

Full Length Research Article
Association patterns of Atrial Fibrillation with symptoms of metabolic syndrome
Saima Sharif1,*, Tasnim Farasat1, Saira Rafaqat1, Shagufta Naz1, Farkhanda Manzoor1, Muhammad Saqib2
Adv. life sci., vol. 4, no. 3, pp. 92-96, May 2017
*- Corresponding Author: Dr. Inaam Ullah (Email: ssharif1978@yahoo.com)
Authors' Affiliations
2- Jinnah Hospital Lahore – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Atrial fibrillation (AF) is the common cardiac arrhythmia in which heart beats irregularly usually greater than 100 beats per minutes. AF is well-documented public health problem causing substantial mortality and morbidity. Metabolic syndrome (MS) is a collection of metabolic risk factors like diabetes, hypertension, dyslipidemia, obesity and impaired glucose level that exists in one person. The aim of the present study is to find the relation between AF and MS.
Methods: 100 patients of AF were sampled from Punjab Institute of Cardiology, Lahore from December, 2014 to June 2015. These patients were divided into two AF groups, 50 without MS and 50 with MS. 25 healthy subjects were also included for the comparison. Lipid profile was assessed by chemistry analyzer and serum insulin was measured by ELISA.
Results: In our population, there was significantly high levels of insulin resistance (IR) and obesity in AF groups (without MS and with MS) as compared with healthy subjects (P<0.05). Highly significant differences was observed in relation with other parameters e.g. hypertension, hypertriglyceridemia, HDL-C among the studied groups (P<0.05). Significant positive correlation was observed between insulin and lipid profile (TC, TG, LDL) while inverse with HDL.
Conclusion: The indictors of metabolic syndrome were significantly correlated with AF in the studied subjects, while IR was found significantly higher in MS group.
Key words: Atrial Fibrillation, metabolic syndrome
Introduction
Atrial fibrillation or AF is usually cardiac arrhythmia in which heart beats irregularly usually too fast. AF affects 33.5 million people at global level [1]. After 80 years of age 8% of the individuals are affected with AF so age is a major risk for the development of AF. “It took 69 years for the percentage to double from 7% to 14% in the United States (1944 to 2013), but this doubling of the over 65 age group is expected to occur in only 26 years in China (2000 to 2026). The burden of AF at age 65 years (226 DALYs/100,000) is nearly 7 times that at age 45 years (33 DALYs/100,000) and only one-quarter that at ages 80 and older (936 DALYs/100,000)” [1].
The causes of AF are aging, cardiomyopathy, valvular heart diseases, coronary artery disease, obesity, diabetes mellitus, chronic obstructive pulmonary diseases, structural heart diseases, hypertension, excessive alcohol consumption, sleep disturbances, thyroid dysfunction, chronic renal diseases, congenital heart diseases and previous heart surgery. Some of the genetic mutations may be responsible for the development of AF [2]. The signs and symptoms of AF are rapid heart rate, shortness of breath, swelling, palpitation, fatigue, discomfort, dizziness, weakness, and exercise intolerance all these symptoms lead to fainting or collapse [3, 4].
Metabolic syndrome is referred to a condition in which energy storage and utilization are present. It is defined as cluster of metabolic risk factors. The clustering category of metabolic syndrome is known as a syndrome X. The prevalence of metabolic syndrome increases as age increased and in USA about 34% adult populations have Metabolic Syndrome [5, 6]. Metabolic syndrome is a premier risk factor for cardiovascular disease. It is also a risk factor for the development AF, it increases the mortality rate about 1.5 fold and 2-fold increases the cardiovascular events [7].
The linking factors that develops the relationship of AF with metabolic syndrome are oxidative stress, inflammation, insulin resistance, high plasma volume, neurohormonal activation, atrial remodeling which changes the ion channel, atrial structure, cellular hypertrophy, tissue fibrosis, activation of fibroblasts, calcium homeostasis, sympathetic activity increase, left ventricular diastolic activity is also increased, loss of muscle mass, mechanical stress, atrium enlargement, spatial remodeling of gap junction, fibrosis and increases the conduction system of heart activity [8].
Insulin is secreted from beta cells of pancreas. The decreased sensitivity of target tissues of insulin secretion is called insulin resistances. It is also called type 2 diabetes mellitus which is non- insulin dependent diabetes mellitus (NIDDM), is caused by decreased sensitivity to insulin. It is primary cause of increased blood glucose concentration. It is also the major cause of cardiovascular diseases [9, 10].
Methods
Study design
This cross-sectional study (n=125) was conducted in Punjab Institute of Cardiology, Lahore from December, 2014 to June 2015. Sample size was calculated by Raosoft software using 7% margin of error, with response distribution of 65%. The subjects were selected from outdoor patients and from Emergency Department of Jilani block. The subjects suffering from atrial fibrillation were diagnosed by the expert physicians of PIC on the basis of ECG and they were not suffering from any other disorder. A total of 100 subjects suffering from AF were selected that were further categorized into two groups on the presence and absence of metabolic syndrome. AF group without MS (n=50) and AF group with MS (n=50). Normal healthy subjects (n=25) of same age group were also included for comparison.
Estimation of BMI and WHR
BMI was calculated by weight in kg and height in meters square by using the formula as Weight (kg) /Height (m)2 [11]. For the measurement of WHR or waist hip ratio, a tape measuring was used to measure circumference of his or her 1 inch (2.54 cm) above the umbilicus and hips.
Estimation of systolic and diastolic blood pressure
Both the systolic and diastolic blood pressure was measured by using the B.P apparatus/ sphygmomanometer.
Estimation of FBG, TC, triglycerides levels, LDL-C and HDL-C parameters
Fasting Blood Glucose (FBG) were measured by using the glucometer. Serum was used for the measurement of total cholesterol, triglycerides levels, LDL-C and HDL-C by using the kits on chemical analyzer.
Estimation of insulin and insulin resistance (IR)
The NCEP-ATP III report (2001) defined the criteria of MS [12]. The insulin levels were measured by Enzyme-Linked Immunosorbent Assay (ELISA). Insulin resistance was measured by using the formula = (Fasting plasma insulin [micro units per milliliter]) x (Fasting plasma glucose [micromole per liter]) / 22.5 [13].
Statistical analysis
The datasheet was made on MS excel 2015. Data was expressed as mean ± SEM. Difference between the groups was determined with the help of one way ANOVA test. While all the statements of significance were based on the probability level of 0.05 and highly significant were based on 0.01 level of probability at 95% confidences interval. The relationship between the parameters was found out by bivariate Pearson correlation analysis. The analysis was done with the help of SPSS version 20.
Results
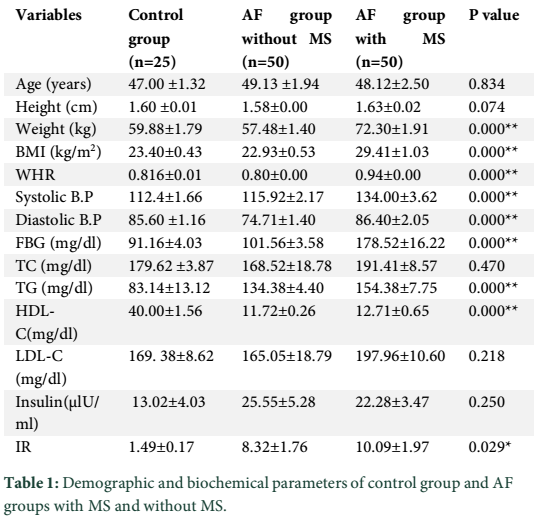
This study was done on 125 subjects that were divided into three groups, control group (n=25), AF group without MS (n=50) and with MS (n=50). The subjects were further categorized on the basis of gender. In control group, 50% (n = 12) were males while 50% (n = 13) subjects were females. In AF groups both without and with MS. 42% (n = 21) subjects were males and 58% (n = 29) subjects were females.
The demographic and biochemical characteristics of the study population were presented in table 1. The subjects with and without metabolic syndrome have higher insulin levels and insulin resistance as compared to the control group. ANOVA revealed significant differences in the BMI, WHR, systolic, diastolic blood pressure and lipid profile in the atrial fibrillated subjects as compared to control (p<0.05). While IR was significantly higher in males of with and without metabolic syndrome groups.
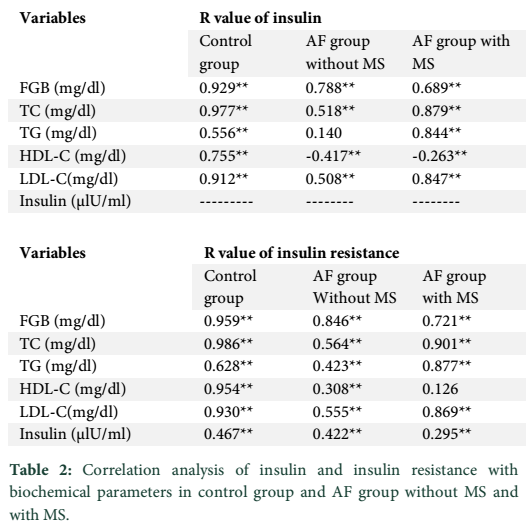
The relationship of insulin with biochemical parameters was also found out by using two-tailed Pearson correlation analysis presented in table 2.
The relationship of insulin and insulin resistance with lipid profile was significantly correlated in AF group with and without MS.
Tables & Figures
Discussion
Atrial fibrillation is a serious public health disease. It is associated with increased systemic thromboembolism, heart failure, and death. In the present study, age is a major risk factor for the prevalence of both the atrial fibrillation and metabolic syndrome. The study group was age matched. Other studies reported that at the age of 40-50 years, the prevalence of AF was ˂ 0.5%. The individuals with the age of 80 years, it was 5-15%. The individual that aged ≥85 years; it was 18%. In the past two decades the incidence of AF had increased about 13%. It was affecting more males as compared to females [14, 15] as compared to this study where 58% subjects were females.
In the present study the BMI and WHR, both are significantly higher in AF group as compared to control. While in the AF group with MS, females were overweight as compared to control females. These results were similar to other studies which indicated that obesity was a major risk factor for the atrial fibrillation. Increased BMI also predispose individuals to other disease like hypertension and diabetes [16, 17]. In our general population it ultimately increases the health risks.
In present study, blood insulin levels have been raised in AF group as compared to control but contradictory results have been reported in the Framingham cohort study between insulin resistance and AF. On the contrary, several studies had shown that in metabolic syndrome, insulin resistance is a crucial component and is related to incidence of AF. Insulin causes vasoconstriction and subsequent blood pressure elevation [18]. In the studied group AF group without MS, the raised insulin levels may affect vascular compliance and predispose subjects to AF.
Insulin resistance is a major component of metabolic syndrome and also a risk factor for cardiovascular diseases. Significant difference in IR was observed in the studied groups. It has been reported that the early onset of type 2 diabetes is the result of IR and then hypertension which also leads to various complications of cardiovascular diseases [19].
Fontes et al. reported that IR was not associated with AF [20]. While our study indicated that IR has a role in causing AF because in group without MS the IR may be the factor contributing towards AF. While it has been reported by Yuji et al. that there was increased evidence of link between MS and the development of AF although the independent effect of MS on LA size was still undetermined. Their study indicated that LA size was influenced by IR and obesity that were integral components of the MS. It was independently associated with LV hypertrophy, LV geometry and LV diastolic function in non-diabetic Japanese hypertensive patients [20]. Yuji et al. study showed that IR was highly prevalent among non-diabetic patients with hypertrophic cardiomyopathy (HCM) [21]. They also reported a possible mechanism by which IR was affected the development of AF that was mediated through its association with increased LA size or impaired LV diastolic function. IR might be an important underlying mechanism for the genesis of AF in HCM [22].
In present study significant direct association was observed with insulin/IR and lipid profile that revealed that as IR increased, the TC, TG also increased because of inability of insulin to perform its function.
Insulin resistance syndrome was clinically defined as the presence of high blood pressure, fasting blood sugar ≥100 mg/dL, large waist circumference, and low HDL and high triglycerides. These factors were also risk factor for AF. Insulin resistance was associated with inflammation, diabetes and obesity. Both diabetes and obesity are associated with insulin resistance. So insulin resistance is an intermediate step for the development of AF and is a common metabolic substrate that is associated with several cardiovascular conditions. IR is correlated with known AF risk factors like hypertension, BMI and fasting impaired glucose.
The indictors of metabolic syndrome were significantly correlated with AF in the studied subjects, while IR was found significantly higher in MS group.
Acknowledgment
Authors are thankful to Punjab Institute of Cardiology, Lahore for providing support in blood collection.
Conflict of Interest
Authors declare no conflict of interest.
References
- Chugh SS, Roth GA, Gillum RF, Mensah GA. Global burden of atrial fibrillation in developed and developing nations. Global Heart, (2014); 9(1): 113-119.
- Anumonwo JM, Kalifa J. Risk factors and genetics of atrial fibrillation. Cardiology clinics, (2014); 32(4): 485-494.
- Heart TN. Atrial fibrillation: Current understandings and research imperatives. Journal of the American College of Cardiology, (1993); 22(7): 1830-1834.
- Disch DL, Greenberg ML, Holzberger PT, Malenka DJ, Birkmeyer JD. Managing chronic atrial fibrillation: a Markov decision analysis comparing warfarin, quinidine, and low-dose amiodarone. Annals of Internal Medicine, (1994); 120(6): 449-457.
- Kaur J. A comprehensive review on metabolic syndrome. Cardiology research and practice, (2014); 2014: 943162.
- Ford ES, Li C. Defining the metabolic syndrome in children and adolescents: will the real definition please stand up? The Journal of pediatrics, (2008); 152(2): 160-164. e113.
- Hung C-L, Chao T-F, Lai Y-H, Yen C-H, Wang K-L, et al. The relationship among atrium electromechanical interval, insulin resistance, and metabolic syndrome. Canadian Journal of Cardiology, (2013); 29(10): 1263-1268.
- Watanabe H, Tanabe N, Watanabe T, Darbar D, Roden DM, et al. Metabolic syndrome and risk of development of atrial fibrillation. Circulation, (2008); 117(10): 1255-1260.
- DeWitt DE, Hirsch IB. Outpatient insulin therapy in type 1 and type 2 diabetes mellitus: scientific review. Jama, (2003); 289(17): 2254-2264.
- Gurnell M, Savage DB, Chatterjee VKK, O’Rahilly S. The metabolic syndrome: peroxisome proliferator-activated receptor γ and its therapeutic modulation. The Journal of Clinical Endocrinology & Metabolism, (2003); 88(6): 2412-2421.
- Östgren CJ, Merlo J, Råstam L, Lindblad U. Atrial fibrillation and its association with type 2 diabetes and hypertension in a Swedish community. Diabetes, Obesity and Metabolism, (2004); 6(5): 367-374.
- Expert Panel on Detection E. Executive summary of the Third Report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). Jama, (2001); 285(19): 2486-2497.
- Pastucha D, Filipcikova R, Horáková D, Radová L, Marinov Z, et al. The incidence of metabolic syndrome in obese Czech children: the importance of early detection of insulin resistance using homeostatic indexes HOMA-IR and QUICKI. Physiological Research, (2013); 62(3): 277-283.
- Heeringa J, van der Kuip DA, Hofman A, Kors JA, van Herpen G, et al. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. European Heart Journal, (2006); 27(8): 949-953.
- Naccarelli GV, Varker H, Lin J, Schulman KL. Increasing prevalence of atrial fibrillation and flutter in the United States. The American Journal of Cardiology, (2009); 104(11): 1534-1539.
- Karasoy D, Bo Jensen T, Hansen ML, Schmiegelow M, Lamberts M, et al. Obesity is a risk factor for atrial fibrillation among fertile young women: a nationwide cohort study. EP Europace, (2013); 15(6): 781-786.
- Kurth T, Gaziano JM, Berger K, Kase CS, Rexrode KM, et al. Body mass index and the risk of stroke in men. Archives of Internal Medicine, (2002); 162(22): 2557-2562.
- Johnson LS, Juhlin T, Engström G, Nilsson PM. Low fasting plasma insulin is associated with atrial fibrillation in men from a cohort study-the Malmö preventive project. BMC Cardiovascular Disorders, (2014); 14(1): 107.
- Lobstein T, Jackson‐Leach R. Estimated burden of paediatric obesity and co‐morbidities in Europe. Part 2. Numbers of children with indicators of obesity‐related disease. International Journal of Pediatric Obesity, (2006); 1(1): 33-41.
- Fontes JD, Lyass A, Massaro JM, Rienstra M, Dallmeier D, et al. Insulin resistance and atrial fibrillation (from the Framingham Heart Study). The American journal of cardiology, (2012); 109(1): 87-90.
- Shigematsu Y, Norimatsu S, Ogimoto A, Ohtsuka T, Okayama H, et al. The influence of insulin resistance and obesity on left atrial size in Japanese hypertensive patients. Hypertension Research, (2009); 32(6): 500-504.
- Shigematsu Y, Hamada M, Nagai T, Nishimura K, Inoue K, et al. Risk for atrial fibrillation in patients with hypertrophic cardiomyopathy: association with insulin resistance. Journal of cardiology, (2011); 58(1): 18-25.

