

Short Communication
Prevalence of MRSA colonization among healthcare-workers and effectiveness of decolonization regimen in ICU of a Tertiary care Hospital, Lahore, Pakistan
Sameena Parveen1, Sheeba Saqib1*, Altaf Ahmed1, 2, Aqeel Shahzad1, Nawal Zarish1, Naveed Ahmed2
Adv. life sci., vol. 8, no. 1, pp. 38-41, November 2020
*- Corresponding Author: Sheeba Saqib (Email: namalik288@gmail.com)
Authors' Affiliations
2. Department of Microbiology, Pakistan Kidney and Liver institute & Research Center (PKLI & RC), Lahore – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The objectives of this study were to evaluate the prevalence of Methicillin Resistant Staphylococcus aureus (MRSA) in the nasal cavity and to determine the effectiveness of decolonization regimen among health care workers working in the Intensive care unit (ICU) at a Tertiary care hospital in Lahore, Pakistan.
Methods: A cross-sectional study was carried out during the period of June, 2018 to August, 2018. A total of 46 healthcare workers were screened to see the prevalence of MRSA in the nasal cavity. Samples from the nasal cavity were collected using sterile swabs, and processed for bacterial cultures. The samples were inoculated on Blood agar and chocolate agar and then incubated at 37℃ for 24 hours. After the incubation period, petri plates were checked for the growth of S. aureus (MRSA). After identification of colonizers, five days decolonization regimen of nasal mupirocin ointment and Chlorhexidine based body wash was used and repeated cultures were done to check the effectiveness of this regimen. IBM SPSS version 25 was used to check the statistically significant relationship between prevalence of MRSA colonization with profession and gender.
Results: Among the total 46 participants, 6 (13%) were found MRSA colonizers, 12 (26.08%) showed Methicillin-Susceptible Staphylococcus aureus (MSSA) and remaining 28 (60.8%) showed no growth of S. aureus. The prevalence of MRSA colonization was found highest in nurses i.e. 66.67%, 16.67% in doctor and 16.67% were in respiratory therapists. The success rate of treatment regimen was 83.33%.
Conclusion: Results of the present study showed that the prevalence of MRSA was high in our setting but effectiveness of decolonization treatment regimen is similar to the worldwide success rate.
Keywords: MRSA; healthcare-workers (HCWs); Colonization; Decolonization
Introduction![]()
Methicillin resistance Staphylococcus aureus (MRSA) is the notorious microorganism causing multi-drug resistance among high-risk patients. Patients, visitors, healthcare workers or any individual may colonizer of MRSA. Therefore, to control the incidence and spread of MRSA infections in healthcare settings various strategies are used as decolonization of MRSA in healthcare workers and patients is effective in reducing the incidence of MRSA. While contact precautions followed over MRSA infected patient can also reduce its spread. The rationale behind this practice is that the MRSA spreads from the hands of HCWS to the patients or between the patients which is the significant source of MRSA incidence and epidemics in chronic healthcare facilities [1,2].
Healthcare workers or patients are decolonized as an effective way to avoid outbreak of MRSA [3,4]. In a previous study 65% success rate of MRSA decolonization was observed in patients after one year of treatment with application of nasal mupirocin ointment, Chlorhexidine based mouthwash and body bath for five days [5]. Another similar study states that the effectiveness of this standardized regimen is dependent on the completion of this treatment course [6,7].
It has been also proven in a study that length of patient stay can be significantly reduced in those patients who were screened and MRSA colonizer were decolonized with mupirocin nasal ointment and Chlorhexidine skin bath [8,9].
The present study was conducted in an intensive care unit with the aim to determine the prevalence of methicillin-resistant MRSA in the nasal cavity of healthcare-workers (HCWs) and to determine the effectiveness of standard decolonization regimen among colonizers.
Methods![]()
Setting and study design
For this cross-sectional study, all the clinical and non-clinical staff working in Intensive care unit of a tertiary care hospital of Lahore, Pakistan was screened to identify the colonizers among them. Nasal swabs were collected from 46 health care workers (HCWs) after taking verbal consent. These healthcare workers included in this study was nurses, doctors, respiratory therapist, housekeeping staff and patient care officers.
Sample collection
Name, gender and profession of the participants were documented and a number was assigned to each participant. The sample from anterior nares were collected by sterile cotton swabs after moistening with sterile water and these samples were immediately sent to microbiology laboratory after marking proper identification by the assigned number.
Microbiology Laboratory work up
The samples were inoculated on blood agar and chocolate agar media and incubated at 37℃ for 24 hours. Based on colony morphology and gram staining, gram positive cocci were isolated. The standard biochemical tests were applied on isolates for the identification of S. aureus. Initially catalase test was performed to identify Staphylococcus species and after that Catalase positive staphylococcus underwent coagulase test to identify S. aureus.
Antibiotic sensitivity pattern determination
To check sensitivity against methicillin cefoxitin disk of 30µg was placed on Mueller-Hinton agar, and plates were incubated for 24 hours. After that sensitivity was checked by considering the sensitivity zone. For cefoxitin a zone of ≥25µg were considered as sensitive and ≤24µg were taken as resistance.
Application of decolonization regimen
Staff identified for MRSA colonization in anterior nares swab was treated with nasal mupirocin ointment and body wash with Chlorhexidine soap for five days. After complete treatment, repeated nasal culture was done and processed as per above stated method.
Statistical analysis
By using statistical tools like Pearson chi square the prevalence of MRSA colonizers in relation to profession and gender was checked for significance.
Ethical Approval
Ethical approval was obtained from the Ethical committee of institute.
Results![]()
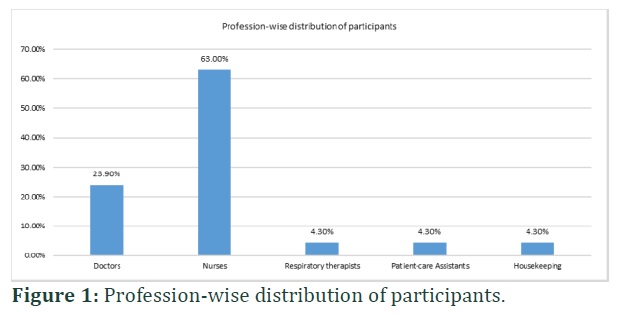
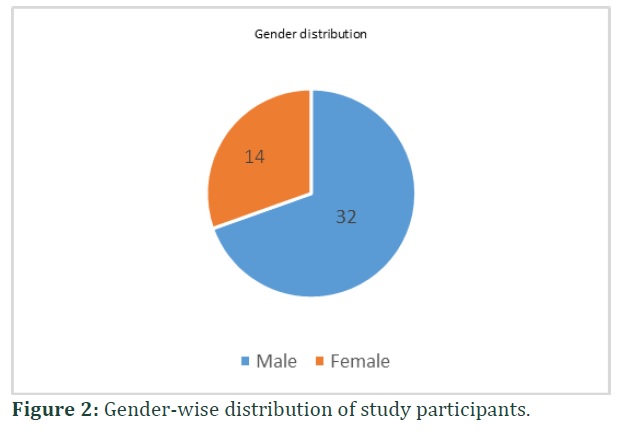
Demographic information of participants is given in below Figure 1 and 2. In ICU staff 23.9% were doctors, 63% were nurses, 4.3% were respiratory therapist, 4.3% patient care assistants and 4.3% housekeeping staff and as shown in below pie chart 69.6% were males and 30.4% were females. Out of 46 participants, 39.13% were carrying Staphylococcus aureus in their nares. Among these Staphylococcus aureus colonizers 8.69% were nurses, 2.17% were doctors and the same percentage was for respiratory therapist while no any patient care assistants or housekeeping staff was colonizer of Staphylococcus aureus.
Sensitivity test of Staphylococcus aureus isolates showed that 66.67% were sensitive to methicillin labeled as MSSA while 33.33% were MRSA. Over all in ICU 60.9% participants were not having Staphylococcus aureus as colonizer in their nares while among colonizer 26.1% were MSSA and 13% were MRSA.
After the application of decolonization regimen in 6 colonizers repeated culture of 5 (83.33%) staff show no growth while one staff (16.67%) show the growth. The staff was investigated about the treatment regimen and it was identified that this staff did not take the proper treatment and due to inconvenience and irritation caused by nasal mupirocin staff stopped the treatment at its own without informing to anyone.
Pearson chi-square was applied to check the prevalence of MRSA and MSSA in relation to gender and profession. It results insignificant p-value 0.529 for profession and 0.943 for gender showing that there is no relation of MRSA or MSSA prevalence with any gender or profession.
Figures & Tables

Discussion![]()
MRSA is involved in multiple infections starting from common infections like skin infections to life threatening infections such as meningitis, kidney failure, lung abscess and endocarditis. It is one of the most common infections encountered in health care settings and result in huge economic burden [7]. Patients with chronic kidney obstruction and liver diseases are immunocompromised and the propensity of them acquiring HAI MRSA is even higher. Thus, it becomes very imperative to analyze the prevalence of MRSA in such patients to introduce early and appropriate antimicrobial therapy [1].
Globally prevalence of MRSA is increasing day by day as in Europe it is 8.7%, 6% in united states and 2.6% in Japan [10] which is far less than the prevalence of MRSA in our setting i.e. 13%. A research study states that among MRSA colonizers in healthcare professionals 10.5% were nurses, 3.8% physician, 1.9% paramedics and 3.6% clerical staff [11] which is relatively high than the prevalence of MRSA in healthcare workers of Pakistan i.e. 8.69% nurses, 2.17% doctor and same for the respiratory therapist. The same study shows 5.1% prevalence of MRSA in intensive care unit while our intensive care unit has 13% prevalence which is higher enough to alarm.
A recent research study in Peshawar, Pakistan about the prevalence of MRSA among healthcare workers and general population states that among 46.80% isolates of MRSA 37.2% were from general population and 62.7% were healthcare workers which is approximately double to the general population [12]. In another study of south region of Punjab, Pakistan shows that there is 9.3% of prevalence of MRSA among healthcare workers of a tertiary care hospital and in this study prevalence was highest among nurses i.e. 10.86%, 6.2% doctors, 3.2% paramedics, and 25% laboratory staff [13]. The findings of our study are closer to the later study of South Punjab but vary markedly from the former study of Peshawar.
Intranasal application of mupirocin ointments is found effective for decolonization of MRSA in nose but it is not effective if the colonizers carry MRSA in multiple body site [14]. Our treatment success rate is 83.33% which is less as compared to another study which shows 87% success rate for standard MRSA decolonization regimen [6].
Limitations
- This study was conducted only in intensive care unit but it must be carried out in all the departments of hospital.
- All the staff must be screened for MRSA colonization at the time of joining the hospital to reduce the risk of MRSA transmission.
- To identify the time dependent effectiveness of regimen, follow up cultures may be taken at different intervals.
This study showed that prevalence of MRSA was greater in healthcare workers of an intensive care unit of tertiary care hospital as compared to other worldwide studies. 13% prevalence of MRSA was identified among healthcare workers and its occurrence was more common among nurses i.e. 8.69%. 83.33% success rate of decolonization regimen was observed among the MRSA colonizers. In order to reduce the MRSA incidence all the healthcare workers and patients must be screened and colonizers must be treated with effective treatment regimen. It will be effective in reducing the disease burden, shortened the length of stay, save direct cost of antibiotic usage and indirect in term of reduced infection rate.
Author Contributions
Conceived and designed the experiments: Sameena Parveen and Altaf Ahmed
Performed the experiments: Naveed Ahmed
Analyzed the data: Aqeel Shehzad, and Sheeba Saqib
Contributed materials/analysis/tools: Aqeel Shehzad and Naveed Ahmed
Wrote the paper: Sameena Parveen, Sheeba Saqib and Naveed Ahmed
Critical Review: Altaf Ahmed
The author declares that there is no conflict of interest regarding the publication of this paper.
Acknowledgment
We are highly thankful to the team of Department of Microbiology, Pakistan Kidney and Liver institute for providing the technical support required for this study especially Mr. Waqas Saleem.
References![]()
- Ahmed N. Gender Based Prevalence of Antibiotic Resistance Patterns in Staphylococcus Aureus. Annals of Life Sciences, (2019); 223-31.
- Shrestha B, Pokhrel BM, Mohapatra TM. Staphylococcus aureus nasal carriage among health care workers in a Nepal Hospital. Brazilian Journal of Infectious Diseases, (2009); 13(5): 322-322.
- Rongpharpi SR, Hazarika NK, Kalita H. The prevalence of nasal carriage of Staphylococcus aureus among healthcare workers at a tertiary care hospital in assam with special reference to MRSA. Journal of Clinical Diagnostic Research, (2013); 7(2): 257.
- Sohail M, Latif Z. Molecular typing of Methicillin Resistance Staphylococcus aureus (MRSA) isolated from device related infections by SCCmec and PCR-RFLP of coagulase gene. Advancements in Life Sciences, (2018); 6(1): 34-40.
- Kohler P, Bregenzer-Witteck A, Rettenmund G, Otterbech S, Schlegel M. MRSA decolonization: success rate, risk factors for failure and optimal duration of follow-up. Infection, (2013); 41(1): 33-40.
- Buehlmann M, Frei R, Fenner L, Dangel M, Fluckiger U, et al. Highly effective regimen for decolonization of methicillin-resistant Staphylococcus aureus carriers. Infection Control Hospital Epidemiology, (2008); 29(6): 510-516.
- Alreshidi MM. Amino acid consumption and secretion patterns of Staphylococcus aureus following growth in sub-optimal environmental conditions. Advancements in Life Sciences, (2020); 7(2): 98-105.
- Kluytmans J, Harbarth S. Methicillin-Resistant Staphylococcus aureus Decolonization “Yes, We Can,” But Will It Help? Infection Control Hospital Epidemiology, (2009); 30(7): 633-635.
- Kumari N, Patoli BB, Patoli AA, Jabeen S. Biocontrol of MRSA and E. coli using bacteriophages from cow manure. Advancements in Life Sciences, (2020); 7(4): 264-269.
- Goyal N, Miller A, Tripathi M, Parvizi J. Methicillin-resistant Staphylococcus aureus (MRSA) colonisation and pre-operative screening. The bone joint journal, (2013); 95(1): 4-9.
- Elie-Turenne M-C, Fernandes H, Mediavilla JR, Rosenthal M, Mathema B, et al. Prevalence and characteristics of Staphylococcus aureus colonization among healthcare professionals in an urban teaching hospital. Infection Control Hospital Epidemiology, (2010); 31(6): 574-580.
- Asghar M, Asghar N, Mumtaz S, Khan SA, Munir AH, et al. Frequency of methicillin resistant staphylococcus aureus (MRSA) colonization amongst hospital staff in teaching hospitals of Peshawar. Journal Of Medical Sciences, (2016); 24(4): 194-198.
- Salman MK, Ashraf MS, Iftikhar S, Baig MAR. Frequency of nasal carriage of Staphylococcus Aureus among health care workers at a Tertiary Care Hospital. Pakistan journal of medical sciences, (2018); 34(5): 1181.
- Boyce J. MRSA patients: proven methods to treat colonization and infection. Journal of Hospital Infection, (2001); 48S9-S14.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0
![]()


