

Full Length Research Article
Diagnosis of Human Cases of Echinococcosis in Iraq (2021-2023): An Analysis of Gender, Age, and Affected Organs
A.O. Humide1, Thaer Abdulqader Salih2*, Ezeddin A. Albayyar3
Adv. life sci., vol. 12, no. 2, pp. 435-439, May 2025
*– Corresponding Author: Thaer Abdulqader Salih (Email: sc.thaerparasit@uoanbar.edu.iq)
Authors' Affiliations 1. Department of Quality Assurance and Performance, University of Fallujah, Iraq
2. College of Education for pure sciences, University of Anbar, Iraq
3. College of Science, University of Anbar, Iraq
2. College of Education for pure sciences, University of Anbar, Iraq
3. College of Science, University of Anbar, Iraq
[Date Received: 27/08/2023; Date Revised: 18/02/2025; Date Available Online: 31/08/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Cystic echinococcosis is a chronic zoonotic disease in humans caused by infection with canine tapeworm larvae. The species of echinococcus has a two-host life cycle. Cystic echinococcosis (CE) is classified as an emergent condition since cysts can develop to a size of 5 to 10 cm during the first year of infection and continue to grow for years or even decades before the illness is spotted affecting several organs.
Methods: 52 patients who were admitted to Al-Ramadi Teaching Hospital, Fallujah Teaching Hospital, and other nearby private hospitals between 2021/7/8 and 2023/8/21 are the subject of this article. Cysts from various organs in patients of both sexes and of varied ages were removed, some of which included the cysts of echinococcosis infected persons.
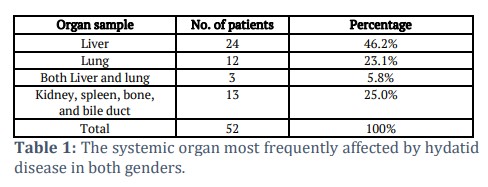
Results: According to our research, the liver was the organ that had hydatid cyst infections most commonly, with a damage frequency of 46.2%. According to the statistics, the prevalence of infection in the other organs, which were listed after the liver, was 25.0% (spleen, bone, and bile duct) and 23.1% cases were of lung infection. It was found that the likelihood of liver and lung injuries happening concurrently was the lowest (5.8%) of all the infections.
Conclusion: The study shows hydatid disease primarily affects the liver and lungs, with females and the 20–40 age group being the most impacted. Infection rates increased from 2021 to 2023. Surgery remains the main treatment, though medical therapies have varied success, especially for lung cases. Gender, age, and cyst location significantly influence disease outcomes.
Keywords: Echinococcus granulosus; Mortality; Hydatid cysts; Human cystic echinococcosis
Introduction![]()
This particular illness is zoonotically significant because it has an impact on both human health and the economy [1]. Canine tapeworm larvae infection is the primary source of chronic zoonotic illness known as human cystic echinococcosis [2]. A well-defined two-host life cycle may be seen in Echinococcus species. [3]. Adult tapeworms (3-6 mm long) reside in the small intestine of carnivorous definitive hosts like dogs or wolves, while echinococcal cyst stages are present in herbivorous intermediate hosts including sheep, cattle, and goats, in many regions of the world [4]. In the typical dog-sheep cycle, tapeworm eggs are passed in an infected dog’s feces and may then be consumed by grazing sheep. These eggs hatch into embryos in the intestine, penetrate the intestinal lining, and are then picked up and transported by blood throughout the body to major filtering organs (primarily the liver and/or lungs). The growing embryos change into larval echinococcal cysts after localizing in a particular organ or place, where a large number of microscopic tapeworm heads (known as protoscolices) are formed by asexual reproduction. [5,6]. These protoscolices are infectious to dogs that consume viscera containing echinococcal cysts. Once ingested, the protoscolices develop into adult tapeworms, which are then capable of releasing infectious eggs into the environment through the dog's feces. Few places, like Iceland, Ireland, and Greenland, are thought to be devoid of autochthonous human CE, even though E. granulosus is thought to have a global distribution [7]. After an incubation period comprising several months or years, depending on the rate of cyst development and the immunological response of the host, clinical indications start to appear. Similar observations were reported in other endemic infection locations, according to Romig et al., and Zhang et al., [8,9]. In most of the bigger patient series, new opportunities for transmission research have emerged as a result of recent advancements in the detection of E. granulosus antigens or DNA in the feces of foxes and other definitive hosts. It has been advised to think about chemotherapy with albendazole as the initial treatment option. ELISA was employed as a screening tool using a multimodality imaging method, such as ultrasound (US), computed tomography (CT), magnetic resonance (MR), and endoscopic retrograde cholangiopancreatography. Diagnostic cues like respiratory symptoms, hepatomegaly, eosinophilia, and radiological suspicion of cystic lesions in the liver or lungs are used to guide the imaging diagnosis (ERCP). When the lesions are modest, surgery should be done, and in general, side effects of albendazole treatment are minimal [10,11]. Studies on AE cases that are incurable have revealed that, in the majority of instances, improvement or stability of the condition requires long-term therapy with mebendazole (or albendazole) over a period of years or for the rest of one’s life [12]. This study aimed to diagnose the human cases of Echinococcosis between 2021-2023 in Iraq.
![]()
Methods
Between 2021 and 2023, information on the disease's prevalence in the city was collected from Fallujah Teaching Hospital, Ramadi Teaching Hospital, and a number of private facilities. During procedures to remove cysts from various organs in patients of both sexes, 52 infected patients' cysts were collected according to approval obtained from the ethical committee at Fallujah Teaching Hospital. Furthermore, information quality may differ based on hospital location, treatment standards and the quality of treatment service. However, the majority of data came from each population's yearly number of cases relevant to this model of study and from patients who have severe clinical diseases but are typically unable to acquire early diagnosis. Such cases were not formally identified and did not receive medical care [13,14]. Due to a lack of access to healthcare and poverty, early treatment was not possible in these patients. In Iraq, human CE cases may not be consistently reported by the healthcare facility, and hospital diagnoses are not often recorded in regional or national databases or public reporting [15,16]. As a result, there is a fundamental lack of information in World Health Organization reports on the epidemiology and severity of the disease's spread throughout Iraq, not only in the city of Fallujah but in all of Iraq, either in terms of reporting known treated cases or documenting them.
Statistical Analysis
In order to evaluate the data using SPSS 16 with a significance threshold of less than 0.05, descriptive statistics and the Chi-square test were used.
The data provides a comprehensive overview of the distribution of hydatid disease cases across various demographics, organ involvement, and time periods.
In terms of organ infection, the liver is the most commonly affected, with 46.2% of cases (24 patients). This is followed by the lungs, which account for 23.1% of cases (12 patients). A smaller percentage of patients (5.8%, or 3 patients) exhibited infection in both the liver and lungs. Kidneys and spleen were affected in 25% of the cases (13 patients), rounding out the total of 52 patients affected by hydatid disease (Table 1).
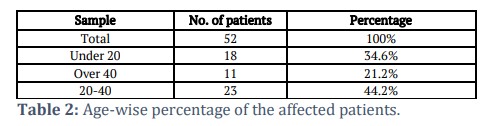
When looking at the age distribution, the most affected group was between 20 and 40 years old, comprising 44.2% (23 patients) of the cases. Patients under 20 years of age represented 34.6% (18 patients), while those over 40 accounted for 21.2% (11 patients). This suggests that young to middle-aged adults are more susceptible to hydatid disease (Table 2).
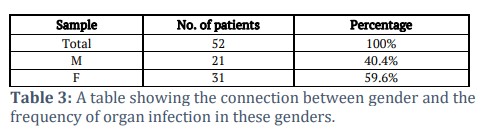
Gender-wise, there is a higher prevalence of infection among females, who made up 59.6% (31 patients) of the cases, compared to males, who represented 40.4% (21 patients). This indicates that hydatid disease is more common in females in this sample (Table 3).
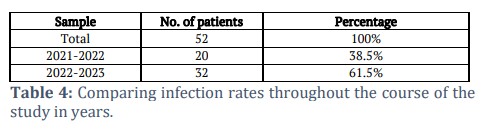
Finally, the study period reveals a sharp increase in infection rates from 2021 to 2023. During 2021–2022, 38.5% of cases (20 patients) were recorded, but in 2022–2023, the number of infections surged to 61.5% (32 patients). This substantial rise highlights the growing prevalence of hydatid disease over the course of the study (Table 4).
According to statistics collected during the time period, the infection rate in 2022–2023 was exceptionally high, reaching 61.5% as opposed to rates in 2021–2022, which reached 38.5%.
![]() Discussion
Discussion
The size and location of the developing cysts affect the clinical signs of hydatid illness. Certain cysts, such as those that cause cirrhosis, bronchial blockage, renal outflow obstruction, elevated intracranial pressure, and hydrocephalus, may result in the malfunction of the organs they are attached to. Anaphylaxis is a side effect of the free rupture of the echinococcal cyst, and it can also release tiny cysts that can spread to other organs [17]. Cysts that are near the pleural membranes might rupture and result in pleural effusion, reactive inflammation, or secondary bacterial infection. If the contents of the cyst leak into the surrounding tissues, either naturally through rupture, extension, and invasion, or artificially through iatrogenic pleural infestation during surgery, secondary lesions may form [18,19]. Lung cysts can burst, releasing tissue fragments that can cause hemoptysis, vomiting, coughing, and chest discomfort. They can also flow into the pleural cavity, where they can cause simple or tension pneumothorax, pleural effusion, or empyema. A higher intracystic pressure is the underlying cause of the compression and necrosis of the walls of nearby bile ducts, integration of tiny biliary ducts into the pericyst, and finally rupture of the biliary ducts [20,21]. Small fissures, which are often asymptomatic, or perforation (i.e., frank communication), which may produce obstructive jaundice and cholangitis, are clinically two possible manifestations of communicating rupture within the biliary system. Hydatid cyst illness has been treated with surgery and medication [22]. According to the city’s computerized archiving system, not all surgical operations performed on patients were recorded after they left the institutions. With the exception of the Fallujah Teaching Hospital, information is written down on paper at the other hospitals. Although the percentage of operations to remove cysts from patients is partially documented, cases were not recorded in the World Health Organization’s records and reports, as in the case in Fallujah and throughout Iraq, which is why it is impossible to assess the extent of the disease’s spread in either Fallujah specifically or Iraq generally. Depending on the procedure used, the mortality rates of surgical patients may increase significantly [23]. Since 1977, albendazole and mebendazole have been widely used to treat hydatid cysts [24]. The original treatment was mebendazole (MBZ), but over time it was shown to be less successful than albendazole (10–15 mg/kg/day, with a maximum of 800 mg orally in two doses) [25]. The medicine is ineffective because MBZ is insoluble in water and has low solubility and bioavailability [26]. The treatment response was better in pulmonary (83%) than in hepatic (18%) regions for small cysts less than 5 cm in size, according to MBZ [27]. Among 52 patients, the liver was affected in 46.2% of cases. Lungs alone (23.1%) were the second most affected organ, according to this data [28]. Following the development and proliferation in the liver, infection spreads to other organs at a 25.0% rate (Table 1), The spleen, pancreas, and other abdominal and thoracic organs may be affected by cysts that breach the liver capsule and continue exogenous growth in the peritoneal cavity [22,29,30], complications from a hepatic hydatid cyst. In around 40% of instances, liver echinococcal cysts can result in problems [31]. Infection, biliary tree rupture, peritoneal cavity rupture, pleural cavity rupture, and lung rupture are the most frequent consequences in that regard (13%). [31,32]. According to the findings, the age group of 20 to 40 had the greatest proportion of illness infection at 44.2%, with the remaining age groups following suit: According to Table 2 (34.6% of those under 20 years old and 21.2% of those over 40). According to earlier research, infection incidence can be significantly influenced by an individual’s age [33]. Data analysis of Table 3 demonstrates that incidence rates with age differences were greater in females (59.6%) than in males (40.4%). By accepting the conclusion reached by researchers examining the influence of sex hormones in mice with hydatid cysts that female hormones enhance the infection of E. granulosus , the findings may be explained. [32]. In order to maintain a favorable environment for its survival, E. granulosus possesses a method through which it promotes the adrenal gland synthesis of estradiol and testosterone [34]. According to reports, women are more vulnerable to illness than men [9]. The sex of the host has a significant role in the susceptibility and kind of reaction to parasitism; in this situation, females are more likely than men to get infected with the metacestode of E. granulosus . The females had a greater granulomatous response than the men did, but this was insufficient to kill the parasite or stop its proliferation [35]. E. granulosus is a member of the cestode family and mostly affects the liver and lungs. Following infection, the parasite develops a number of evasion strategies that influence how long it remains in the host organs. The infection rate in 2022–2023 was exceptionally high, reaching 61.5% compared to rates in 2021–2022, which reached 38.5%, as shown in Table (4). Age, gender, infection intensity, cyst size, and the bodily organ implicated all affect the disease's epidemiological, clinical, and pathological symptoms [36].
This study revealed that the infection predominantly affected the liver and lungs but in some cases, extended to other organs. Females were more infected, probably due to hormonal influences. The most affected age group was between 20–40 years. Infection rates were on the rise from 2021–2023. Surgical treatment is the mainstay of treatment, whereas medical therapies give variable results, especially regarding lung cysts. The important variables that define the outcome of the disease are gender, age, and location of the cysts.
Tables and Figures
Competing Interest
The author declares no conflict of interest.
Acknowledgement
Thanks, and gratitude to the Anbar Health Department / Research and Development Center for the facilities provided, as well as to the staff of surgeons in the hospitals (Fallujah Teaching, Ramadi Teaching).
Authors Contributions
![]() References
References
- Thompson RC. Biology and systematics of Echinococcus. Advances in parasitology, (2017); 95(2017): 65-109.
- Savioli L, Daumerie D. Investing to overcome the global impact of neglected tropical diseases: third WHO report on neglected tropical diseases. 2015; 3(2015): 211. World Health Organization
- Singh SK, Singh V, Kumar S, Devenraj V, Bhandari M, et al. Right ventricular hydatid cyst presented as tachyarrhythmia. Asian Cardiovascular and Thoracic Annals, (2019); 27(6): 489-491.
- Casulli A, Siles-Lucas M, Tamarozzi F. Echinococcus granulosus sensu lato. Trends in parasitology, (2019); 35(8): 663-664.
- Mahdi ZMS, Al-Hamairy AK, Al-Rubaiey HM. Genotyping of Echinococcus granulosus Isolates from Human, Sheep and Cattles Hydatid Cysts in Some Central Euphrates Provinces, Iraq. Medico-legal Update, (2020); 20(2): 570-575.
- Agudelo Higuita NI, Brunetti E, McCloskey C. Cystic echinococcosis. Journal of clinical microbiology, (2016); 54(3): 518-523.
- Akcam AT, Ulku A, Koltas IS, Izol V, Bicer OS, et al. Clinical characterization of unusual cystic echinococcosis in southern part of Turkey. Annals of Saudi medicine, (2014); 34(6): 508-516.
- Romig T, Deplazes P, Jenkins D, Giraudoux P, Massolo A, et al. Ecology and life cycle patterns of Echinococcus species. Advances in parasitology, (2017); 95(2017): 213-314.
- Zhang T, Zhao W, Yang D, Piao D, Huang S, et al. Human cystic echinococcosis in Heilongjiang Province, China: a retrospective study. BMC gastroenterology, (2015); 15(1): 1-5.
- Abdulhameed MF, Habib I, Al-Azizz SA, Robertson I. A retrospective study of human cystic echinococcosis in Basrah province, Iraq. Acta tropica, (2018); 178(2018): 130-133.
- Lopez-Bernus A, Belhassen-García M, Alonso-Sardón M, Carpio-Perez A, Velasco-Tirado V, et al. Surveillance of human echinococcosis in Castilla-Leon (Spain) between 2000-2012. PLoS Neglected Tropical Diseases, (2015); 9(10): e0004154.
- Alvela-Suárez L, Velasco-Tirado V, Belhassen-Garcia M, Novo-Veleiro I, Pardo-Lledías J, et al. Safety of the combined use of praziquantel and albendazole in the treatment of human hydatid disease. The American journal of tropical medicine and hygiene, (2014); 90(5): 819.
- Jiang B, Zhou X-N, Zhang H-B, Tao Y, Huo L-L, et al. Slow-release praziquantel for dogs: presentation of a new formulation for echinococcosis control. Infectious diseases of poverty, (2017); 6(05): 10-20.
- Harmouchi H, Kouache ME, Lakranbi M, Ouadnouni Y, Smahi M. Cardiac hydatid cyst interposed between the right atrium and right ventricle on the tricuspid valve. Asian Cardiovascular and Thoracic Annals, (2022); 30(2): 199-201.
- L’aarje A, Lyazidi S, Kitane Y, Alami A, Habbal R. Cardiac hydatid cyst of the right ventricle: Severe localization. Journal of cardiology cases, (2017); 16(4): 138-140.
- Jamli M, Cherif T, Ajmi N, Besbes T, Mgarrech I, et al. Surgical management and outcomes of cardiac and great vessels echinococcosis: A 16-year experience. The Annals of Thoracic Surgery, (2020); 110(4): 1333-1338.
- Mortezaei S, Afgar A, Mohammadi MA, Mousavi SM, Sadeghi B, et al. The effect of albendazole sulfoxide on the expression of miR-61 and let-7 in different in vitro developmental stages of Echinococcus granulosus. Acta tropica, (2019); 195(2019): 97-102.
- Bălan H, Gurghean A. Anaphylactic shock: are we doing enough and with the right timing and order?. Romanian Journal of Internal Medicine, (2015); 53(3): 191-198.
- Loos JA, Dávila VA, Rodrígues CR, Petrigh R, Zoppi JA, et al. Metformin exhibits preventive and therapeutic efficacy against experimental cystic echinococcosis. PLoS Neglected Tropical Diseases, (2017); 11(2): e0005370.
- Saglican Y, Yalçin Ö, Kaygusuz E. Cystic Echinococcosis: one entity, two unusual locations. Türkiye Parazitolojii Dergisi, (2016); 40(1): 51.
- Lu YM, Zhang L, Xing Q, Zhou XH, Li Y-D, et al. Ventricular tachycardia as the initial symptom of cardiac hydatidosis. Chinese Medical Journal, (2019); 132(22): 2765-2766.
- Stiru O, Geana RC, Antohi L, David L, Goicea M, et al. Incidentally detected cardiac and hepatic hydatid cyst after sudden onset facial paralysis: A case report. Archives of Clinical and Medical Case Reports, (2019); 3(4): 190-198.
- Sonsoz MR, Gunes SC. An intra‐cardiac mass in a patient with Behçet’s disease: Cardiac hydatid cyst. Echocardiography, (2020); 37(4): 646-648.
- Khazaei S, Rezaeian S, Khazaei Z, Goodarzi E, Khazaei S, et al. Epidemiological and clinical characteristics of patients with hydatid cysts in Khorasan Razavi Province, from 2011 to 2014. Iranian Journal of Parasitology, (2016); 11(3): 364.
- Köroğlu M, Erol B, Gürses C, Türkbey B, Baş CY, et al. Hepatic cystic echinococcosis: percutaneous treatment as an outpatient procedure. Asian Pacific Journal of Tropical Medicine, (2014); 7(3): 212-215.
- Nayman A, Guler I, Keskin S, Erdem TB, Borazan H, et al. A novel modified PAIR technique using a trocar catheter for percutaneous treatment of liver hydatid cysts: a six-year experience. Diagnostic and Interventional Radiology, (2016); 22(1): 47.
- Modani S, Karthik DK, Heda S, Deshpande A. Atypical chest pain in a patient with hydatid cyst of the interventricular septum. Case Reports, (2018); 2018(1): 1-3.
- Piccoli L, Tamarozzi F, Cattaneo F, Mariconti M, Filice C, et al. Long-term sonographic and serological follow-up of inactive echinococcal cysts of the liver: hints for a “watch-and-wait” approach. PLoS neglected tropical diseases, (2014); 8(8): e3057.
- Gurzu S, Beleaua MA, Egyed-Zsigmond E, Jung I. Unusual location of hydatid cysts: report of two cases in the heart and hip joint of Romanian patients. The Korean Journal of Parasitology, (2017); 55(4): 429.
- Kahlfuß S, Flieger RR, Roepke TK, Yilmaz K. Diagnosis and treatment of cardiac echinococcosis. Heart, (2016); 102(17): 1348-1353.
- Akkapulu N, Aytac HO, Arer IM, Kus M, Yabanoglu H. Incidence and risk factors of biliary fistulation from a hepatic hydatid cyst in clinically asymptomatic patients. Tropical doctor, (2018); 48(1): 20-24.
- Kulali F, Acar A, Semiz-Oysu A, Canbak T, Tolan K, et al. Misleading findings of liver-specific MR contrast agent for radiological diagnosis of cysto-biliary communication in hydatid cysts. La radiologia medica, (2019); 124(2019): 460-466.
- Alghofaily KA, Saeedan MB, Aljohani IM, Alrasheed M, McWilliams S, et al. Hepatic hydatid disease complications: review of imaging findings and clinical implications. Abdominal Radiology, (2017); 42(2017): 199-210.
- Rodríguez Carnero P, Hernández Mateo P, Martín-Garre S, García Pérez Á, Del Campo L. Unexpected hosts: imaging parasitic diseases. Insights into Imaging, (2017); 8(2017): 101-125.
- Fennira S, Sarray H, Kammoun S, Zoubli A, Kammoun Y, et al. A large cardiac hydatid cyst in the interventricular septum: A case report. International journal of infectious diseases, (2019); 78(2019): 31-33.
- Liu S, Zhou X, Hao L, Piao X, Hou N, et al. Genome-wide transcriptome analysis reveals extensive alternative splicing events in the protoscoleces of Echinococcus granulosus and Echinococcus multilocularis. Frontiers in Microbiology, (2017); 8(2017): 929.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0