

Review Article
Epidemiology of Obesity in Asia: Challenges and Prevention
Asif Raheem1, Rabia Sultan2*, Humaira Yasmeen2
Adv. life sci., vol. 9, no. 2, pp. 125-130, July 2022
*- Corresponding Author: Rabia Sultan (Email: rabiasultan246@gmail.com)
Authors' Affiliations
2. Department of Microbiology and Molecular Genetics, The Women University Multan – Pakistan
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
Obesity is a complex, multifactorial and largely preventable disease affecting over a third of the world’s population today. In this review, prevalence of childhood and adult obesity, its causes, risk factors, interventions and management in different Asian countries was explored. It has been observed that obesity has grown up as an epidemic and it will intensify in the coming years if appropriate preventive measures are not adopted. Proper policies are needed to be implemented. Additionally, massive nation-wide public awareness programs with better structural infrastructure will be answer to this giant problematic challenge.
Keywords: Asia, body mass index; Obesity; Physical Activity; Prevalence; World Health Organization
Introduction![]()
Obesity is defined as an excess accumulation of adipose tissue in the body to the extent that physical health may be adversely affected [1, 2]. The universality of obesity is globally mounting. World Health Organization (WHO) reported 1.9 billion adults as overweight with 650 million obese. Moreover, more than 340 million children and adolescents between the age of 5 to 19 were found to be obese. Interestingly, about 50% of the overweight children under the age of 5 live in Asia [3, 4]. It is linked to various health problems i.e. diabetes mellitus, dyslipidaemia, hypertension, coronary heart disease, cancer, sleep-breathing disorders, osteoarthritis, cardiovascular disease and asthma [5, 1, 6]. Body weight can be determined by finding the balance between energy consumption and food intake. Less than 0.5% increase in caloric consumption as compared to energy expenditure can cause weight gain [5, 1, 6]. Apart from health problems obesity also leads to psychological and social issues like depression, low self-esteem, social withdrawal, isolation, suicidal thoughts, and suicidal attempts. Obese children due to their physical appearance faces social stigma associated [7]. Obesity in developing countries particularly in Asia is not well documented therefore this review will add knowledge to their prevalence rate in Asian countries. Associated aims were to plot obesity trends over time across the last few decades and to identify and discuss the socio-economic factors associated with obesity in the region [8].
Methods![]()
Literature survey and selection criteria
The data on the prevalence of obesity in Asian countries was gathered by searching different online databases such as PubMed and Google Scholar with the search query of obesity, Asia, prevalence, causes, interventions, diet, lifestyle, management, and risk factors. Some data was also gathered by searching different government and international organizations websites like World Health Organization and Central Intelligence Agency. Articles included were population-based surveys published in a peer-reviewed journal from year 2005 and onwards and those articles that involve survey-based age-specific prevalence reports of obesity..
Prevalence of obesity
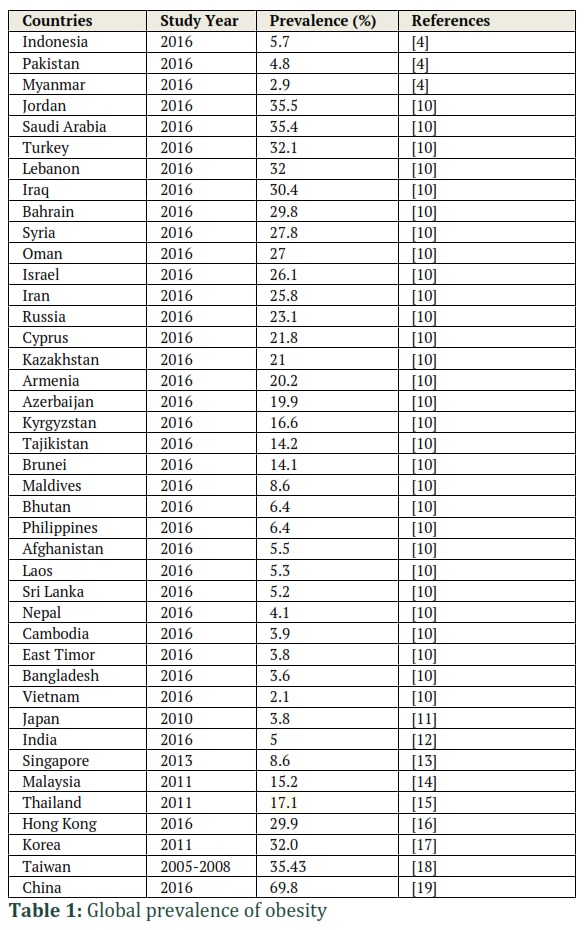
Obesity is prevalent worldwide (table 1). The prevalence of obesity in preschool children has been increasing steadily. In 1990, obesity in Asian preschool children was recorded to be 3.2% equivalent to 12.4 million obese children. In 2010, it increased to 4.9% equivalent to 18 million children and by 6.8% equivalent to 24 million in 2020. Interestingly, in the last 20 years number of obese children in Southeast Asia increased from 1.2 million to 2.5 million [9].
Causes of Obesity
Obesity is multifactorial disorder influenced by genetics, behavior and environmental factors. They may include an imbalance between food intake and physical activity, direct and indirect genetic effects, genetic interaction with the environment, social and physical determinants of health.
i. Behavioral Factors
A healthy behavior incorporates a balanced diet and consistent physical activity. Environment and community also play an important role in someone’s choice to be physically active. For instance, someone might decide not to walk or use bike due to lack of sidewalks or safe bike trails or due to unsafe environment. Some diseases like Cushing’s disease and polycystic ovary syndrome can lead to obesity [20, 21]. Weight change is also affected by personal behaviors like sleep patterns, stress, diet, physical activity. Leisure time activities that do not involve sleep like screen time, television viewing can also contribute to weight gain. A person’s social network also plays an important role in the prevalence of obesity. According to research, the probability of a person’s becoming obese increase by 57% if the said person has a friend who is obese [22].
ii. Dietary Factors
There are many factors that lead to childhood obesity. These factors include consumption of food that is high caloric, dense in fat and sugars but low in healthy nutrients like vitamins, minerals and other micronutrients. Childhood obesity can also be attributed to a sedentary lifestyle, less physical and mechanical activity levels [23]. Bad eating habits and harmful weight regulation routines leads to various eating disorders like binge eating and food addiction are major cause of obesity in adolescents and adults. Leptin is a hormone produced by adipose tissue. The function of leptin is to regulate lipid metabolism but genetic defects in leptin and leptin receptors can lead to obesity in children [24].
iii. Genetic Factors
There is compelling evidence that genetics plays an important role in the onset of obesity. Mutations in melanocortin 4 receptor gene are reported to be linked with obesity [25]. More than 60 genetic markers have been identified which increases the predisposition to becoming obese. There are many genes and gene products that lead to anorexia or satiety because of their ability to influence gut and brain. These genes and gene products include Ghrelin, oxyntomodulin (OXM), carnitine palmitoyltransferase-1 (CPT1), cholecystokinin, adiponectin, β2-adrenoceptor (ADRB2), insulin-induced gene 2 (INSIG2), resistin, syndecan 3 (SDC3), fat mass and obesity-associated (FTO), N-acylphosphatidylethanolamine (NAPE), glucagon-like-peptide-1 (GLP1), peptide YY (PYY), leptin, long-chain fatty acyl-coenzyme A (LCFA-CoA), oleoylethanolamide (OEA), melanocortin-4 receptor (MC4R), neuropeptide Y(NPY) and many others. Several of these biomarkers are linked to obesity-associated traits, even they are not quite linked to obesity [26].
iv. Environmental and Social Factors
Economic development, increased accessibility to cheap and low nutrient food, industrialization, mechanical transport and urbanization are the kind of changes that lead to obesity [21]. Social determinants of health include the environment in which a person is born, bred and lives, socioeconomic status while physical determinants of health comprise of greenery and additional components of natural environment like parks, buildings, sidewalks, schools, recreation facilities, recreation programs, and worksites [27].
Preventive Measures
For the prevention of obesity, dietary principles and physical activity strategies as recommended by the Dietary Guidelines for Americans should be followed. According to these guidelines, a healthy diet should include vegetables, fruits, whole grains, low-fat or fat-free dairy products, lean protein, and drinking water. Physical activity recommendations include moderately intense activity for a minimum of 150 minutes or a vigorously intense activity of 70 minutes. This physical activity regimen should be accompanied by two days of strength training in one week. This physical activity and dietary patterns also help in maintaining long-term health by preventing chronic diseases like Type 2 diabetes and heart disease [20]. Use of certain food components should be reduced. These components include limiting the consumption of sodium to less than 2,300 mg. People who are above the age of 50, should reduce the intake of sodium to 1500 mg. Consumption of calories from saturated fatty acids should be reduced to less than 10% of the total calories. Instead of saturated fatty acids, monounsaturated and polyunsaturated fatty acids should be used. Consumption of dietary cholesterol should be reduced to 300 mg per day [22, 26, 28]. Intake of trans fatty acid should be kept at the lowest possible level. This can be achieved by off-putting the foods that contain synthetic sources of trans fats, for example partially hydrogenated oils and solid fats. Consumption of added sugars should also be reduced. In the case of alcohol consumption, intake of alcohol should be in moderate limits. Moderate limits mean one drink for women in a day and two drinks for men in a day. Aside from decreasing the consumption of the above-mentioned food components, there are certain foods and food components whose consumption should be increased. These foods include fruits and vegetables [2,6,8,18]. A large selection of vegetables should be consumed including dark-green, red, orange vegetables, beans and peas. Grains should be used as whole grains. Fat-free dairy products should be consumed. Consumption of proteinaceous foods like poultry, seafood, eggs, lean meat, soy products, unsalted nuts, and seeds should be increased. Instead of using proteins foods that contain high amounts of solid fats and calories, the foods that contain a low amount of solid fats and calories should be used. Solid fats should be exchanged with oil. In short, foods which contain more potassium, dietary fiber, calcium, and vitamin D should be consumed [16, 28].
Management of Obesity
Educating the patient about the obesity-associated disease, weight loss expectations, goal setting, suitable dietary changes and modifications in physical activity levels is very important in the management of obesity. Many conditions like mood disorders, low self-esteem and poor quality of life can be found in obese people which should be identified and carefully managed. To achieve weight loss, the advantages of weight loss should be emphasized [21, 23]. Patients should be apprised about realistic weight loss expectations and weight loss goals setting. Many people tend to gain weight after the first year of weight loss. So, Significance of lifestyle modifications and maintenance of those modifications should be discussed with the patient. The patient should be made aware of the fact that Asian Indian foods contain total fat, trans fat, carbohydrates, saturated fat, monounsaturated fatty acids (MUFA) and polyunsaturated fatty acids (PUFA) in high amounts. These foods are also low in fiber. Physical activity levels of the patients should be evaluated, and appropriate recommendations should be made [27,29]. Obesity management is essentially entwined with behavior modifications. Medication and surgery play a small role in dealing with obesity, but the management of obesity essentially hinges on food consumption and the extent of physical activity [26]. Another strategy to deal with obesity is intermittent fasting [30]. In intermittent fasting, the period of food intake is limited to a specific time frame like not eating during the night. Research shows that intermittent fasting is an effective strategy not only for weight loss but also for dealing with other diseases [31].
Interventions
i. Therapeutic Interventions
Aside from the usual mode of treatments like diet modification, physical activity and behavioral changes, several medical and surgical options are also accessible for the treatment of obesity. Surgical weight loss options include Roux-en-Y gastric bypass (RYGB), laparoscopic sleeve gastrectomy (LSG) and Fecal microbiota transplantation (FMT). Roux-en-Y gastric bypass changes brain and gut interaction to facilitate weight loss. While FMT includes transplantation of a fecal suspension from a healthy donor into the gastrointestinal (GI) tract of the recipient. Certain weight loss drugs are also available that can be used to prevent fat absorption and inhibit appetite. These drugs include Lorcaserin, Contrave, Xenical and Qsymia. Xenical is a fat absorption inhibitor which works by inhibiting lipase and as a result fat absorption decreases by 30%. Lorcaserin, Contrave, and Qsymia effect the central nervous system as an appetite suppressant. The use of these drugs is not without certain side effects. By far the most successful long-term solution of obesity is Roux-en-Y gastric bypass [24].
ii. Physical Interventions
Increasing physical activity is an important tool while dealing with childhood obesity. For this purpose, the promotion of active travel to school is extremely important. Active travel to school can include cycling and walking. This practice is being promoted in various developing countries. Japan is a country where the prevalence of childhood obesity is at its lowest. The reason behind this is walking to school culture of Japan. To make walk to school culture sustainable in Japan many factors and policies were taken into consideration. Schools are available within walking distances. Strict security and safety measurements were put in place. School or local board of education oversees these security measures. In Japan children are advised to take basic precautions like having a personal alarm, moving in groups, traveling through well lighted and busy area, how to respond when feeling threatened and being approached by a stranger, not getting into a car or any area with a with a stranger and sharing location with their parents. Likewise, it is true for elder people as well [23].
Recommendations
There are several strategies that can be used to prevent and fight obesity. Parents should establish a routine to walk their children [23]. People should be educated to maintain a minimum of 30-45 minutes of physical activity routine for no less than five days a week. The curriculum should include information on the nutritious value of food, good food habits, and a healthy lifestyle. Different sectors of society like the food industry, education department, and the media should play their role in solving this problem of childhood obesity [32]. Moreover, healthy lunch menu should be set up with the help of parents, school principal, teachers and shopkeepers [18].
Conclusion
Obesity is one of the most important public health problems in Asia. Suitable preventive measures and policies should be implemented by the governments to deal with this problem before it gets out of hand. Small effort in reducing obesity may bring long term positive effects. Nevertheless, high-quality studies examining the effectiveness of interventions are needed, especially studies that examine the characteristics of the components contributing to the effectiveness of the interventions.
Author Contributions
The authors declares that there is no conflict of interest regarding the publication of this paper.
References
- Lisco G, De Tullio A, Guastamacchia E, Triggiani V. Fixed-ratio combinations of basal insulin and GLP-1RA in the management of type 2 diabetes mellitus: highlights from the literature. Endocrine, Metabolic and Immune Disorders-Drug Targets (Formerly Current Drug Targets-Immune, Endocrine and Metabolic Disorders), (2021); 21(4): 626-646.
- Sly PD, Trottier B, Carpenter D, Cha’on U, Cormier S, Galluzzo B, Suk WA. Children’s environmental health in South and Southeast Asia: Networking for better child health outcomes. Annals of Global Health, (2019); 85(1).
- Tam BT, Morais JA, Santosa S. Obesity and ageing: Two sides of the same coin. Obesity Reviews, (2020); 21(4): e12991.
- Organization, W. H.O (2021, 9 June 2021). Obesity and overweight. Retrieved from http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
- Smith J, Ayre J, Jansen J, Cvejic E, McCaffery KJ, Doust J, Copp T. Impact of diagnostic labels and causal explanations for weight gain on diet intentions, cognitions and emotions: An experimental online study. Appetite, (2021); 167: 105-612.
- Nakamura C, Ishii A, Matsuo T, Ishida R, Yamaguchi T, Takada K, Yoshikawa T. Neural effects of acute stress on appetite: a magnetoencephalography study. PloS One, (2020); 15(1): e0228039.
- Ran G, Liu J, Niu X, Zhang Q. Associations between Social Withdrawal and Peer Problems in Chinese and North American Youth: A Three-level Meta-analysis. Journal of Child and Family Studies, (2021); 1-12.
- Garrido-Miguel M, Cavero-Redondo I, Álvarez-Bueno C, Rodríguez-Artalejo F, Moreno LA, Ruiz JR, Martínez-Vizcaíno V. Prevalence and trends of overweight and obesity in European children from 1999 to 2016: a systematic review and meta-analysis. JAMA Pediatrics, (2019); 173(10): e192430-e192430.
- Pengpid S, Peltzer K. Overweight or obesity and related lifestyle and psychosocial factors among adolescents in Brunei Darussalam. International Journal of Adolescent Medicine and Health, (2020); 32(6).
- CIA. (2016). The world factbook obesity – adult prevalence rate. Retrieved from https://www.cia.gov/library/publications/the-world-factbook/fields/2228.html
- Watanabe J, Kotani K. Metabolic syndrome for cardiovascular disease morbidity and mortality among general Japanese people: a mini review. Vascular Health and Risk Management, (2020); 16: 149.
- Biradar RA, Singh DP. Spatial clustering of diabetes among reproductive age women and its spatial determinants at the district level in southern India. Clinical Epidemiology and Global Health, (2020); 8(3): 791-796.
- Chen KK, Wee SL, Pang BWJ, Lau LK, Jabbar KA, Seah WT, NgTP. Relationship between BMI with percentage body fat and obesity in Singaporean adults–The Yishun Study. BMC Public Health, (2021); 21(1): 1-9.
- Hidrus A, Kueh YC, Norsaádah B, Chang YK, Hung TM, Naing NN, Kuan G. Effects of brain breaks videos on the motives for the physical activity of Malaysians with type-2 diabetes mellitus. International Journal of Environmental Research and Public Health, (2020); 17(7): 2507.
- Kriengsinyos W, Chan P, Amarra MSV. Consumption and sources of added sugar in Thailand: a review. Asia Pacific Journal of clinical nutrition, (2018); 27(2): 262-283.
- Center for Health Protection. (2019). Non-Communicable Diseases and Healthy Living: Obesity. Retreived from https://www.chp.gov.hk/en/healthtopics/content/25/8802.html
- Ha KH, Lee YH, Song SO, Lee JW, Kim DW, Cho KH, Kim DJ. Development and validation of the Korean diabetes risk score: a 10-year national cohort study. Diabetes and Metabolism Journal, (2018); 42(5): 402-414.
- Chang A, Schulz PJ, Jiao W, Liu MT. Obesity-Related Communication in Digital Chinese News From Mainland China, Hong Kong, and Taiwan: Automated Content Analysis. JMIR Public Health and Surveillance, (2021); 7(11): e26660.
- Motevalli M, Drenowatz C, Tanous DR, Khan NA, Wirnitzer K. Management of childhood obesity—Time to shift from generalized to personalized intervention strategies. Nutrients, (2021); 13(4): 1200.
- CDC. (2018). Adult Obesity Causes & Consequences. Retrieved from https://www.cdc.gov/obesity/adult/causes.html
- Suglia SF, Shelton RC, Hsiao A, Wang YC, Rundle A, Link BG. Why the neighborhood social environment is critical in obesity prevention. Journal of Urban Health, (2016); 93(1): 206-212.
- Meldrum DR, Morris MA, Gambone JC. Obesity pandemic: causes, consequences, and solutions—but do we have the will?. Fertility and Sterility, (2017); 107(4): 833-839.
- Tanaka C, Tanaka S, Inoue S, Miyachi M, Suzuki K, Abe T, Reilly JJ. Results from the Japan's 2018 report card on physical activity for children and youth. Journal of Exercise Science and Fitness, (2019); 17(1): 20-25.
- Karri S, Sharma S, Hatware K, Patil K. Natural anti-obesity agents and their therapeutic role in management of obesity: A future trend perspective. Biomedicine and Pharmacotherapy, (2019); 110: 224-238.
- Aris I M, Rifas-Shiman SL, Li LJ, Kleinman KP, Coull BA, Gold DR, Oken E. Patterns of body mass index milestones in early life and cardiometabolic risk in early adolescence. International Journal of Epidemiology, (2019); 48(1): 157-167.
- Mohamad Nor NS, Ambak R, Mohd Zaki N, Abdul Aziz NS, Cheong SM, Abd Razak MA, Aris T. An update on obesity research pattern among adults in Malaysia: a scoping review. BMC Women's Health, (2018); 18(1): 5-15.
- Fujita K, Hayashi T, Matsushita M, Uemura M, Nonomura N. Obesity, inflammation, and prostate cancer. Journal of Clinical Medicine, (2019); 8(2): 201.
- CNPP. (2020). Dietary guidelines for americans 2015-2020 Retrieved from https://health.gov/sites/default/files/2019-09/2015-2020_Dietary_Guidelines.pdf
- Chopra S, Malhotra A, Ranjan P, Vikram NK, Singh, N. Lifestyle-related advice in the management of obesity: a step-wise approach. Journal of Education and Health Promotion, (2020); 9.
- Cho Y, Hong N, Kim KW, Cho SJ, Lee M, Lee YH, Lee BW. The effectiveness of intermittent fasting to reduce body mass index and glucose metabolism: a systematic review and meta-analysis. Journal of Clinical Medicine, (2019); 8(10): 1645.
- Stekovic S, Hofer SJ, Tripolt N, Aon MA, Royer P, Pein L, Madeo F. Alternate day fasting improves physiological and molecular markers of aging in healthy, non-obese humans. Cell Metabolism, (2019); 30(3): 462-476.
- Gautam S, Jeong HS. Childhood obesity and its associated factors among school children in Udupi, Karnataka, India. Journal of Lifestyle Medicine, (2019); 9(1): 27.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0


