

Full Length Research Article
Prognostically Significant Fusion Oncogenes and Gene Mutations in Pakistani AML Patients
Muhammad Tayyab, Zahra Tariq, Muhammad Imran Qadeer, Mahwish Khan, Tuba Fayyaz, Tanveer Akhtar
Adv. life sci., vol. 10, no. 1, pp. 75-83, March 2023
*- Corresponding Author: Muhammad Tayyab (Email: mranatayyab@hotmail.com)
Authors' Affiliations
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The onset and progression of leukemia is associated with many genetic abnormalities including gene mutations and production of fusion oncogenes. Molecular studies on fusion oncogenes and mutations in different populations have been done. However, not much research on correlation of the fusion oncogenes with acute myeloid leukemia have been done in Pakistan.
Methods: Genetic analysis of 105 AML patients was done to investigate AML1-ETOand CBFB-MYH11 fusion oncogenes and mutations in NPM1 and NRAS genes. The genomic DNA and cDNA were subjected to amplification, electrophoresis, and Sanger sequencing.
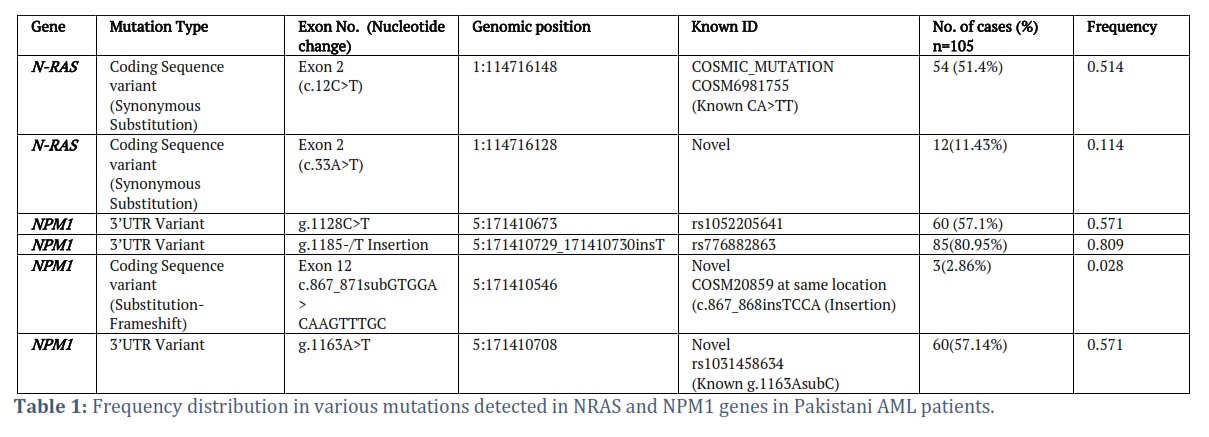
Results: The frequency of AML1-ETO was 26% in AML patients and 34.2% in AML-M2 patients. CBFB-MYH11 was present in 11.4% AML patients. A total of six mutations in 4 regions of NPM1 gene and 2 regions of NRAS gene were detected. 3’UTR of NPMI gene had three variants; g.1128C>T (57.1%), g.1185-/T insertion (80.95%), and g.1163A>T (57.14%) while c.867_871subGTGGA >CAAGTTTGC (2.86%) was present in exon 12. NRAS gene had two mutations c.12C>T (51.4%) and c.33A>T (11.43%) in exon 2. c.867_871subGTGGA >CAAGTTTGC , and g.1163A>T in NPM1 gene and c.33A>T in NRAS gene were the novel findings in this ethnic population.
Conclusion: This genetic analysis may help to modulate the treatment strategies and improve survival of patients.
Keywords: Acute Myeloid Leukemia; Fusion Oncogenes; AML; AML1-ETO; CBFB-MYH11; AML-M2; Nucleophosmin, NPM1; NRAS
Introduction![]()
Acute myeloid leukemia (AML) is a form of white blood cell cancer which is characterized by penetration of myeloid tissue, blood tissue or other tissues by multiplication, aberrant distinction, or badly altered cells [1-3]. Among leukemia patients, AML is the most prevalent in adults with an average 68 years of diagnostic age. While outcomes in the younger age group have increased remarkably, the prognosis in older patients appears to be very poor [4]. AML is responsible for 15-20% of leukemia cases. As been reported, AML in older patients is more likely to be complemented by a myelodysplastic process. It has unfavorable cytogenetic mechanisms which may also demonstrate multidrug resistance [4,5].
Being an exceedingly complex stem cells disease, AML can be associated with various cytogenetic defects and molecular mutations. Many pathogenetic processes involving replication, apoptosis, variations, and DNA repair could have been involved in these anomalies. It is not triggered by a single genetic factor, but rather the result of multiple genetic transformations [6,7]. The genetic abnormalities may disrupt functions of hematopoietic transcription factors encoding genes or give rise to fusion oncogenes that are strongly correlated and differ significantly with respect to disease severity and treatment outcomes [8-10].
During several years of studies, numerous structural and functional effects of various types of translocations have been studied such as the ones causing chronic myeloid leukemia [3]. Similar chromosomal translocations facilitate the production of proteins in AML that are chimeric fusion. Fusion genes like BCR-ABL, MLL-AF4, SIL-TAL1, TEL-AML1, E2A-PBX1CBFB-MYH11 and AML1-ETOare associated with various types of leukemias including AML [11,13,14].The fusion oncogenes BCR-ABL, MLL-AF4, ETV6-RUNX11, E2A-PBX1 and SIL-TAL1 genes have been investigated by Sabir et. al. [11] which demonstrated the role of these fusion oncogenes among Pakistani population in the onset of AML. Iqbal et al.[12] reported that Pakistani Leukemia patients substantially differ from western populations with respect to the frequencies of different classical fusion oncogenes.
Genome sequencing studies of AML patients show it to be an intricate and diverse disease characterized by the existence of numerous leukemic genes, some repeatedly and other uncommonly mutated [13]. Different subtypes of mutations have been recognized which have broadly been classified into two groups; Class I mutations include stimulated signal-transduction pathways, enhancing the expansion or existence of hematopoietic precursor cells which include the mutations in FLT3 and RAS gene family, while class II mutations affect transcription factors and allow distinction to be impeded which include mutations in CEBPA, MLL, and NPM1 [15-18].Clinical characteristics and genetic analysis of about 45% of all AML cases among a wide subgroup of AML patients having a normal karyotype has been carried out. In the case of AML, translocation t(8;21) leads to the generation of AML1-ETO fusion oncogene which has been shown to influence differentiation, proliferation and apoptosis in both in-vitro and in-vivo models having association with a favorable prognosis [19]. Moreover, inv(16)(p13q22) rearrangement resulting in CBFB-MYH11 fusion oncogene is found in approximately 10% of cases with de novo AML [20].
RAS genes regulate cellular proliferation by binding of a ligand to a variety of receptors and regulate cellular proliferation by cycling between inactive state i.e. (GDP) and active state (GTP). RAS gene activates and causes phosphorylation of activated mitogen protein kinase (MAPK) or (RAF) leading to cellular proliferation. So, if the RAS is mutated there will eventually be enhanced cellular proliferation [21, 49]. These pathogenetic mechanisms suggest that the presence of NRAS may have a prognostic significance. Patients harboring NRAS acquired two mutations in the coding sequence at only Exon 2. Activation of NRAS mutations plays a decisive role in oncogenesis in a large percentage of AMLs. NRAS mutations are the most common, occurring in 10–20% of AML patients [22].
NPM1 is a major stress-induced regulator of p53 which functions because of cytotoxic drugs, hypoxia, and UV irradiation [23, 24]. Mutations in NPM1 (exon 12) gene on chromosome 5q35 lead to frame shift and production of an elongated protein, which remains in the cytoplasm [35]. NPM1 mutations relate to higher leukocyte counts[25-27, 35]. Mostly, NPM1 mutations occur almost exclusively in de novo AML cases. Mutations in NPM1 exon 12 are found in numerous patients with AML wit mostly having normal karyotype [35].
This study is designed to carry out genetic analysis of AML patients to figure out the genetic factors contributing to its development in Pakistani population. The nature and frequencies of classical fusion oncogenes, AML1-ETO and CBFB-MYH11 in Pakistani AML patients, their comparison with other ethnic groups, presence of mutations in NPM1 and NRAS genes and the correlation of the mutation data with clinical features must be investigated. This may help in understanding the disease outcomes which may be efficient and cost effective in terms of treatment and diagnostic protocols.
Methods![]()
To conduct this study, the approval was taken from the ethical committee in Institute of Zoology, University of the Punjab, Lahore. Patient recruitment Performa was formulated, patients were recruited, and informed consents signed from the participants. Blood samples were collected from 105 AML patients from August 2013 to December 2014 from Jinnah hospital, Mayo hospital and Institute of Nuclear medicine and oncology (INMOL) Lahore. The experimental work was completed in parasitology lab and central lab, Institute of Zoology, University of the Punjab, Quaid-e-Azam campus Lahore, Pakistan.
Blood was drawn from each AML patient and transferred to properly labelled EDTA coated vacutainer tubes. Screening tests were done to exclude patients having other infectious diseases. Genomic DNA and mRNA were extracted within 24 hours of blood collection and stored at -40°C. All equipment was sterilized properly, the reagents were made using double distilled water and autoclaved. Light sensitive reagents were covered with aluminum foil and kept properly.
Nucleic Acids Extractions
Genomic DNA was isolated from whole white blood cells by using both the manual DNA isolation protocol using TRIzol reagent as well as kit-based isolation protocol (Promega Wizard Genomic DNA purification kit (Cat#A1120) according to the manufacturer’s instructions depending upon the volume of the blood obtained from each AML patient. Both methods were properly optimized. Manual method of DNA extraction DNAzol [29] was used for blood more than 3mL to obtain high quality yield while kit-based method was used for DNA extraction from blood less than 3mL to obtain maximum yield.
For RNA isolation from the whole blood, PBMC pellet was isolated first. The RNA extraction procedure was adopted from previous published studies [30,31]. For this purpose, blood with anticoagulant was aliquoted in Eppendorf tubes and cell lyses solution (Gentra USA) was added. The tubes were vortexed and left at room temperature followed by centrifugation. The process was repeated for the complete lysis of RBCs and appearance of a pellet. The PBMC pellet was dissolved in the lysis solution which was followed by the RNA extraction procedure using TRIzol reagent.
Primer Designing
Sequences of selected human genes were retrieved from NCBI which were then BLAT (www.genome.ucsc.edu) and whole gene intronic and exonic sequences were obtained. Exon primer pairs were designed after preliminary analysis of specific human genes through bioinformatics tool (www.expasy.ch) for oncogenes and (https://primer3.org/) for selected NPM1 and NRAS (table 1,2). The primers were 20-22 nucleotides long with up to 50% GC content and minimal complementarities to avoid dimer formations.
Reverse Transcriptase Polymerase Chain Reaction (RT-PCR)
cDNA was prepared using Fermentas kit (k1622) using the manufacturer’s instructions. The RT-reaction protocol and thermal conditions were optimized. The cDNA was amplified by the nested PCR with optimized conditions.
Agarose Gel Electrophoresis
Genomic DNA and PCR products were visualized by agarose gel electrophoresis. 1.0% agarose was used to visualize genomic DNA and 2% for PCR products. The gel was observed under UV light to analyze the DNA.DNA was observed as fluorescent band and photograph was obtained by Fisher Scientific UVP PhotoDoc-ItTM Imaging System.
DNA/RNA Quantitative and Qualitative Assessment
Quality of DNA/RNA was assessed by native agarose gel electrophoresis. The gel was observed under UV light. DNA was observed as fluorescent band and photograph was obtained by UVP PhotoDoc-ItTM Imaging System. For the quantification of extracted genomic DNA Nano Drop™ 1000 Spectrophotometer (Thermo Scientific, Wilmington, DE) was used. The quantity was estimated, and DNA was diluted accordingly.
Sequencing Analysis of PCR Amplicons
The facility for direct sequencing was provided by Centre of applied molecular biology (CAMB), University of the Punjab, Lahore. The Nested RT-PCR products of fusion oncogenes and amplified PCR products of genomic DNA were subjected to direct sequencing analysis for detection of any possible mutations present in NRAS and NMP1genes of AML patients. Standard procedure for BigDye® Terminator v3.1Cycle Sequencing Kit from Applied Biosystems, USA was used as per manufacturer’s instructions.
Analysis of Sequence Data
The sequenced templates were analysed using sequencing analysis software Geneious R7 [55]. The DNA sequences of NMP1 and NRAS genes of healthy individuals were aligned against the reference sequence (NCBI GenBank accession number M14772.1). Polymorphic variations in our population were analysed to avoid artefact findings with point mutations within AML patient’s sequences. Moreover, the gene sequences representing heterozygous mutations and those with noise in data were repeated for the whole procedure, to ensure the results are accurate and reproducible.
Statistical Analysis
The IBM SPSS statistics, version 22 and Graph pad Prism were used for statistical analysis. The demographic characteristics of patients were analyzed statistically. For all analyses, a p-value of less than 0.05 was considered statistically significant. The continuous and categorical data was analyzed by independent sample t-test and correlation tests.
Results![]()
The Clinical data of 105 AML patients under investigation was arranged according to clinical characteristics and response outcomes. Incidence of AML was more in males (54.2%) than females (45.2%). Majority of patients in the present study were adults. Median age of Pakistani AML patients was 33.5 years with a range (13-72 years). High grade fever was the most frequent clinical characteristic. Weight loss, organomegaly, fatigue, and muscle pains were other important diagnostic features. Complete blood count revealed that 78.09% AML patients had normal total leukocyte count, but others had elevated TLC count. 97.14% individuals had normal platelet count. Mean corpuscular hemoglobin (MCH) within the normal range (26-32 PG) was observed in 96.19% in AML patients. Decreased level of haemoglobin in blood was presented by 90.47% individuals. 54.7% individuals were in chronic phase, 28.7% in accelerated phase and16.6% in blast phase of disease. Mutational analysis indicated the presence of fusion oncogenes and mutated NRAS, and NPM1 genes were found in various samples. Colocalization of several mutations was found in some samples.
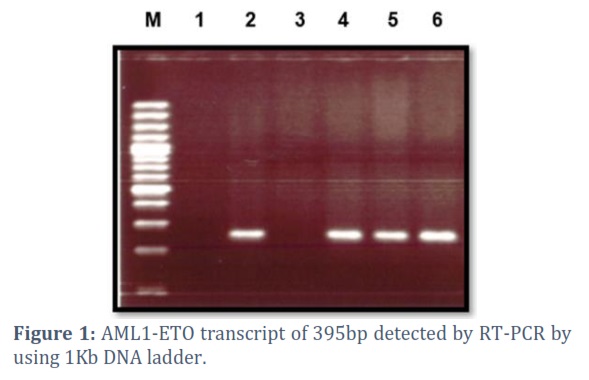
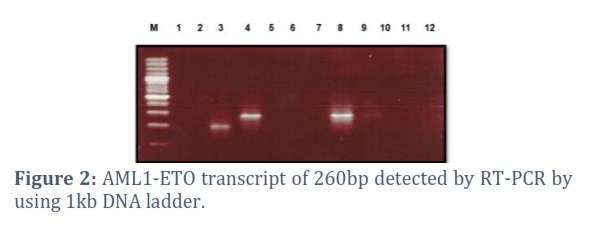
Patient characteristics and detection of AML1-ETO transcripts
AML1-ETO transcripts were detected as 395 bp in the first and 260bp in the second PCR product, which was found in 26.6% individuals. AML1-ETO transcripts in M2 were detected in 34.2%. GAPDH was used as an internal control (Fig 1& 2). A comparison of clinical parameters such as age, gender, hepatomegaly, splenomegaly, and extramedullary tumefaction between AML1-ETO positive groups in AML patients was made but no significant difference was found.
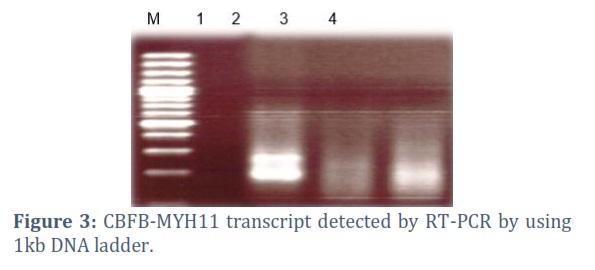
Patient characteristics and detection of CBFB-MYH11 transcripts
CBFB-MYH11 transcripts were detected as 180 bp in the first and 280bp in the second PCR product, which was found in 11.4%. GAPDH was used as internal control. 4.7% AML- M2 patients were present with gender ratio being 3:2 (M:F) and the median age 18 years. CBFB-MYH11 transcripts in M2 were not detected (figure 3).
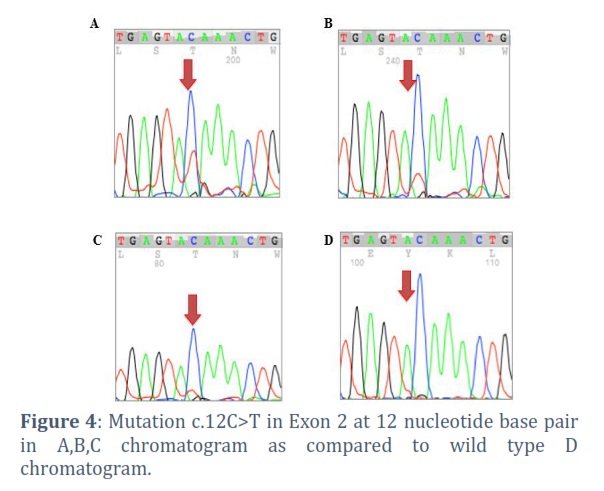
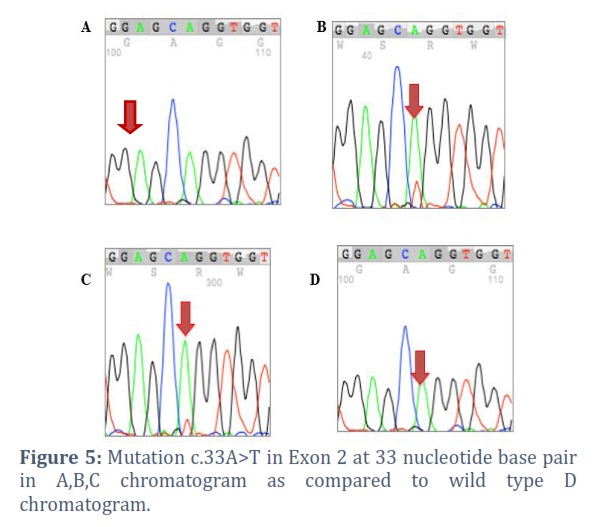
Neuroblastoma RAS (N-RAS)
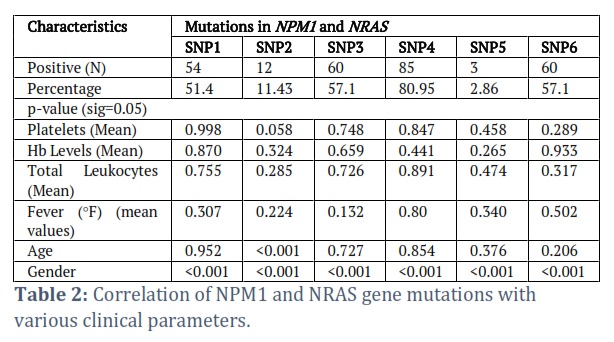
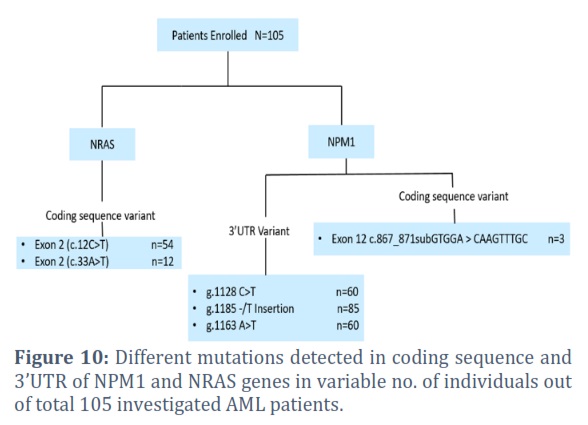
Two alternations were observed in the NRAS gene, a substitution of nucleotide C with T (c.12C>T) in Exon 2 at nucleotide 12 in 54 (51.4%) AML patients which was a known mutation while the other was the replacement of A with T (c.33A>T) in Exon 2 at nucleotide 33 in 12 (11.43%) AML patients (fig 2). The NRAS mutations had a higher prevalence of adults (n=53) predominantly males (83.33%) as compared to few affected females (14.81%). Significant correlation of SNP1 was found with male and female ratio with 0.001 p-value. Other factors including platelet count, Hb levels, TLC count, fever, and age were not significantly correlated. SNP2 had no significant correlation with biochemical parameters. However, it was significantly correlated (p=0.001<0.05) with gender and age.
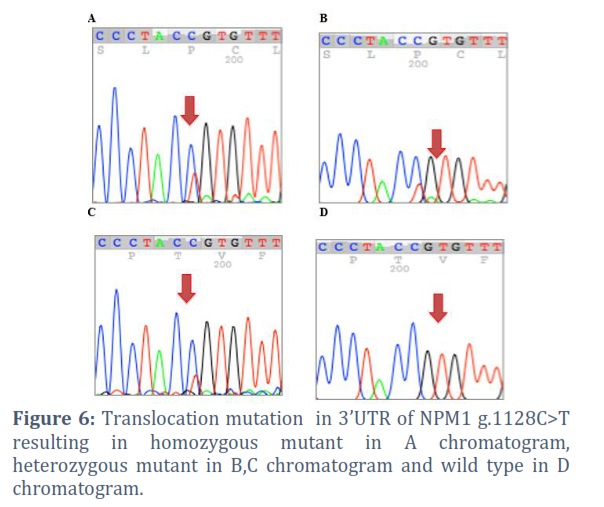
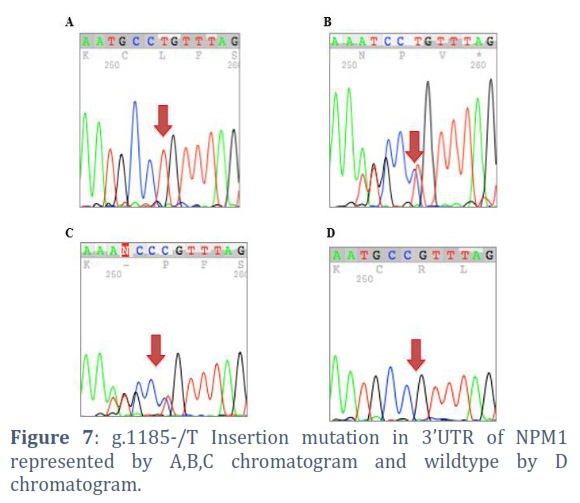
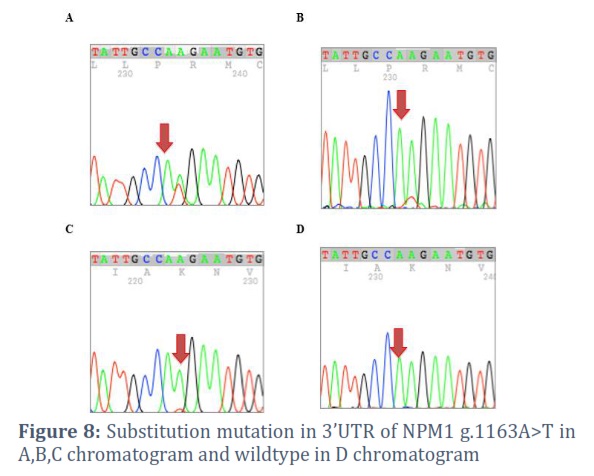
Nucleophosmin1 (NPM1) 3’UTR Variant mutation
Three types of mutations in 3’UTRs of NPM1 gene were observed in the patients. Replacement of nucleotide C with T (g.1128C>T) at genomic position 5:171410673 was found in 60 (57.1%) AML patients. The p-values for platelet count, Hb levels, total leukocytes, fever, and age were non-significant for SNP3 whereas gender ratio had significant correlation with the positive AML patients with more males being affected as compared to females.
Insertion of ‘T’ (g.1185-/T Insertion) at genomic position 5:171410729_171410730insT was the most frequently occurring mutation that was present in 85 (80.95%) AML patients. Platelet count, Hb levels, total leukocytes, fever, and age indicated no correlation between SNP4 found in AML patients whereas gender indicated significant correlation with a higher prevalence of affected males than females (fig 3). Replacement of A with T (g.1163A>T) in nucleotide 1163 at genomic position 5:171410708 was found in 60 (57.1%) AML patients. No significant correlation of SNP6 was found with platelet count, Hb levels, total leukocytes, fever, and age however, significant correlation was found with gender (p-value 0.001<0.05) with equally affected individuals of different age groups but a higher ratio of affected males than females.
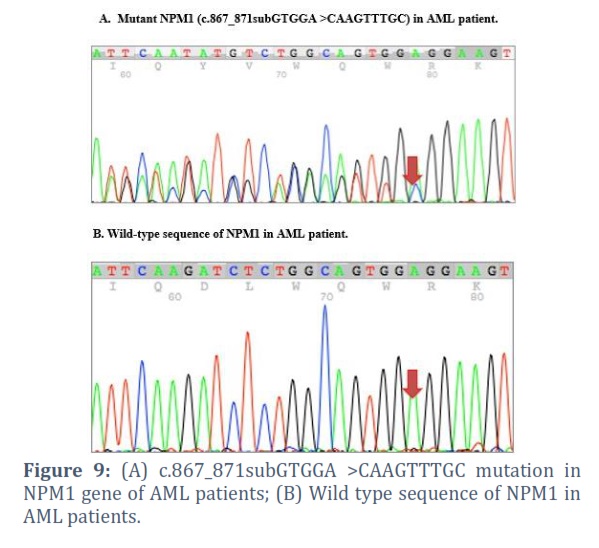
Nucleophosmin1 (NPM1) Gene coding sequence mutation
Replacement of the sequence GTGGA with CAAGTTGC c.867_871subGTGGA >CAAGTTTGC in exon 12 of NPM1 gene in 3 (2.86%) AML patients was a novel finding in this population. SNP5 showed significant correlation with gender ratio with greater no. of males affected (p-value=0.001<0.05) while other parameters were not correlated.
Figures & Tables
Genetic, molecular, and biochemical studies on the onset and progression of leukemia have indicated genetic abnormalities involving oncogene mutation and fusion oncogene production to be the major cause of leukemia. The prevalence of different fusion oncogenes and chromosomal abnormalities associated with leukemia vary in different ethnic groups [32,33]. These studies are aiding in devising strategies for differential diagnosis, prognosis, treatment, and management of leukemia. Pakistani leukemia patients differ from other populations with respect to the frequencies of different classical fusion oncogenes. However, data has not been provided on chromosomal changes and the clinical correlation of the fusion oncogenes [12].
AML is a malignant bone marrow disease wherein hematopoietic precursors are arrested in an early stage of progression. It differs from other related blood disorders by the occurrence of more than 20% blasts in the bone marrow [12,15]. Acute leukemias are characterized by recurring chromosomal aberrations and gene mutations. The pathogenesis of disease at molecular level is not fully assorted and treatment grading is complex, especially for patients who have seemingly normal karyotype. Gene mutations have played an important role as biological and diagnostic markers in the treatment of AML. It is anticipated that molecular classification of AML not only allows accurate analytical predictions in numerous patients but also opens future helpful treatment options for the patients [15].
Acute leukemia associated fusion protein AML1-ETO is a product of the chromosome translocation (8; 21) frequently occurring in AML [34]. This fusion oncoprotein blocks leukemia cell differentiation and induces growth arrest with increased sensitivity to apoptosis induction. The inv(16)(p13q22) rearrangement results in a CBFB-MYH11 fusion gene [14]. In our study, the frequency of AML1-ETO fusion oncogene was 26.6% while frequency of CBFB-MYH11 was 11.4% among the investigated AML patients. The frequency of AML1-ETO fusion oncogene in sub-type AML-M2 was 34.2%. The frequency of AML1-ETO and CBFB-MYH11 fusion oncogenes were significantly high in age between 30-59 yrs.
Mutations in NPM1 gene on chromosome 5q35 lead to frame shift and production of an elongated protein, which occurs in about one third of AML patients [35,36]. It is one of the 3 most common mutations in AML and relates to higher leukocyte counts especially in the presence of FLT3-ITD fusion oncogene [35]. NPM1 mutations may occur in de novo AML cases or can be co-expressed with RUNX1-RUNX1T1 transcripts [37,38]. Similar results of NPM1 gene mutations on exon 12 were found in this study. The most frequently detected mutation in Pakistani AML patients was NPM1 3’UTR Variant (g.1185-/T Insertion), found in 80.95% of the investigated patients while the other 3’UTR variants were g.1128C>T and g.1163A>T with a prevalence rate of 57.1% each. g.1163A>T was a novel mutation in this ethnic region. c.867_871subGTGGA >CAAGTTTGC was another novel mutation in the exon 12 of Pakistani AML patients with a prevalence rate of 2.86%. The probable cause of the onset of AML due to mutations in the 3’UTR be the modification of gene expression or uncontrolled production of abnormal proteins.
A study conducted by Bhattacharyya et al., [39] in India demonstrated 27.9% prevalence of NPM1 in AML patients, while it was 27.5% in Germany [35], 15.4% in China [40], 26.3% in Thailand [41], 7% in South Africa [42], 21% in Egypt [43], and between 19.1%-20.3% in the AML patients in Bulgaria [38]. These statistics show varying prevalence of NPM1 gene with varying geographic areas with prevalence rates higher than 20% in Asia.
This study also showed a disturbance in leukocyte count in AML patients with NPM1 mutation. Hb levels and platelet count were dysregulated with NPM1 mutation in a study by Yi et al., [44] in the AML patients but no dysregulation was found in this study. According to a study, NPM1 mutation were higher in male patients than females [45] which was contradicted by Kern et al., [46] stating higher NPM1 mutations in females than males (7:13). This study also indicated higher prevalence of NPM1 in males than females.
NRAS gene mutation in the pathophysiology of AML patients was also investigated in this study. RAS gene activates and causes phosphorylation of activated mitogen protein kinase (MAPK) leading to cellular proliferation which gets disturbed in the presence of mutations [47]. NRAS mutations are the most common, occurring in 10–20% of AML patients [48]. In Indian population the mutations in NRAS gene in AML patients are about 5%, whereas it is 10% in French population, 11% in the UK and higher in the rest of Europe [49].
This study demonstrated the prevalence rates to be 12% (c.33A>T) and 54.1% (c.12C>T) in two coding regions of exon 2 of NRAS gene which is significantly greater than the prevalence rates around the world. Our study showed a significant correlation of NRAS mutation with reduced leukocyte counts as demonstrated by Bacher et al., [50]. It also showed significant correlation of age and gender with NRAS mutations. Dunna et al., [49]and also concluded higher prevalence of NRAS mutations in males than females.
AML may develop due to activating NRAS mutations simultaneously with NPM1 mutations, occurring commonly in the favorable-risk population [51]. Akram et al., [52] showed disturbance in platelet count, Hb levels and leukocyte count of the AML patient with NRAS mutation. Our study also signified these results with the relation of NRAS mutation with platelet count, leukocyte count and Hb levels.
Although the extrapolative scale of NRAS mutations in AML patients are not decisive [53], yet several large cohort studies indicated that NRAS mutations in AML did not influence the prognosis of patients[54]. That is why, given the prevalence of NRAS mutations in AML patients, more research on clinical characteristics and possible prognostic factors should be done.
In Pakistan, no significant work has been performed to find out frequencies of fusion oncogenes in AML patients, possible mutations in NPM1 and NRAS genes, and their correlation with patient characteristics and clinical response. This study has proven to be beneficial to determine the role of fusion oncogenes in Pakistani AML patients. It has given new insights into the mutational range and prognostic elements of NRAS and NPM1 genes in AML patients. More detailed mutational analysis and large prospective studies are needed in the future for better prognostication of NRAS and NPMI in monitoring the development and proliferation of AML. It must be explored by parallel comparison with non NRAS and NPM1 mutation associated AML. Our conclusion needs validation in a larger and prospective cohort.
Author Contributions
Muhammad Tayyab: Conception and design, Experimental Work, Analysis and interpretation of data, Rough Draft
Tanveer Akhtar: Supervision, Research Project Administration
Zahra Tariq: Analysis and Interpretation,
Mahwish Khan: Final Draft,writing and Revision
Muhammad Imran Qadeer: Final Draft and Revision
Tuba Fayyaz: Draft editing![]()
The authors declare that there is no conflict of interest.
![]()
References
- Döhner H, Estey EH, Amadori S, Appelbaum FR, Büchner T, et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood, The Journal of the American Society of Hematology, (2010); 115(3): 453-474.
- Gorombei P, Guidez F, Ganesan S, Chiquet M, Pellagatti A, et al. BCL-2 Inhibitor ABT-737 Effectively Targets Leukemia-Initiating Cells with Differential Regulation of Relevant Genes Leading to Extended Survival in a NRAS/BCL-2 Mouse Model of High Risk-Myelodysplastic Syndrome. International journal of molecular sciences, (2021); 22(19): 10658.
- Iqbal Z, Aleem A, Iqbal M, Naqvi MI, Gill A, et al. Sensitive detection of pre-existing BCR-ABL kinase domain mutations in CD34+ cells of newly diagnosed chronic-phase chronic myeloid leukemia patients is associated with imatinib resistance: implications in the post-imatinib era. PLoS One, (2013); 8(2): e55717.
- Bhatia S, Sather HN, Heerema NA, Trigg ME, Gaynon PS, et al. Racial and ethnic differences in survival of children with acute lymphoblastic leukemia. Blood, The Journal of the American Society of Hematology, (2002); 100(6): 1957-1964.
- Leith CP, Kopecky KJ, Chen I-M, Eijdems L, Slovak ML, et al. Frequency and clinical significance of the expression of the multidrug resistance proteins MDR1/P-glycoprotein, MRP1, and LRP in acute myeloid leukemia. A Southwest Oncology Group Study. Blood, The Journal of the American Society of Hematology, (1999); 94(3): 1086-1099.
- Kelly LM, Yu J-C, Boulton CL, Apatira M, Li J, et al. CT53518, a novel selective FLT3 antagonist for the treatment of acute myelogenous leukemia (AML). Cancer cell, (2002); 1(5): 421-432.
- Wilbanks AM, Mahajan S, Frank DA, Druker BJ, Gilliland DG, et al. TEL/PDGFβR fusion protein activates STAT1 and STAT5: A common mechanism for transformation by tyrosine kinase fusion proteins. Experimental hematology, (2000); 28(5): 584-593.
- Yu J, Jiang PY, Sun H, Zhang X, Jiang Z, et al. Advances in targeted therapy for acute myeloid leukemia. Biomarker research, (2020); 8(1): 1-11.
- Dutta R, Zhang TY, Köhnke T, Thomas D, Linde M, et al. Enasidenib drives human erythroid differentiation independently of isocitrate dehydrogenase 2. The Journal of clinical investigation, (2020); 130(4): 1843-1849.
- Mueller BU, Pabst T, Fos J, Petkovic V, Fey MF, et al. ATRA resolves the differentiation block in t (15; 17) acute myeloid leukemia by restoring PU. 1 expression. Blood, (2006); 107(8): 3330-3338.
- Sabir N, Iqbal Z, Aleem A, Awan T, Naeem T, et al. Prognostically significant fusion oncogenes in Pakistani patients with adult acute lymphoblastic leukemia and their association with disease biology and outcome. Asian Pacific Journal of Cancer Prevention, (2012); 13(7).
- Iqbal J, Kucuk C, Deleeuw R, Srivastava G, Tam W, et al. Genomic analyses reveal global functional alterations that promote tumor growth and novel tumor suppressor genes in natural killer-cell malignancies. Leukemia, (2009); 23(6): 1139-1151.
- Döhner H, Weisdorf DJ, Bloomfield CD. Acute myeloid leukemia. New England Journal of Medicine, (2015); 373(12): 1136-1152.
- Ernst P, Wang J, Korsmeyer SJ. The role of MLL in hematopoiesis and leukemia. Current opinion in hematology, (2002); 9(4): 282-287.
- Stirewalt DL, Radich JP. The role of FLT3 in haematopoietic malignancies. Nature Reviews Cancer, (2003); 3(9): 650-665.
- Grisendi S, Mecucci C, Falini B, Pandolfi PP. Nucleophosmin and cancer. Nature Reviews Cancer, (2006); 6(7): 493-505.
- Schubbert S, Shannon K, Bollag G. Hyperactive Ras in developmental disorders and cancer. Nature Reviews Cancer, (2007); 7(4): 295-308.
- Haferlach T. Molecular genetic pathways as therapeutic targets in acute myeloid leukemia. ASH Education Program Book, (2008); 2008(1): 400-411.
- Schnittger S, Kohl TM, Haferlach T, Kern W, Hiddemann W, et al. KIT-D816 mutations in AML1-ETO-positive AML are associated with impaired event-free and overall survival. Blood, (2006); 107(5): 1791-1799.
- Kurata K, Yamamoto K, Okazaki Y, Noguchi Y, Matsui K, et al. Detection of a novel CBFB-MYH11 fusion transcript in acute myeloid leukemia M1 with inv (16)(p13q22). Cancer Genetics, (2020); 24172-76.
- Yohe, S. (2015). Molecular genetic markers in acute myeloid leukemia. Journal of clinical medicine, 4(3), 460-478. https://doi.org/10.3390/jcm4030460
- Blau, O. (2015). Gene mutations in acute myeloid leukemia-incidence, prognostic influence, and association with other molecular markers. Leukemias-Updates and New Insights. Croatia: Intech Open, 75-100. http://dx.doi.org/10.5772/6092823.
- Wu, M. H., & Yung, B. Y. (2002). UV stimulation of nucleophosmin/B23 expression is an immediate-early gene response induced by damaged DNA. Journal of Biological Chemistry, 277(50), 48234-48240. https://doi.org/10.1074/jbc.M206550200
- Karimi Dermani, F., Gholamzadeh Khoei, S., Afshar, S., & Amini, R. (2021). The potential role of nucleophosmin (NPM1) in the development of cancer. Journal of cellular physiology, 236(11), 7832-7852.
- Khanolkar, R. A., Faridi, R. M., Kinzel, M., Jamani, K., Savoie, M. L., Shafey, M., . . . Storek, J. (2022). Impact of FLT3 internal tandem duplication and NPM1 mutations in acute myeloid leukemia treated with allogeneic hematopoietic cell transplantation. Cytotherapy, 24(4), 413-420.
- Sakaguchi, M., Yamaguchi, H., Najima, Y., Usuki, K., Ueki, T., Oh, I., . . . Kobayashi, Y. (2018). Prognostic impact of low allelic ratio FLT3-ITD and NPM1 mutation in acute myeloid leukemia. Blood advances, 2(20), 2744-2754.
- Falini B, Nicoletti I, Bolli N, Martelli MP, Liso A, et al. Translocations and mutations involving the nucleophosmin (NPM1) gene in lymphomas and leukemias. (2007).
- Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, et al. WHO classification of tumours of haematopoietic and lymphoid tissues. Chapter: Book Name. 2008 of publication; 2; International agency for research on cancer Lyon.
- Chomczynski P, Mackey K, Drews R, Wilfinger W. DNAzol®: a reagent for the rapid isolation of genomic DNA. Biotechniques, (1997); 22(3): 550-553.
- Chomczynski P, Sacchi N. Single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction. Analytical biochemistry, (1987); 162(1): 156-159.
- Liedtke W, Battistini L, Brosnan C, Raine C. A comparison of methods for RNA extraction from lymphocytes for RT-PCR. Genome Research, (1994); 4(3): 185-187.
- Ariffin H, Chen S-P, Kwok CS, Quah T-C, Lin H-P, et al. Ethnic differences in the frequency of subtypes of childhood acute lymphoblastic leukemia: results of the Malaysia-Singapore Leukemia Study Group. Journal of pediatric hematology/oncology, (2007); 29(1): 27-31.
- Jiménez-Morales S, Hidalgo-Miranda A, Ramírez-Bello J. Acute lymphoblastic leukemia: a genomic perspective. Boletín Médico Del Hospital Infantil de México (English Edition), (2017); 74(1): 13-26.
- Osman D, Gobert V, Ponthan F, Heidenreich O, Haenlin M, et al. A Drosophila model identifies calpains as modulators of the human leukemogenic fusion protein AML1-ETO. Proceedings of the National Academy of Sciences, (2009); 106(29): 12043-12048.
- Thiede C, Koch S, Creutzig E, Steudel C, Illmer T, et al. Prevalence and prognostic impact of NPM1 mutations in 1485 adult patients with acute myeloid leukemia (AML). Blood, (2006); 107(10): 4011-4020.
- DiNardo CD, Cortes JE. Mutations in AML: prognostic and therapeutic implications. Hematology 2014, the American Society of Hematology Education Program Book, (2016); 2016(1): 348-355.
- Renneville A, Roumier C, Biggio V, Nibourel O, Boissel N, et al. Cooperating gene mutations in acute myeloid leukemia: a review of the literature. leukemia, (2008); 22(5): 915-931.
- Balatzenko G, Spassov B, Stoyanov N, Ganeva P, Dikov T, et al. NPM1 gene type A mutation in Bulgarian adults with acute myeloid leukemia: a single-institution study. Turkish Journal of Hematology, (2014); 31(1): 40.
- Bhattacharyya J, Nath S, Saikia KK, Saxena R, Sazawal S, et al. Prevalence and clinical significance of FLT3 and NPM1 mutations in acute myeloid leukaemia patients of Assam, India. Indian Journal of Hematology and Blood Transfusion, (2018); 34(1): 32-42.
- Su L, Gao SJ, Li W, Tan YH, Cui JW, et al. NPM1, FLT3-ITD, CEBPA, and c-kit mutations in 312 Chinese patients with de novo acute myeloid leukemia. Hematology, (2014); 19(6): 324-328.
- Boonthimat C, Thongnoppakhun W, Auewarakul CU. Nucleophosmin mutation in Southeast Asian acute myeloid leukemia: eight novel variants, FLT3 coexistence and prognostic impact of NPM1/FLT3 mutations. haematologica, (2008); 93(10): 1565-1569.
- Marshall R, Tlagadi A, Bronze M, Kana V, Naidoo S, et al. Lower frequency of NPM 1 and FLT 3‐ITD mutations in a South African adult de novo AML cohort. International journal of laboratory hematology, (2014); 36(6): 656-664.
- Zidan M, Shaaban H, El Ghannam D. Prognostic impact of nucleophosmin 1 (NPM1) gene mutations in Egyptian acute myeloid leukemia patients. Turkish Journal of Hematology, (2013); 30(2): 129.
- Yi H, Zeng D, Shen Z, Liao J, Wang X, et al. Integrin alphavbeta3 enhances β-catenin signaling in acute myeloid leukemia harboring Fms-like tyrosine kinase-3 internal tandem duplication mutations: implications for microenvironment influence on sorafenib sensitivity. Oncotarget, (2016); 7(26): 40387.
- Chauhan PS, Ihsan R, Singh LC, Gupta DK, Mittal V, et al. Mutation of NPM1 and FLT3 genes in acute myeloid leukemia and their association with clinical and immunophenotypic features. Dis Markers, (2013); 35(5): 581-588.
- Kern W, Haferlach C, Bacher U, Haferlach T, Schnittger S. Flow cytometric identification of acute myeloid leukemia with limited differentiation and NPM1 type A mutation: a new biologically defined entity. Leukemia, (2009); 23(7): 1361-1364.
- Jarell AD, Lawrence D, Tsao H. The RAS/mitogen activated protein (MAP) kinase pathway in melanoma biology and therapeutics. Biologics, (2007); 1(4): 407-414.
- Olga B (2015) Gene Mutations in Acute Myeloid Leukemia — Incidence, Prognostic Influence, and Association with Other Molecular Markers. In: Margarita G, Gueorgui B, editors. Leukemias. Rijeka: IntechOpen. pp. Ch. 4.
- Dunna NR, Vuree S, Anuradha C, Sailaja K, Surekha D, et al. NRAS mutations in de novo acute leukemia: prevalence and clinical significance. Indian J Biochem Biophys, (2014); 51(3): 207-210.
- Bacher U, Haferlach T, Schoch C, Kern W, Schnittger S. Implications of NRAS mutations in AML: a study of 2502 patients. Blood, (2006); 107(10): 3847-3853.
- Irahara N, Baba Y, Nosho K, Shima K, Yan L, et al. NRAS mutations are rare in colorectal cancer. Diagn Mol Pathol, (2010); 19(3): 157-163.
- Akram AM, Chaudhary A, Kausar H, Althobaiti F, Abbas AS, et al. Analysis of RAS gene mutations in cytogenetically normal de novo acute myeloid leukemia patients reveals some novel alterations. Saudi J Biol Sci, (2021); 28(7): 3735-3740.
- De Melo MB, Lorand-Metze I, Lima CS, Saad ST, Costa FF. N-ras gene point mutations in Brazilian acute myelogenous leukemia patients correlate with a poor prognosis. Leuk Lymphoma, (1997); 24(3-4): 309-317.
- Yang X, Qian J, Sun A, Lin J, Xiao G, et al. RAS mutation analysis in a large cohort of Chinese patients with acute myeloid leukemia. Clin Biochem, (2013); 46(7-8): 579-583.
- Olsen C, Qaadri K, Moir R, Kearse M, Buxton S, Cheung M. Geneious R7: a bioinformatics platform for biologists. InInternational plant and animal genome conference Xxii 2014.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0

