

Review Article
Dry sockets – a systemic review
Bassam Mohammad Almutairi
Adv. life sci., vol. 7, no. 1, pp. 48-57, November 2019
Corresponding Author: Bassam Mohammad Almutairi (Email: Bassam.alhumaiani@gmail.com)
Author's Affiliation
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
This is a systematic review, which shows a compendious review about the aetiology, prevention and treatment of Alveolar Osteitis. After tooth extraction the most common postoperative complication is dry socket. In oral surgery it is very essential to know about the pathophysiology aetiology, prevention and treatment of dry socket. The main purpose of this review article is to provide enough knowledge about the processes that are involved in the clinical management of dry socket. This article shows certain risk factors involved in the incidence of dry socket. surgical trauma, lack of operator experience, mandibular third molars, oral contraceptives, menstrual cycles, smoking, bacterial infections, excessive irrigation, age, bone fragments, local anaesthetics, we will discuss all of these factors which are involved in the incidence of alveolar osteitis in this article. Furthermore, some prevention methods have also been discovered which can be applied to prevent from the incidence of dry socket. Certain treatment methods have also been identified and the have played the vital role in treating the dry socket disease, this article also shows the relation between the Fibrinolysis and the occurrence of dry socket. Various treatment methods, which involve the use of antibiotics, chlorhexidine (as preventive measure also), steroids, anti-fibrinolytics, low-level laser therapy, have been identified which play a vital role in the treatment of dry socket disease.
Keywords: Dry Socket; Joints; Anti-fibrinolytics; Review; Chlorhexidine
Introduction![]()
The most common complication of tooth extraction is dry socket and is characterized by a severe type of pain usually starting due to the extraction of tooth [1] after two or three days [2]. It has been reported that prevalence of dry socket varies from 0% to more than 35.5% [3] occurs following mandibular third molar extraction commonly. Patients subjected to this disease, experience certain conditions like loss of functioning and severe pain. An aquatic blood clot starts to accumulate in the extraction site after the removal that will reveal the alveolar bone with a dry mien [4], due to this dry appearance it is known as dry socket. Pathogenesis of dry socket is not only confined to one single method, involves various pathogenesis procedures. Several factors which are contributing to an increased risk of dry socket have been reported to be in association with is direct increase. Please clarify or simplify the previous sentences factors which are directly involved in increasing the risk [5] of dry socket involves site of extraction, pre-operative infections, local anaesthetics used with vasoconstrictors, sex, traumatic extraction, low level of operator experience and inadequate post-operative irrigation. It is better to categorize them in order, biological, physiological, then psychological and social, follow this pattern in the literature about aetiology.
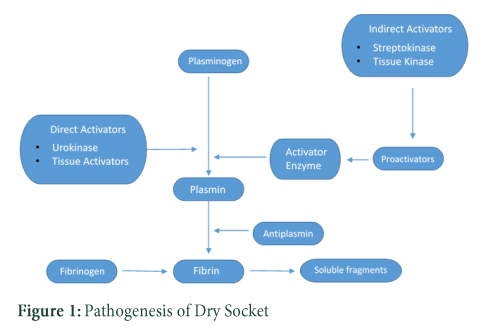
In the past, several other methods for the detection in the incidence of dry socket were advocated, these methods involve antiseptic mouthwashes, antibiotics, steroids, antifibrinolytic agents [6], intra alveolar dressings, intra alveolar medicaments and clot supporting agents. The observations have shown that fibrinolytic activity is one of the main etiological factor in the development [7] of dry socket. There can be premature loss of intra alveolar blood clot, after extraction, caused by an increase in fibrinolytic activity [8]. Fibrinolysis results due to the activation of plasminogen pathway [9] which can be attained by both physiologically (directly) and non-physiologically (indirectly) activated substances [10]. After trauma to the alveolar bone cells direct activators are released while bacteria releases indirect activators. In spite of its vital role in fibrinolytic processes, the exact etiology of dry socket is unknown yet.
Methods![]()
Literature search and selection criteria
The main journal publishers e.g. Wiley online libraries, Elsevier, PubMed were searched with the key words like dry socket, joint, anti-fibrinolytics, review, chlorhexidine and the articles matching above 70% to the key words were included to write this review.
Discussion![]()
Aetiology
Aetiology of dry socket has been presented by several theories. Trauma, bacterial infection and biochemical agents [11] are the main components of these theories. Dry socket is a condition [12] in which there is elevation in the activation of plasminogen and fibrinolytic activity to plasma in the presence of tissue activators [13]. Post extraction blood clot integrity may be affected by fibrinolytic activity according to, need reference. Fibrinogen and thrombin in a normal post extraction socket combine [14] together and form a fabric clot and this clot helps epithelium to migrate. After this, there is a formation of new blood vessels in the clot during the granulation tissue formation [15] and along with this, the degradation [16] starts with the help of plasma by the activity of fibrinolysis and fibroblasts before the osteoproliferation [17] phenomena initiates.
Studies have shown that in dry socket, the increased fibrinolytic activity is elicited by elevated liberation [18] of tissue activators from the alveolar bone resulting from infections or trauma [19]. Tissue activators release some sort of enzymes which play a vital role in the generation of pain senescence, two enzymes kininogenases [20] and bradykinins [21] effectively released by these tissue activators. It was also found that, at the site of normal extraction there was no plasmin-like activity. An experiment was conducted by using tissue activator inhibitor tranexamic acid [22] but it was unsuccessful in reducing the incidence of dry socket on the other hand another acid 2-(acetyloxy) benzoic acid in combination with propyl 4-hydroxybenzoate which is a plasmin inhibitor was used and it was successful in reducing the incidence of dry socket occurrence. Further studies showed that plasmin was an independent product and it was not activated by any tissue activators [23]. Use of local antibiotics were also successful in reducing the dry socket and this was inconsistent to tissue activators concept. Bacteria were involved in treating certain thromboembolic diseases by elevating the fibrinolysis [24] and on this basis, an
implication was made that bacteria are the producers of plasmin-like products. It was found that Treponema denticola [25] is a reason that lies, blood clots multiply without even producing clinical symptoms of infection such as pus formation, redness, swelling and on the basis of an experiment in which the patient’s sample, which was suffering from dry socket, was collected which contained T. denticola. T. denticola is one of the type of anaerobic bacteria and exhibits plasmin-like fibrinolytic activity [14].
Risk Factors
Age:
Age has a direct impact on the incidence of dry socket, studies have shown and supports that incidence of dry socket occurs generally in childhood [26] and dry socket occurrence is increased with the increase in age [27]. The severity and intensity of the disease varies from people to people and at different stages of life, the onset of this disease is at its peak in 3rd and 4th decade of life [28]. Smoking in this period of life also contributes in the elevation of dry socket incidence. Age is considered to be associated with higher incidence of alveolar osteitis experiment concluded that removal of impacted mandibular third molars surgically must be carried out properly before the age of 24 years because in older patients the risk of postoperative complications are greater as compared to postoperative complications in younger patients in general [29]. With the onset of age, cells lose their efficiency of proper functioning and are more viable to dysfunctions and exposure to certain diseases[30].
Smoking:
Smoking has been the key factor in the reduction of phagocytosis and neutrophil chemotaxis [31] along with the disruption in immunoglobulin production [32]. There was high incidence of dry socket occurrence in heavy smokers as compared to the non-users [33] of smoking because smoking significantly contributes in efficiently lowering the immediate post extraction filling of sockets with blood [34]. Sockets with reduced ability to fill them with the blood are more viable to the incidence of dry socket occurrence. Cigarettes contain nicotine [35] and nicotine is a vasoconstrictor [36] which is efficiently absorbed through the oral mucosa and plays its vital role in constricting the blood vessels.
Inadequate Irrigation:
An experiment was conducted on the bilateral impacted mandibular third molars in 200 patients and it was observed that one side was irrigated with 176 mL of saline and other side was irrigated with 24mL of saline [37]. In high volume lavage group 12 instances of dry socket occurrence are observed in the study and 23 instances of dry socket occurrence were observed in the low volume lavage group, result was statistical notable and on the base of this result it was also postulated that there is reduced bacterial contamination of the socket by lavage [38].
Pericoronitis:
A third molar tissue surrounded by the inflammation, a condition known as pericoronitis [39] also contributes in the incidence of dry socket occurrence. The third molar tissues, which are not fully visible or partially impacted, are more into this disease. The incidence of pericoronitis was observed to be seen more commonly in lower molars as compared to the upper molars [40]. Study of 942 patients was done and out of which 14.2% of patients, which were previously affected with pericoronitis, developed dry socket as compared to 6.6 % of the patients without the pericoronitis along with this it was also observed that there was an effective reduction [41] in the progression of incidence when there was use of pro-phylactic antibiotics [42]. Furthermore, the scientist Nitzan which was conducting the experiment was successfully able to isolate T. denticola from sites affected by pericoronitis.
Use of Anaesthetics:
Studies were conducted to observe the effects of local anaesthetics on the dry socket [43] occurrence. Incidence of dry socket is known to develop under general anaesthesia without use of any local anaesthetics in cases of extractions. It was observed that periodontal ligament anaesthesia [44] does not contributes in the elevation of dry socket incidents as compared to block anaesthesia. It was also found that forceful infiltration of to 2mL extra anaesthetic lead to higher but insignificant dry socket incidents statistically. It was postulated by some investigators that there is no such vital role of vasoconstrictor in local anaesthesia on dry socket incidence [45]. But later studies showed that repeated PDL anaesthetic injections used after single nonsurgical tooth extractions in males led to the formation of dry socket up to 10.9% as compared to the 2.1% for block injections. It was also found that the repeated use of conventional infiltration ultimately leads to the increased dry socket [46] occurrence to 5.5%. It was also found that dry socket was also prevalent with the use of prilocaine with epinephrine in a ratio of 1:200,000 as compared to lidocaine with epinephrine in a ratio of 1:100,000 [47]. It was postulated that epinephrine could reduce [48] the bleeding along with this it can also interfere with oxygen tension and ultimately reducing the healing, epinephrine was also observed to play a vital role in the elevation of fibrinolysis [49], on this basis while using the repeated PDL anaesthetic injections caution must be noticed.
Flap Design:
It has been reported that the altered triangular flap [50] reduces the chance of alveolar osteitis occurrence more than the buccal envelope flap. Patients with extraction of a bilateral impacted mandibular third molar with the same difficulty have been examined, a buccal envelope flap was placed on one side and an altered triangular flap was placed on the other side, at day 3 and day 7 after surgery Alveolar Osteitis and healing was assessed [51].
Trauma:
Certain experiments were performed to observe the correlations between dry socket and surgical trauma but the authors were unable to find any sort of association between them. In spite of this, the literature still supports the relationship between dry socket and surgical trauma. It is postulated that trauma results in the compression of possible thrombosis of the underlying vessels as well as compression of the bone lining the socket [52], leading towards the reduction of blood perfusion [53]. Some studies correlated wound infection by anaerobes and the reduction in tissue resistance as trauma. Some studies relates alveolar bone damage and cell damage to the release of fibrinolytic activity activators of tissues. These factors usually involves XII factor [54], endothelial plasminogen activators and urokinase [55] from blood and tissues.
Various studies have shown that extraction of mandibular third molars is commonly followed by Alveolar Osteitis but on the contrary basis some authors believe that there are some other factors which are responsible for the specificity of the site [56], these factors involve increased bone density, reduced capacity of producing granulation tissue and decreased vascularity. The incidence of dry socket due to the smoking, surgical trauma, extraction site, operator experience, antibiotics, difficulty of surgery and systemic disorder have shown higher pain levels and persistent pain longer than two days with more traumatic surgeries [57]. Smoking was observed as one of the main factor which is directly linked with the development of postoperative complications or traumatic surgeries [58]. Factors like extraction site, sex, and age, amount of anaesthesia, medical history and operator experience have no such effect [59] on the observation of dry socket meanwhile on the other hand surgical trauma, single extractions and smoking are considered as predisposing factors in the incidence of dry socket. Incidence of dry socket was observed to be more common in patients with smoking [45], smoking is directly related to the incidence of dry socket and it was significantly high in single extraction cases rather than multiple extraction cases (extraction site, operator experience, age, sex have no vital role in dry socket occurrence).
Menstrual cycle and Oral contraceptives:
A lot of experiments were done to ensure that the link between the menstrual cycle and the frequency of Alveolar Osteitis. The patients with bilateral impacted third molar teeth underwent randomised surgical extraction [60], one tooth gel in the middle of the cycle and one during the menstrual period, post-operative examination was aware of the patient’s menstrual cycle status, frequency of Alveolar Osteitis was about 23.35%. In both the oral contraceptive users and non-users the frequency of Alveolar Osteitis was greater in the middle of the cycle then during the menstrual period. It revealed that oral contraceptive users have significantly greater frequency of Alveolar Osteitis as compared to the users without oral contraceptive intakes [61]. A study showed that control of preoperative infection, avoidance of trauma, avoidance of surgery on days 1 to 21 of menstrual cycle in non-menopausal women and persistence on good oral hygiene in women may reduce the occurrence of dry socket [62]. In females the oral contraceptive use was elicited up to 25% and during days 1 to 21 of their menstrual cycle extractions were performed. About 66% of extractions were traumatic, elicited risk factors just that in both genders infected posterior was at equal risk. In males traumatic extraction in mandibular tooth and poor oral hygiene were prominent [53] meanwhile extractions performed in females between the day 1 and 22 of their menstrual cycle were in high amount.
Microorganisms’ role in the Alveolar Ostetis development:
A study was conducted to observe the effect of infection induced experimentally, Fusobacterium nucleatum [63], Prevotella melaninogenica, Streptococcus anginosus, Streptococcus sanguis and Treponema socranskii [64] were present in the inoculation material. This experiment was conducted in the sockets of rats and it showed that there was a higher level of serum C reactive protein along with this it also showed the potential of infection propagation and disturbance in the repairing process of alveolar Osteitis [65]. It was a valuable experimental model for studying the stages and processes of alveolitis. Another experiment was conducted and it reported that process of healing in certain patients can be delayed in some cases because the sites in the patients were effected by osteomyelitis [66] previously [67].
Irrigation of Post-Extraction Socket with Normal Saline:
Another study was conducted and it showed the role of socket irrigation with the normal saline solution on the development of alveolar osteitis [68] at the end of extraction routinely and after mandibular third molars removal it was observed that there is a difference of dry socket occurrence, 22.1 percent on non-irrigated site and 77.7 percent on irrigated site, this study demonstrated between the modified approaches without ending surgery irrigation and traditional extraction protocols. Along with this, study also showed that for proper socket healing and to avoid uncomplicated socket healing post extraction socket bleeding is very crucial [69] and if post extraction socket bleeding is not washed out then there will be the formation of normal blood clot this normal blood clot can be further progressed in the formation of uncomplicated [70] socket healing without even the alveolar osteitis development. Alveolus might interfere with the blood clot formation due to the repeated excessive irrigation and ultimately lead to a violent curettage which might cause harm to the alveolar bone [71].
Remnants of Debris and Bone/Root Fragments:
Studies have shown that some other factors are also contributing towards the development of alveolar osteitis and disturbance in its healing, these factors includes remnants of the debris and fragments of bones/root [72]. Studies have shown that bone/ root fragments are actively contributing towards the disturbance in healing and improper development of normal cells ultimately leading towards the development of alveolar osteitis [73]. After tooth extraction small fragments of bone/root are commonly present, these remnants do not take part in any sort of complications because the epithelium cells of the oral cavity often concretize them.
Treatment:
Alveolitis treatment solely depends on the clinical experience of a professional. For an exposed bone to be covered with new granulation tissues a time period of 7 to 10 days [74] is required on average basis, and during this time period certain efforts are made to reduce the intensity of pain and to relieve the patient’s discomfort. Different materials have been known to be valuable and recent studies have showed that eugenol containing dressing play a vital role in the prevention of dry socket immediately but it also contribute to the slowed or delayed healing of wound [75]. Turner used removal of bone particles, removal of granulation tissues, curettage and reflection of flap with irrigation and observed that the method required very few visits as compared to zinc oxide-eugenol [76]. He also mentioned that the socket packing contributes to the delayed healing of socket and elevated infection risk. Irrigation usually involves the removal of bacteria from the denuded bone sequestra and debris. Packing must be changed in every 3 to 4 days and when there is reduced pain it must be removed [77].
Role of antibiotics:
The most effective drugs to ease the discomfort caused by dry socket is the use of non-steroidal anti-inflammatory drugs such as aspirin and ibuprofen [78]. If the drugs fail to reduce the pain then doctors prescribe an even stronger drug or they may anesthetize the targeted area. Most of the dentists clean the tooth socket and fill it with some sort of medicated product and you need to visit your dentist every few days for the dressing of socket until it starts to heal. Your doctor may recommend salt water or good mouthwash at home to prevent the socket from infection.
Low level laser, alvogyl and SaliCept patch:
These three modes of treatment are used for the management of alveolar osteitis. These strategies can be compared in terms of their effectiveness. The comparison between alvogyl[79] and SaliCept[8] resulted in no striking difference. For example, patients treated with alvogyl, which was applied, directly to the socket after curettage and irrigation and the patients treated with SaliCept rather than alvogyl brought the same results. Application of continuous-mode diode laser irradiation was a significantly better option than the other two discussed before. The laser technique managed the disorder in a better way.
Use of sutures and local homeostatic:
A research revealed less pain, inflammation and other complications in suture-less group and a considerably longer operation time in various suture groups[77]. But in terms of pain and swelling there were no differences between the two groups. Use of tranexamine acid and sutures lowered the postoperative bleeding after tooth removal in patients on continued warfarin medication[80].
The use of eugenol on a gauze stripe and a thermosetting gel:
In one study thirty one patients with post-extraction alveolar osteitis were assigned to two different groups i.e. either control or test group. Control patients were treated with eugenol on a gauze strip placed in the socket and test groups were treated with thermosetting gel containing 2.5% prilocaine and 2.5% lidocaine directly placed into the socket. All patients were also given an analgesic in case of any pain during 48 hour period. Consequently, thermosetting resulted in greater reduction in pain as compared to eugenol gel over the period of next 48 hours.
Use of pastille GECB:
In another study patients were again distributed in two groups. Test patients were given GECB [76] and control patients were given ZOE dressing [81]. After the administration the elapsed time for relieve of pain was recorded. Ibuprofen drug was prescribed after the treatment as per need. Patients were analysed for 20 days, severity of pain was assessed by visual analogue scale and after this time period, the number of pills taken by the patients was recorded and the whole data was analysed. It was found that application of GECB significantly reduced the complications than ZOE [82].
Use of plasma rich in growth factors:
Following surgery the healing of mouth tissue can also be achieved by patient’s own blood called PRGF (Plasma rich in growth factors). Various studies have proved that PRGF [83] not only promotes tissue healing effectively but also reduces the numbers of clinical concerns after surgical procedures. Before operation patient’s own venous blood is taken and then treated and heated to get gel like consistency and finally applied to the targeted site. PRGF encourages the healing of dry socket, surrounding tissues and also aid in regeneration.
Prevention:
Many researchers have tried to find a way or method of prevention from incidence of alveolar osteitis. After extraction the most common postoperative complication is alveolar osteitis and that's why it is mandatory to find a successful method to cope up with this disease. Many methods have been used in the treatment of dry socket but none of these methods can be accepted as universal method for treating dry socket, some of these popular techniques are discussed below.
Antibiotics:
Antibiotics have played a vital role in treating a lot of diseases [84] and it is also reported that antibiotics are used for in the prevention of dry socket occurrence. Use of antiseptic rinses and antibiotic preparations after the extraction was mentioned as one of the pharmacological methods which are used in the prevention of dry socket occurrence [85]. It was also suggested that for patients with the previous history of multiple dry sockets occurrence must not use antibiotics in the extraction socket [86]. Alveolar osteitis can be prevented by use of some systemic antibiotics, these antibiotics includes erythromycin, metronidazole [87], clindamycin and penicillin. By the repeated use of pre or postoperative systemic antibiotics, there is possibility of development of resistance in bacterial strains and hypersensitivity. In contrast with other antibiotics other factors which involves acv is suspension gauze, drain gel foam, sponges and some applications of tetracycline [88] have shown efficient results in reducing the alveolar osteitis occurrence. Another antibiotic azithromycin as compared to the other antimicrobials have played a significant role as a pro-phylactic use in the impacted mandibular third molar surgery, in this surgery mainly cephalosporins [89] and penicillins [90] were used. Another study was conducted to observe the effect of lincomycin applications on (TCP) Beta-tricalcium phosphate [91] to alveolus. It was seen that there was a reduction in the complications in the form of pain and trismus and along with this lincomycin on TCP also prevented from the development of alveolar osteitis[92]. It was also observed that atrophy of alveolar process is also prevented by Beta-tricalcium phosphate (TCP).
Chlorhexidine:
Chlorhexidine plays an important role in the prevention of dry socket [93], its use have been monitored and it has shown positive effects against the incidence of dry socket. Chlorhexidine exists in two forms one is gel and the other is rinse form, studies have shown that by the use of different forms of chlorhexidine there was a significant reduction in the incidence of dry socket. Use of chlorhexidine mouth rinse pre or postoperatively resulted in the significant reduction in the development of dry socket after extraction of mandibular third molars [72]. It was observed that in 30 seconds of 0.12% chlorhexidine solution use, there was 50% reduction in the occurrence of dry socket along with this 0.2% of bio adhesive chlorhexidine gel use, also contributed in the reduction of alveolar osteitis development.
Eugenol containing dressing:
Eugenol has a crucial role as a reducer [88]. Dressing Alvogyl that contains butamben, idoform and eugenol easily available commercially and must be replaced after two days. It was observed that the incidence of dry socket [94] in the sockets which were immediately packed was about 8% and the sockets which were not immediately packed with medicated dressing, the incidence of dry socket was 26%.
Steroids:
Steroids have also shown a valuable role in the reduction of dry socket incidence. Topical application of a mixture of oxytetracycline and hydrocortisone has shown significant decrease in the incidence of dry socket [95] after the extraction of impacted mandibular third molars.
Antifibrinolytics:
Some antifibrinolytics have also shown positive effects in prevention of dry socket incidence [96]. One of the antifibrinolytic (Tranexamic acid) has shown its vital role in the prevention of incidence of dry socket.
Low level laser therapy:
Certain studies on the low level laser therapy in preventing dry socket have been conducted and it was found that low level laser therapy plays a significant role in the reduction of inflammation [97] as well as it also contributes in elevating the speed of wound healing as compared to SaliCept and Alvogyl. After the irrigation of socket with the help of continuous-mode diode laser irradiation low level laser therapy is applied.
Dextranomer granule:
Studies have shown that the use of dextranomer granule significantly reduces the incidence of dry socket and effectively promote faster pain relief.
Conclusion![]()
Aetiology of the dry socket is complex and the duration and severity of the disease is totally determined by the healing potential of the host. The cause of dry socket occurrence remains evasive because dry socket is a self-limiting constrain. Different sort of strategies are used and management is aimed, until healing of the dry socket begins, to relieve the patient's pain. Dry Socket wound healing is achieved by the reduction in facilitating the wound with food debris and microorganisms, it can be accelerated with the help of irrigation of socket with chlorhexidine which is followed by the prescription of analgesics and medicated dressing placement on the wound. When the dressing is placed then the patient should be kept under observation or review to check if the socket is healing or not. Make sure the repetitions are excluded or summarized once in the whole content.
Availability of the options for the treatment of dry socket is generally limited and these are directed towards the soothing care. Smoking or use of cigarettes after the surgery or before the surgery is prohibited and is enlisted as a prevention method to prevent from dry socket occurrence after traumatic surgery. Antibiotics such as azithromycin can be taken to cop against this disease. Along with this, chlorhexidine rinse or gel can be very valuable in efficiently effecting the reduction of dry socket incidence occurrence.
The authors declare that there is no conflict of interest regarding the publication of this paper.
References![]()
- Van der Weijden F, Dell'Acqua F, Slot DE. Alveolar bone dimensional changes of post‐extraction sockets in humans: a systematic review. Journal of clinical periodontology, (2009); 36(12): 1048-1058.
- Cardoso CL, Rodrigues MTV, Júnior OF, Garlet GP, de Carvalho PSP. Clinical concepts of dry socket. Journal of Oral and Maxillofacial Surgery, (2010); 68(8): 1922-1932.
- Younis MHA, Ra'ed O. Dry socket: frequency, clinical picture, and risk factors in a palestinian dental teaching center. The open dentistry journal, (2011); 57.
- Iwabuchi H, Imai Y, Asanami S, Shirakawa M, Yamane G-y, et al. Evaluation of postextraction bleeding incidence to compare patients receiving and not receiving warfarin therapy: a cross-sectional, multicentre, observational study. BMJ open, (2014); 4(12): e005777.
- Gwinnutt M, Gwinnutt CL Clinical anaesthesia. 2016; John Wiley & Sons.
- Ortmann E, Besser M, Klein A. Antifibrinolytic agents in current anaesthetic practice. British journal of anaesthesia, (2013); 111(4): 549-563.
- Kolokythas A, Olech E, Miloro M. Alveolar osteitis: a comprehensive review of concepts and controversies. International journal of dentistry, (2010); 2010.
- Taberner-Vallverdú M, Nazir M, Sánchez-Garcés MÁ, Gay-Escoda C. Efficacy of different methods used for dry socket management: A systematic review. Medicina oral, patologia oral y cirugia bucal, (2015); 20(5): e633.
- Yeung CA, Tsang T, Yau P, Kwok T. Human papillomavirus type 16 E6 induces cervical cancer cell migration through the p53/microRNA-23b/urokinase-type plasminogen activator pathway. Oncogene, (2011); 30(21): 2401.
- Gemin M. A Potential Role for Sortilin in Lp (a) and Apo (a) Metabolism. (2018). Electronic Theses and Dissertations. 5937. https://scholar.uwindsor.ca/etd/5937
- Preetha S. An overview of dry socket and Its management. IOSR Journal of Dental and Medical Sciences, (2014); 13(5): 2.
- Puidokas T, Kubilius M, Nomeika D, Januzis G, Skrodeniene E. Comparative Analysis of Blood Clot, Plasma Rich in Growth Factors and Platelet-Rich Fibrin Resistance to Bacteria-Induced Fibrinolysis. Microorganisms, (2019); 7(9): 328.
- Hasumi K, Yamamichi S, Harada T. Small‐molecule modulators of zymogen activation in the fibrinolytic and coagulation systems. The FEBS journal, (2010); 277(18): 3675-3687.
- Barman SP (2011) Compositions and methods to prevent and treat dry socket post-operatively after tooth extraction surgery. Google Patents.
- Matsuo K, Akasaki Y, Adachi K, Zhang M, Ishikawa A, et al. Promoting effects of thymosin β4 on granulation tissue and new bone formation after tooth extraction in rats. Oral surgery, oral medicine, oral pathology and oral radiology, (2012); 114(1): 17-26.
- Anitua E, Cugat R, Sánchez M. Platelet Rich Plasma in Orthopaedics and Sports Medicine. (2018): Springer.
- Klingberg E, Nurkkala M, Carlsten H, Forsblad-d’Elia H. Biomarkers of bone metabolism in ankylosing spondylitis in relation to osteoproliferation and osteoporosis. The Journal of rheumatology, (2014); 41(7): 1349-1356.
- Andreasen JO, Andreasen FM, Andersson L Textbook and color atlas of traumatic injuries to the teeth. (2018); John Wiley & Sons.
- Khiyavi R, Barghi V, Yazdani J, Ghavimi MA, Khiyavi SG, et al. Effect of Biotene mouth wash on prevention of alveolar osteitis after extraction of permanent mandibular first molar teeth. Elixir Hum Physiol, (2012); 478672-8674.
- HABERLAND GL. FUNCTIONS OF THE KALLIKREIN-KININ SYSTEM OUTSIDE THE CLOTTING CASCADE; 2014. Elsevier. pp. 205.
- Erdös EG, Wilde AF Bradykinin, kallidin and kallikrein. Chapter: Book Name. 2013 of publication; Springer Science & Business Media.
- Anand K, PAtro S, MohAPAtrA A, MiShrA S. The efficacy of Tranexamic acid in the reduction of incidence of dry socket: an Institutional double blind study. Journal of clinical and diagnostic research: JCDR, (2015); 9(9): ZC25.
- Veale B. Alveolar osteitis: a critical review of the aetiology and management. Oral Surgery, (2015); 8(2): 68-77.
- Emmi G, Silvestri E, Squatrito D, Amedei A, Niccolai E, et al. Thrombosis in vasculitis: from pathogenesis to treatment. Thrombosis Journal, (2015); 13(1): 15.
- Dashper S, Seers C, Tan K, Reynolds E. Virulence factors of the oral spirochete Treponema denticola. Journal of dental research, (2011); 90(6): 691-703.
- Haraji A, Rakhshan V. Single-dose intra-alveolar chlorhexidine gel application, easier surgeries, and younger ages are associated with reduced dry socket risk. Journal of Oral and Maxillofacial Surgery, (2014); 72(2): 259-265.
- Eshghpour M, Nejat A. Dry socket following surgical removal of impacted third molar in an Iranian population: Incidence and risk factors. Nigerian journal of clinical practice, (2013); 16(4).
- Khitab U, Khan A, Shah SM. Clinical characteristics and treatment of dry socket-A Study. Pakistan oral & dental journal, (2012); 32(2): 206-209.
- Saxton A, Velanovich V. Preoperative frailty and quality of life as predictors of postoperative complications. Annals of surgery, (2011); 253(6): 1223-1229.
- Sahin E, DePinho RA. Linking functional decline of telomeres, mitochondria and stem cells during ageing. nature, (2010); 464(7288): 520.
- Majumdar R, Tameh AT, Parent CA. Exosomes mediate LTB4 release during neutrophil chemotaxis. PLoS biology, (2016); 14(1): e1002336.
- Guo Sa, DiPietro LA. Factors affecting wound healing. Journal of dental research, (2010); 89(3): 219-229.
- Al–Mahozi S, Salim Z, Malden NJ, Scully C, Lopes V. Tobacco habit-associated oral disease and the negative effects on surgical outcomes. Dental Update, (2017); 44(11): 1065-1070.
- Eshghpour M, Danaeifar N, Kermani H, Nejat AH. Does intra-alveolar application of chlorhexidine gel in combination with platelet-rich fibrin have an advantage over application of platelet-rich fibrin in decreasing alveolar osteitis after mandibular third molar surgery? A double-blinded randomized clinical trial. Journal of Oral and Maxillofacial Surgery, (2018); 76(5): 939. e931-939. e937.
- Marynak KL, Gammon DG, Rogers T, Coats EM, Singh T, et al. Sales of nicotine-containing electronic cigarette products: United States, 2015. American journal of public health, (2017); 107(5): 702-705.
- Davies CS, Ismail A. Nicotine has deleterious effects on wound healing through increased vasoconstriction. Bmj, (2016); 353i2709.
- Haraji A, Rakhshan V. Chlorhexidine gel and less difficult surgeries might reduce post‐operative pain, controlling for dry socket, infection and analgesic consumption: a split‐mouth controlled randomised clinical trial. Journal of oral rehabilitation, (2015); 42(3): 209-219.
- Smith JA (2018) Peri-Operative Infection Control in Maxillofacial Surgery. Perioperative Assessment of the Maxillofacial Surgery Patient: Springer. pp. 129-144.
- Magraw CB, Golden B, Phillips C, Tang DT, Munson J, et al. Pain with pericoronitis affects quality of life. Journal of Oral and Maxillofacial Surgery, (2015); 73(1): 7-12.
- Singh P, Nath P, Bindra S, Rao SS, Reddy KR. The predictivity of mandibular third molar position as a risk indicator for pericoronitis: A prospective study. National journal of maxillofacial surgery, (2018); 9(2): 215.
- Błochowiak K, Aleksandrzak P, Kropielnicki K, Handschuh J, Pawlik P, et al. Extraction of asymptomatic impacted third molars–a review. (2019); European Journal of Clinical and Experimental Medicine; 17 (1): 71–78.
- Bauer M, Krüger R, Kölsch U, Unterwalder N, Meisel C, et al. Antibiotic prophylaxis, immunoglobulin substitution and supportive measures prevent infections in MECP2 duplication syndrome. The Pediatric infectious disease journal, (2018); 37(5): 466-468.
- Lim HW, Mahmod NI, Zaki FHA, Tan FY, Balasundram S, et al. Wisdom Tooth Surgery Complications—Local Anaesthesia versus General Anaesthesia. Open Journal of Stomatology, (2019); 9(03): 51.
- Marques-Ferreira M, Carrilho E, Paulo S, Carrilho T, Figueiredo JP, et al. Anaesthesia in dental medicine with local infiltrative anaesthetic technique versus diploe anaesthesia delivery systems: efficacy and behaviour, an experimental study. Acta medica portuguesa, (2017); 30(12): 848-853.
- Rakhshan V. Common risk factors of dry socket (alveolitis osteitis) following dental extraction: A brief narrative review. Journal of stomatology, oral and maxillofacial surgery, (2018); 119(5): 407-411.
- do Nascimento Poubel VL, Silva CAB, Mezzomo LAM, Canto GDL, Rivero ERC. The risk of osteonecrosis on alveolar healing after tooth extraction and systemic administration of antiresorptive drugs in rodents: a systematic review. Journal of Cranio-Maxillofacial Surgery, (2018); 46(2): 245-256.
- PRIYATHAM S, NUVVULA S. INTRAORAL TOPICAL ANAESTHESIA IN PEDIATRIC DENTISTRY. Int J Pharm Bio Sci, (2016); 7(4): 346-353.
- Mittal R, Debs LH, Patel AP, Nguyen D, Patel K, et al. Neurotransmitters: The critical modulators regulating gut–brain axis. Journal of cellular physiology, (2017); 232(9): 2359-2372.
- Keihanian F, Saeidinia A, Bagheri RK, Johnston TP, Sahebkar A. Curcumin, hemostasis, thrombosis, and coagulation. Journal of cellular physiology, (2018); 233(6): 4497-4511.
- Elo JA, Sun H-HB, Dong F, Tandon R, Singh HM. Novel incision design and primary flap closure reduces the incidence of alveolar osteitis and infection in impacted mandibular third molar surgery. Oral surgery, oral medicine, oral pathology and oral radiology, (2016); 122(2): 124-133.
- Bataineh AB, Ra’ad AB. The effect of modified surgical flap design for removal of lower third molars on lingual nerve injury. Clinical oral investigations, (2017); 21(6): 2091-2099.
- Sykes LM, Herbst D, Dullabh H, Fernandes N. Comparison of alveolar osteitis with post implant removal osteitis (Can a" dry socket" occur after implant removal?). South African Dental Journal, (2017); 72(6): 278-281.
- Mudali V, Mahomed O. Incidence and predisposing factors for dry socket following extraction of permanent teeth at a regional hospital in Kwa-Zulu Natal. South African Dental Journal, (2016); 71(4): 166-169.
- Daugela P, Grimuta V, Sakavicius D, Jonaitis J, Juodzbalys G. Influence of leukocyte-and platelet-rich fibrin (L-PRF) on the outcomes of impacted mandibular third molar removal surgery: A split-mouth randomized clinical trial. Quintessence International, (2018); 49(5):377-388. doi: 10.3290/j.qi.a40113.
- Mamoun J. Dry socket etiology, diagnosis, and clinical treatment techniques. Journal of the Korean Association of Oral and Maxillofacial Surgeons, (2018); 44(2): 52-58.
- Al‐Nuaimi N, Patel S, Foschi F, Mannocci F. The detection of simulated periapical lesions in human dry mandibles with cone‐beam computed tomography: a dose reduction study. International endodontic journal, (2016); 49(11): 1095-1104.
- Choung H-W, Lee S-H, Ham AR, Lee NR, Kim B, et al. Effectiveness of Low-Level Laser Therapy with a 915 Nm Wavelength Diode Laser on the Healing of Intraoral Mucosal Wound: An Animal Study and a Double-Blind Randomized Clinical Trial. Medicina, (2019); 55(8): 405.
- Klug A, Wincheringer D, Harth J, Schmidt-Horlohé K, Hoffmann R, et al. Complications after surgical treatment of proximal humerus fractures in the elderly—an analysis of complication patterns and risk factors for reverse shoulder arthroplasty and angular-stable plating. Journal of shoulder and elbow surgery, (2019); Sep;28(9):1674-1684. doi: 10.1016/j.jse.2019.02.017.
- Barone A, Toti P, Marconcini S, Derchi G, Saverio M, et al. Esthetic Outcome of Implants Placed in Fresh Extraction Sockets by Clinicians with or without Experience: A Medium-Term Retrospective Evaluation. International Journal of Oral & Maxillofacial Implants, (2016); 31(6): 35-41.
- Khan MA, Ahmad T, Khadija SH. Frequency of dry socket, pain, wound dehiscence and swelling one week after removal of mandibular third molar impaction. Journl of Khyber College of Dentistry, (2015); 5(2): 20-23.
- Yüce E, Kömerik N. Potential effects of advanced platelet rich fibrin as a wound-healing accelerator in the management of alveolar osteitis: A randomized clinical trial. Nigerian journal of clinical practice, (2019); 22(9): 1189.
- Tarakji B, Saleh LA, Umair A, Azzeghaiby SN, Hanouneh S. Systemic review of dry socket: aetiology, treatment, and prevention. Journal of clinical and diagnostic research: JCDR, (2015); 9(4): ZE10.
- Aguilar-Durán L, Figueiredo R, Seminago R, Roig FJ, Llorens C, et al. A metagenomic study of patients with alveolar osteitis after tooth extraction. A preliminary case-control study. Clinical oral investigations, (2019); 1-10.
- Krishnan K, Chen T, Paster B. A practical guide to the oral microbiome and its relation to health and disease. Oral diseases, (2017); 23(3): 276-286.
- Scasso F, Ferrari G, DE GV, Arosio A, Bottero S, et al. Emerging and re-emerging infectious disease in otorhinolaryngology. Acta otorhinolaryngologica Italica: organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale, (2018); 38(SUPPL. 1): S1-S106.
- Vakil N, Singh A, Sadiq H. COMPARATIVE STUDY OF USEFULNESS OF ALVOGYL AND ZINC OXIDE EUGENOL AFTER SALINE IRRIGATION FOR MANAGEMENT OF DRY SOCKET. Paripex-Indian Journal Of Research, (2019); 8(5): 166-167.
- Goldblatt LI, Adams WR, Spolnik KJ, Deardorf KA, Parks ET. Chronic fibrosing osteomyelitis of the jaws: an important cause of recalcitrant facial pain. A clinicopathologic study of 331 cases in 227 patients. Oral surgery, oral medicine, oral pathology and oral radiology, (2017); 124(4): 403-412. e403.
- Mahmoud M, Gutknecht N, AlNaggar A, de Cara SPHM, Marques MM. The effect of photobiomodulation therapy in the management of alveolar osteitis after tooth extraction: a scoping review. Lasers in Dental Science, (2019); 3(1): 11-20.
- Pippi R. Post-surgical clinical monitoring of soft tissue wound healing in periodontal and implant surgery. International journal of medical sciences, (2017); 14(8): 721.
- Flanagan D, Mancini M. Bimaxillary full arch fixed dental implant supported treatment for a patient with renal failure and secondary hyperparathyroidism and osteodystrophy. Journal of Oral Implantology, (2015); 41(2): e36-e43.
- Wayland J. Impacted Third Molars. (2018); Wiley Online Library.
- Ghaeminia H, Hoppenreijs TJ, Xi T, Fennis J, Maal T, et al. Postoperative socket irrigation with drinking tap water reduces the risk of inflammatory complications following surgical removal of third molars: a multicenter randomized trial. Clinical oral investigations, (2017); 21(1): 71-83.
- Chenicheri S, Usha R, Ramachandran R, Thomas V, Wood A. Insight into oral biofilm: primary, secondary and residual caries and phyto-challenged solutions. The open dentistry journal, (2017); 11312.
- Martin-Thomé H, Bourdin D, Strube N, Saffarzadeh A, Morlock J-F, et al. Clinical Safety of a New Synthetic Resorbable Dental Membrane: A Case Series Study. Journal of Oral Implantology, (2018); 44(2): 138-145.
- Sharon E, Polak D, Sharon S, Beyth N. Wound Dressing in the Oral Cavity. In: . Recent Clinical Techniques, Results, and Research in Wounds. (2017). Springer. DOI: https://doi.org/10.1007/15695_2017_5.
- Ezhil I, Kumar M. Recent advances in the management of dry socket-A review. Drug Invention Today, (2018); 10(4): 450-455.
- Tuk JG, Lindeboom JA, Sana F, van Wijk AJ, Milstein DM. Alveolar Iodine Tampon Packing Reduces Postoperative Morbidity After Third Molar Surgery. Journal of Oral and Maxillofacial Surgery, (2019): Article in Press. DOI: https://doi.org/10.1016/j.joms.2019.06.175.
- Sidana S, Mistry Y, Gandevivala A, Motwani N. Evaluation of the need for antibiotic prophylaxis during routine intra-alveolar dental extractions in healthy patients: a randomized double-blind controlled trial. Journal of Evidence Based Dental Practice, (2017); 17(3): 184-189.
- Kumar R, Verma N. A COMPARATIVE STUDY IN TREATMENT OF DRY SOCKET ZINC OXIDE AND EUGENOL VS ALVOGYL. Paripex-Indian Journal Of Research, (2019); 8(2): 125-129.
- Febbo A, Cheng A, Stein B, Goss A, Sambrook P. Postoperative bleeding following dental extractions in patients anticoagulated with warfarin. Journal of Oral and Maxillofacial Surgery, (2016); 74(8): 1518-1523.
- Yan Z, Ni Y, Park JW, Will S, Loh H, et al. Microwave dressing of ultracold 23Na40K molecules. APS Division of Atomic, Molecular and Optical Physics Meeting Abstracts. (2017).
- Chakravarthi S. Platelet rich fibrin in the management of established dry socket. Journal of the Korean Association of Oral and Maxillofacial Surgeons, (2017); 43(3): 160-165.
- Anitua E, Muruzabal F, de la Fuente M, Merayo J, Durán J, et al. Plasma rich in growth factors for the treatment of ocular surface diseases. Current eye research, (2016); 41(7): 875-882.
- Jepsen K, Jepsen S. Antibiotics/antimicrobials: systemic and local administration in the therapy of mild to moderately advanced periodontitis. Periodontology 2000, (2016); 71(1): 82-112.
- Nagarajappa S, Bathija P, Mishra P, Bansal V, Gupta S, et al. ANTIBACTERIAL AND ANTIFUNGAL ACTIVITY OF NEEM AND CLOVE EXTRACT AGAINST S. MUTANS AND C. ALBICANS-AN INVITRO STUDY. World Journal of Pharmaceutical Research (2018); 7(5): 1484-93.
- Cervino G, Cicciù M, Biondi A, Bocchieri S, Herford AS, et al. Antibiotic prophylaxis on third molar extraction: Systematic review of recent data. Antibiotics, (2019); 8(2): 53.
- Kaur J, Raval R, Bansal A, Kumawat V. Repercussions of intraalveolar placement of combination of 0.2% chlorhexidine & 10 Mg metronidazole gel on the occurrence of dry sockets-A randomized control trial. Journal of clinical and experimental dentistry, (2017); 9(2): e284.
- Sharma A, Aggarwal N, Rastogi S, Choudhury R, Tripathi S. Effectiveness of platelet-rich fibrin in the management of pain and delayed wound healing associated with established alveolar osteitis (dry socket). European journal of dentistry, (2017); 11(4): 508.
- Sturrock A, Landes D, Robson T, Bird L, Ojelabi A, et al. An audit of antimicrobial prescribing by dental practitioners in the north east of England and Cumbria. BMC oral health, (2018); 18(1): 206.
- Ramos E, Santamaria J, Santamaria G, Barbier L, Arteagoitia I. Do systemic antibiotics prevent dry socket and infection after third molar extraction? A systematic review and meta-analysis. Oral surgery, oral medicine, oral pathology and oral radiology, (2016); 122(4): 403-425.
- Joshi CP, Dani NH, Khedkar SU. Alveolar ridge preservation using autogenous tooth graft versus beta-tricalcium phosphate alloplast: A randomized, controlled, prospective, clinical pilot study. Journal of Indian Society of Periodontology, (2016); 20(4): 429.
- Saghiri MA, Asatourian A, Sheibani N. Angiogenesis and the prevention of alveolar osteitis: a review study. Journal of the Korean Association of Oral and Maxillofacial Surgeons, (2018); 44(3): 93-102.
- Sajjan P, Laxminarayan N, Kar PP, Sajjanar M. Chlorhexidine as an antimicrobial agent in dentistry–a review. Oral Health Dent Manag, (2016); 15(2): 93-100.
- Tasoulas J, Daskalopoulos A, Droukas C, Nonni A, Nikitakis NG. An unusual microscopic pattern of foreign body reaction as a complication of dry socket management. Oral surgery, oral medicine, oral pathology and oral radiology, (2018); 125(5): e118-e123.
- Latta MA, Gross SM, McHale WA (2019) Buffered microencapsulated compositions and methods. Google Patents.
- Catanzano O, D'Esposito V, Formisano P, Boateng JS, Quaglia F. Composite alginate-hyaluronan sponges for the delivery of tranexamic acid in postextractive alveolar wounds. Journal of pharmaceutical sciences, (2018); 107(2): 654-661.
- Longo M, Garcia VG, Ervolino E, Alves MLF, Duque C, et al. Multiple aPDT sessions on periodontitis in rats treated with chemotherapy: histomorphometrical, immunohistochemical, immunological and microbiological analyses. Photodiagnosis and photodynamic therapy, (2019); 2592-102.
![]()
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0

