

Full Length Research Article
Biofilm Forming Bacteria Isolated from Medical Implants
Aimen Fatima, Mahwish Batool Kazmi, Humaira Yasmeen*
Adv. life sci., vol. 8, no. 3, pp. 251-256, July 2021
*– Corresponding Author: Humaira Yasmeen (Email: humaira.6127@wum.edu.pk)
Authors' Affiliations
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Biofilm formation in indwelling medical devices poses serious risk of infection and increases the likelihood of recurrence of infections. The study was carried out to identify the microbes which form biofilms on medical implants and are thus involved in nosocomial infections, to assess the potential of biofilm producing ability of these isolated microbes and to determine antibiotic resistance towards ampicillin, vancomycin ceftazidime, streptomycin and tetracycline.
Methods: For this, 11 samples of 5 different implants were taken from Tertiary Care Hospital Multan, Pakistan. Bacteria were isolated and identified by culture plate method. Tryptone soy broth (TBS) media was used for biofilm development by microbes in plastic tubes. Developed biofilm in tubes was visualized with crystal violet staining method and then biofilm forming potential was estimated by measuring the optical density through spectrophotometer. Antibiotic susceptibility was done by Kirby Bauer disk diffusion method to determine the resistance and susceptibility pattern of biofilm producers.
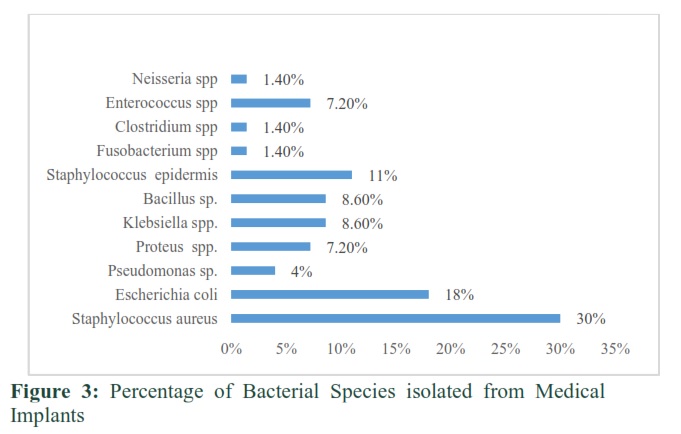
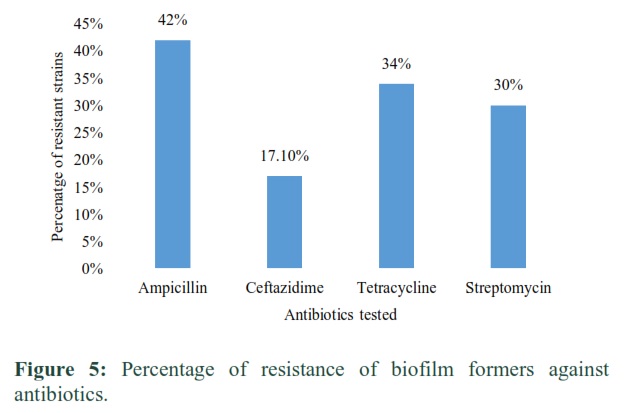
Results: Out of 11 different samples of indwelling medical devices, a total of 131 bacterial strains were isolated. The percentage of bacterial isolates which produced biofilms were Staphylococcus spp. (41%) followed by Escherichia coli (18%), Pseudomonas spp. (4%), Proteus spp. (7.2%), Klebsiella spp. (8.6%), Bacillus spp. (8.6%), Fusobacterium spp. (1.4%) Clostridium spp.(1.4%), Enterococcus spp. (7.2%) and Neisseria spp. (1.4%). Sixty-nine isolates were considered positive for biofilm formation while 58 were considered negative. The resistance was maximum against ampicillin (42%) followed by ceftazidime (17.1%), tetracycline (34%) and streptomycin (30%) while against vancomycin no resistance was observed.
Conclusion: Biofilms produced on medical implants by different bacteria are considered to be the major cause of hospital acquired infections and are very difficult to eradicate. These biofilms associated implant infections are challenging to treat because of their resistance towards various antibiotic therapies. Therefore, some efficient methods of prevention of biofilm formation should be introduced.
Keywords: Bacterial biofilms; Biofilm associated infections; Medical implants; Hospital acquired infections; Antibiotic resistance
Introduction![]()
Biofilms are defined as an aggregate of microorganisms in which the microbial cells attach irreversibly to each other or to living or non-living surfaces to form self-organized communities. The cells in these complex communities are embedded in an adhesive matrix made up of the extracellular polymeric substances (EPS) that are produced by the cells in the community [1].The EPS matrix is an insoluble and oily secretion composed of polysaccharides, proteins and nucleic acids [2]. This matrix encapsulates the cells residing in a biofilm, alters their phenotype by changing growth rates, gene regulation and therefore enables them to withstand harsh environmental conditions by seizing and captivating nutrients from the environment [3]. EPS also prevents the incorporation of antimicrobial drugs and increases microbial tolerance against drugs [4]. Microbes living in a biofilm have adopted several modifications with which they have become more resistant [5]. They have altered their phenotype and have modified their enzymatic activity and have acquired a mutated genotype that includes more resistant genes which makes them resistant to antimicrobials [6]. The cells in a biofilm communicate with each other with the help of different biochemical signals, this cell to cell interaction is known as quorum sensing [7]. During biofilm formation the attachment of cells to the substratum is facilitated by adhesin proteins; formation of macro colony and finally dissemination of bacterial cells [8].
Now-a-days medical implants are used in almost every health care facility, so a number of medical devices are used on daily basis. The bacteria which produce biofilms are often opportunistic and often colonize the available implants such as urinary catheter, intravascular catheter, central venous catheter and endotracheal tube. The encrustation of microbes in medical implants may lead to nosocomial infection [9]. Nosocomial infections may occur repeatedly because these microbes form complex colonies and have developed antibiotic resistance. The leading cause of nosocomial infection is biofilm formation in medical devices. Bacteria producing biofilms on medical device surfaces pose great risk of infection to the patients using these medical implants. Pathogens responsible of nosocomial infection might also come from patients own natural flora depending upon the type of implant used by the patient. Hospital staff and surrounding environment also plays important role in the spread of these bacteria [10]. Due to this reason biofilms are associated with 65% of nosocomial infections [11]. Indwelling medical devices, such as prosthetics, catheters and several other may have helped a lot hospital acquired infections, but they still pose a greater risk of infection [12]. Certainly, implant colonization causes the most recurrent and severe infection associated when biomaterial is used. The association of the pathogen , biomaterial and the host defense system plays important role in implant infection [13]. Host immune systems remove the tissue infections caused by opportunistic pathogens without generation of an immune response by the entry of a foreign body. Whereas in implant associated infection an immune response is generated by the biomaterial of the implant. The infection can be acute and, a foreign body infection or tissue granulation. As a result of this a series of immune depression takes place which helps microbes to colonize the invasive device and cause infection [14] The aims of this research were to characterize common bacterial strains contaminating the medical implants, to evaluate their potential to produce biofilm and to determine antibiotic susceptibility of the isolates.
Methods![]()
Sample Collection and Bacterial Characterization
Different samples of indwelling medical implants (Urinary Catheter, Central Venous Catheter, Intravascular Catheter Foley’s Urinary Catheter Endotracheal Tubes, Stomach Drains and Nasopharyngeal Tube) were collected in sterile polythene bags under sterile conditions and transported to the lab within 2-3 hours. All samples were collected from different wards of Tertiary Care Hospital Multan after consent. Samples were specifically collected from one week or before from old patients who had been catharized and were suffering from nosocomial infections during their stay at hospital. Approval for this study was obtained from the Ethical committee of Nishtar Medical College and Hospital Multan, Pakistan. Informed consents were obtained from the participants or their guardians before sample collection. All medical implants were cut into 2-3 cm long and thick discs or tubes and placed in sterile beakers filled with phosphate buffer saline (PBS) solution. Samples in PBS were stored in refrigerator at 4˚C for 24 hours. Sample discs or tubes were also placed directly on the surface of the culture media and plates were placed in incubator at 37˚C for 24 hours. Following incubation, the distinct colonies were furthered processed on nutrient agar and MacConkey agar and biochemically characterized using Bergey's manual of systematic bacteriology.
Biofilm Formation and Quantification
Tube method (TM) was used to detect microbial biofilm production. Three ml tryptone soy broth (TSB) was placed in sterile glass tubes. TSB media tubes were inoculated with loopful colony of each isolated strain and were incubated at 37˚C for 24 hours. After 24 hours, 2 ml of 2% glucose was added in each TSB test tube and was again incubated for 24 hours at same temperature. After total incubation of 48 hours, TSB growth media was discarded, and the test tubes were washed thrice aseptically with phosphate saline buffer (PBS) of pH 7.4 to remove any unbound bacteria. After washing with PBS, the remaining attached microbes were then fixed by using 3 ml of 99% methanol and tubes were left for 15 minutes. After that, methanol was discarded. The tubes were left for drying. In order to observe biofilm production by microorganisms, each test tube was stained with 0.3 ml of 0.1% crystal violet for 5-6 minutes. After 5-6 minutes, the test tubes were washed carefully with running tap water in order to remove the excess stain. Once the excess stain was removed, the tubes were left to dry by placing them in inverted position. After air drying the tubes dyed adherent cells were solubilized by using 33% glacial acetic acid. 1.5 ml glacial acetic acid was added in each test tube and optical density was measured at 570 nm using spectrophotometer. The blank for each test tube was phosphate saline buffer PBS [10].
Antimicrobial Susceptibility Assay
Purified strains were tested against a panel of 5 antibiotics namely Ampicillin (10 µg), Ceftazidime (30 µg), Streptomycin (10 µg), Tetracycline (30 µg) and Vancomycin (10 µg) for detection of resistant strains by Kirby Bauer disk diffusion method. Diameter of zone of inhibition was calculated in millimeters. If the zone of inhibition was present around the disc, it showed that bacteria were sensitive to tested antibiotic while the absence of zone formation showed that the bacteria were resistant. The zones were measured and strains were categorized according to Clinical and Laboratory Standards Institute (CLSI) guidelines [15].
Results![]()
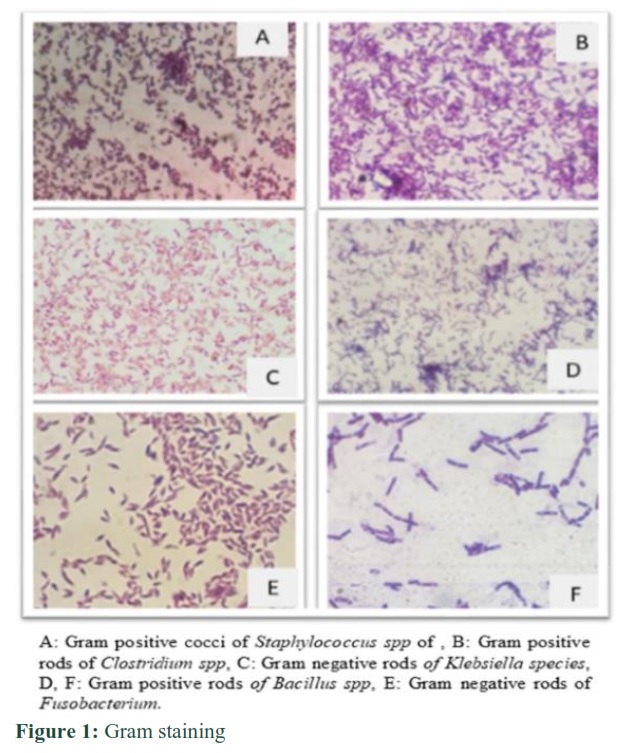
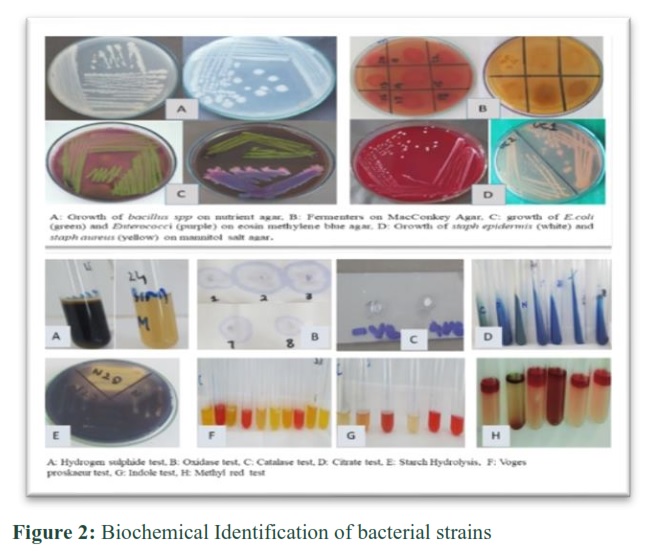
A total of 131 bacterial strains from fifteen different samples of indwelling medical implants, were isolated. The isolated strains were identified by culture plate method, gram staining and biochemical testing system according to Bergey’s manual of determinative bacteriology as shown in the Figure number 1 and Figure 2 respectively.
Biofilm Formation
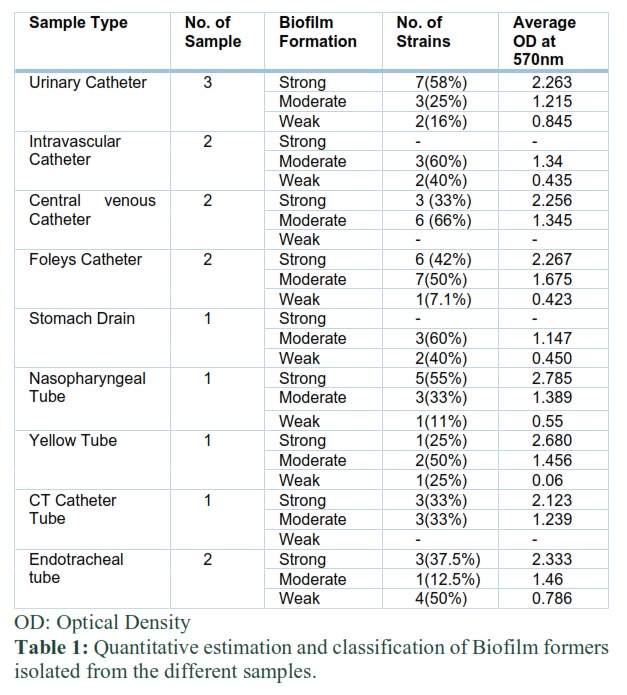
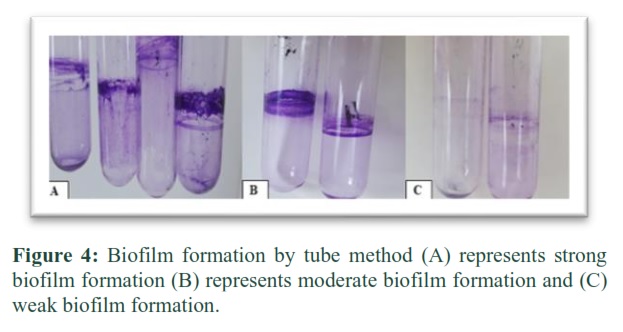
Out of 131 isolates 69 (52.7%) strains were considered biofilm former. Strains were classified as strong, moderate and weak biofilm formers based on crystal violet stain formation (Figure 3). Quantitative estimation of biofilm producer was OD=2×ODc for Weak, moderate by 2×ODc≤4×ODc and for strong biofilm former by OD≥4×ODc. Isolates from urinary catheters were the strongest biofilm producers (58%) while from Endotracheal tube weak biofilm formers (50%) were observed (table 1).
Antibiotic Susceptibility Assay
Antibiotic susceptibility testing was performed on specific strains on the basis of the differences in their colony morphology, and biochemical testing. Antibiotic testing was performed only on those strains which showed biofilm production. Percentage of isolates showing resistance to ampicillin, streptomycin, tetracycline, ceftazidime (figure 5). Vancomycin was susceptible to all tested isolates.
Figures & Tables
Discussion![]()
In this current study samples from urinary catheter, central venous catheter, intravascular catheter and Foley’s urinary catheter were aseptically collected from different wards of Tertiary Care Hospital Multan to evaluate tentative biofilm forming microbes colonizing these samples. Three samples of urinary catheter were collected from patients that were catherized for more than 4 days approximately. The catheters from patients suffering from urinary tract infections were collected and then processed for isolation of biofilm forming bacteria. The urinary catheter samples were from 7 days’ old admitted patients. All the samples of endotracheal tubes were collected from patients who had been on ventilator for more than 5 days [16]. The tubes were contaminated with biofilm forming bacteria which were main cause of ventilator associated pneumonia (VAP) as it was found that there is a relationship between colonization of endotracheal tube and nosocomial infections [17]. Examination of biofilm that was detached from the samples was found to harbor groups of microbial communities. An assessment of the different bacteria that produced the biofilm showed that the Staphylococcus spp. (41%) had the highest incidence followed by Escherichia coli (18%), Pseudomonas spp. (4%), Proteus spp. (7.2%), Klebsiella spp. (8.6%), Bacillus spp. (8.6%), Fusobacterium spp. (1.4%), Clostridium spp. (1.4%), Enterococcus spp. (7.2%) and Neisseria spp. (1.4%) [18].
Among all the 69 bacterial strain, 28 (40%) isolates were strong biofilm producing bacteria, 32 (46%) were moderate and 09 (13%) were weak biofilm producing bacteria (Figure 4). Among medical implants urinary catheter and Foley’s catheter were highly contaminated with Staphylococcus aureus (30%) and Escherichia coli (18%) respectively. For detection of biofilms crystal violet staining was done. 0.1% crystal violet solution was used to stain test tubes for 5 minutes, washed with water and dried. On contrary in a study the concentration of CV used was 2% for 5 minutes [10]. Optical density at 570 nm was measured for quantification of biofilm production. OD values equal to 2 were considered strong, less than 2 but more than 1 were considered moderate and OD values less than 1 were considered weak. In a similar study optical density values less than 0.120 were considered weak biofilm producer, 0.120 – 0.240 was moderate and greater than 0.240 were strong biofilm producers. Number of strong, moderate and weak biofilm producers was 28, 32 and 09 respectively [19]. Similarly in a study 25 strong biofilm producers , 21 moderate and 4 weak biofilm producers were isolated [20]. In the current study, 15 strains are isolated from endotracheal tube (ETT) samples and 8 showed the ability of forming biofilm. Mostly the strains isolated were species of Staphylococci spp. (62.5%), E.coli (18%) and Enterococci spp. (12.5%) which is in good agreement to another study where the percentage of endotracheal tube contamination was very high, consisting of S. epidermidis (37.1%) followed by E. coli (27.1%), K. pneumoniae (15.7%), S. aureus (11.4%), E. faecalis (4.2%) and P. aeruginosa (4.2%). But contrary to a study endotracheal tube was colonized by Acinetobacter, Pseudomonas and Klebsiella species. These species were dominant bacterial isolates followed by E. coli [21]. One sample of ETT did not have any microbe that could produce biofilm because the patient from whom the sample was taken was given antibiotic treatment. Biofilm can be prevented in cases when someone was given a systemic digestive decontamination treatment [22]. Biofilm formation on endotracheal tubes was associated with the presence of airway passage microbes. These microbes were able to colonize endotracheal tube and became the reason of ventilator associated pneumonia [23]. It was noted that using bacterial filters during intubation may prevent thick accumulation of microbes and hence may prevent biofilm formation in endotracheal tube [24]. Central venous catheters were collected from ICU patients. These catheters are made-up of silicone tubing and are inserted percutaneously. Catheter samples were collected from patients who had been catherized for more than 15 days suffering from bacteremia and the percentage of contamination with microbes was 40%. The microbes isolated from these samples were mostly opportunistic flora which indicates that the catheter could be contaminated while inserting the catheter into the skin i.e. microbes from the body or skin colonized the outer layer of catheter and caused infection. It was reported that contamination of central venous catheter mostly occurs due to skin microflora [24].
The bacterial strains that were isolated in this study were mostly found in patients GIT or were normal human micro flora. A study reported that these indwelling medical plants were mostly colonized by microbes that are normal inhabitants of the skin which migrate from the skin and accumulate on the outside surface of intravascular catheters thereby multiplying on the other surface making complex colonies and form biofilms [10].These implants colonized by microbes are responsible for causing urinary tract infections, ventilator associated pneumonia and bloodstream infections etc [20]. Development of biofilms on invasive devices is usually due to coagulase negative Staphylococci [25]. Staphylococci being a member of natural skin flora allowed catheters to be colonized by them and provides favorable environment for their growth and dissemination of infections. In tube method of biofilm formation, out of 131 bacterial strains only 69 (52%) strains were considered as biofilm producers while 62(47%) strains were considered non-biofilm producers whereas 76 biofilm producers and 103 non biofilm formers were isolated by tube method in an another study [26]. In this study antibiotic susceptibility of the biofilm producers was checked [27]. Antibiotic susceptibility testing was performed on biofilm producing strains. None of the strain showed resistance against vancomycin. However, 56 strains were resistant against ampicillin, 45 were resistant against tetracycline, 40 against streptomycin and 02 were against Ceftazidime (Figure 3). Similarly, 80 % of strains were resistant to ampicillin [28] and no strain was resistant vancomycin [20]. In this study, 45 strains were resistant against tetracycline whereas in a study tetracycline showed resistance to all of the gram positive biofilm producing isolates [29]. Due to persistent infections the bacterial biofilms are almost resistant to conventional antibiotic therapies. This property aids in dissemination of resistant genes and characteristics in organisms involved in biofilm formation [30].
Biofilm formers isolated from medical implants had shown resistance towards commonly used antibiotics. Therefore, efficient methods for preventing biofilm formation on medical implants are needed.
Author Contributions
AF: Performed research work and drafted manuscript; MB: Design and supervised the research work, reviewed manuscript; HY: supervised the research work, reviewed manuscript.
The authors declare that they have no conflict of interests in this work.
References![]()
- Flemming HC, Wingender J. The biofilm matrix. Nature review microbiology, (2010); 8(9): 623-633.
- Azeredo J, Azevedo NF, Briandet R, Cerca N, Coenye T, Costa AR, Desvaux M, Di Bonaventura G, Hébraud M, Jaglic Z, Kačániová M, Knøchel S, Lourenço A, Mergulhão F, Meyer RL, Nychas G, Simões M, Tresse O, Sternberg C. Critical review on biofilm methods. Critical reviews in microbiology, (2017); 43(3): 313-351.
- Flemming HC, Neu TR, Wozniak DJ. The EPS matrix: the “house of biofilm cells. Journal of bacteriology, (2007); 189(22): 7945.
- Stewart PS. Mechanisms of antibiotic resistance in bacterial biofilms. International journal of medical microbiology, (2002); 292(2): 107-113.
- Yin W, Wang Y, Liu L, He J. Biofilms: The microbial “protective clothing” in extreme environments. International journal of molecular sciences, (2019); 20(14): 3423.
- Schwartz T, Kohnen W, Jansen B, Obst U. Detection of antibiotic-resistant bacteria and their resistance genes in wastewater, surface water, and drinking water biofilms. FEMS microbiology ecology, (2003); 43(3): 325-335.
- Galante J, CY Ho A, Tingey S, M Charalambous B. Quorum sensing and biofilms in the pathogen, Streptococcus pneumoniae. Current pharmaceutical design, (2015); 21(1): 25-30.
- Trunk T, Khalil HS, Leo JC. Bacterial autoaggregation. AIMS microbiology, (2018); 4(1): 140.
- Percival SL, Suleman L, Vuotto C, Donelli G. Healthcare-associated infections, medical devices and biofilms: risk, tolerance and control. Journal of medical microbiology, (2015); 64(4): 323-334.
- Shaheen A, Baqai R. Biofilm Formation by Environmental Microbes Isolated from Hospitals in Karachi, Pakistan. American scientific research journal for engineering, technology, and sciences, (2016); 15(1): 240-251.
- Jamal M, Ahmad W, Andleeb S, Jalil F, Imran M, Nawaz MA, Hussain T, Ali M, Rafiq M, Kamil MA. Bacterial biofilm and associated infections. Journal of the chinese medical association, (2018); 81(1): 7-11.
- VanEpps JS, Younger JG. Implantable Device-Related Infection. Shock (Augusta G). (2016); 46(6): 597.
- Arciola CR, Campoccia D, Montanaro L. Implant infections: adhesion, biofilm formation and immune evasion. Nature reviews microbiology, (2018); 16(7): 397.
- Mariani E, Lisignoli G, Borzì RM, Pulsatelli L. Biomaterials: foreign bodies or tuners for the immune response? International journal of molecular sciences, (2019); 20(3): 636.
- Cappuccino JG, Sherman N. 9: Microbiology: A Laboratory Manual. 2013;10: 567. Pearson
- Djeribi R, Bouchloukh W, Jouenne T, Menaa B. Characterization of bacterial biofilms formed on urinary catheters. American journal of infection control, (2012); 40(9): 854-859.
- Gil-Perotin S, Ramirez P, Marti V, Sahuquillo JM, Gonzalez E, Calleja I, Menendez R, Bonastre J. Implications of endotracheal tube biofilm in ventilator-associated pneumonia response: a state of concept. Critical care, (2012); 16(3): 1-9.
- Sandoe JA, Wysome J, West AP, Heritage J, Wilcox MH. Measurement of ampicillin, vancomycin, linezolid and gentamicin activity against enterococcal biofilms. Journal of antimicrobial chemotherapy, (2006); 57(4): 767-770.
- Bakir SH, Ali FA. Comparison of different methods for detection of biofilm production in multi-drug resistance bacteria causing pharyngotonsillitis. International journal of research h in pharmacy and biosciences, (2016); 3(2): 13-22.
- Hassan A, Usman J, Kaleem F, Omair M, Khalid A, Iqbal M. Evaluation of different detection methods of biofilm formation in the clinical isolates. Brazilian journal of infectious diseases, (2011); 15(4): 305-311.
- Revdiwala S, Rajdev BM, Mulla S. Characterization of bacterial etiologic agents of biofilm formation in medical devices in critical care setup. Critical care research and practice, (2012); 2012: 945805.
- Björling G, Johansson D, Bergström L, Jalal S, Kohn I, Frostell C, Kalman S. Tolerability and performance of BIP endotracheal tubes with noble metal alloy coating–a randomized clinical evaluation study. BMC anesthesiology, (2015); 15(1):1-10.
- Barnes M, Feit C, Grant TA, Brisbois EJ. Antimicrobial polymer modifications to reduce microbial bioburden on endotracheal tubes and ventilator associated pneumonia. Acta biomaterialia, (2019); 91: 220-234.
- Donlan RM. Biofilms and device-associated infections. Emerging infectious diseases, (2001); 7(2): 277.
- Fitzpatrick F, Humphreys H, O'gara JP. The genetics of staphylococcal biofilm formation—will a greater understanding of pathogenesis lead to better management of device-related infection? Clinical microbiology and infection, (2005); 11(12): 967-973.
- Hedayati S, Eftekhar F, Hosseini S. Biofilm formation by bacteria isolated from intravenous catheters. Journal of medical bacteriology, (2014); 3(3-4): 26-31.
- Dhanawade NB, Kalorey DR, Srinivasan R, Barbuddhe SB, Kurkure NV. Detection of intercellular adhesion genes and biofilm production in Staphylococcus aureus isolated from bovine subclinical mastitis. Veterinary research communications, (2010); 34(1): 81-89.
- Subramanian P, Shanmugam N, Sivaraman U, Kumar S, Selvaraj S. Antiobiotic resistance pattern of biofilm-forming uropathogens isolated from catheterised patients in Pondicherry, India. The Australasian medical journal, (2012); 5(7): 344.
- Maharjan G, Khadka P, Siddhi Shilpakar G, Chapagain G, Dhungana GR. Catheter-associated urinary tract infection and obstinate biofilm producers. Canadian journal of infectious diseases and medical microbiology, (2018); 7: 20-25
- Lynch AS, Robertson GT. Bacterial and fungal biofilm infections. Annual review in medicine, (2008); 59: 415-428.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0