

![]()
Comparative in-vitro evaluation of antibacterial activity of levofloxacin brands available in Pakistan
Sajid Bashir1, Syeda Rabia Nasir1, Faisal Usman2, Ibrahim Javed2*
Adv. life sci., vol. 2, no. 4, pp. 165-170, August 2015
*- Corresponding Author: Ibrahim Javed (Email: ibr_pharmacist@yahoo.com)
Authors' Affiliations[Date Received: 25/05/2015; Date Revised: 10/08/2015; Date Published Online: 25/08/2015]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Supplementary Data
Abstract
Background: Antimicrobial susceptibility against marketed antibiotic products is dynamic and changes with development of resistance in microbes. Susceptibility status of antibiotics helps health care practitioners in refining their prescribing trends and selection of suitable antibiotic and its commercial brand. Objective of this study was to evaluate the antimicrobial sensitivity and susceptibility patterns of levofloxacin of different national and multinational brands in Pakistan. Levofloxacin is among the commonly mis-prescribed antibiotic in Pakistan and this study will give an insight of microbial resistance/susceptibility status against quinolones and help prescribing practice.
Methods: In this study 29 different brands of levofloxacin from different cities of Pakistan are evaluated for their sensitivity against four microbial strains i.e. Staphylococcus aureus, Staphylococcus epidermidis, Escherichia coli, Klebsiella Pneumonia. Evaluation was performed via disc diffusion method against standard drug discs.
Result: Different brands exhibited different antimicrobial status regardless of their price and national or multinational status. In low price range, Levomerc while Tavanic in high price range showed significant antimicrobial activity. Different brands are evaluated and compared statistically with price and activity as variant.
Conclusion: Antimicrobial activity of different brands of levofloxacin varied regardless of their national/multinational status and price factor. This study refined the suitability of different brands of levofloxacin against respective pathogens and disease indications.
Keywords: Levofloxacin, Brands, Infections, Resistance, Staphylococcus aureus, Staphylococcus epidermidis, Escherichia coli, Klebsiella Pneumonia
Introduction
Resistance against numerous antimicrobial drugs has become a serious threat in health care centers and hospitals. As per usage, an abrupt increase in resistance has been recorded for Quinolones from last few years [1-3]. Among quinolones, levofloxacin is a model drug and is commonly prescribed in many infections. So, it is always interesting for the practitioners to have an updated insight of antimicrobial resistance and susceptibility pattern of these frequently used antimicrobial drugs against common infections.
Developing countries, as in Asia, are more prone to infectious diseases either topically acquired via contagious and unhygienic contact with environment or from food i.e. food poisoning which leads to more frequent prescriptions of antibiotics [4, 5]. This is also associated with increased misuse of antibiotics leading to development of microbial resistance [6]. Levofloxacin is one of the most commonly prescribed antibiotic in developing countries, participating majorly in emergence of antibiotic resistance in Asia. It is commonly used as effective agent against food borne poisoning related to E. coli and Staphylococcus strains [7, 8].
Thus sensitivity pattern of different brands of levofloxacin is evaluated and compared with standard, against 4 different bacterial strains which are more likely and reported to acquire resistance against quinolones [9-11].
Methods
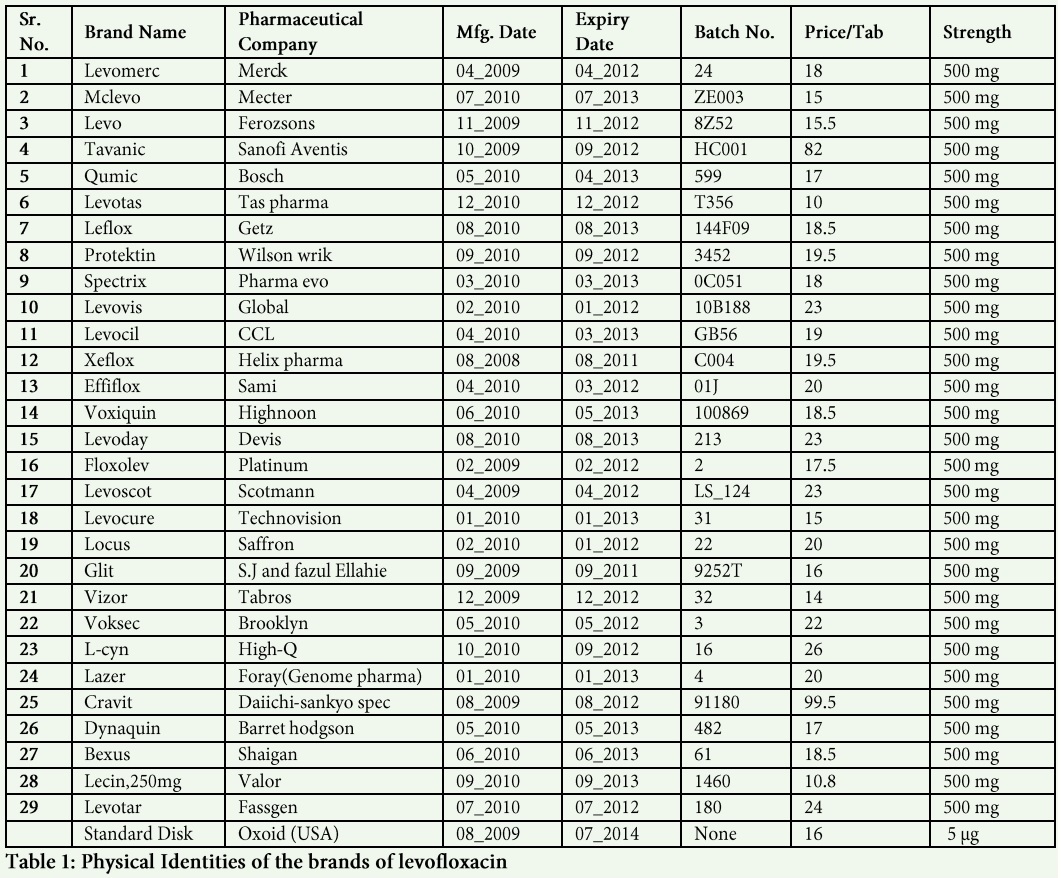
Twenty nine (29) different local and multinational brands of levofloxacin were collected from different cities of Pakistan (Lahore, Faisalabad and Sargodha) and used in this study (Table 1). Antibiotic sensitive levofloxacin discs (Oxoid CT 1615 B, USA) were used as standard. Bacterial strains i.e. Staphylococcus aureus (ATCC 25923), Staphylococcus epidermidis (ATCC 12228), Escherichia coli (ATCC 8739), Klebsiella pneumonia (ATCC 700603) (Liofilchem, Italy) were used for susceptibility testing.
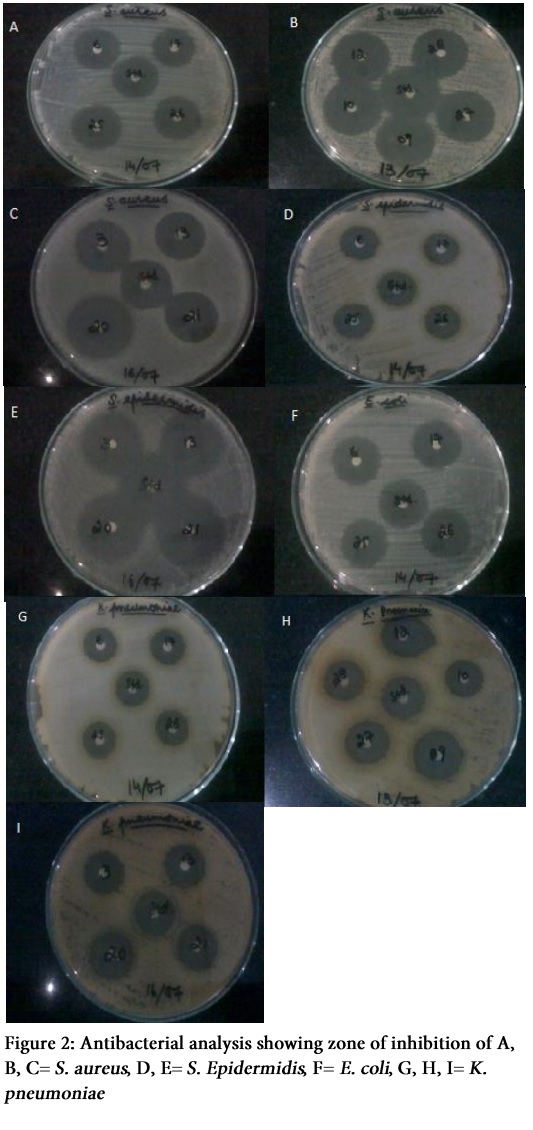
All required bacterial media i.e. Mueller Hinton Agar, Nutrient Agar, Broth and sample antibiotic discs were prepared according to standard laboratory protocols [12]. Briefly, sample tablets were dissolved in deionized and double distilled water. The solution was diluted to obtain the final concentration of 5 µg / 20 µl, which was pipetted on pre-sterilized, 6 mm Whattman filter paper discs. Bacterial inoculum of 0.5% McFarland standard solution was prepared by method reported in literature [13, 14]. Bacterial susceptibility testing was performed via disc diffusion method according to National Committee for Clinical Laboratory Standards (NCCL, M100-S12, 2002). Petri dishes containing Mueller Hinton Agar were inoculated with bacterial strains using a sterilized swab. Filter paper discs, impregnated with sample antibiotic (5 µg) and standard discs were placed and pressed in agar. These discs were incubated and zone of inhibition was measured in mm. One way ANOVA and Tukey test was applied to interpret the results.
Results
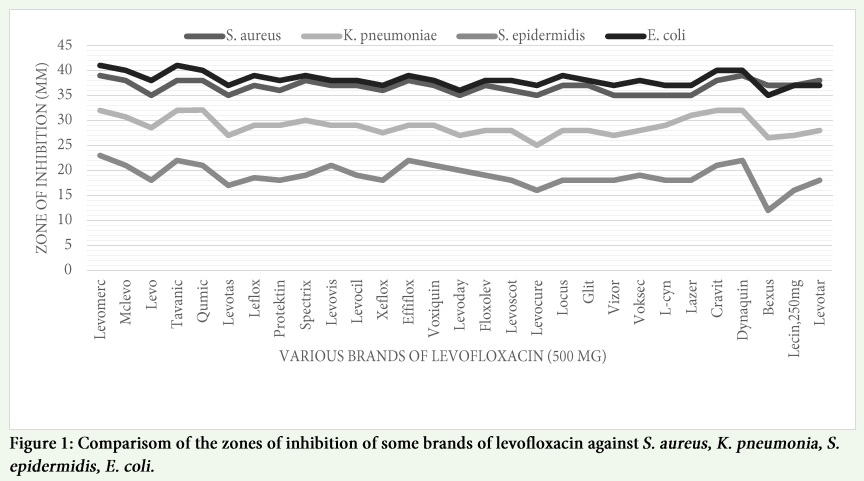
The results of each levofloxacin products against S. aureus revealed that all brands gave satisfactory inhibition zones (Table S1). Levomer and Dynaquin had shown excellent zones of inhibition while Lazer, Levoday, Levocure, L-cyn, Levotasm, Voksec, Levo and Vizor gave the minimum zones. From the results of ANOVA F-test (Table S2) there was a statistical difference among the brands (P = 0.000). Results from Tukey comparison test (Table S3) revealed that there was significant difference among Levomerc, Levo, Levotas, Vizor, Voksec, L-cyn, Lazer, Levoday, Levocure, Dynaquin (P = 0.006).
In case of S. epidermidis, “Levomerc” (23 ± 0.3266 mm) gave excellent zone and “Bexus” (12 ± 0.8165 mm) gave minimum zone of inhibition that shows less effectiveness of “Bexus” as compared to rest of three bacteria (Table S1). The results of ANOVA F-test (Table S4) have shown that data was statistically significant (P = 0.000). Tukey comparison test (Table S5) indicated that activity of “Levomerc” was statistically different from “Levocure”, “Bexus”, “Lecin” (P = 0.00) and from “Levotas” (P = 0.001).
Most interestingly, remarkable zones of inhibition were seen with the “Levomerc” (41 ± 0.141 mm) and “Tavanic” (41 ± 0.408) against E. coli. “Bexus” (35 ± 0.326 mm) gave minimum zone of inhibition (Table S1). From the results of ANOVA F-test (Table S6), there was statistically significant difference among brands (P = 0.000). The zones of inhibition of brands against K. pneumonia indicated that “Levomerc” (32 ± 0 mm), “Cravit” (32 ± 0.04082), “Qumic” (32 ± 0.12472 mm), “Dynaquin” (32 ± 0.36742 mm) and “Tavanic” (32 ± 0.40825 mm) gave maximum zones and “Levocure” (25 ± 1.22474 mm) gave minimum zone of inhibition. Results were statistically significant (P = 0.000) as shown in ANOVA Table (Table S8). Results of Tukey test (Table S9) indicated that most of brands were statistically different from one another. “Levomerc” was statistically different from all brands except from “Spectrix” (P = 0.396), “Mclevo” (P = 0.969), “Lazer” (P = 0.999), “Tavanic”, “Qumic”, “Cravit” and “Dynaquin” (P = 1).
Figures and Tables
Discussion
Present study was conducted to evaluate the susceptibility of S. aureus, S. epidermidis, E. coli and K. pneumonia against 29 local and multinational brands of levofloxacin in Pakistan. Infections caused by these bacteria are more prevalent in developing countries of Asia. Usually, fluoroquinolones are mostly prescribed to cure these infections, so their chances to develop resistance are fairly high. Out of these 4 selected strains, S. aureus, E. coli and K. pneumoniea are among the major strains investigated for food borne diseases [15]. Among major food sources in Pakistan, milk and poultry is found to be directly associated with Staphylococcal and Klebsiella based infections [16,17]. Disc diffusion method is employed in this study to perform anti-microbial activity of collected brands [18,19]. However, this method has reported to impart inaccuracies in results and somewhat results are not comparable across laboratories but in case of macrolide and quinolones i.e. ciprofloxacin and levofloxacin, this method is suitable and can be employed for initial susceptibility testing [20].
It was depicted in this study that the recorded efficacies of some brands of the levofloxacin sold in Pakistan, differ in their efficacies or potencies depending upon their brands or manufacturers. Some showed a higher efficacy and some showed lower efficacy when compared to the standard control. The differences in activities may be due to variations in the sources of raw materials (active and excipients), defective storage facilities and mishandling during distribution as described by previous reported studies [21,22]. Furthermore stability and storage conditions of the medications can also influence its therapeutic potency and this effect is more prominent when medication contain hydrophilic excipients and transported in humid and high temperature countries like Pakistan [23,24]. These differences in efficacies among available brands of antibiotic constitute a possible risk to health of patients. It was evaluated by various studies [25,26] that in developing countries, many manufactured drugs are implicated to be substandard. In developing countries the choice is influenced by manufacturer’s marketing strategies [22,27].
The different local and multinational brands of levofloxacin available in Pakistan showed effective but varying antibacterial activities against four selected susceptible organisms. As a whole “Levomerc” and “Dynaquin” have showed excellent efficacies with low price and their choice would be cost-effective while “Tavanic” and “Cravit” have shown comparatively less activity with high price but good activity in comparison to remaining brands. Levofloxacin is one of the most promising and commonly used newer quinolones that has broad spectrum of activity against both gram-positive and gram-negative organisms. The results of present study invite and give directions for evaluation of quinolones against other common disease causing microbes specifically in developing countries of Asia.
Conflict of Interest
Authors have no conflict of interest to declare.
References
- Robicsek A, Jacoby GA, Hooper DC. The worldwide emergence of plasmid-mediated quinolone resistance. The Lancet infectious diseases, (2006); 6(10): 629-640.
- Jacoby GA. Mechanisms of resistance to quinolones. Clinical Infectious Diseases, (2005); 41(Supplement 2): S120-S126.
- Lowy FD. Antimicrobial resistance: the example of Staphylococcus aureus. Journal of Clinical Investigation, (2003); 111(9): 1265.
- Istúriz RE, Carbon C. Antibiotic use in developing countries. Infection Control and Hospital Epidemiology, (2000); 21(6): 394-397.
- Zaidi AK, Awasthi S, Janaka deSilva H. Burden of infectious diseases in South Asia. British Medical Journal, (2004); 328811-815.
- Okeke IN, Lamikanra A, Edelman R. Socioeconomic and behavioral factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerging Infectious Diseases, (1999); 5(1): 18.
- Zhang Y, Cheng S, Ding G, Zhu M, Pan X, et al. Molecular analysis and antibiotic resistance investigation of Staphylococcus aureus isolates associated with staphylococcal food poisoning and nosocomial infections. African Journal of Biotechnology, (2013); 10(15): 2965-2972.
- Saito N, Kawano M, Kobayashi T, Watanabe S, Yamada W, et al. An outbreak of food poisoning caused by an enteropathogenic Escherichia coli O115: H19 in Miyagi Prefecture. Japanese Journal of Infectious Diseases, (2005); 58(3): 189.
- Cantón R, Loza E, Morosini MI, Baquero F. Antimicrobial resistance amongst isolates of Streptococcus pyogenes and Staphylococcus aureus in the PROTEKT antimicrobial surveillance programme during 1999-2000. Journal of Antimicrobial Chemotherapy, (2002); 50(suppl 2): 9-24.
- Emmerson A, Jones A. The quinolones: decades of development and use. Journal of Antimicrobial Chemotherapy, (2003); 51(suppl 1): 13-20.
- Johnson L, Sabel A, Burman WJ, Everhart RM, Rome M, et al. Emergence of Fluoroquinolone Resistance in Outpatient Urinary Escherichia coli Isolates. The American Journal of Medicine, (2008); 121(10): 876-884.
- Nkang A, Okonko I, Lennox J, Eyarefe O, Abubakar M, et al. Assessment of the efficacies, potencies and bacteriological qualities of some of the antibiotics sold in Calabar, Nigeria. African Journal of Biotechnology, (2010); 9(41): 6987-7002.
- Bartlett J, Finegold S. Bacteriology of expectorated sputum with quantitative culture and wash technique compared to transtracheal aspirates. The American Review of Respiratory Disease, (1978); 117(6): 1019-1027.
- Shaikh D, Ashfaq S, Shaikh K, Shaikh M, Naqvi BS, et al. Studies on resistance/sensitivity pattern of bacteria related with urinary tract infections. Medical Journal of Islamic World Academy of Sciences, (2005); 15(4): 129-133.
- Thong K, Lai M, Teh C, Chua K. Simultaneous detection of methicillin-resistant Staphylococcus aureus, Acinetobacter baumannii, Escherichia coli, Klebsiella pneumoniae and Pseudomonas aeruginosa by multiplex PCR. Tropical Biomedicine, (2011); 28(1): 21-31.
- Batool SA, Kalsoom R, Rauf N, Tahir S, Hussain F. Microbial and physico–chemical quality assessment of the raw and pasteurized milk supplied in the locality of Twin city of Pakistan. Internet Journal of Food Safety, (2012); 1417-22.
- Ashraf MR, Asif M, Firyal S, Anjum AA, Waheed U, et al. Molecular Characterization and Association of Local Isolates of Staphylococcus aureus on The Basis of 16S rRNA in Poultry and Human in Pakistan. Life, (2014); 12(3): 160-164.
- Matuschek E, Brown D, Kahlmeter G. Development of the EUCAST disk diffusion antimicrobial susceptibility testing method and its implementation in routine microbiology laboratories. Clinical Microbiology and Infection, (2014); 20(4): O255-O266.
- Kronvall G, Giske CG, Kahlmeter G. Setting interpretive breakpoints for antimicrobial susceptibility testing using disk diffusion. International Journal of Antimicrobial Agents, (2011); 38(4): 281-290.
- Lehtopolku M, Kotilainen P, Puukka P, Nakari U-M, Siitonen A, et al. Inaccuracy of the disk diffusion method compared with the agar dilution method for susceptibility testing of Campylobacter spp. Journal of Clinical Microbiology, (2012); 50(1): 52-56.
- Mukhtar M, Chedi BZ, Aliyu M, Umar MS, Abdullahi, AA. In-Vitro Assessment of Some Oral Ciprofloxacin Brands Traded in Kano–Nigeria. International Journal of Pharmaceutical Sciences, (2010); 2(1): 13-17.
- Representing B. Ofloxacin: laboratory evaluation of the antibacterial activity of 34 brands representing 31 manufacturers available in Pakistan. Pakistan Journal of Medical Sciences, (2004); 20(4): 349-356.
- Javed I, Ranjha NM, Massud A, Hussain L. Accelerated Stability Studies of Flurbiprofen Film Coated Tablets of Five Different National Brands in Pakistan. Journal of Drug Delivery and Therapeutics, (2013); 3(2): 9-11.
- Javed I, Ranjha N, Mahmood K, Kashif S, Rehman M, et al. Drug release optimization from microparticles of poly (E-caprolactone) and hydroxypropyl methylcellulose polymeric blends: formulation and characterization. Journal of Drug Delivery Science and Technology, (2014); 24(6): 607-612.
- Kelesidis T, Kelesidis I, Rafailidis PI, Falagas ME. Counterfeit or substandard antimicrobial drugs: a review of the scientific evidence. Journal of Antimicrobial Chemotherapy, (2007); 60(2): 214-236.
- Shakoor O, Taylor R, Behrens R. Assessment of the incidence of substandard drugs in developing countries. Tropical Medicine & International Health, (1997); 2(9): 839-845.
- Newton PN, Fernandez FM, Green MD, Primo-Carpenter J, White NJ (2010). Counterfeit and substandard anti-infectives in developing countries. Antimicrobial Resistance in Developing Countries: Springer. pp. 413-443.