

Full Length Research Article
T-cell Imbalance or Decreased Th:Tc Ratio in Immune Thrombocytopenia: Is it Clinically Significant?
Aisha Arshad1,2, Samina Naz Mukry1*, Munira Borhany2, Tahir Shamsi2
Adv. life sci., vol. 10, no. 1, pp. 109-114, March 2023
*- Corresponding Author: Samina Naz Mukry (Email: smukry@gmail.com)
Authors' Affiliations
2. Department of Clinical Hematology, National Institute of Blood Diseases and Bone Marrow Transplantation, Karachi – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Immune thrombocytopenic purpura (ITP) is an autoimmune disorder characterized by low platelet count and various contributing factor. The imbalance in T cells may also cause ITP. Therefore, the present study was planned to assess the role of T-cells in pathogenesis of ITP and also to evaluate any possible link of Th:Tc imbalance to disease severity.
Methods: The present study was conducted with 111 patients of ITP and similar number of controls as case control study with 1:1 ratio of from January 2017 to July 2019. The patients were grouped according to the guideline of ASH as newly diagnosed/persistent ITP(ND-ITP/P-ITP) and chronic/refractory ITP(C-ITP/R-ITP).The blood samples were obtained, and CBC parameters were observed using advanced hematology analyzer XN-1000.The T cells subset analysis was evaluated by BD FACS Calibur flow cytometer. The Fisher exact test was done to evaluated the difference among the groups with (p=<0.05) by using SPSS version 19.
Results: Significantly reduced levels of hemoglobin, platelet counts with elevated IPF were observed in ND-ITP/P-ITP and C-ITP/R-ITP patients (p=<0.001).The significantly low Th:Tc ratio (p=<0.001) predicts imbalance of T cells in ND-ITP/P-ITP (0.86±0.47) as compared to control group (1.73±0.46).The mean of 0.84±0.34 Th:Tc ratio was observed in C-ITP/R-ITP children with ≤16 years. An insignificant difference (p= 0.89) was linked between children with non-severe chronic (0.84±0.42), severe chronic (0.82±0.49) and refractory ITP (0.85±0.51).
Conclusion: In ITP patients’ low levels of Th:Tc ratio was observed suggesting dysregulation of immune system. The chronicity of the disease may be linked to elevated production of Tc in children (≤16 years) with C-ITP/R-ITP.
Keywords: Immune thrombocytopenia; Platelets counts; Helper T-cells (Th); Cytotoxic T-cells (Tc)
Introduction![]()
Immune thrombocytopenia (ITP) is an autoimmune disease which is characterized by the breach in immune tolerance [1]. The exact etiology of the disorder is still unknown. The disease etiology may involve auto-reactive antibodies to platelet antigens, hyper-reactive B cells and abnormal function of cytotoxic T-lymphocytes(Tc) and T-helper cells (Th). Inadequate production of platelets or maturation defects during thrombopoiesis may lead to decreased platelets counts in ITP. The ITP is primary or secondary to an underlying disorder. It may additionally be divided according to duration as newly diagnosed (less than 3 months), persistent (longer than 3 up to 12 months) or chronic ITP (longer than 12 months). Male and female are equally affected [2]. ITP has complex and heterogeneous pathophysiology. The common symptoms include bruises, epistaxis, petechiae and menorrhagia etc. [3]. The antibodies production against platelet glycoproteins have a significant role in ITP [4-5]. One of the important features of immune system is the immunological tolerance that leads the cells to distinguish self from the non-self which helps in defense in response to pathogens [6]. The overall control of immune system is through the mechanisms of central and peripheral tolerance involving various cells and their products. The Th and the cytokine have an important role in ITP by regulating the production of autoantibodies and activating other cells [7-10]. In the pathogenesis of ITP, one of the factors is the lysis of platelets which were mediated by the Tc cells. The loss in peripheral tolerance in ITP occurred due to cytokine imbalance and autoreactive B and T cells[10].
Despite extensive research the controversy is still there about the clinical association of T-cell count in ITP patients. Therefore, the current study was done to assess any possible association of absolute counts of Th, Tc cells and their ratio in newly diagnosed/persistent ITP and chronic/refractory ITP patients and whether these findings could be included in predicting chronicity in ITP .
Methods![]()
The present case control (1:1) study was approved by the Research ethics committee of the NIBD in accordance with the declaration of Helsinki (NIBD/RD-/152-33-2013). A total of 111 patients with ITP including (64 females and 47 males) as test group and 111 healthy individuals of either sex was included in control group during the period of January 2015 to July 2017. Inclusion of all healthy participants was voluntary while patients in this study were selected in accordance with the American Society of Hematology (ASH) criteria for ITP[11]. The patients were categorized into two groups: i) ND-ITP/P-ITP patients with platelets count <100 x 109/L presented with sudden onset of bleeding and/or bruising and; ii) C-ITP/R-ITP patients with platelets count <100 x 109/L for more than 12 months post standard immunosuppressive/ steroid treatment. Severe ITP was defined as presentation with significant bleeding requiring increase in drug dose, and refractory ITP; was persistence of severe ITP even after splenectomy. In order to study any association of Th:Tc ratio with disease severity and age the C-ITP/R-ITP group was further divided into six groups: a) Chronic non-severe ITP patients ≤16 years ; b) Chronic severe ITP patients ≤ 16 years ; c) Refractory ITP patients ≤16 years d) Chronic non-severe ITP patients >16 years ; e) Chronic severe ITP patients >16 years and f) Refractory ITP >16 years respectively. Moreover, all participants in the control group were healthy.
The information regarding demographic, laboratory findings and outcomes such as ITP diagnosis, age at diagnosis, gender, bleeding type, treatments and blood counts etc. were collected from the patients. Peripheral blood sample (10mL each), was collected from all the subjects and distributed in different anticoagulants tubes including EDTA, citrate and without anticoagulant. Blood kept in EDTA anticoagulant tube was then analyzed for complete blood picture (CBC) with cell lineage specific extended parameters using Sysmex XN-1000(Sysmex Corporation, Kobe, Japan).Other blood samples were centrifuged immediately, and their sera/plasma was separated and stored at −80°C until use. Viral profile i.e. Anti-HCV, HBsAg, Anti-HIV I/II screening was performed using chemiluminescence technique (Abbot Architect). Active viral infection was further confirmed by PCR. The ratio of Th: Tc was analyzed by BD Tri-test CD4 FITC/ CD8 PE/ CD3 PerCP (Cat #: 340298) antibody cocktail using BD FACS Calibur flow cytometer (BD Biosciences, New Jersey, USA). The acquired data was analyzed by Multiset version 3.0.2. The normal Th:Tc ratio ranged from 0.9- 6.
Statistical Analysis:
The data obtained was analyzed by using SPSS version 19 (SPSS Inc., Chicago, IL, USA). The mean with standard deviation was done for quantitative variables. A p value of < 0.05 was indicate as significant statistical difference. The calculation and comparison of mean in patients and control group was evaluated by Fisher exact test. Pearson’s regression was applied to find the strength of correlation between Th:Tc ratio in different groups.
Results![]()
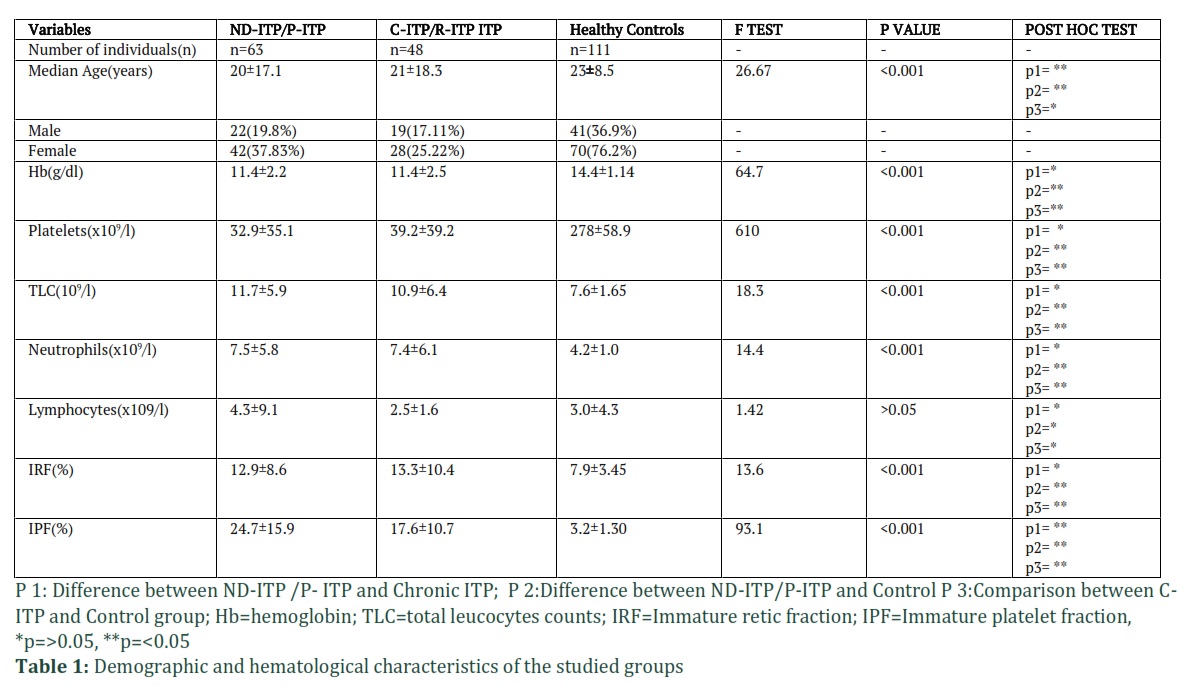
The patients of ITP were categorized into two groups i.e., ND-ITP/P-ITP (n=63) and C-ITP/R-ITP (n=48).Out of 111 ITP patients, 101 received treatments as 10 were refractory ITP. The median age of the ITP patient was 23±17.1 years as compared to controls 29±8.5years. Thirty-eight (34.2%) received oral prednisolone followed by Methylprednisolone (IV) 23(20.7%), Imuran 30(27%), IVIg and Revolade 4(3.6%), and dexamethasone 2(1.8%). The median age of ND-ITP/P-ITP, C-ITP/R-ITP was 20±17.21 and 21±18.06 years compared to control group which was 23±8.5years respectively. There were 42 children with age ≤16 years; among these 17 had chronic ITP while 2 children progressed to refractory ITP. A high proportion (n=56, 54.95%) of patients’ population was female (Table 1). The most frequent symptoms found in patients were bruises (n=52, 46.8%) followed by petechiae (n=30,27.02%) and bleeding from different body sites (n=17;15.31%). Two out of 111 patients presented with active HCV infection with anti-HCV antibodies and viremia confirmed by PCR. None of the patients was found positive for HBV or HIV.
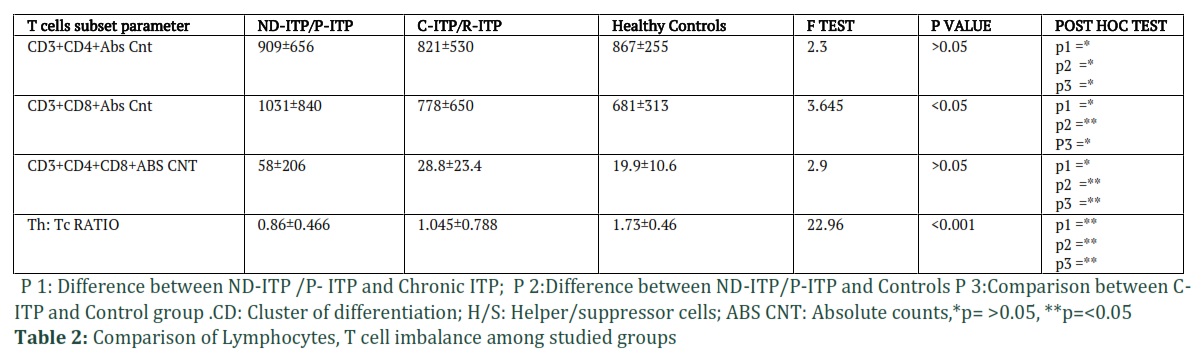
Significantly lower counts of platelets and elevated reticulated/immature platelet fraction (IPF) were observed in patients of ITP (p = <0.001; Table-1). The Th:Tc ratio was also significantly lower(0.86±0.466) in ND-ITP/P-ITP & C-ITP/R-ITP groups as compared to controls (p = <0.001; Table 2).
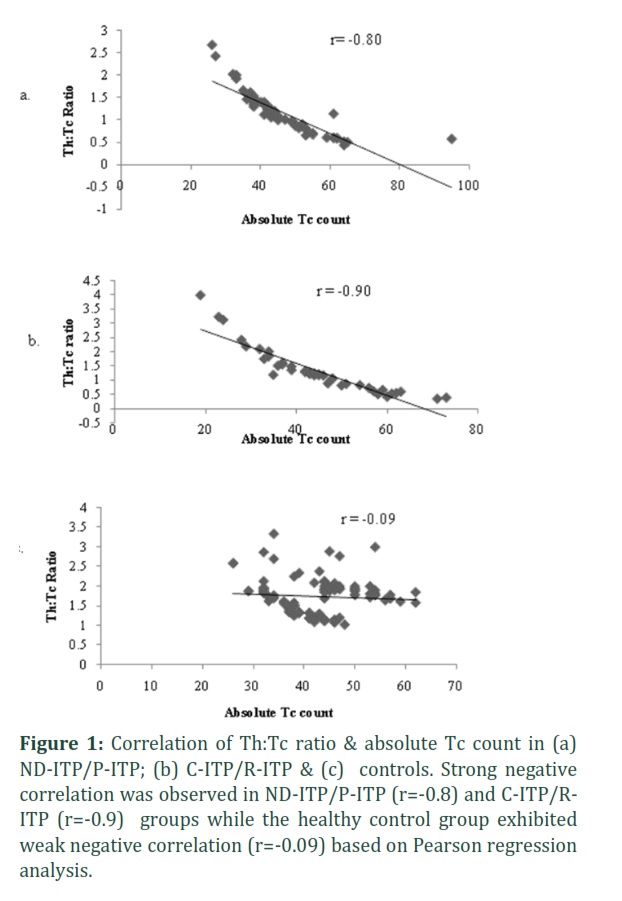
The correlation of Th:Tc ratio and high absolute Tc count was strongly negative in ND-ITP/P-ITP (r=-0.80) and chronic/refractory ITP (r=-0.90) as compared to healthy control group where only a weak negative correlation was observed. An interestingly high double positivity of CD4+and CD8+ T cells (DP-T cells) count was recorded in ND-ITP/P-ITP patients compared to controls (Table-2).
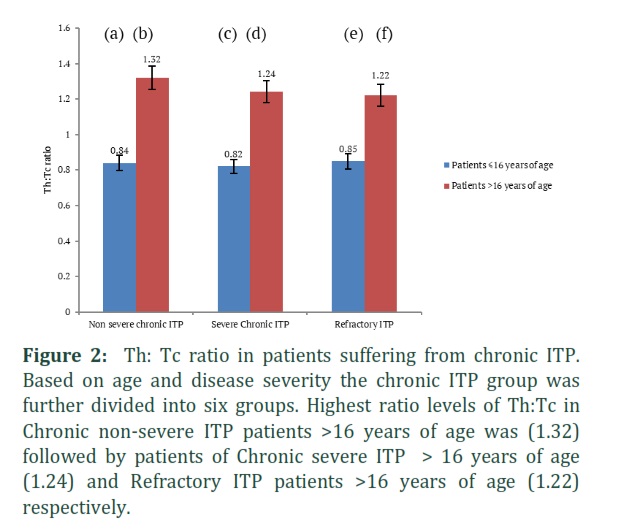
Altogether there were 19 children ≤16 years and 29 patients >16 years of age with chronic/refractory ITP enrolled in this study. In order to analyze the possible association of Th:Tc ratio with disease severity and chronicity; patients with non-severe C-ITP, severe C-ITP/R-ITP were grouped separately. A significantly low Th: Tc ratio was found in ≤16 years of age children with C-ITP/R-ITP (Figure:1). An insignificant difference (p= 0.89) between children with non-severe chronic (0.84±0.42), severe chronic (0.82±0.49) and refractory ITP (0.85±0.51) respectively. The flow cytometric presentation of T cell subset has been shown in (Figure 2).
Most of the refractory ITP patients (11/13) were adults (21-55years) with a predominantly high number of females (9/11). The average Th:Tc ratio for refractory ITP group was 1.03±0.42 altogether. Again, it was observed that the children ≤16 years with refractory ITP had a comparatively lower Th:Tc ratio 0.85±0.51 than patients >16 years (1.22±.52). According to platelet counts,53(47.7%) ITP patients were in active phase, 17(15.3%) partial remission, 11(9.9%) complete remission and 10(9.0%) patients were unresponsive to all given treatment. The T H/S ratio was low in active phase of disease with median of 0.99(1.40) indicating active patients were more prone to the involved in severity of ITP as compared with remission and non-responders’ groups. (Table 3)
Figures & Tables

ITP is not a gender dependent autoimmune disease but in our study most (63%) of the enrolled confirmed ITP patients were females, which is similar to previous observations [2,12-13]. It was observed that patients were presented with typical symptoms of ITP such as bruises, petechiae and bleeding from different sites; and reticulated or immature platelets fractions (IPF) were high which was in line with previous studies [14-16].
In ITP the immune tolerance is generally breached leading to overall immune dysregulation. It may involve anti-platelets antibody mediated destruction of platelets as well as Tc (CD8+) cells mediated platelets destruction in response to anti-platelets antibody dissolution. Tc cells are also capable of initiating antibody independent destruction of autologous platelets in ITP through cytolysis [17]. The Tc cause suppression of megakaryopoiesis resulting in decreased platelets production by stopping the apoptosis of bone marrow megakaryocytes in vitro study [18]. Thus, the cellular dysfunction leading to ITP may include abnormal functioning of Th, Tc and CD4+ regulatory cells [19-21]. In our study a significantly low Th:Tc ratio was observed in newly diagnosed/persistent ITP group suggesting that Th count was lower (909±656 /µl) as compared to Tc count (Table 2) which is supported by a previous study of Zhao et al., where CD4+/CD8+ ratio was significantly reduced in both ITP group (1.29±0.61;p <0.01), elderly group (1.32±0.62; p<0.05) in comparison to controls (1.56±0.29) [22]. Zahran and Elsayh also reported an apparently increased Tc% (26.21±0.89) in newly diagnosed acute ITP patients than in controls (22.95±0.83; 25) [23]. A small proportion i.e. 2-3% of peripheral blood of healthy individuals is CD4+CD8+DP T cells with occasional rise of up to 10% [24]. A diagnostically significant increased DP T cells count have been reported in autoimmune disorders like Kawasaki disease, multiple sclerosis, myasthenia gravis and ITP etc [25-28]. During the present study a twofold increased count was found in ND-ITP/P-ITP as compared to HC (Table 2). An insignificantly high DP T cell count (p=<0.05) was also observed in C-ITP/R-ITP confirming imbalance of T cell subpopulation in ITP.
In adults the average Th:Tc ratio for the chronic/refractory ITP group was high (1.32±0.52) indicating that it might have no correlation with the persistence of ITP in this group. A new and interesting finding of this study is that in children; with chronic/refractory ITP (n=19); aged ≤ 16 the average Th:Tc ratio was skewed towards a higher proportion of Tc (ratio 0.84±0.34). This suggests that the low Th:Tc ratio may be linked to chronicity/persistence of ITP in these children but not with the severity of disease. Since no apparent difference in Th:Tc ratio was found among the children with non-severe, severe and refractory ITP (Figure 2). This is in contrary to a previous study on 15 chronic ITP children where Th:Tc ratio was 1.17±0.52 and thus did not seem to had any association with the chronicity of ITP in children [29].
Elevated IPF and decreased platelet counts were observed in most ITP patients with clinically significant T cells imbalance. An age dependent T-cell imbalance i.e. increased Tc count in chronic/refractory ITP children (≤ 16 years) was observed compared to chronic/refractory ITP adults. Hence it can be concluded that elevation in levels of Tc in ITP may be influenced by patient’s age and thus a possible cause of chronicity in younger patients. This study is based on minimum individuals of participating children; therefore further studies are needed with larger sample size and additional parameters such as different lymphocyte subsets (Th1/Th2; Tc1/Tc2, T regs, natural killer cells etc.) to gain deeper insight.
Author Contributions
**AA performed tests, collected/ analyzed data. Prepared the initial draft of manuscript. **SNM planned and supervised the study. Reviewed, edited and finalized the paper. MB helped in sample collection and reviewed the manuscript. TSS provided the patients sample and reviewed the manuscript. **Both AA and SNM contributed equally to this study.
The authors declare that there is no conflict of interest.
![]()
References
- Coopamah MD, Garvey MB, Freedman J, Semple JW. Cellular immune mechanisms in autoimmune thrombocytopenic purpura: An update. Transfusion Medicine Reviews, (2003); 17(1): 69-80.
- Cines DB, Blanchette VS. Immune thrombocytopenic purpura. New England Journal of Medicine, (2002); 346(13): 995-1008.
- Stasi R, Evangelista ML, Stipa E, Buccisano F, Venditti A, Amadori S. Idiopathic thrombocytopenic purpura: current concepts in pathophysiology and management. Thrombosis and Haemostasis, (2008); 99(01): 4-13.
- Nomura S. Advances in diagnosis and treatments for immune thrombocytopenia. Clinical Medicine Insights: Blood Disorders, (2016); 9: 15-22.
- Zhang F, Chu X, Wang L, Zhu Y, Li L, Ma D, Peng J, Hou M. Cell‐mediated lysis of autologous platelets in chronic idiopathic thrombocytopenic purpura. European Journal of Haematology, (2006); 76(5): 427-431.
- Cines DB, Bussel JB, Liebman HA, Luning Prak ET. The ITP syndrome: pathogenic and clinical diversity. Blood, The Journal of the American Society of Hematology, (2009); 113(26): 6511-6521.
- Ogawara H, Handa H, Morita K, Hayakawa M, Kojima J, Amagai H, Tsumita Y, Kaneko Y, Tsukamoto N, Nojima Y, Murakami H. High Th1/Th2 ratio in patients with chronic idiopathic thrombocytopenic purpura. European Journal of Haematology, (2003); 71(4): 283-288.
- Kuwana M, Kaburaki J, Kitasato H, Kato M, Kawai S, Kawakami Y, Ikeda Y. Immunodominant epitopes on glycoprotein IIb-IIIa recognized by autoreactive T cells in patients with immune thrombocytopenic purpura. Blood, The Journal of the American Society of Hematology, (2001); 98(1): 130-139.
- Culic S, Labar B, Marusic A, Salamunic I. Correlations among age, cytokines, lymphocyte subtypes, and platelet counts in autoimmune thrombocytopenic purpura. Pediatric Blood and Cancer, (2006); 47(5): 671-674.
- Talaat RM, Elmaghraby AM, Barakat SS, El-Shahat M. Alterations in immune cell subsets and their cytokine secretion profile in childhood idiopathic thrombocytopenic purpura (ITP). Clinical and Experimental Immunology, (2014): 176(2): 291-300.
- Neunert C, Lim W, Crowther M, Cohen A, Solberg Jr L, Crowther MA. The American Society of Hematology 2011 evidence-based practice guideline for immune thrombocytopenia. Blood, The Journal of the American Society of Hematology, (2011); 117(16): 4190-4207.
- Cines DB, Bussel JB. How I treat idiopathic thrombocytopenic purpura (ITP). Blood. The Journal of the American Society of Hematology, (2005); 106(7): 2244-2251.
- Stasi R, Stipa E, Masi M, Cecconi M, Scimò MT, Oliva F, Sciarra A, Perrotti AP, Adomo G, Amadori S, Papa G. Long-term observation of 208 adults with chronic idiopathic thrombocytopenic purpura. The American journal of medicine, (1995); 98(5): 436-442.
- Page LK, Psaila B, Provan D, Michael Hamilton J, Jenkins JM, Elish AS, Lesser ML, Bussel JB. The immune thrombocytopenic purpura (ITP) bleeding score: assessment of bleeding in patients with ITP.The British Journal of Haematology, (2007); 138(2): 245-248.
- Naz A, Mukry SN, Shaikh MR, Bukhari AR, Shamsi TS. Importance of immature platelet fraction as predictor of immune thrombocytopenic purpura. Pakistan Journal of Medical Sciences, (2016); 32(3): 575-579.
- Briggs C, Kunka S, Hart D, Oguni S, Machin SJ. Assessment of an immature platelet fraction (IPF) in peripheral thrombocytopenia. British Journal of Haematology, (2004); 126(1): 93-99.
- Zhao C, Li X, Zhang F, Wang L, Peng J, Hou M. Increased cytotoxic T-lymphocyte-mediated cytotoxicity predominant in patients with idiopathic thrombocytopenic purpura without platelet autoantibodies.Haematologica, (2008); 93(9): 1428-1430.
- Yang L, Wang L, Zhao CH, Zhu XJ, Hou Y, Jun P, Hou M. Contributions of TRAIL-mediated megakaryocyte apoptosis to impaired megakaryocyte and platelet production in immune thrombocytopenia. Blood,The Journal of the American Society of Hematology, (2010); 116(20): 4307-4316.
- Semple JW, Milev Y, Cosgrave D, Mody M, Hornstein A, Blanchette V, Freedman J. Differences in serum cytokine levels in acute and chronic autoimmune thrombocytopenic purpura: relationship to platelet phenotype and antiplatelet T-cell reactivity.Blood.The American Journal of Hematology, (1996); 87(10): 4245-4254.
- Sakakura M, Wada H, Tawara I, Nobori T, Sugiyama T, Sagawa N, Shiku H. Reduced Cd4+ Cd25+ T cells in patients with idiopathic thrombocytopenic purpura. Thrombosis Research, (2007); 120(2): 187-193.
- Olsson B, Andersson PO, Jernås M, Jacobsson S, Carlsson B, Carlsson LM, Wadenvik H. T-cell-mediated cytotoxicity toward platelets in chronic idiopathic thrombocytopenic purpura. Nature Medicine, (2003); 9(9): 1123-1124.
- Zhao Z, Yang L, Yang G, Zhuang Y, Qian X, Zhou X, Xiao D, Shen Y. Contributions of T lymphocyte abnormalities to therapeutic outcomes in newly diagnosed patients with immune thrombocytopenia. PLoS One, (2015); 10(5): e0126601.
- Zahran AM, Elsayh KI. CD4+ CD25+ High Foxp3+ regulatory T cells, B lymphocytes, and T lymphocytes in patients with acute ITP in Assiut Children Hospital. Clinical and Applied Thrombosis/Hemostasis, (2014); 20(1): 61-67.
- Sala P, Tonutti E, Feruglio C, Florian F, Colombatti A. Persistent expansions of CD4+ CD8+ peripheral blood T cells. Blood. The American Journal of Hematology, (1993); 82(5): 1546-1552.
- Hirao JI, Sugita K. Circulating CD4+ CD8+ T lymphocytes in patients with Kawasaki disease. Clinical and Experimental Immunology, (1998); 111(2): 397-401.
- Berrih S, Gaud C, Bach MA, Le Brigand H, Binet JP, Bach JF. Evaluation of T cell subsets in myasthenia gravis using anti-T cell monoclonal antibodies. Clinical and Experimental Immunology, (1981); 45(1): 1-8.
- Waschbisch A, Sammet L, Schröder S, Lee DH, Barrantes-Freer A, Stadelmann C, Linker RA. Analysis of CD4+ CD8+ double-positive T cells in blood, cerebrospinal fluid and multiple sclerosis lesions. Clinical and Experimental Immunology, (2014); 177(2): 404-411.
- Scott CS, Wheeler R, Ford P, Bynoe AG, Roberts BE. T lymphocyte subpopulations in idiopathic thrombocytopenic purpura (ITP). Scandinavian Journal of Haematology, (1983); 30(5): 401-406.
- El-Rashedi FH, El-Hawy MA, Helwa MA, Abd-Allah SS. Study of CD4+, CD8+, and natural killer cells (CD16+, CD56+) in children with immune thrombocytopenic purpura. Hematology/oncology and Stem Cell Therapy, (2017); 10(1): 8-14.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0

