

Full Length Research Article
Prevalence of hepatitis B and hepatitis C Virus infections among male to female (MFT) transgenders in Rawalpindi (Pakistan)
Hashaam Akhtar1,5*, Yasmeen Badshah1, Samar Akhtar2,5, Faheem Hasan3, Muhammad Faisal4, Najam us Sahar Sadaf Zaidi1, Ishtiaq Qadri6
Adv. life sci., vol. 5, no. 2, pp. 46-55, February 2018
*– Corresponding Author: Hashaam Akhtar (Email: hashaamakhtar@gmail.com)
Authors' Affiliations
2- Riphah Institute of Pharmaceutical Sciences, Riphah International University, Islamabad, Pakistan
3- Pir Mehr Ali Shah Arid Agriculture University Rawalpinid, Punjab, Pakistan
4- National Center for Bioinformatics, Quaid-i-Azam University, Islamabad , Pakistan
5-Yusra Institute of Pharmaceutical Sciences, Yusra Health and Education Foundation, Islamabad, Pakistan
6-King Fahd Medical Research Center, King Abdul Aziz University, Jeddah, Saudi Arabia
Abstract![]()
Introduction
Methods
Results
Discussion
References
Supplementary Data
Abstract
Background: Transgenders are the individuals, who due to certain psychological or physical requirement mismatch with their naturally received genders. Among transgender types, male to female (MTF) transgenders are highly prevalent in Indo-Pak and are feared to be at high risk for sexually transmitted viral (human immunodeficiency virus HIV, hepatitis B virus HBV, hepatitis C virus HCV and Epstein Barr virus EBV) and bacterial diseases (gonorrhea, syphilis, campylobacter, chancroid, shigella, granuloma inguinale and chlamydia). This sensitive issue, therefore, requires more attention of researchers, policy-makers, and non-governmental organizations (NGOs) in Pakistan.
Methods: Prevalence of HCV and HBV infection was studied in 306 transgender males with a median age of 29 years (range 15-64years) living in Rawalpindi, Pakistan. Molecular techniques such as ELISA and Nested PCR were performed to confirm the presence of the both viruses in each sample of subjects. Furthermore, logistic regression and chi-square test were used for statistical analysis.
Results: This study showed that occurrence of HCV infection was predominant among the studied group; whereas presence of HBV was insignificant and was not included for statistical analysis. PCR confirmed that 25.5% of the test group was HCV positive, with the highest percentage (83.33 %) of HCV positive among the individuals who claimed safe sex practices and had knowledge about the medical condition of their partners. 34.61% of the transgender men who shave outside their homes, were found to be HCV positive.
Conclusion: In light of these statistics, ignoring this threat could be dangerous not only for the transgender community but also for the society, in general.
Key words: HCV, HBV, Transgender, Pakistan, Unsafe sex
Introduction
Hepatitis B virus and Hepatitis C virus infections are threatening health problems with almost three to four hundred million carriers worldwide [1-3]. Sixty to eighty percent of the carriers progresses to chronic liver diseases [1-4]. Chronic infections caused by both of these viruses results in over 900,000 deaths annually and are the leading cause of hepatocellular carcinomas, fibrosis and liver cirrhosis [1,2,5].
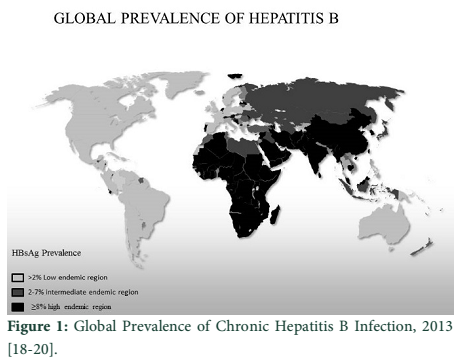
HBV is endemic in South Asia, affecting about 10% of the population [5]. According to WHO, the prevalence of HBV in Pakistan is around 3% and it falls in the low endemic zone of the world (Fig. 1) [6-8]. Even though a universal HBV vaccination program has been implemented, there is still a need for an efficient and individualized therapy regimen for chronic hepatitis B infection to prevent its progression into end-stage liver diseases and hepatocellular carcinomas. Similarly, one out of every twelve individuals is at a risk of hepatitis C and it is also a wide spread viral diseases across the globe (Fig. 2) [9].
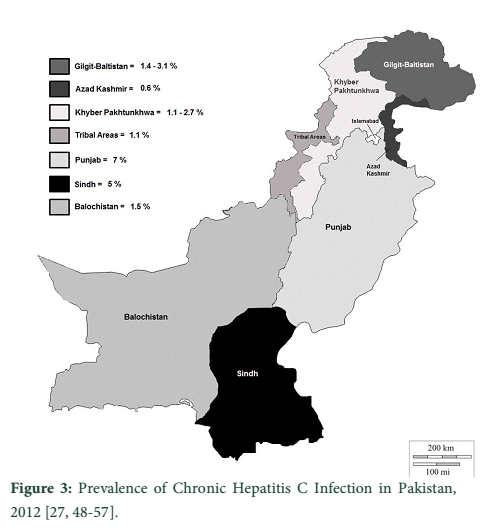
In some recent studies conducted in different cities of Pakistan, the prevalence of HCV was 6.5% in Hafizabad (Punjab) and 5.5% in Kech (Balochistan) (Fig. 3), whereas it has also been comparably found across the border with India [10-17]. Both HCV and HBV are blood-borne viruses that spread via contact with body fluids during unsafe sex practices, blood transfusions, child birth and sharing of blades or needles [21-23]. HBV/HCV co-infections are very common and are associated with life threatening complications like liver cirrhosis and hepatocellular carcinomas [24-27].
The aim of the present study is to draw a focus on HCV and HBV infections among transgender men in the city of Rawalpindi (Pakistan). Transgender is a broad term for individuals whose self-perceived gender identity is opposite to their biological gender. Transgenders are mostly under-privileged and constitute an economically and socially stigmatized class of our Indo-Pak society with a variety of gender identities such as: male to female, (MTF), female to male, (FTM) or just transvestites [34-41]. In Pakistani society MTFs or transgender men are known as Girya, Hijra, Chava, and Zanana [42-47]. Unemployment and social stigmas makes the MTFs become a part of the sex industry, thus, providing a cheaper alternative to other sex workers. Being under privileged, these MTFs are at a high risk of various infections, including skin diseases, malaria, diarrhea, tuberculosis and especially sexually transmitted diseases (STD) such as acquired immunodefiency syndrome (AIDS) and hepatitis [23,26].
Being transgender man in Indo-Pak society is a major social taboo which has been firmly discouraged by the majority resulting in their seclusion from the society [58]. Mostly these individuals spend their lives with their fellows and boss (guru) and drug dealing, sexual activities, dancing and begging are part of their livelihood [59-62]. Besides, they are also involved in selling unsafe sex due to lack of understanding of safe sex practices [63].” The main objective of this study is to find the relation of unsafe sexual activities practiced by MTFs due to lack of awareness or other business limitations with respect to the prevalence of sexually transmitted viral diseases (STVD) in this group of society. Customers of MTFs are mostly poor and illiterate, who seek for easy and cheap sex around their localities and according to a guru interviewed in this study, he said, “many of our customers run away if we ask them to use condom, because they then presume that there is something suspicious or we are having some disease. Many of us don’t even know about STDs other than AIDS’’.
Methods
A cross sectional study for prevalence of HBV and HCV infections was conducted among transgender men located in Rawalpindi (Pakistan) from November 2009 to June 2010 [64]. The sampling procedure and data collection was done in the same way as previously described [64] but some additional information and a brief summary of other parameters is described as follows:
Sex Partner Test
Subjects were inquired that whether they or their partners were ever diagnosed for STVDs and whether they used a condom last time they had sexual intercourse. The two response options were yes = 1, no = 0.
Shaving Habits
Subjects were inquired about their shaving habits such as whether they shave their body and face at home or they visit a barber shop. The response options were given numerical values as shaving at home is 1, shaving at a barber is 2 or for both is 3 [64].
Marital Status
This variable was measured by evaluating this question, ‘Are you married?’ and response has two options which were 1 for married and 0 for unmarried. Few of the subjects were married and had kids, which verified their bisexual activities [64].
Sexual Activity
Subjects were inquired about their normal sexual activities and the age of their first sexual experience and whether they ever have had anal intercourse (numerical criteria for answers: 1=yes, 0= no). Present study varies from already conducted studies related to STVD transmission, as the group understudy is always involved in homosexual activities [64].
Street Dentist
This variable was measured by evaluating the answers of the following questions; ‘Do you have any dental problem? Have you ever been to any dentist? Which dental hospital did you visit?’ As the use of paan and gutka among transgender men is very common, we found this variable to be an important determinant in exposing this mode of transmission of STVDs [65, 66]. The response options were yes = 1, no = 2 and we further divided yes into three categories; treatment from hospitals, treatment from street dentists (present on footpaths and mostly are without roofs) or no treatment [67, 68].
Education
The three grade levels were coded into a dummy variable (till 5th grade = 1, till 10th grade = 2, higher than 10th grade = 3) [64].
Blood Transfusion
This variable was measured by this question, ‘Have you ever undergone blood transfusion?’ and response options were same as previous criteria i.e. 1 for yes and 0 for no. Furthermore some of the responses were divided into donors or recipients of blood and their frequency was also recorded.
Sex Rate per Week
A variable was generated to measure the frequency of sex per week of the subjects under study and response was categorized as less than or equal to 20 and more than 20.
Sample Collection/Preparation
To study the the prevalence of HCV and HBV infection among 306 transgender men in the city of Rawalpindi (Pakistan). For molecular analysis, 15ml venous blood from each subject was collected and stored into EDTA anti-coagulating tubes. 1.5ml of the collected blood was centrifuged at 2400 rpm for 10 minutes which separated the serum from whole blood. Sera of all subjects were used for immunochromatographic method (Accurate, one step HBsAg Devices) to screen HBsAg and HCV-Ab in blood samples. Samples with positive antigen or antibody were further validated by PCR.HBV and HCV testing was carried out anonymously, however all of the subjects obtained their reports of the survey data only with lab serial numbers.
Detection of HBV-DNA by Nested PCR
HBV DNA was extracted from serum using the QIAamp Viral DNA kit (QIAGEN Inc., Hilden, Germany) and subjected to Polymerase chain reaction (PCR) by using Esco (96 well thermocycler). Twenty five cycles of DNA amplification were performed. The first round PCR was performed using sense and antisense primers followed by second round PCR (nested PCR), using the first round product with inner sense and antisense primers. PCRs were carried out using PCR Master Mix (Promega, Cat. # M7502) for 25 cycles. Nested PCR products (10 µl) were analyzed by electrophoresis on 2% agarose gels and visualized under UV fluorescence.
Detection of HCV-RNA by Nested PCR
HCV RNA was extracted from serum using the Roboscreen kit (Germany) and subjected to Polymerase chain reaction (PCR). Viral RNA was taken to reverse transcribe the 5’ NCR of HCV using Moloney murine leukemia virus reverse transcriptase (M-MLV RTase, Fermentas) in a total reaction volume of 20 µl. The reaction mixture contained 4 µl MMLV (5X) buffer, 1 µl M-MLV reverse transciptase (RT) enzyme, 1 µl dNTPs (10mM), 0.13 µl RNase inhibiter (Fermentas), 1.5 µl RNase free water, 1 µl specific anti-sense primer and 10 µl template (viral RNA). cDNA was synthesized using thermocycler. Cycle conditions for cDNA were as follows: 37°C for 55 minutes followed by 95°C for 5 minutes. cDNA product was used for qualitative analysis of HCV infection. The first round PCR was performed using sense and antisense primers followed by second round PCR (nested PCR), using the first round product with inner sense and antisense primers. PCRs were carried out using PCR Master Mix (Promega, Cat.# M7502) for 25 cycles. Finally, 10 µl of the second round PCR product was electrophoresed on 2% agarose gel. Specific bands of HCV detections were visualized under UV light.
Inclusion Criteria
All transgender men- hijras were included [64].
Exclusion Criteria
Female sex workers, FTMs (Female to Male), transgender females, gender queer and drag queen/kings were excluded from this study [64].
Results
Data Analysis
Investigation of statistically significant links between shaving, education, heterosexuality, number of sex partners per week and prevalence of HCV are described in this article. The data analysis was performed by means of SPSS (16.0 version) for Windows XP [69]. Detailed analyses were conducted by calculating the frequency distribution of HCV and HBV infections (prevalence of HBV infection is very low, as assumed because of its vaccination, so it is not shown in comparison with different parameters used with in the study) among transgender men in association with the eight parameters described previously. Multiple logistic regression model was applied to illustrate the association between the prevalence of HCV (HBV data not shown in results) among transgender men and its dependence on some other factors correlated to them. Seven predictor variables were considered for this purpose.
- Age of the respondent (transgender)
- Sex frequency in a week\ number of partners per week
- Education of transgender men
- Marital status or heterosexuality
- Body shaving behavior
- Blood transfusion history
- Dental problems and visits to street dentists
First two variables; Age and Sex frequency in a week were classified into categorical variables because the frequency of sex was showing a relation with the age, as it was higher among young age groups. Asking for safe sex habits of sex partner, visit to street dentists, heterosexuality behavior or marital status and blood transfusion history were split into binary variables; 0 and 1 [0= No and 1= yes]. Education of transgender men and shaving behavior were split into binary variables, as they were categorical variables; if a variable has 4 categories then it was transformed in 4-1 binary variables e.g. shave variable has 3 categories; shave at home, from barber and both so it was split into two binary variables i.e. home and barber. Frequency of sex partners per week was divided into 3 categories based upon number of sex partners per week ranging from one to twenty, more than twenty up to forty and more than forty as 1, 2 and 3 respectively. Hence the 3rd function cannot be introduced since an intercept is present in the model so the last category in each variable was a reference category. Hierarchical technique was used to select the model. Associations of these variables for HCV are performed by the Chi-Square test, as summarized in Table 1 (supplementary data).
Overall the prevalence of HCV was found to be 25.5% in a total of 306 transgender men. The highest percentage was found to be 83.33 % among those, who claimed to have knowledge about the safe sex habits of their partners (Fig. 4 in supplementary data). Statistical analysis shows that 34.61% of the individuals who went to barbers were infected with HCV against 28.08% of those who shaved at home (Fig. 5 in supplementary data). Body shaving was found to be common among this class of sex workers and they frequently share razors due to lack of awareness and shortage of assets (Fig. 5 in supplementary data). 90 out of 306 transgender men were found to have had blood transfusions and 19 out of these 90 were found to be HCV positive (Fig. 6 in supplementary data). 85 out of 306 transgender men included in this study had some dental problems and visited at least once in the past 3 months the nearest street dentist. 28 out of these 85 had HCV and it seems that the other patients of those street clinics are in jeopardy, as the sterilization facilities of these clinics are not satisfactory (Fig. 7 in supplementary data). Two categories were defined to measure the prevalence of HCV with respect to the number of sexual partners per week; first one was with less then and equal to twenty different partners and the second one was with greater than twenty sexual partners per week. 34 out of 101 (33.66%) subjects with a high number of sexual partners per week were found to be HCV positive, as compared to 44 out of 205 (21.46%) subjects, who had fewer sexual partners per week. (Fig. 8 in supplementary data). Prevalence of HCV among homo and bisexual transgender men was found to be 28.4 % and 12.5 % respectively. Transgender men involved in horizontal transmission of STVDs can further spread these diseases to opposite genders, as few of the married transgender men were fathers of kids too. Vertical transmission of STVDs through female sex partners of heterosexual transgender men can also be a risk in raising the prevalence of HCV (Fig. 9 in supplementary data). Awareness comes through education and results shows the same as the educational background had a significant association (p-value = 0.012), likewise the prevalence of HCV dropped dramatically (i.e. 9.52% for transgender men, educated above 10th standard). However, education was found to be insignificant in the logistic regression model (Table 2 in supplementary data) (Fig. 10 in supplementary data).
Multivariate Analysis
Multiple logistic regression model was used to illustrate the relationship between the transmission of HCV among transgender men and its connection with related factors. The following five predictors were found to be important for this purpose (see Table 2).
- Asking for safe sex habits of the sex partner
- Body shaving behavior
- History of blood transfusion
- Visits to street dentists
- Number of sex partners per week
The relative odds with respect to their daily routine activities and behaviors are shown in table 2. During interviews, we observed that the level of education was linked with the knowledge about different diseases and their modes of transmissions. However, educational background of transgender men was insignificant by stepwise variable selection method in this Logistic regression equation (in supplementary data).
The analysis shows that all the predictors have significant predicting power i.e. the question asked about the knowledge related to the safe sex habits of their sec partners has shown highly significance in the studied group. Respondents were categorized into three groups according to their shaving behavior, i.e. shave at home, shave from barber shop, or both. The third category was used as a reference in this model. Results showed that the odds for shaving from barber were two times greater than the other group, whereas shaving at home was also quite high and reached almost two and half times more. The odds for having HCV in transgender men were two times higher when they were involved in blood transfusions. Visits to street dentists also increased the odds up to one time, as compared to the transgender men visiting a proper dental hospital. In addition to this, the odds were one and a half times higher, if the transgender men had more than 20 partners per week.
Tables & Figures

Discussion
Pakistan is a developing country with much trepidation like economic strains, illiteracy, poverty, social and ethical issues and much more. One out of these apprehensions is health related issues, which includes STDs and STVDs. Pakistan lacks proper data on the prevalence of HBV and HCV infections and particularly co-infections among sex workers of the transgender societies. Transgender men are one of the stigmatized and under privileged groups of Indo-Pak community with a lot of social, ethical and cultural issues at the national level. Illiteracy and lack of awareness leads them to poverty and a number of other factors add to their seclusion from society [58,59].
One out of many reasons behinds the swift spread of viral diseases in transgender populations can be the lack of attention paid by the government or discrimination in the private and public health related sectors. Unemployment and the economic strains of society have dragged many of them towards prostitution as source of employment [70,71]. Client based sex, unprotected anal sex, survival hurdles, physical abuse and drug abuse adds a lot in the increasing prevalence of these STDs and STVDs amongst these groups [72,73]. The present study focuses on the behavioral patterns of transgender men with reference to the prevalence of HBV and HCV among this group. A group of 306 transgender men were questioned about their weekly sexual activities and their answers were confirmed by their gurus (boss), who were also part of this business. Results showed that HCV (25.5%) is more prevalent than HBV (2.941%) amongst the studied group, whereas, the prevalence of HCV in Pakistan is believed to be much lower than this [72]. The highest percentage was found to be 83.33% among those, who claimed to have knowledge about the safe sex habits of their sex partners (Fig. 4 in supplementary data).
Young respondents included in the study were mostly dancers and paid much attention to their appearance because they had to earn money through their personal presentations, but due to their good body maintenance, they are also more involved in the sex selling business. Results showed that, 12 out of 306 transgender men claimed to have sex with customers, whom they know very well including their health related issues. 10 out of those 12 were found to be HCV positive (83.33%), whereas the prevalence of HCV among the repudiating group of 294 transgender men was 23.13%. This might be interesting because either they are harmless for the society or they told untruth stories.
As education means knowledge or awareness towards many aspects of life, health care is also somehow related to this parameter. Results showed that transgender men, who only had the most basic education, i.e. they didn’t even cleared their primary education, had a higher risk of being infected with HCV, as compared to those, who cleared their 10th grade. Educated transgender men were found to be more vigilant about avoiding unprotected sex and had lower prevalence of HCV i.e. about 9.82% as compared to 22.58% and 30.99% among subjects who were less educated below 10th and 5th standards respectively. Juvenile school drop outs or lack of education may end into unsafe sexual activities, as the data shows a high prevalence of HCV in that class. Lower literacy rate and lack of awareness were found to have a direct relation with the prevalence of HCV and HBV in transgender community.
The analysis highlighted bisexuality as another important factor involved in dispersion of STVDs, as 18.3 % of the respondents involved in this study were married and were involved in both hetero- or homo- sexual activities. Results showed that unmarried\homosexuals had a high prevalence of HCV (28.4%) as compared with married\heterosexuals (12.5%). Few married respondents do have kids, so had to give time to their married lives, which somehow implicated more responsibilities on them and they had a reduced sexual activities. Transgender males have many shaving behaviors and patterns. They were categorized into two groups i.e. those who shave at home and those who shave at barbers. Home shaving included razors, threading and clipping through tweezers or a pair of scissors. Subjects who shaved at barber’s shop had a high prevalence of HCV (34.61%) in contrast to those who shaved at home (28.08%). Thus sterility at low budget barbers shop can be questioned because they may reuse the same instruments without sterilizing them or reuse sterilizing liquids for many days. Another key factor at low budget barber shop can be the use of potash alum, which is still used for facial cuts and thus comes in contact with the blood of many [74]. Transgender men living in clans also stated that they in routine share scissors and razors for body shaving. Sharing of blades due to lack of resources can be a vital factor in the dispersal of HCV at home.
Number of sex partners per week was found to be a significant factor after analysis. Transgender men with twenty plus sex partners per week had a very high prevalence of HCV (33.66%) as compared with those, who had few sex partners per week (21.46%). Sexual contact is the key factor in transmission of STVDs and our results showed the same. Spread of HCV through unsterilized dentistry equipment is also an important parameter and was included in the study, because the transgender community of Pakistan frequently use cheap brain stimulants or mouth fresheners like areca nut/supari, gutka and pan (with or without tobacco) [75].
The use of these products leads to many dental and buccal problems, including tumors [75]. Dental problems lead those to dental clinics and due to a lack of resources, they visit low budget dental clinic or even street dentists, which are without proper hygiene practices. Unsatisfactory sterilization of dental instruments is quite common in these clinics, which leads to increase the risk of STVD spread. Visits to street dentists were found to be an important parameter in this case too and the prevalence of HCV was 10.32 % higher in the group, which claimed to visit street dentist quite often. Transgender men belong to an economically stigmatized community of our society who cannot afford to visit health care facilities. Poverty, unemployment and economic stress answer the fact that they cannot afford professional dentists. 85 transgender men claimed to visit street dentists and 28 out of them were diagnosed as HCV positive.
Blood transfusion is a sensitive issue with respect to the spread of STVDs, but still many of the respondents had a history of blood transfusion. Blood transfusion was not very common in this community, as those who answered ‘yes’ had hardly undergone this process thrice within the last 5 years. Though there was a contrasting trend observed in the analysis, with the decreased rate of prevalence in transgender men who had undergone blood transfusion (21.11%) against those who had never undergone this process in the last 5 years (27.32%). This study do depicts a fact that few parameters like history of blood transfusion and visits to street dentist may have a significant role in the propagation of HCV so an extensive research should be conducted to increase our knowledge towards these concealed issues in this community.
Alcoholism, prostitution, promiscuity and drugs are widespread among dancers in the transgender community. Injectable drug users (IDUs) add a lot to the prevalence of STVDs besides sexual contact, however, this case study showed a negligible number of IDUs in the transgender community thereby eliminating this risk factor. Use of condom was added as the factor to study the significance of HCV and HBV spread in the community but it could not be strongly related in the analysis, as a negligible number of respondents claimed to use it regularly. According to the respondents, the reason behind not using condoms regularly was due to an apprehension on the customer’s part.
Domestic violence, unemployment, lack of awareness, poverty, ethical issues, rape, early age sexual activities and illiteracy are some of the factors believed to be contributing to the isolation of transgender community. This study evidently characterizes some problems of this community and further highlight the social stigmas of cultural and religious origin in Pakistan, furthermore, enlightening the need towards STVDs prevention in ignorant transgender communities. The health care department needs to be more concerned about the conditions and living environment of the transgender communities and should implicate regular free check-ups. They should be given rights to live their life as normal citizens of a country.
Pakistan has a rising prevalence of HCV and HBV infections. This study stresses the importance of health care among minority groups in Pakistan. A number of issues concerning STVDs control was highlighted i.e. illiteracy, ignorance and background status leads to this unusual behavior. Transgender men are a secluded class within society with no proper rights, such as access to the basic life necessities, health care facilities, quality education or employment and are constantly felling depressed and never looked upon as normal citizens of our society. Education, awareness and health care services should be provided to this community.
The statistical analysis of the above mentioned parameters: age, education, knowledge about sex partners, number of sex partners per week, blood transfusion, shaving behavior, street dentist and marital status showed that they all contribute to the high prevalence of hepatitis C in the transgender community. The overall prevalence of HCV was 25.5% among the total 306 transgender subjects in study.
Implications of the Study
The findings and conclusions of this study have implications for health care practitioners, NGO’s and health educators trying to better understand the rate of prostitution and risk behaviors among transgender men in Rawalpindi and perhaps other cities of Indo-Pak. The prevalence of HCV, the sexual behavior and the use of condom among transgender men in the current study suggests that current educational efforts, awareness programs and strategies are inadequate. The conclusion of this study suggests that transgender men should be provided with proper medical facilities and treatments after screening.
Declared Ethical Approval
All the samples were collected, with the approval of the Institutional Review Board, Atta-ur-Rahman School of Applied Biosciences, National University of Sciences and Technology (NUST), Islamabad, Pakistan. The candidates who gave permission were informed about the tests to be conducted from that blood samples and the interviews were conducted in front of the Guru (chief or supervisor) of that community.
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
- Shepard CW, Finelli L, Alter MJ. Global epidemiology of hepatitis C virus infection. Lancet Infectious Diseases, (2005); 5(9): 558-567.
- Bowen DG, Walker CM. The origin of quasispecies: cause or consequence of chronic hepatitis C viral infection? Journal of Hepatology, (2005); 42(3): 408-417.
- Lauer GM, Walker BD. Hepatitis C virus infection. New England Journal of Medicine, (2001); 345(1): 41-52.
- Kao JH, Chen PJ, Lai MY, Chen DS. Occult hepatitis B virus infection and clinical outcomes of patients with chronic hepatitis C. Journal of Clinical Microbiology, (2002); 40(11): 4068-4071.
- Purow DB, Jacobson IM. Slowing the progression of chronic hepatitis B. Early antiviral therapy can help minimize complications. Postgraduate Medicine, (2003); 114(1): 65-68, 73-66.
- Baig S, Siddiqui AA, Ahmed W, Qureshi H, Arif A. The association of complex liver disorders with HBV genotypes prevalent in Pakistan. Virology Journal, (2007); 4: 128.
- Khichi GQK CM. Prevalence of hepatitis B carriers among children in Bahawalpur urban slums. Pakistan Journal of Medical Sciences, (2000); 16(4): 238-241.
- Khattak MF, Salamat N, Bhatti FA, Qureshi TZ. Seroprevalence of hepatitis B, C and HIV in blood donors in northern Pakistan. Journal of Pakistan Medical Association, (2002); 52(9): 398-402.
- Nwokediuko S. Seroprevalence of Hepatitis C virus antibody in public servants of Enugu state of Nigeria. Journal of College of Medicine, (2010); 15(1): 40-43.
- Ali NS, Jamal K, Qureshi R. Hepatitis B vaccination status and identification of risk factors for hepatitis B in health care workers. Journal of the College of Physicians and Surgeons Pakistan, (2005); 15(5): 257-260.
- Luby SP, Qamruddin K, Shah AA, Omair A, Pahsa O, et al. The relationship between therapeutic injections and high prevalence of hepatitis C infection in Hafizabad, Pakistan. Epidemiology Infections, (1997); 119(3): 349-356.
- Aziz H, Raza A, Murtaza S, Waheed Y, Khalid A, et al. Molecular epidemiology of hepatitis C virus genotypes in different geographical regions of Punjab Province in Pakistan and a phylogenetic analysis. International Journal of Infectious Diseases, (2013); 17(4): e247-253.
- Ahmed F, Irving WL, Anwar M, Myles P, Neal KR. Prevalence and risk factors for hepatitis C virus infection in Kech District, Balochistan, Pakistan: most infections remain unexplained. A cross-sectional study. Epidemiology Infections, (2012); 140(4): 716-723.
- Basu D, Kumar V, Sharma AK, Barnwal PK, Mattoo SK. Seroprevalence of anti-hepatitis C virus (anti-HCV) antibody and HCV-related risk in injecting drug users in northern India: comparison with non-injecting drug users. Asian Journal of Psychiatry, (2013); 6(1): 52-55.
- Sood A, Sarin SK, Midha V, Hissar S, Sood N, et al. Prevalence of hepatitis C virus in a selected geographical area of northern India: a population based survey. Indian Journal of Gastroenterology, (2012); 31(5): 232-236.
- Sarma MP, Asim M, Medhi S, Bharathi T, Kar P. Hepatitis C virus related hepatocellular carcinoma: a case control study from Indian Journal of Medical Virology, (2012); 84(7): 1009-1017.
- Sood A, Midha V, Bansal M, Sood N, Puri S, et al. Perinatal transmission of hepatitis C virus in northern India. Indian Journal of Gastroenterology, (2012); 31(1): 27-29.
- Ott JJ, Stevens GA, Groeger J, Wiersma ST. Global epidemiology of hepatitis B virus infection: new estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine, (2012); 30(12): 2212-2219.
- Firnhaber C, Chen CY, Evans D, Maskew M, Schulz D, et al. Prevalence of hepatitis B virus (HBV) co-infection in HBV serologically-negative South African HIV patients and retrospective evaluation of the clinical course of mono- and co-infection. International Journal of Infectious Diseases, (2012); 16(4): e268-272.
- Khuwaja AK, Qureshi R, Fatmi Z. Knowledge about hepatitis B and C among patients attending family medicine clinics in Karachi. Eastern Mediterranean Health Journal, (2002); 8(6): 787-793.
- Kane A, Lloyd J, Zaffran M, Simonsen L, Kane M. Transmission of hepatitis B, hepatitis C and human immunodeficiency viruses through unsafe injections in the developing world: model-based regional estimates. Bull World Health Organ, (1999); 77(10): 801-807.
- Alberti A, Pontisso P, Chemello L, Fattovich G, Benvegnu L, et al. The interaction between hepatitis B virus and hepatitis C virus in acute and chronic liver disease. Journal of Hepatology, (1995); 22(1 Suppl): 38-41.
- Rajabali A, Khan S, Warraich HJ, Khanani MR, Ali SH. HIV and homosexuality in Pakistan. Lancet Infectious Diseases, (2008); 8(8): 511-515.
- Raimondo G, Saitta C. Treatment of the hepatitis B virus and hepatitis C virus co-infection: still a challenge for the hepatologist. Journal of Hepatology, (2008); 49(5): 677-679.
- Lehman EM, Wilson ML. Epidemic hepatitis C virus infection in Egypt: estimates of past incidence and future morbidity and mortality. Journal of Viral Hepatitis, (2009); 16(9): 650-658.
- Khan S, Rai MA, Khanani MR, Khan MN, Ali SH. HIV-1 subtype A infection in a community of intravenous drug users in Pakistan. BMC Infectious Diseases, (2006); 6164.
- Naeem MA WUZT, Usman M and Sabeen K. Seroprevalence And Demography Of Hepatitis B And C Among Healthy Young Males Of Northern Areas Of Pakistan. International journal of pathology, (2008); 1(1).
- Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: New estimates of age-specific antibody to HCV seroprevalence. Hepatology, (2013); 57(4): 1333-1342.
- Sievert W, Altraif I, Razavi HA, Abdo A, Ahmed EA, et al. A systematic review of hepatitis C virus epidemiology in Asia, Australia and Egypt. Liver International, (2011); 31 Suppl 261-80.
- Nguyen LH, Nguyen MH. Systematic review: Asian patients with chronic hepatitis C infection. Alimentary Pharmacology & Therapeutics, (2013).
- Randriamanantany ZA, Rajaonatahina DH, Razafimanantsoa FE, Rasamindrakotroka MT, Andriamahenina R, et al. Prevalence and trends of hepatitis C virus among blood donors in Antananarivo, from 2003 to 2009. Transfusion Clinical Biology, (2012); 19(2): 52-56.
- Gutierrez Domingo I, Pascasio Acevedo JM, Alcalde Vargas A, Ramos Cuadra A, Ferrer Rios MT, et al. Prevalence of hepatitis B and A virus markers and vaccination indication in cirrhotic patients evaluated for liver transplantation in Spain. Transplantation Proceedings, (2012); 44(6): 1502-1504.
- Morris MD, Shiboski S, Bruneau J, Hahn JA, Hellard M, et al. Geographic Differences in Temporal Incidence Trends of Hepatitis C Virus Infection Among People Who Inject Drugs: The InC3 Collaboration. Clinical Infectious Diseases, (2017); 64(7): 860-869.
- Pinto RM, Melendez RM, Spector AY. Male-to-Female Transgender Individuals Building Social Support and Capital From Within a Gender-Focused Network. Journal of Gay & Lesbian Society Services, (2008); 20(3): 203-220.
- Ramirez-Valles J, Garcia D, Campbell RT, Diaz RM, Heckathorn DD. HIV infection, sexual risk behavior, and substance use among Latino gay and bisexual men and transgender persons. American Journal of Public Health, (2008); 98(6): 1036-1042.
- Mayer KH, Bradford JB, Makadon HJ, Stall R, Goldhammer H, et al. Sexual and gender minority health: what we know and what needs to be done. American Journal of Public Health, (2008); 98(6): 989-995.
- Herbst JH, Jacobs ED, Finlayson TJ, McKleroy VS, Neumann MS, et al. Estimating HIV prevalence and risk behaviors of transgender persons in the United States: a systematic review. AIDS Behaviour, (2008); 12(1): 1-17.
- Chakrapani V, Newman PA, Shunmugam M, Dubrow R. Barriers to free antiretroviral treatment access among kothi-identified men who have sex with men and aravanis (transgender women) in Chennai, India. AIDS Care, (2011); 23(12): 1687-1694.
- Sahastrabuddhe S, Gupta A, Stuart E, Godbole S, Ghate M, et al. Sexually transmitted infections and risk behaviors among transgender persons (Hijras) of Pune, India. Journal of Acquired Immune Deficiency Syndrome, (2012); 59(1): 72-78.
- Gupte S, Daly C, Agarwal V, Gaikwad SB, George B. Introduction of rapid tests for large-scale syphilis screening among female, male, and transgender sex workers in Mumbai, Indian Journal of Sexually Transmitted Diseases (2011); 38(6): 499-502.
- Raj A, Saggurti N, Cheng DM, Dasgupta A, Bridden C, et al. Transactional sex risk and STI among HIV-infected female sex workers and HIV-infected male clients of FSWs in India. AIDS Care, (2011); 23(11): 1374-1381.
- Lipovsek V, Mukherjee A, Navin D, Marjara P, Sharma A, et al. Increases in self-reported consistent condom use among male clients of female sex workers following exposure to an integrated behaviour change programme in four states in southern India. Sexually Transmitted Infections, (2010); 86 Suppl 1i25-32.
- Bakshi S. A comparative analysis of hijras and drag queens: the subversive possibilities and limits of parading effeminacy and negotiating masculinity. Journal of Homosexuality, (2004); 46(3-4): 211-223.
- Hawkes S, Collumbien M, Platt L, Lalji N, Rizvi N, et al. HIV and other sexually transmitted infections among men, transgenders and women selling sex in two cities in Pakistan: a cross-sectional prevalence survey. Sexually Transmitted Infections, (2009); 85 Suppl 2ii8-16.
- Platt L, Vickerman P, Collumbien M, Hasan S, Lalji N, et al. Prevalence of HIV, HCV and sexually transmitted infections among injecting drug users in Rawalpindi and Abbottabad, Pakistan: evidence for an emerging injection-related HIV epidemic. Sexually Transmitted Infections, (2009); 85 Suppl 2ii17-22.
- Khan S KT (2002) Pakistan enhanced HIV/AIDS program: social assessment and mapping of men who have sex with men (MSM) in Lahore, Pakistan. In: International NF, editor. 1 ed. London. pp. 31.
- Phillips AE, Molitor J, Boily MC, Lowndes CM, Gurav K, et al. Informal confidential voting interviewing in a sexual risk assessment of men who have sex with men (MSM) and transgenders (hijra) in Bangalore, India. Sexually Transmitted Infections, (2013); 89(3): 245-50.
- Rizwan Hashim ABH, Khalil ur Rehman. Seroprevalence of Hepatitis-C Virus Antibodies Among Healthy Young Men in Pakistan. Pakistan Journal of Medical Research, (2005); 44(4): 140-142.
- Afridi SQ, Zahid MN, Shabbir MZ, Hussain Z, Mukhtar N, et al. Prevalence of HCV genotypes in district Mardan. Virology Journal, (2013); 10(1): 90.
- Lavanchy D. The global burden of hepatitis C. Liver International, (2009); 29 Suppl 174-81.
- Idrees M, Riazuddin S. Frequency distribution of hepatitis C virus genotypes in different geographical regions of Pakistan and their possible routes of transmission. BMC Infectious Diseases, (2008); 8: 69.
- Tariq WU, Hussain AB, Karamat KA, Ghani E, Hussain T, et al. Demographic aspects of hepatitis C in northern Pakistan. Journal of Pakistan Medical Association, (1999); 49(8): 198-201.
- Khan AJ, Luby SP, Fikree F, Karim A, Obaid S, et al. Unsafe injections and the transmission of hepatitis B and C in a periurban community in Pakistan. Bulletin World Health Organization, (2000); 78(8): 956-963.
- Butt G, Paterson BL, McGuinness LK. Living with the stigma of hepatitis C. Western Journal of Nursing Research, (2008); 30(2): 204-221.
- Muhammad Umar MB. Hepatitis C, A Mega Menace: A Pakistani Perspective. Journal of poineering medical sciences, (2012); 2(2): 68-72.
- Chaudhary IAS, Khan SS, Masood R, Sardar MA, Mallhi AA. Seroprevalence of Hepatitis B and C among the healthy blood donors at Fauji Foundation Hospital, Rawalpindi. Pak J Med Sci (2007); 23(1): 64-67.
- (2010) Hepatitis control plan entering second phase. The Express Tribune. 23rd October ed. Pakistan.
- Collumbien M, Qureshi AA, Mayhew SH, Rizvi N, Rabbani A, et al. Understanding the context of male and transgender sex work using peer ethnography. Sexually Transmitted Infections, (2009); 85 Suppl 2ii3-7.
- Zaheer HA, Hawkes S, Buse K, O'Dwyer M. STIs and HIV in Pakistan: from analysis to action. Sexually Transmitted Infections, (2009); 85 Suppl 2ii1-2.
- Mayhew S, Collumbien M, Qureshi A, Platt L, Rafiq N, et al. Protecting the unprotected: mixed-method research on drug use, sex work and rights in Pakistan's fight against HIV/AIDS. Sexually Transmitted Infections, (2009); 85 Suppl 2ii31-36.
- Baqi S, Shah SA, Baig MA, Mujeeb SA, Memon A. Seroprevalence of HIV, HBV, and syphilis and associated risk behaviours in male transvestites (Hijras) in Karachi, Pakistan. International Journal of STD & AIDS, (1999); 10(5): 300-304.
- Lubis I, Master J, Munif A, Iskandar N, Bambang M, et al. Second report of AIDS related attitudes and sexual practices of the Jakarta Waria (male transvestites) in 1995. Southeast Asian Journal of Tropical Medicine and Public Health, (1997); 28(3): 525-529.
- Jenkins C (2004) Male Sexuality, Diversity and Culture: Implications for HIV prevention and care, Geneva. USA: UNAIDS.
- Akhtar H, Badshah Y, Akhtar S, Kanwal N, Akhtar MN, et al. Prevalence of human immunodeficiency virus infection among transgender men in Rawalpindi (Pakistan). Virology Journal, (2012); 9229.
- Banerjee SC, Ostroff JS, Bari S, D'Agostino TA, Khera M, et al. Gutka and Tambaku Paan Use Among South Asian Immigrants: A Focus Group Study. Journal of Immigrant and Minority Health, (2014); 16: 531-539.
- Changrani J, Gany F. Paan and Gutka in the United States: an emerging threat. Journal of Immigrant and Minority Health, (2005); 7(2): 103-108.
- Ahmad W, Ijaz B, Javed FT, Jahan S, Shahid I, et al. HCV genotype distribution and possible transmission risks in Lahore, Pakistan. World Journal of Gastroenterology, (2010); 16(34): 4321-4328.
- Hyder Q, Burhan-ul-Haq M, Rashid R, Qazi S, Mehmood S, et al. Non-conventional transmission of hepatitis C: a true possibility ignored. Journal of Pakistan Medical Association, (2009); 59(7): 430-433.
- ( 2008) SPSS 16.0 for Windows. SPSS Inc. Chicago.
- Clements-Nolle K, Guzman R, Harris SG. Sex trade in a male-to-female transgender population: psychosocial correlates of inconsistent condom use. Sex Health, (2008); 5(1): 49-54.
- Lemon SM. Current status of antiviral therapy for chronic hepatitis C. Advances in Experimental Medicine and Biology, (1999); 45: 829-37.
- Laxmi T GS, Payal K, Revati, Priya B, Jeeva R, Amitava S, Agniva L, Anindya H, Laxmi Bai, Pramod, Simran S, Abhina A, Rajan K, Sanjeev J, Mridu M, Govind B, J K Mishra, Ernest N (2011) Transgender – Hijra strategy. India: NACO, NACP IV working groups Hijras TG. pp. 1-16.
- Perappadan BS (2012) Erasing the stigma of HIV.
- Waheed Y, Safi SZ, Qadri I. Role of Potash Alum in hepatitis C virus transmission at barber's shop. Virology Journal, (2011); 8: 211.
- THE DENTAL PANORAMA (2011). Smilekraft. India: Dental Clinic & Dental Hospital Chain, Delhi, Bangalore, Hyderabad, India.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0/