- Khan AS, Tshioko FK, Heymann DL, Le Guenno B, Nabeth P, et al. The reemergence of Ebola hemorrhagic fever, Democratic Republic of the Congo, 1995. The Journal of infectious diseases, (1999); 179(Supplement_1): S76-S86.
- Leroy EM, Epelboin A, Mondonge V, Pourrut X, Gonzalez J-P, et al. Human Ebola outbreak resulting from direct exposure to fruit bats in Luebo, Democratic Republic of Congo, 2007. Vector-borne and zoonotic diseases, (2009); 9(6): 723-728.
- Brainard J, Pond K, Hooper L, Edmunds K, Hunter P. Presence and persistence of Ebola or Marburg virus in patients and survivors: a rapid systematic review. PLoS neglected tropical diseases, (2016); 10(2): 1-17.
- Rodriguez L, De Roo A, Guimard Y, Trappier S, Sanchez A, et al. Persistence and genetic stability of Ebola virus during the outbreak in Kikwit, Democratic Republic of the Congo, 1995. The Journal of infectious diseases, (1999); 179(Supplement_1): S170-S176.
- Mate SE, Kugelman JR, Nyenswah TG, Ladner JT, Wiley MR, et al. Molecular evidence of sexual transmission of Ebola virus. New England Journal of Medicine, (2015); 373(25): 2448-2454.
- Christie A, Davies-Wayne GJ, Cordier-Lasalle T, Blackley DJ, Laney AS, et al. Possible sexual transmission of Ebola virus—Liberia, 2015. MMWR Morbidity and mortality weekly report, (2015); 64(17): 479.
- Roels T, Bloom A, Buffington J, Muhungu G, Mac Kenzie W, et al. Ebola hemorrhagic fever, Kikwit, Democratic Republic of the Congo, 1995: risk factors for patients without a reported exposure. The Journal of infectious diseases, (1999); 179(Supplement_1): S92-S97.
- Srinivasan A, Burton EC, Kuehnert MJ, Rupprecht C, Sutker WL, et al. Transmission of rabies virus from an organ donor to four transplant recipients. New England Journal of Medicine, (2005); 352(11): 1103-1111.
- Consales C, Bolzan V. Rabies review: immunopathology, clinical aspects and treatment. Journal of Venomous Animals and Toxins including Tropical Diseases, (2007); 13(1): 5-38.
- Gibbons RV. Cryptogenic rabies, bats, and the question of aerosol transmission. Annals of emergency medicine, (2002); 39(5): 528-536.
- Taylor LH, Wallace RM, Balaram D, Lindenmayer JM, Eckery DC, et al. The role of dog population management in rabies elimination—a review of current approaches and future opportunities. Frontiers in Veterinary Science, (2017); 4: 1-15.
- Hammond SA, Walwender D, Alving CR, Glenn GM. Transcutaneous immunization: T cell responses and boosting of existing immunity. Vaccine, (2001); 19(17-19): 2701-2707.
- Warrell M, Warrell D. Rabies and other lyssavirus diseases. The Lancet, (2004); 363(9413): 959-969.
- Hemachudha T, Laothamatas J, Rupprecht CE. Human rabies: a disease of complex neuropathogenetic mechanisms and diagnostic challenges. The Lancet Neurology, (2002); 1(2): 101-109.
- Dietzschold B, Morimoto K, Hooper D, Smith J, Rupprecht C, et al. Genotypic and phenotypic diversity of rabies virus variants involved in human rabies: implications for postexposure prophylaxis. Journal of human virology, (2000); 3(1): 50-57.
- Da Rosa ES, Kotait I, Barbosa TF, Carrieri ML, Brandão PE, et al. Bat-transmitted human rabies outbreaks, Brazilian Amazon. Emerging infectious diseases, (2006); 12(8): 1197.
- Lopez RA, Miranda PP, Tejada VE, Fishbein D. Outbreak of human rabies in the Peruvian jungle. The lancet, (1992); 339(8790): 408-411.
- De Mattos CC, De Mattos CA, Loza-Rubio E, Aguilar-Setién A, Orciari LA, et al. Molecular characterization of rabies virus isolates from Mexico: implications for transmission dynamics and human risk. The American journal of tropical medicine and hygiene, (1999); 61(4): 587-597.
- Schneider MC, Santos-Burgoa C, Aron J, Munoz B, Ruiz-Velazco S, et al. Potential force of infection of human rabies transmitted by vampire bats in the Amazonian region of Brazil. The American journal of tropical medicine and hygiene, (1996); 55(6): 680-684.
- Broder S. The development of antiretroviral therapy and its impact on the HIV-1/AIDS pandemic. Antiviral research, (2010); 85(1): 1-18.
- Faria NR, Rambaut A, Suchard MA, Baele G, Bedford T, et al. The early spread and epidemic ignition of HIV-1 in human populations. science, (2014); 346(6205): 56-61.
- De Bruyn M. Women and aids in developing countries: The XIIth international conference on the social sciences and medicine. Social Science & Medicine, (1992); 34(3): 249-262.
- Herek GM. AIDS and stigma. American behavioral scientist, (1999); 42(7): 1106-1116.
- Varni SE, Miller CT, Solomon SE. Sexual behavior as a function of stigma and coping with stigma among people with HIV/AIDS in rural New England. AIDS and Behavior, (2012); 16(8): 2330-2339.
- Ferguson NM, Keeling MJ, Edmunds WJ, Gani R, Grenfell BT, et al. Planning for smallpox outbreaks. Nature, (2003); 425(6959): 681-685.
- Smith GL, McFadden G. Smallpox: anything to declare? Nature Reviews Immunology, (2002); 2(7): 521-527.
- Enserink M. Biowarfare. Did bioweapons test cause a deadly smallpox outbreak? Science, (2002); 296(5576): 2116-2117.
- Riley S, Ferguson NM. Smallpox transmission and control: spatial dynamics in Great Britain. Proceedings of the National Academy of Sciences, (2006); 103(33): 12637-12642.
- Kaplan EH, Craft DL, Wein LM. Emergency response to a smallpox attack: the case for mass vaccination. Proceedings of the National Academy of Sciences, (2002); 99(16): 10935-10940.
- Tovey D. The Bradford smallpox outbreak in 1962: a personal account. Journal of the Royal Society of Medicine, (2004); 97(5): 244-247.
- Bhatnagar V, Stoto MA, Morton SC, Boer R, Bozzette SA. Transmission patterns of smallpox: systematic review of natural outbreaks in Europe and North America since World War II. BMC Public Health, (2006); 6(1): 126.
- Milton DM. What was the primary mode of smallpox transmission? Implications for biodefense. Frontiers in cellular and infection microbiology, (2012); 2: 1-7.
- Henderson R, Yekpe M. Smallpox transmission in southern Dahomey: a study of a village outbreak. American journal of epidemiology, (1969); 90(5): 423-428.
- Childs JE, Ksiazek TG, Spiropoulou CF, Krebs JW, Morzunov S, et al. Serologic and genetic identification of Peromyscus maniculatus as the primary rodent reservoir for a new hantavirus in the southwestern United States. Journal of Infectious Diseases, (1994); 169(6): 1271-1280.
- Hjelle B, Glass GE. Outbreak of hantavirus infection in the Four Corners region of the United States in the wake of the 1997–1998 El Nino—Southern Oscillation. The Journal of Infectious Diseases, (2000); 181(5): 1569-1573.
- Krüger DH, Ulrich R, Lundkvist Å. Hantavirus infections and their prevention. Microbes and infection, (2001); 3(13): 1129-1144.
- Hofmann J, Meisel H, Klempa B, Vesenbeckh SM, Beck R, et al. Hantavirus outbreak, Germany, 2007. Emerging Infectious Diseases, (2008); 14(5): 850.
- Wells RM, Estani SS, Yadon ZE, Enria D, Padula P, et al. An unusual hantavirus outbreak in southern Argentina: person-to-person transmission? Hantavirus Pulmonary Syndrome Study Group for Patagonia. Emerging Infectious Diseases, (1997); 3(2): 171.
- Wells RM, Young J, Williams RJ, Armstrong LR, Busico K, et al. Hantavirus transmission in the United States. Emerging Infectious Diseases, (1997); 3(3): 361.
- Kallio ER, Klingström J, Gustafsson E, Manni T, Vaheri A, et al. Prolonged survival of Puumala hantavirus outside the host: evidence for indirect transmission via the environment. Journal of General Virology, (2006); 87(8): 2127-2134.
- Rao B. Epidemiology and control of influenza. National medical journal of india, (2003); 16(3): 143-149.
- Tellier R. Review of aerosol transmission of influenza A virus. Emerging infectious diseases, (2006); 12(11): 1657.
- Bridges C, Kuehnert M, Hall C. Transmission of influenza: implications for control in health care settings (vol 37, pg 1094, 2003). Clinical infectious diseases, (2006); 42(5): 737-737.
- Nicas M, Nazaroff WW, Hubbard A. Toward understanding the risk of secondary airborne infection: emission of respirable pathogens. Journal of occupational and environmental hygiene, (2005); 2(3): 143-154.
- Ehelepola NDB, Wijesinghe WMCM. An Analysis of a Dengue Outbreak at a Large Hospital and Epidemiological Evidence for Nosocomial Dengue. Journal of Tropical Medicine, (2018); 2018: 1-9.
- Brady OJ, Gething PW, Bhatt S, Messina JP, Brownstein JS, et al. Refining the global spatial limits of dengue virus transmission by evidence-based consensus. PLoS neglected tropical diseases, (2012); 6(8): 1-15.
- Kuno G. Review of the Factors Modulating Dengue Transmission. Epidemiologic Reviews, (1995); 17(2): 321-335.
- Scott TW, Naksathit A, Day JF, Kittayapong P, Edman JD. A fitness advantage for Aedes aegypti and the viruses it transmits when females feed only on human blood. The American journal of tropical medicine and hygiene, (1997); 57(2): 235-239.
- Thammapalo S, Meksawi S, Chongsuvivatwong V. Effectiveness of space spraying on the transmission of dengue/dengue hemorrhagic fever (DF/DHF) in an urban area of Southern Thailand. Journal of tropical medicine, (2012); 2012: 1-7.
- Gratz NG. EMERGING AND RESURGING VECTOR-BORNE DISEASES. Annual Review of Entomology, (1999); 44(1): 51-75.
- Chen LH, Wilson ME. Transmission of Dengue Virus without a Mosquito Vector: Nosocomial Mucocutaneous Transmission and Other Routes of Transmission. Clinical Infectious Diseases, (2004); 39(6): e56-e60.
- Bowman LR, Donegan S, McCall PJ. Is dengue vector control deficient in effectiveness or evidence?: Systematic review and meta-analysis. PLoS neglected tropical diseases, (2016); 10(3).
- Kroeger A, Nathan M, Hombach J. Focus: dengue. Nature Reviews Microbiology, (2004); 2(5): 360-361.
- Crawford SE, Ramani S, Tate JE, Parashar UD, Svensson L, et al. Rotavirus infection. Nature Reviews Disease Primers, (2017); 3: 1-16.
- Woyessa AB, Abebe A, Beyene B, Tefera M, Assefa E, et al. Rotavirus-associated acute diarrhea outbreak in West Shewa Zone of Oromia Regional State, Ethiopia, 2017. Pan African Medical Journal, (2019); 32: 1-10.
- Lestari FB, Vongpunsawad S, Wanlapakorn N, Poovorawan Y. Rotavirus infection in children in Southeast Asia 2008–2018: disease burden, genotype distribution, seasonality, and vaccination. Journal of Biomedical Science, (2020); 27(1): 66.
- Dennehy PH. Transmission of rotavirus and other enteric pathogens in the home. The Pediatric infectious disease journal, (2000); 19(10): S103-S105.
- Flewett T. Rotavirus in the home and hospital nursery. British medical journal (Clinical research ed), (1983); 287(6392): 568.
- Zhaori G, Fu L, Xu Y, Guo Y, Peng Z, et al. Detection of rotavirus antigen in tracheal aspirates of infants and children with pneumonia. Chinese medical journal, (1991); 104(10): 830-833.
- Keswick B, Pickering L, DuPont H, Woodward W. Survival and detection of rotaviruses on environmental surfaces in day care centers. Applied and Environmental Microbiology, (1983); 46(4): 813-816.
- Pickering LK, Bartlett III AV, Reves RR, Morrow A. Asymptomatic excretion of rotavirus before and after rotavirus diarrhea in children in day care centers. The Journal of pediatrics, (1988); 112(3): 361-365.
- Anderson A, Shwiff S, Gebhardt K, Ramírez AJ, Shwiff S, et al. Economic Evaluation of Vampire Bat (D esmodus rotundus) Rabies Prevention in M exico. Transboundary and emerging diseases, (2014); 61(2): 140-146.
- Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, et al. Estimating the global burden of endemic canine rabies. PLoS neglected tropical diseases, (2015); 9(4).
- Sackey J, Raparla T. Lesotho: The Development, Impact of HIV/AIDS-Selected Issues and Options. World Bank Report, (2000); (21103-LSO).
- Nelson AM. The cost of disease eradication: smallpox and bovine tuberculosis. Annals of the New York Academy of Sciences, (1999); 894(1): 83-91.
- Macfarlane JT, Lim WS (2005) Bird flu and pandemic flu. British Medical Journal Publishing Group.
- Smith RD, Keogh-Brown MR, Barnett T, Tait J. The economy-wide impact of pandemic influenza on the UK: a computable general equilibrium modelling experiment. BMJ, (2009); 339: 1-7.
- Hung TM, Clapham HE, Bettis AA, Cuong HQ, Thwaites GE, et al. The estimates of the health and economic burden of dengue in Vietnam. Trends in parasitology, (2018); 34(10): 904-918.
- Godói IP, Da Silva LVD, Sarker AR, Megiddo I, Morton A, et al. Economic and epidemiological impact of dengue illness over 16 years from a public health system perspective in Brazil to inform future health policies including the adoption of a dengue vaccine. Expert review of vaccines, (2018); 17(12): 1123-1133.
- Bartsch SM, Lopman BA, Ozawa S, Hall AJ, Lee BY. Global economic burden of norovirus gastroenteritis. PloS one, (2016); 11(4): 1-16.
- Joo H, Maskery BA, Berro AD, Rotz LD, Lee Y-K, et al. Economic Impact of the 2015 MERS Outbreak on the Republic of Korea's Tourism-Related Industries. Health security, (2019); 17(2): 100-108.
- Gemechu R. Review on Economic Importance’s of Rabies in Developing Countries and Its Controls. Archives of Preventive Medicine, (2017); 2(1): 15-21.
- Shah M, Risher K, Berry SA, Dowdy DW. The epidemiologic and economic impact of improving HIV testing, linkage, and retention in care in the United States. Clinical infectious diseases, (2016); 62(2): 220-229.
- Lee J-W, McKibbin WJ. Estimating the global economic costs of SARS; 2004. National Academies Press Washington, DC. pp. 92.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


