

Full Length Research Article
Comparative safety and efficacy of Rituximab biosimilar (Truxima) and the reference rituximab product (MabThera) in the treatment of different types of adult glomerulonephritis
Mahmoud Mansour1*, Tariq Aldebasi2,3, Abeer Alzubaidi4, Abdulsalam Alanazi1, Abdulaziz Alarifi1, Fahad Almutairi1, Mohammed Alfaifi1, Norah Aldeghaither1, Yousef Al-Rajhi1,4, Saad Alnofaie4
Adv. life sci., vol. 12, no. 2, pp. 418-424, May 2025
*– Corresponding Author: Mahmoud Mansour (Email: mansoura@ksau-hs.edu.sa)
Authors' Affiliations 1. College of Pharmacy, King Saud bin Abdulaziz University for Health Sciences, Riyadh, 11481 – Saudi Arabia
2. College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, 11481 – Saudi Arabia
3. Ophthalmology Department, King Abdulaziz Medical City, Riyadh, Saudi Arabia
4.Pharmaceutical Care Department, King Abdulaziz Medical City, National Guard Health Affairs, Riyadh, 11426, Saudi Arabia
2. College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, 11481 – Saudi Arabia
3. Ophthalmology Department, King Abdulaziz Medical City, Riyadh, Saudi Arabia
4.Pharmaceutical Care Department, King Abdulaziz Medical City, National Guard Health Affairs, Riyadh, 11426, Saudi Arabia
[Date Received: 20/10/2024; Date Revised: 05/01/2025; Date Available Online: 31/08/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The most important advancement in the treatment of glomerulonephritis is the application of rituximab (MabThera®), for several decades. Rituximab biosimilar (Truxima®) was approved for the same indications offering significant cost savings. This study aimed to compare the safety and efficacy of rituximab biosimilar (Truxima) with the reference rituximab product (MabThera) in the treatment of glomerulonephritis, using both laboratory and clinical parameters to assess their similarity.
Methods: We examined the clinical results retrospectively and collected the data of the laboratory parameters from 65 patients suffering from glomerulonephritis treated with either Truxima or MabThera, for disease induction and maintenance of remission, at the King Abdulaziz Medical Centre, Al-Riyadh between 2019 and 2023.
Result: The present study shows no significant difference in rates of remission and relapse between patients receiving Truxima or MabThera treatment. There were no significant differences in the patients’ complete renal recovery at 6 months between the two groups, P = .692. Additionally, no remarkable differences between both medications in the patients' time to relapse. A comparison of mean clinical data for serum creatinine, cholesterol and blood indices at baseline, 6 months and 12 months of the patients in Truxima® and MabThera® groups revealed that patients who received MabThera® had a significantly higher WBC count at 6th month, P = .030 only.
Conclusion: The current study shows that (Truxima) is just as safe and effective as its original product, (MabThera). Therefore, Truxima is a more affordable and safer alternative that potentially increases rituximab accessibility to patients.
Keywords: Truxima; Mabthera; Glomerulonephritis; Efficacy; Safety
Introduction![]()
Glomerulonephritis (GN) involves inflammation in the glomeruli of the kidneys due to immune system dysregulation. Immune complexes and inflammatory cells cause damage to the glomerular structures, compromising their filtration function. This can lead to protein and red blood cell leakage into the urine. Genetic factors, infections, and systemic diseases can contribute to glomerulonephritis. GN is a significant cause of kidney failure worldwide, contributing to both acute and chronic kidney disease. If untreated, it can result in progressive kidney damage. Proper diagnosis, management of underlying causes, and targeted therapies are crucial for treating glomerulonephritis [1].
Rituximab, a monoclonal antibody directed against and targeting CD20, is an antigen produced at most stages of B cell development that is thought to function as a calcium channel and contribute to B cell maturation and activation leading to depletion of B cells [2]. It is known to cause multiple side effects, including hypogammaglobinaemia, infusion reactions, and late-onset neutropenia, and it can lead to various infections [3].
Among the various treatment strategies for GN, Rituximab has emerged as a cornerstone therapy for managing autoimmune forms of GN, particularly in patients with minimal change disease, focal segmental glomerulosclerosis, membranous nephropathy, lupus nephritis, and anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis [4,5]. Its function in lupus nephritis (LN) and C3GN is still unknown, and it has not yet been demonstrated to play a part in IgA nephropathy (IgAN) [6,7]. Rituximab has demonstrated efficacy in inducing remission and reducing relapse rates, positioning it as a key immunosuppressive agent in GN treatment [8].
A biosimilar drug is a nearly identical version of an existing biological drug. The approval process for biosimilars involves a comprehensive evaluation to demonstrate that there are no profound differences in terms of clinical outcomes between both products. Regulatory authorities require a systematic approach to assess biosimilars, which may involve varying types of clinical studies. However, it is typically necessary to establish statistical equivalence in pharmacokinetics and efficacy between the biosimilar and reference product, as well as to demonstrate acceptable levels of safety and immunogenicity [9,10]. In 2018, the biosimilar known as Truxima, obtained approval from both the Agency of European Medicines and the Food and Drug Administration (FDA) for the treatment of rheumatoid arthritis, both polyangiitis granulomatosis and microscopic. Clinical trials have shown the similarity between reference rituximab (MabThera) and its biosimilar in terms of pharmacokinetics, pharmacodynamics, effectiveness, safety, and potential for causing immune reactions, through randomized, double-blind, controlled studies [11]. In another research, they found no difference in the rates of remission, hospitalization, and relapse due to repeated infection occurred between patients received rituximab (MabThera) and biosimilars (Truxima) for maintenance of remission or induction of associated vasculitis, anti-neutrophil cytoplasmic antibody (ANCA) Additionally [12].
Rituximab biosimilars offer a cost-effective alternative to the original drug. Given the complex nature of GN and the immunomodulatory role of Rituximab, it is crucial to thoroughly assess whether these biosimilars perform as effectively as the original in both efficacy and safety profiles [13]. As healthcare systems strive to reduce costs, the development of biosimilars, generic versions of biological drugs, has gained momentum. The goal of these biosimilars is to closely resemble their original equivalents, with no clinically meaningful differences in terms of safety, purity, or potency. However, despite regulatory approvals, concerns remain regarding the efficacy and safety of biosimilars in relation and comparison to the original biologics, especially in sensitive therapeutic areas such as GN. Following EMA guidelines, UK institutions began using Truxima for all rituximab indications in 2017 [9].
Therefore, our study’s goal is to evaluate both the efficacy and safety of Truxima in the management of patients with all types of glomerulonephritis at King Abdulaziz Medical City in Riyadh. This research article aims to compare both safety and efficacy of original Rituximab to its counterparts in the treatment of patients with glomerulonephritis and evaluate clinical outcomes, relapse rates, and adverse events between the two groups, providing critical insight into the interchangeability and reliability of Rituximab biosimilars in routine clinical practice.
![]() Methods
Methods
Study design
The primary site for this retrospective, non-interventional, observational study is the Medical City of King Abdulaziz, National Guard, which is the largest tertiary hospital in the Middle East, located in the city of Al- Riyadh, Saudi Arabia. The research was approved by the International Medical Research Centre of King Abdullah (KAIMRC) and the King Abdulaziz Medical City Independent Ethics Committee. This research was performed between July 1, 2019, and December 2023. Patients who were diagnosed with glomerulonephritis disease and received rituximab biosimilar were identified using electronic health record reports. We found that 65 patients in the renal center received Truxima or MabThera for the maintenance or induction of GN remission. MabThera was administered to 32 of these individuals 15 were female and 17 were male. And 33 received Truxima 15 were female and 18 were male.
For the first time, patients were under medical treatment with rituximab biosimilars (Truxima) and MabThera. Before starting treatment was considered week 0 as a baseline. The administration frequency of rituximab biosimilars (Truxima) and MabThera comply with all regulations. The patients were followed for 12 months. The following were the inclusion criteria; the age of the patients should be 18 years or more and should receive Truxima or original MabThera for the first time. However, the presence of certain established diseases such as uncontrolled arterial hypertension, specific heart disorders or diseases including different types of angina, heart failure or diseases requiring an emergency blood transfusion or platelet transfusion, active neoplasia or with viral hepatitis were considered the exclusion criteria.
Variables and Outcomes
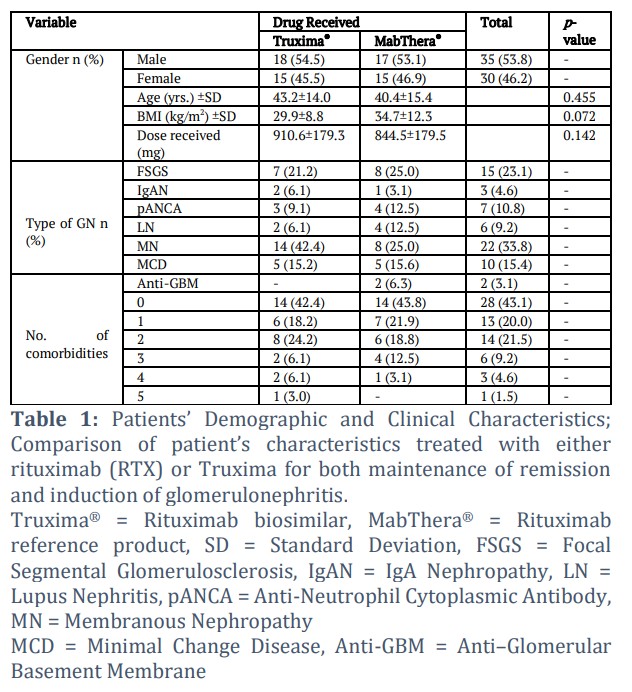
Based on clinical data confidentiality protection medical record review was performed. For each patient, a blinded number (ID) was assigned to take confidentiality into consideration. Age, gender, height, weight, body mass index and other variables follow-up were considered demographic data of concerned recipients (Table 1).
Furthermore, the following data concerning, primary renal diseases, information about urinary infections, early or late acute renal rejections, immunosuppressive treatment data and renal functions at the end of the follow-up period were recorded.
Laboratory Biochemical Parameters
We have collected biochemical variables like serum creatinine, serum cholesterol, white blood cells and haemoglobin from the patient’s medical record either before starting treatment or at the beginning of the treatment and every 6 months. The key components are (demographic data, glomerulonephritis, comorbid condition data, and the study primary and secondary outcome data).
Effectiveness, Improvement of kidney functions and adverse drug reactions
The effectiveness of MabThera and Truxima in causing and maintaining GN remission, recurrence rates, renal outcomes, and adverse effects, which were measured by hospitalization rates for infection and infusion responses were recorded. Furthermore, the improvement of kidney function post-administration of both drugs and adverse drug reactions related to it were reported.
Statistical Analysis
After sorting, coding, and entering the data into SPSS software V. 24 (SPSS Inc., Chicago, IL, USA) for Windows, the data was then examined. Based on treatment protocol, the patients were classified according to whether they were prescribed MabThera® or Truxima®. The data was condensed into means ± SD, percentages, and frequencies. Comparisons of proportions were carried out using Chi-square Pearson’s test. Independent sample t-test was used to determine the mean differences in the patient’s age, BMI, and doses received between the Truxima® and MabThera® The association between the patient’s demographic and clinical characteristics and improvement in renal function were determined using Pearson’s correlation. A P < 0.05 was considered significant throughout.
Patients Baseline Characteristic
We found that 65 patients in the renal center were administered Truxima or MabThera for the induction or maintenance of GN remission between 2019 and 2023. Patients receiving Truxima mean age was 43.2+14 while other patients were 40.4+15.4 years. The distribution of glomerulonephritis types was as follows: 23.1% of patients had Focal Segmental Glomerulosclerosis (FSGS), 4.6% had IgA Nephropathy (IgAN), 10.8% had Anti-Neutrophil Cytoplasmic Antibody (ANCA) negative vasculitis, 9.2% had Lupus Nephritis (LN), 33.8% had Membranous Nephropathy (MN), 15.4% had Minimal Change Disease (MCD), and 3.1% had Anti–Glomerular Basement Membrane (Anti-GBM) disease.
A total of 35 (53.8%) patients were male, out of which 18 (51.4%) received Truxima. Of the 30 (46.2%) female patients, 15 (50%) received MabThera. There were no remarkable differences between the patients on Truxima and MabThera; age (yrs.)±SD, [43.2±14.0 vs 40.4±15.4, (t = 0.752, P = .455)], BMI (kg/m2)±SD, [29.9±8.8 vs 34.7±12.3, (t= -1.831, P = .072)], and the dose received (mg) ±SD, [910.6±179.3 vs 844.5±179.5, (t = 1.486, P = .142)]. MN was the most frequent type of glomerulonephritis (GN) presented by 22 (33.8%) patients. The majority, 14 (21.5%) of the patients presented with two (2) comorbidities (Table 1).
Comparative Effectiveness of Truxima Versus MabThera
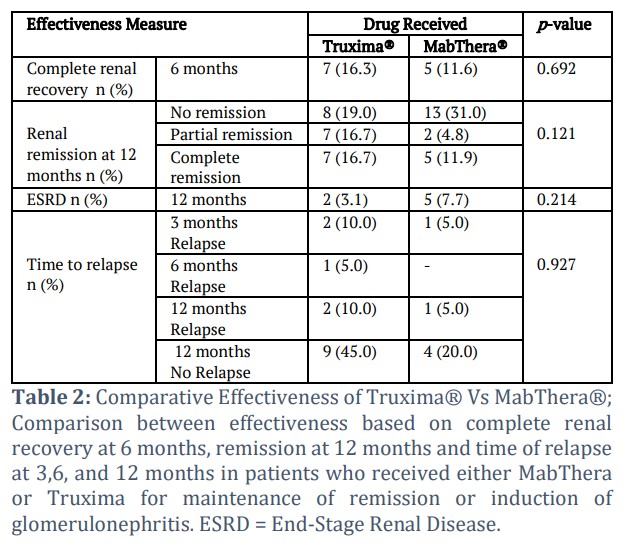
There were no significant differences in the patients’ complete renal recovery at 6 months between the Truxima, 7 (16.3), and MabThera, 5 (11.6), P = .692. Although the majority, 13 (40.6%) of patients in the MabThera group had no remission at 12 months, there were no statistical differences in the patients' renal remission at 12 months between the two drugs, P = .121. On the other hand, the majority, 9 (45.0%), P = .927, of patients in the Truxima group had no relapse at 12 months. However, there were no statistically pronounced differences in the patients’ time to relapse between the two drugs (Table 2).
Comparative of Safety between Truxima Vs MabThera
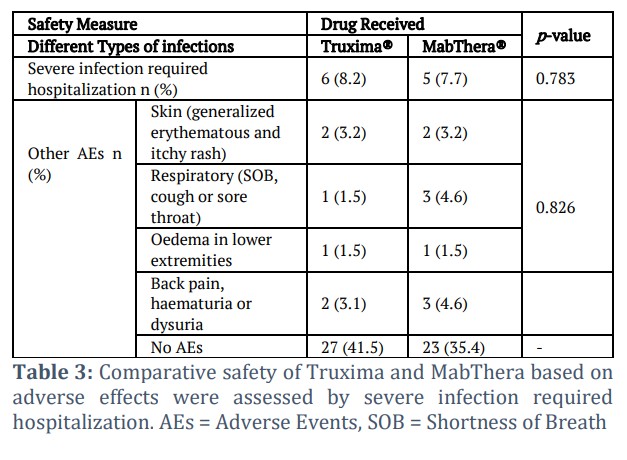
There were 3 (4.6%), incidences of respiratory AEs (shortness of breath (SOB), cough, or sore throat); and back pain, haematuria, or dysuria in patients taking MabThera. However, no profound safety differences were noticed between both drugs regarding severe infection requiring hospitalization, P = .783, and other AEs (skin, respiratory, edema, back pain), P = .826 (Table 3).
Correlation between Complete renal recovery and number of co-morbidities
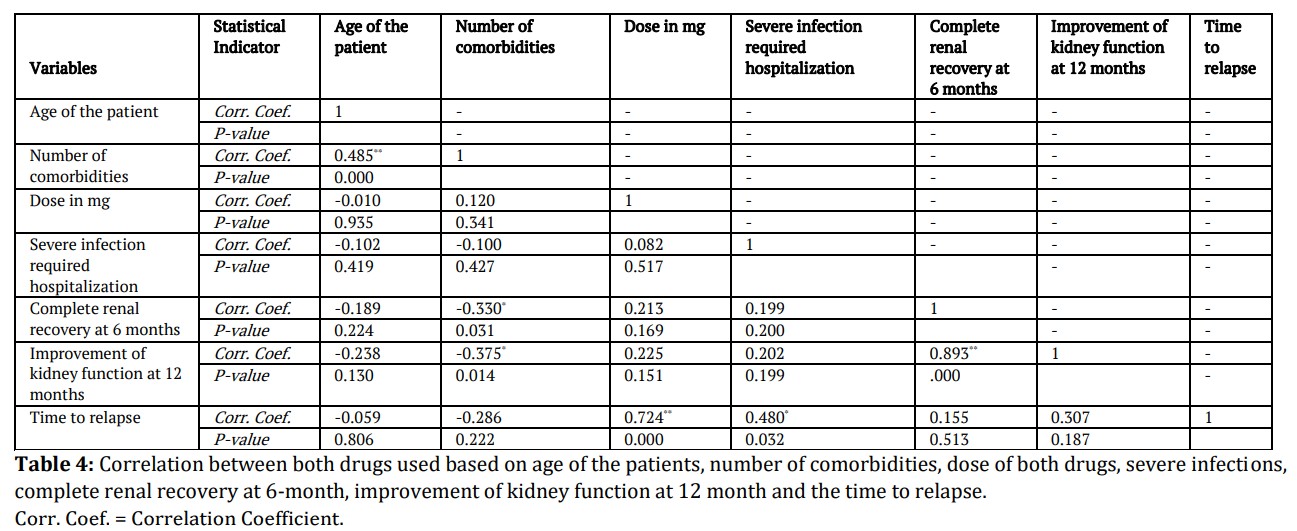
Pearson correlation showed a significant negative association between the patients' complete renal recovery at 6 months and the number of comorbidities, (r = – 0.330, P = .031). Thus, implying that the more the number of comorbidities the less the patients achieve complete renal recovery at 6 months. There was a profound positive correlation between the dose of the rituximab received and time to relapse, (r = 0.724, P <0.001). Implying that the higher the dose received, the longer it takes for the GN to relapse. The older the patient, the more the number of comorbidities, (r = 0.485, P = .000) (Table 4).
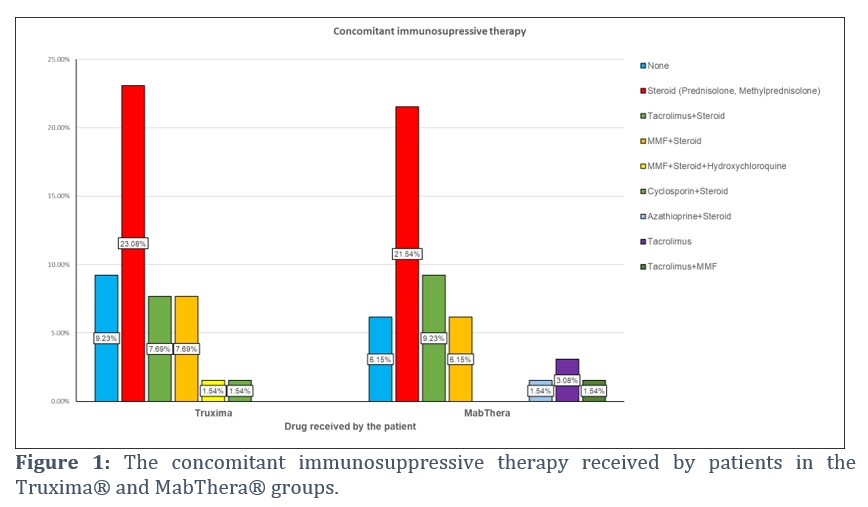
Immunosuppressive Therapy
Prednisolone monotherapy was the most concomitant immunosuppressive therapy received by the patients in both the Truxima®, (23.08%) and MabThera® groups (21.54%). However, there was no notable distinction in the proportions of concomitant immunosuppressive drugs received by the patients in the Truxima® and MabThera® groups, P = .642 (Figure 1).
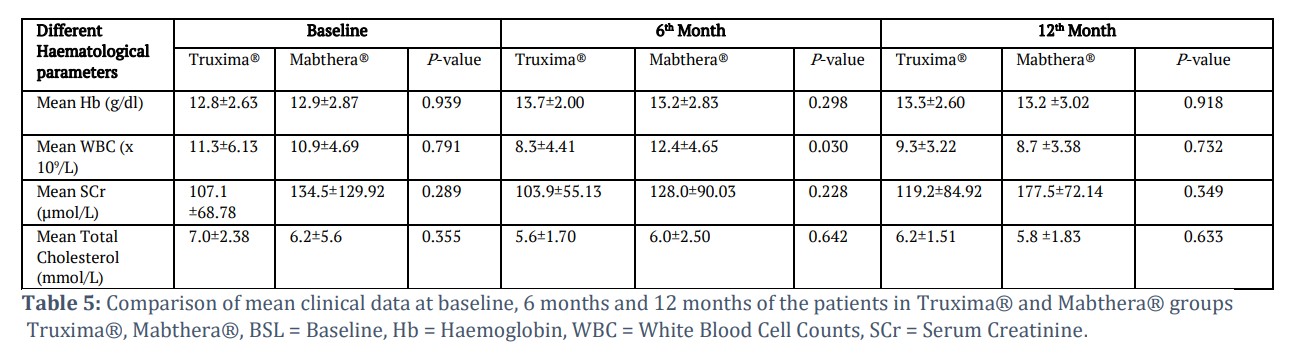
Effect of Truxima or MabThera on WBC count
Table 5 shows the comparison of mean clinical data at baseline, 6 months and 12 months of the patients in Truxima® and MabThera® groups. Compared to Truxima®, the patients who received MabThera® had a significantly higher WBC count at 6th month, t = -2.303, P = .030. On the other hand, patients in the MabThera® group had a 2.2 x 10⁹ /L decrease in WBC count at the 12th month from the baseline.
![]() Discussion
Discussion
One of the efficient therapy options in the management of rheumatoid arthritis and other autoimmune diseases is Rituximab. To reduce the healthcare systems financial burden cost for treating such autoimmune diseases which globally proliferate significantly, new biosimilar products availability may open a new window to down
the high cost-related charge for management and improvement of patient therapies.
So, it is crucial to examine how laboratory and clinical indicators react to reference and biosimilar medications. Based on clinical data such as serum creatinine and cholesterol, the current study shows a similarity between MabThera and Truxima in several terms as relapse, remission, and hospitalization with infection.
Our results support earlier findings mentioned that rituximab-treated vasculitis patients without any effect on the induction of remission, relapse, or all-cause mortality [14,15], depending on a comparison of the laboratory parameters. In other disciplines, a comparative performance of MabThera and Truxima was conducted in Rheumatoid arthritis which indicated pharmacodynamics, immunogenicity, and safety profiles similarity between MabThera and Truxima in phase III clinical trial study [16]. Furthermore, in other autoimmune diseases, in patients with multiple sclerosis [17], and immune thrombocytopenic purpura [18], there were no significant differences in the clinical outcomes between the originator and the biosimilar, adding to also infusion reactions and infective complications. Furthermore, several drugs directed against CD20 second generation were in clinical trial development. McAdoo et al. reported that a fully humanized monoclonal antibody ofatumumab, directed against CD20, showed therapeutic benefit in eight patients with AAV as a small case series [19].
Our study found no statistically significant differences in clinical efficacy between the Truxima and MabThera groups. While there were slight numerical variations in outcomes, these were not statistically significant, including the rates of complete renal recovery at 6 months (P = .692) , overall renal remission at 12 months (P = .121) , and time to relapse (P = .927). Similarly, the incidence of end-stage renal disease was not significantly different between the two cohorts (P = .214). These findings align with the study's overall conclusion that Truxima and MabThera have comparable efficacy and safety in this patient population. These variations may be partially explained by the different lengths of time the drugs have been in clinical use. In our present study, the mean clinical data of serum creatinine at baseline, 6 months and 12 months of the patients in Truxima® and MabThera® groups showed no significant difference while the white blood cell count was significantly higher in the MabThera group compared to the Truxima group at 6 months.
It has been reported significant budget savings in European healthcare systems when using biological biosimilars instead of Rituximab [20]. In 2017, a budget analysis showed that using Truxima in the first year in the European Union would save €90.04 million, allowing a high percentage of patients with access to rituximab [21].
In this study, we offered a comparison of the biosimilar and the reference rituximab in the age of biosimilar treatment. In GN patients, we have shown no differences between the two formulations in terms of laboratory markers or clinical results. Treatment costs for autoimmune illnesses are steadily increasing, which puts a strain on global healthcare budgets. This dilemma can be resolved using biosimilars, which lower the costs of therapy and enhance patient access to the therapy of rituximab.
Tables and Figures
Data Availability Statement
The availability of Data will be made on request.
Authors Contributions
All performed experimental work and the study was supervised by Tariq Al-Debasi and Mahmoud Mansour. The study design and project execution were carried out by Abeer Alzubaidi, Abdulsalam Alanazi, Abdulaziz Alarifi, Fahad Almutairi, Mohammed Alfaifi, Norah Aldeghaither, Yousef Al-Rajhi, and Saad Alnofaie. The final manuscript was read and approved by all named authors.
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or article publication: This work was supported by a grant from King Abdullah International Research Centre, National Guard Health Affairs, Riyadh, Saudi Arabia (grant no. SPR24/005/5).
![]() References
References
- Anders H-J, Kitching AR, Leung N, Romagnani P. Glomerulonephritis: immunopathogenesis and immunotherapy. Nature Reviews Immunology, (2023); 23(7): 453-471.
- Sanz I. Indications of rituximab in autoimmune diseases. Drug Discovery Today: Therapeutic Strategies, (2009); 6(1): 13-19.
- Geetha D, Jefferson JA. ANCA-associated vasculitis: core curriculum 2020. American Journal of Kidney Diseases, (2020); 75(1): 124-137.
- Stone JH, Merkel PA, Spiera R, Seo P, Langford CA, et al. Rituximab versus cyclophosphamide for ANCA-associated vasculitis. New England Journal of Medicine, (2010); 363(3): 221-232.
- Fervenza F, Cosio F, Erickson S, Specks U, Herzenberg A, et al. Rituximab treatment of idiopathic membranous nephropathy. Kidney international, (2008); 73(1): 117-125.
- Lafayette RA, Canetta PA, Rovin BH, Appel GB, Novak J, et al. A randomized, controlled trial of rituximab in IgA nephropathy with proteinuria and renal dysfunction. Journal of the American Society of Nephrology, (2017); 28(4): 1306-1313.
- Rovin BH, Furie R, Latinis K, Looney RJ, Fervenza FC, et al. Efficacy and safety of rituximab in patients with active proliferative lupus nephritis: the Lupus Nephritis Assessment with Rituximab study. Arthritis & Rheumatism, (2012); 64(4): 1215-1226.
- Fervenza FC, Appel GB, Barbour SJ, Rovin BH, Lafayette RA, et al. Rituximab or cyclosporine in the treatment of membranous nephropathy. New England Journal of Medicine, (2019); 381(1): 36-46.
- Committee for Medicinal Products for Human Use. European Medicines Agency. Guideline on similar biological medicinal products containing biotechnology-derived proteins as active substance: non-clinical and clinical issues. Accessed 26 May, 2024. https://www.tga.gov.au/sites/default/files/202407/rev1similar_biological_medicinal_products_containing_clinical_and_clinical_issues.pdf.
- US Food and Drug Administration. Drug Administration Guidance for industry: scientific considerations in demonstrating biosimilarity to a reference product. Accessed 10 Oct., 2024. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/scientific-considerations-demonstrating-biosimilarity-reference-product.
- Park W, Božić-Majstorović L, Milakovic D, Berrocal Kasay A, El-Khouri EC, et al. Comparison of biosimilar CT-P10 and innovator rituximab in patients with rheumatoid arthritis: a randomized controlled Phase 3 trial. Monoclonal Antibodies, (2018); 10(6): 934-943.
- Antonelou M, Abro A, Heath R, Iacovou A, Ashley C, et al. Comparison of outcomes using the rituximab originator MabThera with the biosimilar truxima in patients with ANCA-associated vasculitis. Scandinavian Journal of Rheumatology, (2022); 51(2): 135-141.
- Greenwald M, Tesser J, Sewell KL. Biosimilars have arrived: rituximab. Arthritis, (2018); 2018(1): 3762864.
- Kwon HC, Kim MK, Song JJ, Park Y-B, Lee S-W. Rituximab biosimilar prevents poor outcomes of microscopic polyangiitis and granulomatosis with polyangiitis as effectively as rituximab originator. Yonsei medical journal, (2020); 61(8): 712-719.
- Mittal S, Naidu GSRSNK, Jha S, Rathi M, Nada R, et al. Experience with similar biologic rituximab in 77 patients of granulomatosis with polyangiitis—a real-life experience. Clinical Rheumatology, (2021); 40(2): 645-651.
- Coiffier B. Pharmacokinetics, efficacy and safety of the rituximab biosimilar CT-P10. Expert Review of Clinical Pharmacology, (2017); 10(9): 923-933.
- Perez T, Rico A, Boutière C, Maarouf A, Roudot M, et al. Comparison of rituximab originator (MabThera®) to biosimilar (Truxima®) in patients with multiple sclerosis. Multiple Sclerosis Journal, (2021); 27(4): 585-592.
- Stubbs MJ, Low R, McGuckin S, Newton R, Thomas M, et al. Comparison of rituximab originator (MabThera) to biosimilar (Truxima) in patients with immune‐mediated thrombotic thrombocytopenic purpura. British Journal of Haematology, (2019); 185(5): 912-917.
- McAdoo SP, Bedi R, Tarzi R, Griffith M, Pusey CD, et al. Ofatumumab for B cell depletion therapy in ANCA-associated vasculitis: a single-centre case series. Rheumatology, (2016); 55(8): 1437-1442.
- Tabernero J, Vyas M, Giuliani R, Arnold D, Cardoso F, et al. Biosimilars: a position paper of the European Society for Medical Oncology, with particular reference to oncology prescribers. ESMO open, (2016); 1(6): e000142.
- Gulácsi L, Brodszky V, Baji P, Rencz F, Péntek M. The rituximab biosimilar CT-P10 in rheumatology and cancer: a budget impact analysis in 28 European countries. Advances in Therapy, (2017); 34(5): 1128-1144
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0