

Full Length Research Article
Analyzing the Possible Impact of Herpes Simplex Virus-1 in Relation to Interleukin-6 Levels in Patients with Oral Squamous Cell Carcinoma
Marwa Mohammed Ali Jassim1, Shireen Ahmed Dzayee2, Majid Mohammed Mahmood3*
Adv. life sci., vol. 12, no. 2, pp. 440-444, May 2025
*– Corresponding Author: Majid Mohammed Mahmood (Email: majidmahmood93@yahoo.com)
Authors' Affiliations 1. College of Dentistry, Al-Muthanna University, Al-Muthanna – Iraq
2. Department of Physiology, Microbiology and Genetics, College of Medicine Hawler Medical University Erbil – Iraq
3. Department of Biology, College of Science, Mustansiriyah University, Baghdad – Iraq
2. Department of Physiology, Microbiology and Genetics, College of Medicine Hawler Medical University Erbil – Iraq
3. Department of Biology, College of Science, Mustansiriyah University, Baghdad – Iraq
[Date Received: 21/09/2024; Date Revised: 13/12/2024; Date Available Online: 31/08/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Oral squamous cell carcinoma (OSCC) is the most common malignant tumor of the oral cavity, accounting for more than 90% of all cases. Oral herpes is caused by herpes simplex virus type 1 (HSV-1), a common, benign virus that affects the skin and mucous membranes of individuals with weakened immune systems, causing ulcers. There are several cellular processes that rely on the pleiotropic cytokine interleukin-6 (IL-6), including migration, invasion, differentiation, proliferation, and survival. By modifying tumor angiogenesis and tumor lymphangiogenesis, IL-6 controls tumor growth and its effects on tumor cells.
Methods: The study involved 60 patients divided into two groups: those with and those without oral cancer. The blood was drawn and examined for HSV-1 Immunoglobulin G levels using the Herpe Select-1 ELISA kit. A sandwich ELISA was also employed to study IL-6 levels.
Result: HSV-1 incidence in these oral squamous cell carcinoma grade groups increased significantly. This research found that the OSCC group had somewhat greater IL-6 levels than the control groups.
Conclusion: HSV-1 is not carcinogenic in its own right; however, it is linked to an increased risk of oral squamous cell carcinoma. In addition, the present study discovered that the pro-inflammatory cytokine IL-6 was present in greater quantities in patients' blood than in controls. Interleukin-6 was identified as a potentially hazardous factor in the development of oral cancer and has the potential to function as a valuable biomarker for the assessment of OSCC severity.
Keywords: Oral squamous cell carcinoma; Interleukin 6; Enzyme-Linked Immunosorbent Assay; Herpes simplex virus-1; IgG
Introduction![]()
The sixth most common cancer is oral cancer worldwide. Mouth cancer remains a deadly and disfiguring illness in Iraq despite regional differences. The progression of OSCC is modulated by viral infections, genetic variations, and environmental factors [1]. Based on the findings from the in vitro cell cultures and patient examinations it is evident that HSV-1 can contribute to cancer development by enhancing the tumorigenic potential of other risk factors and there is evidence that HSV-1 antibody levels are related to oral cancer [2]. It may increase the incidence of head and neck cancer by inducing chromosomal mutation, gene amplification and oncogene overexpression in neoplastic tissue [3, 4]. Although HSV-1 is not thought to be an oncogenic virus by itself, it may predispose to malignant development in the research by Brown et al., and others [5-8]. This is because the virus remains in the oral mucosa and stimulates host cell DNA synthesis and repair.
The term "host cutoff" in the context of viral infections generally refers to the point at which a virus can no longer effectively infect a host or replicate within a host organism. This can occur due to (immune response, viral adaptation, host factors, and therapeutic interventions) [7].
Cytokines play a crucial role in managing the tumor microenvironment and preventing long-term pro-tumorigenic inflammation. Polypeptides, which are low molecular weight proteins produced by the immune system, tissue, and tumor cells, are involved in the regulation of cellular behavior, growth, differentiation, and function; however, their production during inflammation or carcinogenesis can be detrimental to physiological activities [9]. In lung cancer, hepatocellular carcinoma, colorectal cancer and oral squamous cell carcinoma (OSCC), the progression of these cancers has been associated with proinflammatory cytokines, as studied. IL-6 can interact with cell receptors via autocrine or paracrine pathways, facilitating the transmission and exchange of intercellular signals, potentially completing cell biological activities. IL-6 is linked to tumor formation, differentiation, apoptosis, immune response, and treatment resistance, according to a recent investigation [10].
One of the indications indicated as being useful for early diagnosis and predicting prognosis in OSCC patients is interleukin (IL-6) expression. Various investigations confirmed that those who suffer from OSCC have higher IL-6 levels than healthy controls [11, 12]. As with Harini et al., it is revealed that the fundamental oncogene in the composition of malignancies such as OSCC is IL-6. Therefore, IL-6 can be considered beneficial for diagnosis or prognosis [13]. Moreover, Xiao et al., confirmed that IL-6 is the main oncogene for the OSCC biological processes. Thus, it was suggested as a potential biomarker for identifying OSCC [14]. The investigation was an endeavor for assessing the blood IL-6 levels effects on the differential diagnosis of OSCC.
In this present study, the levels of HSV-1 IgG in the blood of thirty persons suffering from OSCC and thirty healthy controls are examined. Both groups were from the same age and lived in the same area. Then, Moreover, the identified concentrations of IL-6 in the blood of both groups were examined.
![]() Methods
Methods
The study identified 60 individuals (30 with OSCC and 30 controls) using Human Anti-Herpes Simplex Virus Type 1 IgG ELISA Kits, Abcam, UK. IL-6 serum expression levels were evaluated employing a human Sandwich IL-6-ELISA Kit application (purchased from Abcam, UK) (Cat. No.: ab178013). The assessment was performed in compliance with the manufacturer's guidelines.
Statistical Analysis:
To perform statistical analysis on the data collected in this investigation, the program SPSS (version 24) was applied. The variables' significance was assessed using Chi-Square, and the mean was calculated. Statistical tests were conducted to confirm noteworthy alterations in categorical variables among groups and ROC analysis was used to establish the ideal cutoff for OSCC patients, which demonstrates excellent specificity and sensitivity.
Assessment of Serum Interleukin-6 in study groups:
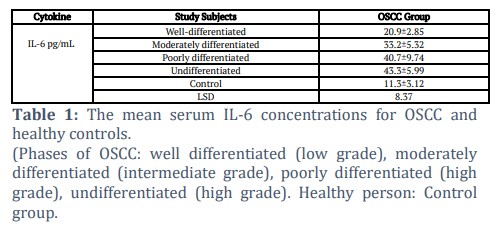
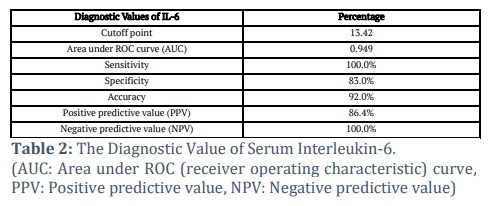
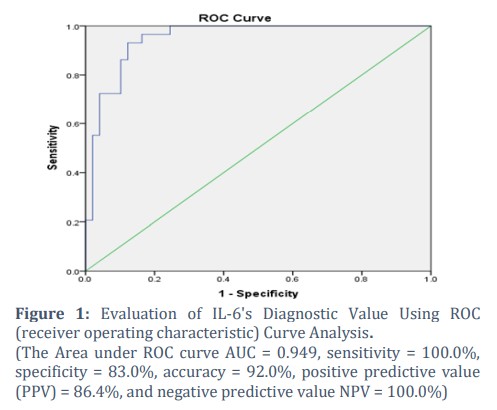
The study showed that oral squamous cell carcinomas have different levels of mean IL-6 in different stages of the disease; well, moderately, poorly and undifferentiated. Table 1 presents the mean serum IL-6 concentrations for OSCC and healthy controls, revealing a difference in serum interleukin-6 levels in OSCC tissues of all grades associated with the Healthy individual group. Diagnostic efficacy of the IL-6 (ROC) test is illustrated in Table 2 and Figure 1, with a positive predictive value (PPV) of 86.4%, a negative predictive value (NPV) of 100.0%, sensitivity of 100.0%, specificity of 83.0%, accuracy of 92.0%, and an area under the ROC curve (AUC) of 0.949. The genuine positive rate is signified by sensitivity, while the specificity means the true negative rate of IL-6. However, AUC > 0.8 to IL-6, indicates excellent model performance to use it as a good marker for diagnostic OSCC.
Detection of HSV-1 IgG in Studied groups:
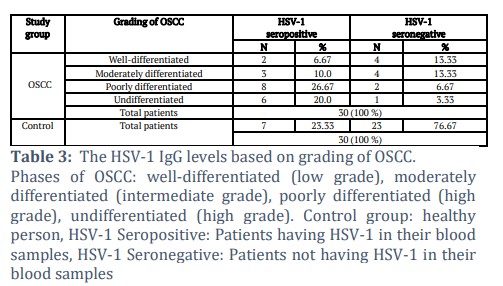
In the current investigation, significant differences were observed between the OSCC groups and the healthy control group (P˂0.05). Among the 30 OSCC patients studied 6.67%, 10.0%, 26.67%, and 20.0% tested positive for HSV1 antibodies in well, moderately, poorly, and undifferentiated grades of OSCC, respectively. At the same time, the seronegative percentages were (13.33%, 13.33%, 6.67%, and 3.33%) for well, moderately, poorly, and undifferentiated grade groups of OSCC. Besides that, among the 30 control participants, 7 (23.33%) were HSV1 antibody-positive, while 23 (76.67%) were seronegative for HSV1, as illustrated in Table 3.
![]() Discussion
Discussion
ROC curve analysis, specificity, and sensitivity calculations suggest that serum IL-6 is the most precise predictor of oral cancer. This and previous studies show that OSCC and other malignancies may be diagnosed using IL-6.
High levels of IL-6 have been associated with a poor prognosis in many types of cancer, including cancers of the stomach, kidney, colon, prostate, and non-small cell lung, as well as melanomas, skin, head, and neck cancers, and hematologic malignancies such as myeloma and non-Hodgkin's lymphoma. Researchers have found a link between elevated IL-6 levels and Hodgkin's lymphoma. Many studies have shown a connection between a person's blood IL-6 genotype and the risk of infected cancer [15-20].
Serum IL-6 can start a tumor by paracrine or autocrine mechanisms and impede the immune response against it. Therefore, it likely contributes to or indicates how cancer grows and operates [21]. IL-6 stops dendritic cells from growing, which makes the immune system less sensitive to cancer and speeds up the spread of metastatic disease [22]. Even though it has been shown that most serum comes from tumors, it has also been found that monocytes in people with head and neck SCC release more than in healthy people [23]. Reduced cellular immunity and abnormal monocyte function are well-known to be frequent and early characteristics of OSCC patients [24, 25].
This study, like others, demonstrates that IL-6 levels can be correlated with the aggressiveness and severity of a disease. The current investigation found that these pro-inflammatory cytokines are greater in OSCC patients' blood than in controls, suggesting they have diagnostic and/or prognostic value, which large multicenter studies must verify.
Recent research has looked at the effect of histopathological variables on OSCC patients' overall survival, with tumor differentiation impacting clinical behavior. Since the 1960s, HSV1 has been thought to contribute to the development of OSCC. Only some epidemiological studies have been done to test this idea. The Herpes simplex virus is a virus that replicates by copying its DNA in an envelope. When it invades a cell, it triggers a series of intricate reactions. HSV-1 usually causes infections in the mouth. It has been investigated as a potential method for HSV transformation to induce cellular proteins (such as heat shock proteins) [26]. Another significant component brought on by HSV is known to be the host cell cutoff. The infected cell ceases protein synthesis, and cell RNA is rapidly destroyed. Another HSV activity that may be connected to cell transformation is viral replication stimulation. An enhancement in immune response can be attributed to the higher levels of IL-6 and HSV-1 infections in OSCC patients in the current investigation. Also, it has been thought that HSV1’s ability to cause mutations could directly change cells into cancerous ones as in the results of this study possibly by causing chromosomal rearrangements or amplifying host genes that cause cancer [27, 28].
Jalouli et al., used biopsy to find out how often HSV caused OSCC. These results demonstrate the prevalence of HSV infections, which may have consequences for oral health and the emergence of malignancy [29]. This study matches these findings. Eglin and coworkers examined OSCC biopsy samples for HSV1-complementary RNA using in situ hybridization. Approximately 50% of oral squamous cell carcinomas had HSV RNA [30]. For the first time, Delavarian et al., investigated OSCC viruses in 21 formalin-fixed, paraffin-embedded sections of adolescent Iranian patients [31].
Finally, this study has also offered some data on HSV-1 infection in OSCC patients. This is because HSV-1 is involved in OSCC due to the significant variance in IL-6 levels between control and patient groups. More data is, however, desired to completely comprehend the HSV-1’s role in OSCC.
Tables and Figures
Acknowledgement
The College of Science at Mustansiriyah University provided funding for the present study, and the authors are appreciative of the Deanship's technical help.
Authors Contributions
Conceptualization: Marwa Mohammed Ali Jassim, Shireen Ahmed Dzayee, Majid Mohammed Mahmood.
Data Curation: Majid Mohammed Mahmood, Marwa Mohammed Ali Jassim, Shireen Ahmed Dzayee.
Formal Analysis: Marwa Mohammed Ali Jassim, Shireen Ahmed Dzayee, Majid Mohammed Mahmood.
Funding Acquisition: Shireen Ahmed Dzayee, Marwa Mohammed Ali Jassim, Majid Mohammed Mahmood.
Investigation: Mohammed Ali Jassim, Majid Mohammed Mahmood, Shireen Ahmed Dzayee.
Methodology: Majid Mohammed Mahmood, Marwa Mohammed Ali Jassim, Shireen Ahmed Dzayee.
Project Administration: Marwa Mohammed Ali Jassim, Majid Mohammed Mahmood, Shireen Ahmed Dzayee.
Resources: Shireen Ahmed Dzayee, Marwa Mohammed Ali Jassim, Majid Mohammed Mahmood.
Competing interest
![]() References
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians, (2021); 71(3): 209-249.
- Koivikko T, Rodrigues PC, Vehviläinen M, Hyvönen P, Sundquist E, et al. Detection of herpes simplex virus in oral tongue squamous cell carcinoma. Frontiers in Pharmacology, (2023); 14(2023): 1182152.
- Yan M, Xiao LY, Gosau M, Smeets R, Feng HC, et al. The role of herpes simplex virus infection in the etiology of head and neck cancer–a Mendelian randomization study. Frontiers in Immunology, (2024); 15(2024): 1278327.
- Imbesi Bellantoni M, Picciolo G, Pirrotta I, Irrera N, Vaccaro M, et al. Oral cavity squamous cell carcinoma: an update of the pharmacological treatment. Biomedicines, (2023); 11(4): 1112-1117.
- Brown SH, States VA, Afghan AK, Satyanarayana G. Herpes simplex virus-infected squamous cell carcinoma: a case report. BMC Infectious Diseases, (2022); 22(1): 1-25.
- Jassim MMA, Naji SA, Mahmood MM. BRCA1, BCL2, and the RB Tumor Suppressor have abnormal expressions in lung cancer. Research Journal of Pharmacy and Technology, (2022); 15(9): 4083-4087.
- Jain M. Assessment of correlation of herpes simplex virus-1 with oral cancer and precancer-a comparative study. Journal of clinical and diagnostic research, (2016); 10(8): ZC14-7.
- Kazem SH, Hussein MH. Immunological Role of IL-17A and Biochemical Factors in Patients with Renal Failure Induced by Systemic Lupus Erythematosus. Iranian Journal of War and Public Health, (2024); 16(1): 61-65.
- Abdul-Razzaq LN, Jassim MMA, Mahmood MM. The High Presence of HCMV pp71 Proteins, Correlate with P63 Expression in Pancreatic Cancer Tumor Tissue. Asian Pacific Journal of Cancer Prevention, (2023); 24(4): 1443–1447.
- Riedel F, Zaiss I, Herzog D, Götte K, Naim R, et al. Serum levels of interleukin-6 in patients with primary head and neck squamous cell carcinoma. Anticancer research, (2005); 25(4): 2761-2765.
- Singh PK, Chandra G, Bogra J, Gupta R, Kumar V, et al. Association of interleukin-6 genetic polymorphisms with risk of OSCC in Indian population. Meta Gene, (2005); 4(2005): 142-151.
- Dineshkumar T, Ashwini BK, Rameshkumar A, Rajashree P, Ramya R, et al. Salivary and serum interleukin-6 levels in oral premalignant disorders and squamous cell carcinoma: diagnostic value and clinicopathologic correlations. Asian Pacific journal of cancer prevention, (2016); 17(11): 4899–4906.
- Harini P, Neralla M, Preethi A, Selvakumar SC. Impact of Interleukin-6 on Oral Squamous Cell Carcinoma Among the South Indian Population. Cureus, (2024); 16(7): 1-6.
- Xiao L, Li X, Cao P, Fei W, Zhou H, et al. Interleukin-6 mediated inflammasome activation promotes oral squamous cell carcinoma progression via JAK2/STAT3/Sox4/NLRP3 signaling pathway. Journal of Experimental & Clinical Cancer Research, (2022); 41(1): 166.
- St John MA, Li Y, Zhou X, Denny P, Ho CM, et al. Interleukin 6 and interleukin 8 as potential biomarkers for oral cavity and oropharyngeal squamous cell carcinoma. Archives of Otolaryngology–Head & Neck Surgery, (2004); 130(8): 929-935.
- Lippitz BE. Cytokine patterns in patients with cancer: a systematic review. The lancet oncology, (2013); 14(6): 218-228.
- Maccio A, Madeddu C. The role of interleukin-6 in the evolution of ovarian cancer: clinical and prognostic implications – a review. Journal of Molecular Medicine, (2013); 91(2013): 1355-1368.
- Ohishi W, Cologne JB, Fujiwara S. Serum interleukin-6 associated with hepatocellular carcinoma risk: a nested case-control study. International Journal of Cancer, (2014); 134(1): 154-163.
- Tripsianis G, Papadopoulou E, Anagnostopoulos K. Coexpression of IL-6 and TNF-alpha: prognostic significance on breast cancer outcome. Neoplasma, (1996); 61(2): 205-212.
- Lederle W, Depner S, Schnur S. IL-6 promotes malignant growth of skin SCCs by regulating a network of autocrine and paracrine cytokines. International Journal of Cancer, (2011); 128(12): 2803-2814.
- Qaysar MS, Mohammed AJM, Mohammed MM. Tracing some salivary immune elements in Iraqi SARS-2 patients. Archives of Razi Institute, (2022); 77(5): 1587-1591.
- Kross KW, Heimdal JH, Olsnes C, Olofsson J, Aarstad HJ. Tumor-associated macrophages secrete IL-6 and MCP-1 in head and neck squamous cell carcinoma tissue. Acta oto-laryngologica, (2007); 127(5): 532-539.
- Lam-ubol A, Hopkin D, Letuchy EM. Squamous carcinoma cells influence monocyte phenotype and suppress lipopolysaccharide-induced TNF-alpha in monocytes. Inflammation, (2010); 33(4): 207-223.
- Lisa Cheng YS, Jordan L, Gorugantula LM. Salivary interleukin-6 and -8 in patients with oral cancer and patients with chronic oral inflammatory diseases. Journal of Periodontology, (2014); 85(7): 956-965.
- Chiu YH, Spiegelman D, Dockery DW, Garshick E, Hammond SK, et al. Secondhand smoke exposure and inflammatory markers in nonsmokers in the trucking industry. Environmental health perspectives, (2011); 119(9): 1294-1300.
- Jassim MM, Mahmood MM, Ali SH, Kamal MS. Interplay between EBERS and P27 tumor suppressor proteins in molecular transformation of nasopharyngeal and sinonasal carcinomas. Indian Journal of Public Health, (2019); 10(6): 19-26.
- Radoi CL, Cristea OM, Vulcanescu DD, Voinescu A, Dragomir TL, et al. Seroprevalence of Herpes Simplex Virus Types 1 and 2 among Pregnant Women in South-Western Romania. Life, (2024); 14(5): 596-533.
- Sharma D, Sharma S, Akojwar N, Dondulkar A, Yenorkar N, et al. An insight into current treatment strategies, their limitations, and ongoing developments in vaccine technologies against herpes simplex infections. Vaccines, (2023); 11(2): 206-212.
- Jassim MMA, Mahmood MM, Musa SQ. Herpetic Oncogenic Virus Co-Infections Impinge Cell Cycle Regulatory Gene Expressions in Oral Cavity Malignancies. Systematic Reviews in Pharmacy, (2020); 11(3): 760–764.
- Eglin RP, Lehner T, Subak-Sharpe JH. Detection of RNA complementary to herpes-simplex virus in mononuclear cells from patients with Behcet's syndrome and recurrent oral ulcers. The Lancet, (1982); 320(8312): 1356-1361.
- Delavarian Z, Pakfetrat A, Falaki F, Pazouki M, Pazouki N. The role of viruses in oral squamous cell carcinoma in young patients in Khorasan (Northeast of Iran). Journal of Applied Science, (2010); 10(11): 981-985.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0