

Full Length Research Article
DNA methylation profile of multiple genes involved in bladder cancer among Saudi population – A pilot study
Ahmed Yaqinuddin*, Amna Shoaib Siddiqui, Faizah A. Alshehri**, Ayesha Rahman Ambia
Adv. life sci., vol. 8, no. 3, pp. 293-299, July 2021
*– Corresponding Author: Ahmed Yaqinuddin (Email: ayaqinuddin@alfaisal.edu)
Authors' Affiliations
** Honors Office of Research and Innovation ORI Alfaisal University, Riyadh – Saudi Arabia
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: To identify bladder cancer specific methylated DNA sequences for the Saudi population in order to detect and predict bladder cancer progression.
Methods: In this study, we analysed DNA methylation levels of 48 tumour suppressor genes loci in 24 bladder tissues (19 bladder cancer samples and 5 control samples taken from histologically normal bladders). DNA Methylation analysis was done using Human Tumour Suppressor Genes EpiTect Methyl II Complete PCR Array from Qiagen TM.
Results: We identified significant difference in DNA hypermethylation levels at APC, BRCA1, CDH1, CDH13, CDKN2A, DAPK1, ESR1, FHIT, MGMT, RASSF1, SOCS1, TIMP3, TP73, VHL, WIF1 between controls and cancerous samples. It was also observed that CADM1 and DKK3 were differentially methylated in non-muscle invasive versus muscle invasive bladder cancer samples. Additionally, DNA hypermethylation of ESR1 was notified as the novel tumour suppressor gene specific for the Saudi population in bladder cancer.
Conclusion: Our findings suggest that these aberrant DNA methylation patterns in bladder cancer are disease and population specific and have a potential to develop as distinct DNA methylation-based biomarkers in future.
Keywords: Bladder Cancer; DNA methylation; Epigenetics; Hypermethylation; Tumor Markers
Introduction![]()
Bladder cancer (BC) ranked 13th in Saudi population, while it is ninth common cancer in the world [1]. Although, BC is much less prevalent in this region, but alarmingly it ranked first among the genitourinary cancers [2]. Its incidence is particularly high in north-western region of Saudi Arabia, because of its association with schistosomiasis [3]. Although not reported, other risk factors associated with the development of BC in the Saudi population could be excessive smoking, exposure to increased levels of toxic chemicals and petroleum products.
BC can be divided into two groups, Non-Muscle Invasive Bladder Cancer (NMBC) and Muscle Invasive Bladder Cancer (MBC). Approximately, 80% patients’ presents with NMIBC and have good prognosis, however, majority of treated cases recur and progress to MIBC [4]. Hence, such patients require long term follow up with periodic cystoscopy [5]. Although, cystoscopy is an essential prognostic and diagnostic tool, but it is invasive and levies enormous burden in terms of procedural cost in outpatient clinics [6]. Protein based biomarkers (NMP22, Fibrin/FDP, BTA) has also been introduced as a non-invasive method for early BC detection and monitoring, however each lack specificity and sensitivity particularly in low grade tumours [7].
Epigenetic alteration plays an important role in bladder carcinogenesis and DNA methylation reveals important epigenetic mutations with further downstream effects, without altering the DNA sequence [8,9]. BC has significantly pronounced differential DNA methylation compared to non-urothelial cancer patients. Specifically, DNA hypermethylation of CpG dinucleotide at the promoter region, a “bladder-specific region,” of tumour suppressor genes causing gene suppression is the most frequent epigenetic change seen in BC [10,11] .Interestingly, these differential DNA methylation patterns can also be found as cell free DNA (cfDNA) in the body fluids of cancer patients and can be used as robust biomarkers to detect and predict cancer progression [12]. Alterations in DNA methylation has been recognized and localized in at least 50 cancer types, these modifications of DNA without change in sequence are heritable and can change gene expression [13,14]. Thus, such molecular diagnosis may present as a powerful tool for BC detection before it presents clinically, especially for types of BCs with better outcomes. These studies should not only be able to detect the cancerous tissue, but also localize the tissue of origin (TOO) in asymptomatic patients. They can also be utilized to understand therapeutic response and prognosis of BC patients [13,14]. Urine cfDNA is also gaining attention recently for diagnosis of BC through full void, pellet or supernatant urine. This method is less invasive and has better sensitivity than urine cytology and FISH, especially in diagnosing earlier stages of BC [9,15,16].
Bladder cancer-related epigenetic alterations is by far, studied widely among various populations of BC patients. Evidence suggests that these alterations are dynamic and respond to environmental influences [17]. However, no study to-date has profiled DNA methylation of BC patients in Saudi population in spite of ranking top on the list among other urogenital cancers. Therefore, in this study, we aim to profile methylation pattern of 48 candidate tumour suppressor genes in normal and cancerous bladder tissue among the Saudi population. Based on our results, we will be able to reveal distinctive methylation patterns between normal and cancerous, invasive and non-invasive cancerous bladder tissue, specific for the Saudi population. This will later help us to recognise a newer molecular biomarker specifically for the Saudi population and help us to improve clinical decision making and treatment planning in this region.
Methods![]()
Tissue Samples
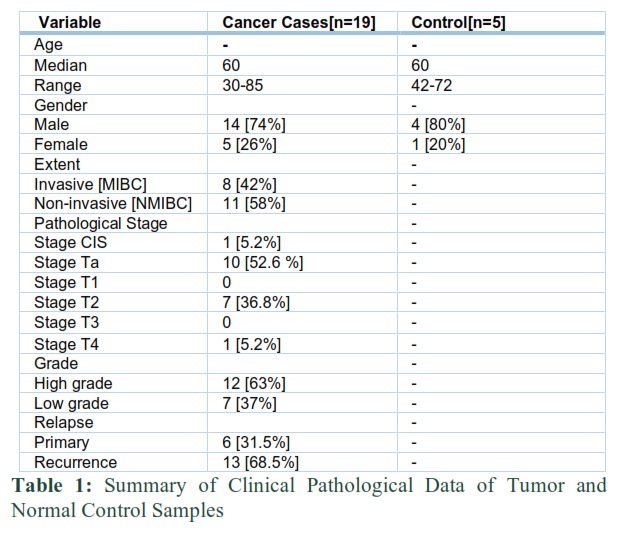
Fresh samples of cancerous bladder tissue were collected from 19 patients during cystoscopy, at King Faisal Hospital and Research Centre Urology Clinic, before the initiation of any kind of treatment. As control, 5 corresponding normal appearing tissue samples, adjacent to tumour were also obtained for the study. Patients with the history of cystitis and tumour other than bladder region were excluded. Fragments from each tissue sample were embedded in paraffin and stained with H&E stain. The clinicopathological parameters were confirmed by the pathologist. Tumours were staged according to TNM classification system. Detail demographic and clinic-pathologic parameters for all the samples are listed in Table 1. The collected samples were stored at -80oC until use. All samples were collected after taking informed consent. Ethical approval was obtained from Office of Research (ORA) of King Faisal Specialist Hospital and Research Centre (KFSHRC).
DNA Extraction
The DNA was extracted as per protocol of the Qiagen tissue kit. The quality and quantity of the extracted DNA was confirmed by measuring 260/280 ratios on spectrophotometer (ND-1000; Nano Drop Technologies).
Selection of Genes
The 48 tumour suppressor genes selected for this study were selected based on previous studies examining DNA methylation markers for diagnosis and prognosis of different cancers. Majority of these genes evaluated here are implicated in tumorigenesis of BC.
Methylation PCR Array
The EpiTect Methyl II PCR Array (Qiagen) was performed to evaluate the DNA methylation status at 48 tumour suppressor gene promoters in 24 samples. The EpiTect Methyl II DNA restriction digestion assays were used as per Qiagen’s protocol. This method detects the remaining input DNA after restriction digestion by methylation dependent and methylation sensitive enzymes. Briefly, 4 micrograms of genomic DNA were used with 100ul of 5x digestion buffer and RNase-DNase free water without enzymes. This mix was further incubated at 37oC with four different treatments 1) DNA methylation-dependent restriction enzyme (Md) 2) DNA methylation Sensitive restriction enzyme (Ms) 3) Restriction enzyme digestion by both Md and Ms (Md/Ms) 4) Mock enzyme treatment (Mo). The remaining DNA after digestion in each of the four reactions was amplified by real time-PCR using predesigned primers. The real time PCR was performed using 7000 Sequence Detection System (Applied Bio systems, Foster City, CA, USA) using SYBR® Green and CT values were recorded. The cycling conditions were 95 ◦C for 10 min followed by 40 cycles of 97 ◦C for 15 s and 72 ◦C for 1 min. SABiosciences Excel-Based Data Analysis was performed. This template uses the percent of hypermethylated DNA by comparing the amount of DNA in each digest with mock digest. This represents the fraction of input DNA containing at least two methylated CpG sites in the targeted gene region. Differences in methylation levels among three groups were noted and later use for further statistical evaluation.
Statistical Analysis
Descriptive statistics were used to summarize patient data and DNA methylation status of 48 genes. Pairwise associations followed dichotomous variables defined according to presence or absence of tumour, tumour invasiveness [non-invasive versus invasive] and differentiation grade (low versus high).The association of promoter methylation of each gene with outcomes was assessed by Mann-Whitney U test with a 5% significance level. SPSS v 20.0 (SPSS – Statistical Package for The Social Sciences v20.0, SPSS Inc.) was used for all statistical analysis.
Results![]()
Clinical Pathological Data of Cancerous Cases and Control Samples-
The cases (n=19) and control (n=5) were well matched on age and race. The median age of all cancerous and normal patients was 60, with no significant difference. However the number of male and females varies in both the groups i.e., males were 74% and females 25%. Tumour samples were further stratified based on tumour staging into NMIBC (58%) and MIBC (42%); and based on tumour grading into low grade (7 %) and high grade (12 %) (Table 1). Based on pathological staging, most common type was non-invasive papillary carcinoma (52.6%) among all cancerous tissue samples. 68.5 % of the cases were positive with a history of relapse.
Comparison of Variable Groups
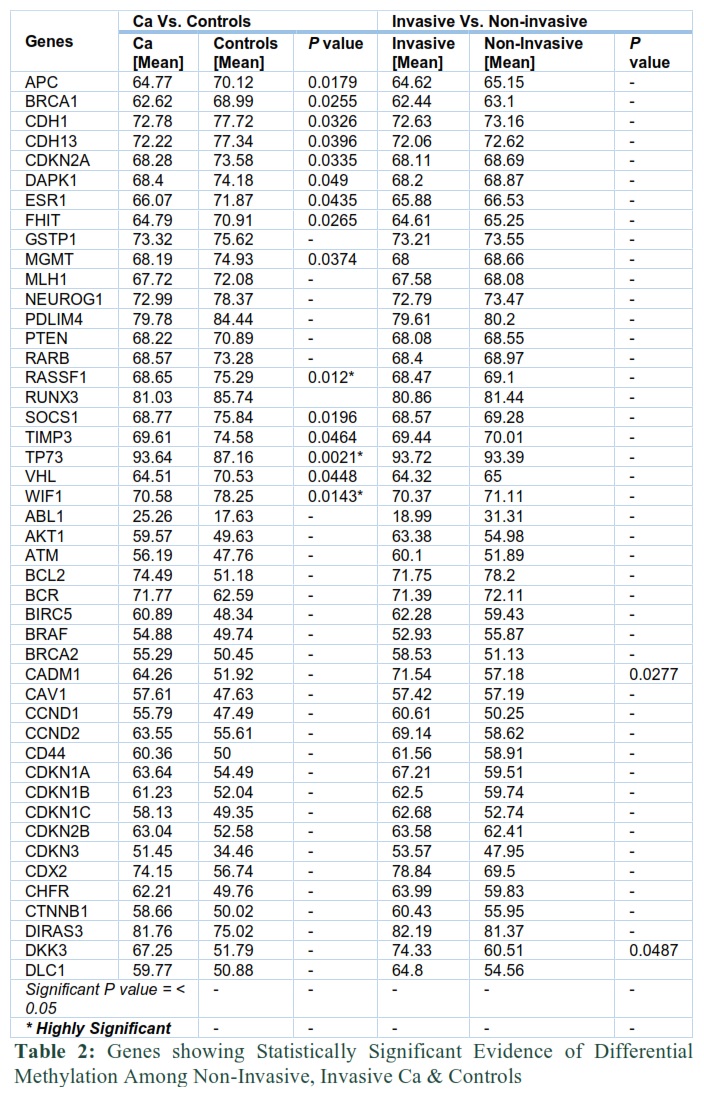
Clustering results of our tissue sample between 3 paired groups [divided according to the presence or absence of tumour, tumour invasiveness and differentiation grade] showed hypermethylation in all samples. However, statistically significant differential gene methylation frequency has been noted among few gene loci for each of these compared groups (Table 2).
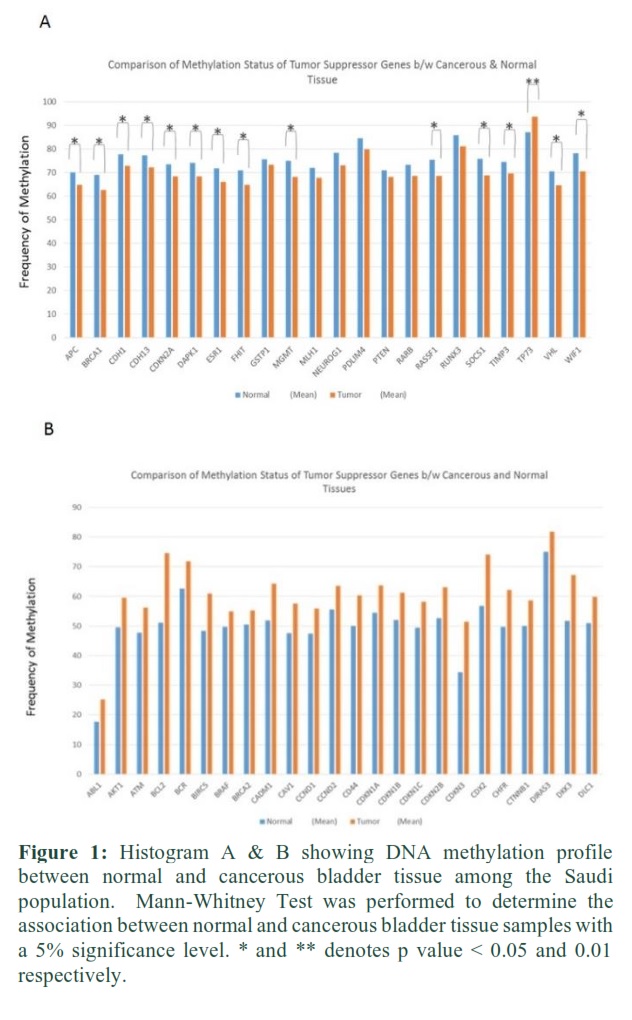
Regarding the tumour existence, 15 genes (APC, BRCA1, CDH1, CDH13, CDKN2A, DAPK1, ESR1, FHIT, MGMT, RASSF1, SOCS1, TIMP3, TP73, VHL, and WIF1) showed significant difference in DNA methylation status in cancerous tissue compared to normal. Interestingly, only TP73 showed significantly high hypermethylation levels in the cancerous tissue as compare to normal with p value = 0.0021 (Table 2). However, all the other 14 genes showed lower hypermethylation levels in bladder cancerous tissue samples with most significant RASSF1, WIF1 and TIMP3 genes. We also identified one novel tumour suppressor gene (ESR1) in this group, which showed significantly low hypermethylation levels in bladder cancer tissue compared to normal samples. The methylation status of the remaining genes in bladder cancer samples did not differ significantly from the methylation status of healthy controls as shown in Figure 1 (A&B).
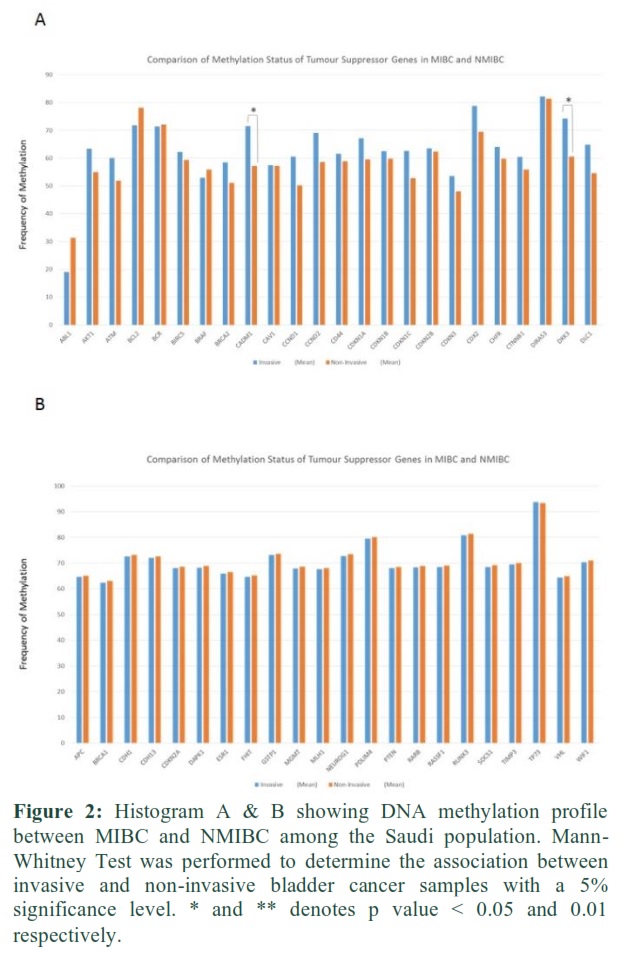
Regarding the tumour invasiveness, only two genes (CADM1 and DKK3) were found to demonstrate significantly high hypermethylation (p = 0.0277 and 0.0487 respectively) in patients with MIBC compared to NMIBC (Fig 2-A, Table 2). Some genes show higher hypermethylation in invasive than non-invasive cancer samples, but they do not reach the statistically significant threshold (Fig 2). All other genes show less or no change in methylation pattern in invasive compared to non-invasive tissue samples.
Regarding the tumour grading, no gene was reported to have significant methylation difference in comparison of low and high grade tumours.
Figures & Tables
Discussion![]()
In our study, significant difference in DNA hypermethylation levels was observed at APC, BRCA1, CDH1, CDH13, CDKN2A, DAPK1, ESR1, FHIT, MGMT, RASSF1, SOCS1, TIMP3, TP73, VHL, WIF1 between controls and cancerous samples.
It was also observed that CADM1 and DKK3 are differentially methylated in NMIBC versus MIBC samples. In contrast, no significant difference in DNA methylation levels at any gene promoter was found to be associated with tumour grade.
Evidence suggests that these altered DNA methylation patterns are dynamic and respond to environmental influences [17]. To our knowledge, this is the first study which has analysed the methylation patterns in BC, using a panel of 48 candidate genes loci in 19 bladder cancer patients from the Saudi population.
Many studies have identified RASSF1 and WIF1 as candidate tumour suppressor gene which epigenetically gets inactivated during various human carcinogenesis [18]. Their hypermethylation has also been reported in BC which is significantly higher than healthy controls [19]. Recently, the RASSF1 gene has been highlighted as most commonly hypermethylated genes in tumours [20]. Likewise, our study reveals the significant difference in hypermethylation patterns in both these genes between cancerous and control samples; however the hypermethylation levels were much higher in controls which was an unexpected finding. As the controls were taken from the adjacent normal tissue of matched cancerous samples. This suggests that genomic changes and DNA methylation changes in bladder tissue may occur before the morphological changes [21]. Aberrant methylation patterns in the control samples suggest to be a characteristic of a premalignant lesion as bladder cancer is a multifocal tumour with high recurrence index [22]. A genome-wide DNA methylation study on upper urinary tract urothelial cancer also noted increased DNA methylation in non-cancerous cells at numerous CpG sites without histological changes, suggesting that field effect of tumour agents can induce transformation in neighbouring cells [23]. Thus, this verifies the hypothesis that DNA methylation changes in cancers may pre-exists in normal looking cells and it can be beneficial for the early detection of BC even in the Saudi population.
TP73 gene was found to be significantly hypermethylated tumour suppressor in this study. This gene belongs to the TP53 family of transcription factor genes and it leads to apoptosis in response to DNA damage [24]. TP73 has been particularly well studied in breast tumours [25]. Overexpression of TP73 has also been reported in bladder and prostate cancers [26]. Interestingly, we showed higher levels of hypermethylation at this gene locus among BC samples of Saudi origin compared to controls.
TIMP3 gene, encodes the inhibitor of the matrix metalloproteinase, a peptidase involved in degradation of the extracellular matrix [27]. Significant difference in the hypermethylation status of this gene locus found in this study can be considered a significant finding in relation to Saudi Arabia, since previous reports suggested links between hypermethylation of TIMP3 gene with schistosome-infected bladder cancer [28].
Although, our results have confirmed previous studies showing varied hypermethylation frequencies among different genes in BC. Interestingly, one novel tumour suppressor genes ESR1 is also notified showing significant difference in DNA hypermethylation status in BC tissue samples as compared to controls. Hypermethylation of this gene has not been reported earlier in the literature in relation to BC and can be considered specific for the Saudi population. ESR1 encodes the estrogen receptor 1, this protein influences the growth and differentiation function of different tissues in response to estrogen. This gene shows high frequency of genetic variation in many types of human malignant tumours especially in breast tissues [29] but no link with BC was reported earlier.
Several studies have identified methylated genes and panel of loci that are associated with the bladder cancer invasion, such as IPF1, GALR1, TAL1, PENK, TJP2, HOXB2, RASSF1A and RARβ genes [30]. Interestingly, current study shows for the first time that differential hypermethylation of CADM1 and DKK is associated with MIBC.
The CADM1 gene (also known as TSLC1 or IGSF4) codes for cell-to-cell adhesion in Ca+ independent manner. It has been generally investigated as a tumour-suppressor gene in prostate, oesophageal, nasopharyngeal, non-small cell lung and cervical cancers [31,32]. CADM1 is down regulated frequently in many cancers via promoter hypermethylation [33]. However, relevance of its hypermethylation in BC prognosis is not well known. A significant increase in DNA methylation levels of CADM1 among MIBC observed in our study supports its possible down regulation in invasive bladder tumours.
DKK3 encodes a protein that is a member of the dickkopf family. The secreted protein through its interactions with the Wnt signalling pathway is involved in embryonic development. Variety of cancer cell lines have shown decreased expression of this genes and it may function as tumour suppressor [34]. It has been shown previously that hypermethylation of DKK3 in cervical cancer cell lines can lead to activation of Wnt/β-catenin pathway and increased tumorigenesis [35]. Therefore, it would be interesting to decipher its role in invasive bladder cancer. A study with larger sample size can determine its value in prognosticating BC in the Saudi population.
There have also been studies identifying the role of DNA methyltransferase 3B (DNMT3B) in the tumourigenesis of BC through microRNA (miR)-34a promoter methylation, through its downregulation [36]. Matrix Metalloproteinase 11 (MMP11) is also a differentially expressed gene in BCs due to its promoter hypomethylation. MMPs are extracellular enzymes that break down the extracellular matrix [37]. Methylation status of genes such as SOX-1, IRAK3 and LI-MET were shown to be more useful in determining tumour progression than cystoscopy. Furthermore, hypermethylated TIG1, GSTP1 and APC were associated with worse survival rates [14]. Hypomethylation, and consequently downregulation of the promoter region of the AJAP1 gene (which codes for adherens junction-associated protein 1) by the ten-eleven translocation 1 (TET1), indicates poor prognosis due to subsequent activation of the β-catenin signalling pathway leading to BC pathogenesis [38].
Recently, it has been shown that cell free DNA in the urine can be used as a sensitive and specific biomarker for detection of bladder cancer [39,40]. Studies from Rose et al and Wu et al have demonstrated several DNA methylation based urinary biomarkers including ITIH5, ECRG4, HOXA9, PCDh17, POU4F2 and ONECUT2 can be used for diagnosis of bladder cancer [39,40].
In conclusion, in this study we have identified distinctive genes that show evidence of differential methylation between cancerous and normal tissue, non-invasive and invasive cancer tissue specific for the Saudi population. This is a pilot study where we were able to screen DNA methylation of status of genes which can be used as potential biomarkers for BC diagnosis and prognosis However, larger studies on BC-associated changes in DNA methylation are required for developing sensitive and specific biomarkers for diagnosis and prediction of the disease. Recent studies have shown that cell free tumour derived DNA in urine and blood samples can be easily detected using specific DNA methylation patterns. Since the DNA methylation patterns are tumour specific and population specific so identification of DNA methylation patterns specific to Saudi population of bladder cancer is an important first step to develop distinct DNA methylation-based biomarkers specific for the Saudi population.
This is a pilot study to screen out potential DNA methylation markers which can used in future for detection and prognosis of bladder cancer on a large representing sample size of Saudi population. As we were screening 48 tumor suppressors we needed large quantity of good quality DNA (4 microgram) from our biopsy samples to conduct our experiments, which was not available from small size of the normal bladder biopsies. This is the reason we had only 5 control samples taken from the adjacent normal tissues of the bladder cancer patients. However, we were able to compare the DNA methylation status for 48 genes in three different group which was quite extensive and conducted for the first time in this region. We will utilise data from this study to select significantly differentially methylated genes with larger sample size to develop sensitive and specific tumour markers for BC in future.
Author Contributions
AY contributed in designing the study, analysis of data and writing of the manuscript. ASS contributed in data collection, analysis and writing of the manuscript. AA contributed in analysis and writing of the manuscript.
Acknowledgement
This work was funded by KACST grant# 09-BIO812-20.
None.
References![]()
- Alkhateeb S, Al-Mansour M, Alotaibi M, Saadeddin A, Abusamra A, et al. Saudi Oncology Society and Saudi Urology Association combined clinical management guidelines for urothelial cell carcinoma of the urinary bladder. Urology Annals, (2016); 8(2): 131-135.
- Al-Othman K, Al-Hathal N. Pattern of management of urologic cancer in Saudi Arabia. Urology Annals, (2010); 2(1): 21-25.
- Scrimgeour EM. Bladder carcinoma and schistosomiasis haematobia in Saudi Arabia. Annals of Saudi Medicine, (1995); 15(2): 192.
- Kaufman DS, Shipley WU, Feldman AS. Bladder cancer. Lancet, (2009); 374(9685): 239-249.
- Shariat SF, Karam JA, Lotan Y, Karakiewizc PI. Critical evaluation of urinary markers for bladder cancer detection and monitoring. Reviews in Urology, (2008); 10(2): 120-135.
- Goodison S, Rosser CJ, Urquidi V. Bladder cancer detection and monitoring: assessment of urine- and blood-based marker tests. Molecular Diagnosis & Therapy, (2013); 17(2): 71-84.
- van Rhijn BW, van der Poel HG, van der Kwast TH. Urine markers for bladder cancer surveillance: a systematic review. European Urology, (2005); 47(6): 736-748.
- Jordahl KM, Phipps AI, Randolph TW, Tinker LF, Nassir R, et al. Mediation by differential DNA methylation of known associations between single nucleotide polymorphisms and bladder cancer risk. BMC Medical Genetics, (2020); 21(1): 228.
- Mancini M, Righetto M, Zumerle S, Montopoli M, Zattoni F. The Bladder EpiCheck Test as a Non-Invasive Tool Based on the Identification of DNA Methylation in Bladder Cancer Cells in the Urine: A Review of Published Evidence. International Journal of Molecular Sciences, (2020); 21(18): 6542.
- Kohler CU, Walter M, Lang K, Plottner S, Roghmann F, et al. In-Vitro Identification and In-Vivo Confirmation of DNA Methylation Biomarkers for Urothelial Cancer. Biomedicines, (2020); 8(8): 233.
- Vaissiere T, Sawan C, Herceg Z. Epigenetic interplay between histone modifications and DNA methylation in gene silencing. Mutation Research, (2008); 659(1-2): 40-48.
- Chihara Y, Kanai Y, Fujimoto H, Sugano K, Kawashima K, et al. Diagnostic markers of urothelial cancer based on DNA methylation analysis. BMC Cancer, (2013); 13275.
- Liu MC, Oxnard GR, Klein EA, Swanton C, Seiden MV, et al. Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA. Annals of Oncology, (2020); 31(6): 745-759.
- Tian Z, Meng L, Long X, Diao T, Hu M, et al. DNA methylation-based classification and identification of bladder cancer prognosis-associated subgroups. Cancer Cell International, (2020); 20255.
- Chen X, Zhang J, Ruan W, Huang M, Wang C, et al. Urine DNA methylation assay enables early detection and recurrence monitoring for bladder cancer. Journal of Clinical Investigation, (2020); 130(12): 6278-6289.
- Hentschel AE, Nieuwenhuijzen JA, Bosschieter J, Splunter APV, Lissenberg-Witte BI, et al. Comparative Analysis of Urine Fractions for Optimal Bladder Cancer Detection Using DNA Methylation Markers. Cancers (Basel), (2020); 12(4): 859.
- Turner BM. Epigenetic responses to environmental change and their evolutionary implications. Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences, (2009); 364(1534): 3403-3418.
- Garrigou S, Perkins G, Garlan F, Normand C, Didelot A, et al. A Study of Hypermethylated Circulating Tumor DNA as a Universal Colorectal Cancer Biomarker. Clincal Chemistry, (2016); 62(8): 1129-1139.
- Negraes PD, Favaro FP, Camargo JL, Oliveira ML, Goldberg J, et al. DNA methylation patterns in bladder cancer and washing cell sediments: a perspective for tumor recurrence detection. BMC Cancer, (2008); 8238: 1-12.
- Zhan L, Zhang B, Tan Y, Yang C, Huang C, et al. Quantitative assessment of the relationship between RASSF1A gene promoter methylation and bladder cancer (PRISMA). Medicine (Baltimore), (2017); 96(7): e6097.
- Cianciulli AM, Leonardo C, Guadagni F, Marzano R, Iori F, et al. Genetic instability in superficial bladder cancer and adjacent mucosa: an interphase cytogenetic study. Human Pathology, (2003); 34(3): 214-221.
- Trkova M, Babjuk M, Duskova J, Benesova-Minarikova L, Soukup V, et al. Analysis of genetic events in 17p13 and 9p21 regions supports predominant monoclonal origin of multifocal and recurrent bladder cancer. Cancer Letters, (2006); 242(1): 68-76.
- Fujimoto M, Arai E, Tsumura K, Yotani T, Yamada Y, et al. Establishment of diagnostic criteria for upper urinary tract urothelial carcinoma based on genome-wide DNA methylation analysis. Epigenetics, (2020); 15(12): 1289-1301.
- Rufini A, Agostini M, Grespi F, Tomasini R, Sayan BS, et al. p73 in Cancer. Genes Cancer, (2011); 2(4): 491-502.
- Dominguez G, Garcia JM, Pena C, Silva J, Garcia V, et al. DeltaTAp73 upregulation correlates with poor prognosis in human tumors: putative in vivo network involving p73 isoforms, p53, and E2F-1. Journal of Clincal Oncology, (2006); 24(5): 805-815.
- Yokomizo A, Mai M, Tindall DJ, Cheng L, Bostwick DG, et al. Overexpression of the wild type p73 gene in human bladder cancer. Oncogene, (1999); 18(8): 1629-1633.
- Lindsey JC, Lusher ME, Anderton JA, Bailey S, Gilbertson RJ, et al. Identification of tumour-specific epigenetic events in medulloblastoma development by hypermethylation profiling. Carcinogenesis, (2004); 25(5): 661-668.
- Zhong X, Isharwal S, Naples JM, Shiff C, Veltri RW, et al. Hypermethylation of genes detected in urine from Ghanaian adults with bladder pathology associated with Schistosoma haematobium infection. PLoS One, (2013); 8(3): e59089.
- Gaudet MM, Campan M, Figueroa JD, Yang XR, Lissowska J, et al. DNA hypermethylation of ESR1 and PGR in breast cancer: pathologic and epidemiologic associations. Cancer Epidemiology, Biomarkers & Prevention, (2009); 18(11): 3036-3043.
- Wolff EM, Chihara Y, Pan F, Weisenberger DJ, Siegmund KD, et al. Unique DNA methylation patterns distinguish noninvasive and invasive urothelial cancers and establish an epigenetic field defect in premalignant tissue. Cancer Research, (2010); 70(20): 8169-8178.
- Fukuhara H, Kuramochi M, Fukami T, Kasahara K, Furuhata M, et al. Promoter methylation of TSLC1 and tumor suppression by its gene product in human prostate cancer. Japenes Journal of Cancer Research, (2002); 93(6): 605-609.
- Lung HL, Cheung AK, Xie D, Cheng Y, Kwong FM, et al. TSLC1 is a tumor suppressor gene associated with metastasis in nasopharyngeal carcinoma. Cancer Research, (2006); 66(19): 9385-9392.
- Murakami Y. Involvement of a cell adhesion molecule, TSLC1/IGSF4, in human oncogenesis. Cancer Science, (2005); 96(9): 543-552.
- Hayashi T, Asano H, Toyooka S, Tsukuda K, Soh J, et al. DNA methylation status of REIC/Dkk-3 gene in human malignancies. Journal of Cancer Research and Clinical Oncology, (2012); 138(5): 799-809.
- Lee EJ, Jo M, Rho SB, Park K, Yoo YN, et al. Dkk3, downregulated in cervical cancer, functions as a negative regulator of beta-catenin. Internation Journal of Cancer, (2009); 124(2): 287-297.
- Xu K, Chen B, Li B, Li C, Zhang Y, et al. DNMT3B silencing suppresses migration and invasion by epigenetically promoting miR-34a in bladder cancer. Aging (Albany NY), (2020); 12(23): 23668-23683.
- Wu Y, Jiang G, Zhang N, Liu S, Lin X, et al. HOXA9, PCDH17, POU4F2, and ONECUT2 as a Urinary Biomarker Combination for the Detection of Bladder Cancer in Chinese Patients with Hematuria. European Urology Focus, (2020); 6(2): 284-291.
- Liu B, Sun W, Gao W, Li L, Cao Z, et al. microRNA-451a promoter methylation regulated by DNMT3B expedites bladder cancer development via the EPHA2/PI3K/AKT axis. BMC Cancer, (2020); 20(1): 1019.
- Yan YL, Huang ZN, Zhu Z, Cui YY, Li MQ, et al. Downregulation of TET1 Promotes Bladder Cancer Cell Proliferation and Invasion by Reducing DNA Hydroxymethylation of AJAP1. Fronteirs in Oncology, (2020); 10667.
- Rose M, Bringezu S, Godfrey L, Fiedler D, Gaisa NT, et al. ITIH5 and ECRG4 DNA Methylation Biomarker Test (EI-BLA) for Urine-Based Non-Invasive Detection of Bladder Cancer. Internation Journal of Molecular Sciences, (2020); 21(3).
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0