

Full Length Research Article
Epidemiology, incidence and mortality of Nasopharynx Cancer in Southeast Asia: an update report
Thuan Duc Lao, Thuy Ai Huyen Le*
Adv. life sci., vol. 7, no. 2, pp. 86-90, February 2020
*– Corresponding Author: Thuy Ai Huyen Le (Email: thuy.lha@ou.edu.vn)
Authors' Affiliations
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Nasopharyngeal cancer, with a distinct geographical and racial distribution, is the common neck and head cancer. Knowledge about the ecological factors including incidence, mortality, and so on, is important to find out the best way for its prevention in future. The aim of current study was to find out the incidence(-ASR), mortality(-ASR) of nasopharyngeal cancer and its correlation between those factors with HDI as well as its components in Southeast Asian countries in 2018.
Methods: The data of the incidence(-ASR), mortality(-ASR), Human development index (HDI) were extracted from the GLOBOCAN project and Human Development Reports database. The relationships were evaluated by using Pearson Correlation Coefficient method.
Results: In Southeast Asian region, incidence of 34,681, and mortality of 22,231 were recorded. The high incidence and mortality were related to medium human development countries. The significant positive correlations were observed between HDI with incidence-ASR (r = 6.25, p = 0.04) and mortality-ASR (r = 0.38, p = 0.26). No significant correlations were found between HDI component with incidence-ASR and mortality-ASR, except for the relationship between incidence-ASR and GNI/capita (r = 0.71, p = 0.02).
Conclusion: The nasopharyngeal cancer is native to Asian region, includes Southeast Asian countries. The highest incidence and mortality were recorded in medium HDI countries.
Keywords: Nasopharyngeal cancer; Epidemiology; Ecology, Southeast Asia
Introduction![]()
Nasopharyngeal cancer (NPC), arises from the epithelium of the nasopharynx, stands outs from other epithelial cancers in the head and neck regions with a distinct geographical and racial distribution [1-5]. The main etiological factors include Epstein Barr Virus infection, genetic susceptibilities, environmental factors, lead to the nasopharyngeal cancer [1,5,6]. Worldwide, in 2012, 86,691 new nasopharyngeal cancer cases were recorded. Among them, 60,896 and 25,795 cases were recorded in men and women (sex ratio = 2.36), respectively [2,3,7]. In addition to the geographical distribution, according to the global cancer project in 2012, 68,272 cases, counting for more than 75% NPC patients were seen in Asia, so that 71.03%, 28.97% patients were seen in male, female, respectively, (sex ratio: 2.64). According to age-specific incidence rate (ASIR), the highest ASIR of NC countries were Malaysia, Singapore, Indonesia, Viet Nam and Brunei, which are belonged to Southeast Asia [3]. One of the reasons for the differences in nasopharyngeal cancer incidence and mortality in different populations are conventional personal attribute information such as age, gender, ethnicity, family history, and an additional attribute other factors, such as smoking, pollution, chemicals, Cantonese-style salted fish used in many Southeast countries [1,3-5,8].
Human development index (HDI), a summary measure of average achievement in key dimensions of human development, includes life expectancy index, education index, and gross national income per capita [9,10]. Furthermore, HDI is classified as four levels, includes low (HDI < 0.535), medium (0.710 ≥ HDI ≥ 0.535), high (0.80 > HDI > 0.710) and very high (HDI ≥ 0.80) level [2,9]. The low and very high HDI level indicates countries that are the lease developed and the most developed countries [9]. To now, the HDI classification is considered as the useful criteria to make the comparison between the incidence, and mortality of many human diseases, includes cancer, in worldwide population. The association between HDI and the incidence, mortality of human cancers has been previously studied [9,10-13]. The known its association could lead to the accurate understanding of human cancer’s distribution [11]. Because the nasopharyngeal cancer incidence and mortality have been annually increasing in Southeast Asian countries, therefore, informing about the incidence, morality rate of nasopharyngeal cancer in the cancer prevention program is very important. Since the information about the nasopharyngeal cancer incidence, mortality rate in Southeast Asian countries could be useful applied for health program and research activities, current study aimed to determine the incidence, mortality of nasopharyngeal cancer, and its association with the HDI and its components in Southeast Asia in 2018.
Methods![]()
Study design
The current ecological study is performed to evaluate the correlation between HDI as well as its components, includes life expectancy at birth, mean years of schooling and gross national income per capita (GIN), and age-specific incidence and mortality of nasopharyngeal cancer in Southeast Asian countries. Data of age-specific incidence and mortality of nasopharyngeal cancer in 2018 was obtained from the global cancer observatory for each countries in Southeast Asia, available from http://gco.iarc.fr/today/home [14]. Data of HDI and its components were collected from Human Development Reports database, United Nations Development Program, available from http://hdr.undp.org/en/data [15].
Statistical analysis
Results![]()
Finding nasopharyngeal cancer case, HDI and its components
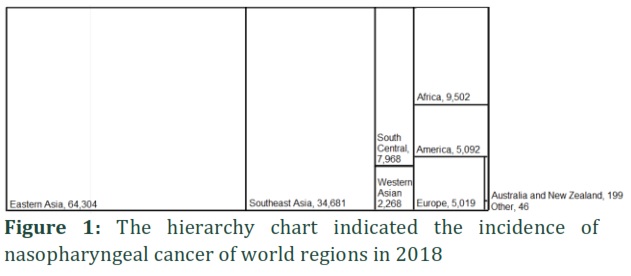
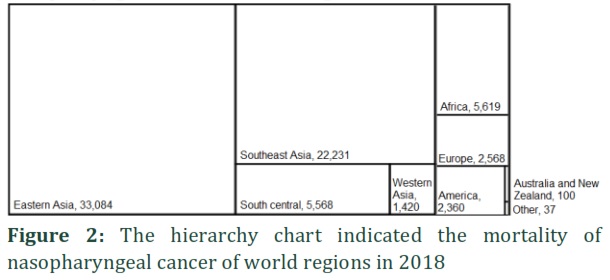
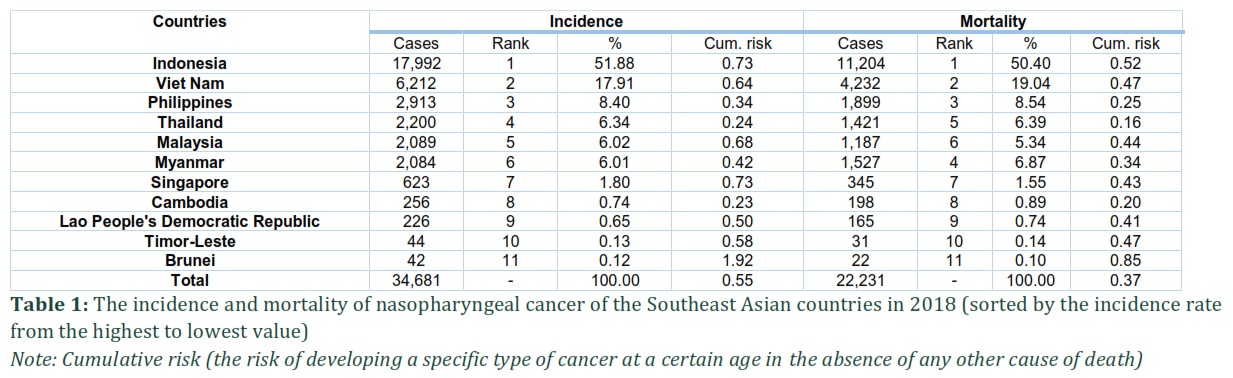
Generally, in 2018, a total of 129,079 new nasopharyngeal cases were recorded in the world, of which 93,416 cases (counting for 72.37%) were diagnosed in male, and 35,663 cases (counting for 27.63%) were diagnosed in female. This data figured out the male/female ratio is 2.62 : 1. A total of 72,987 nasopharyngeal death cases were occurred in the world, so that 54,280 nasopharyngeal death cases (counting for 74.37%) were recorded in male, 18,707 death cases (counting for 25.63%) were seen in female (sex ratio: 2.90 : 1). In Southeast Asian region, a total of 34,681 new cases (Fig. 1), of which 25,895 cases (counting for 74.67%) and 8,786 cases (counting for 25.33%) were diagnosed in male, and female (sex ratio: 2.95 : 1), respectively, were seen. 22,231 nasopharyngeal death cases were recorded (Fig. 2). Among them, 15,057 death cases and 5,174 death cases were seen in male, female, (ratio: 2.91 : 1) respectively.
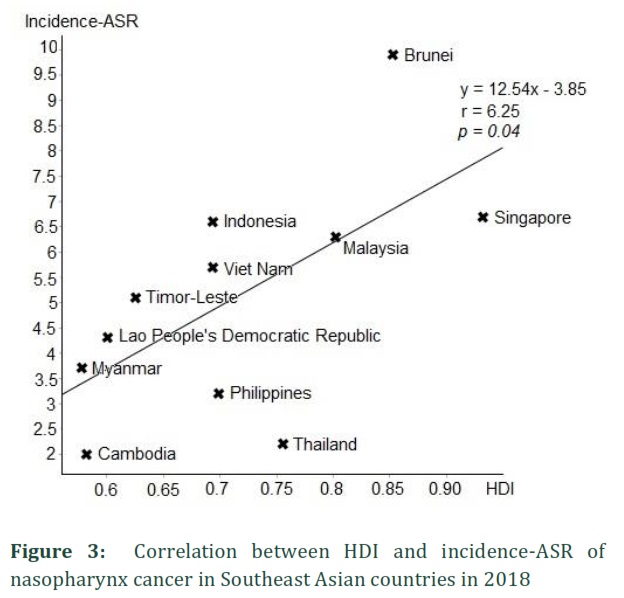
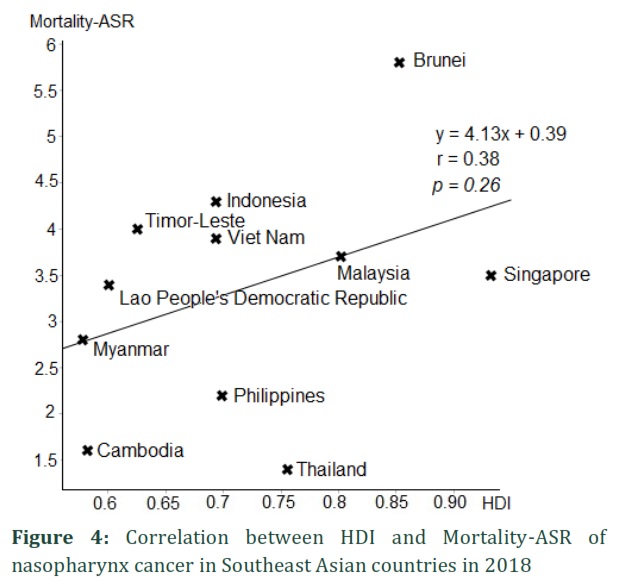
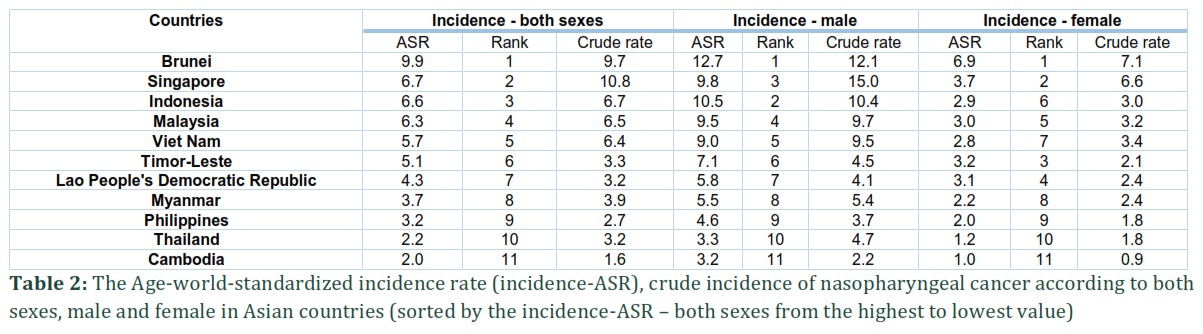
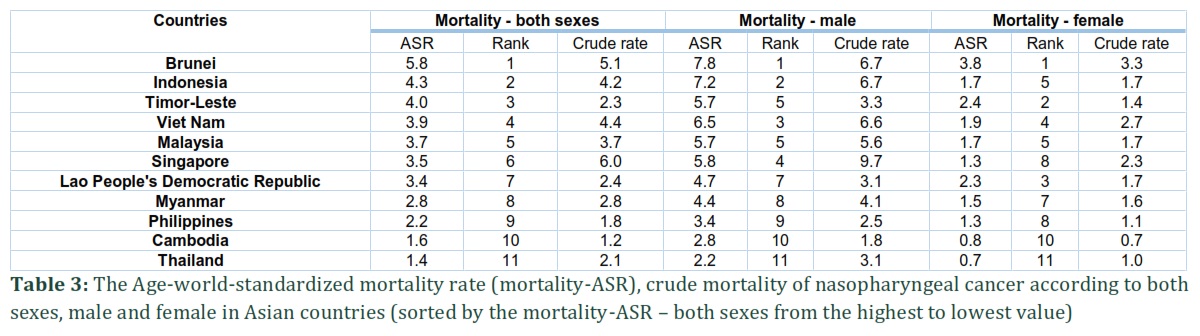
Individually, the incidence and mortality of the Southeast Asian countries according to sex were shown in table 1. Furthermore, the Age-world-standardized incidence rate (incidence-ASR), crude incidence, the Age-world-standardized mortality rate (mortality-ASR), crude mortality of nasopharyngeal cancer according to both sexes, male and female in Asian countries were shown in table 2, table 3. The five countries with the highest standardized incidence rate of nasopharyngeal cancer are as follows: (1) Bruneri: with the highest Incidence-ASR of 9.9 per 100,000 people; (2) Singapore: 6.7 per 100,000 people; (3) Indonesia: 6.6 per 100,000 people; (4) Malaysia: 6.3 per 100,000 people; and (5) Viet Nam: 5.7 per 100,000 people. The five countries with the highest standardized mortality rate of nasopharyngeal cancer are as follows: (1) Bruneri: with the highest mortality-ASR of 5.8 per 100,000 people; (2) Indonesia: 4.3 per 100,000 people; (3) Timor-Leste: 4.0 per 100,000 people; (4) Viet Nam: 3.9 per 100,000 people; and (5) Malaysia: 3.7 per 100,000 people.
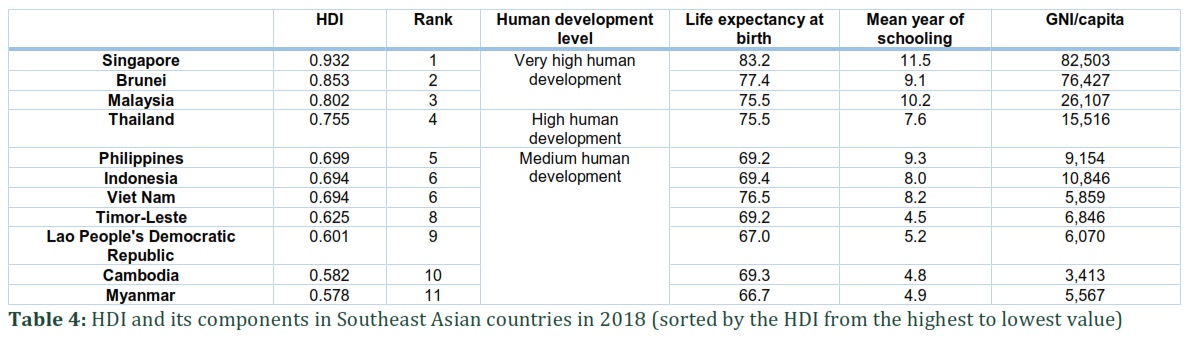
The values of HDI and its components of Southeast Asian countries were shown in table 4. Of them, Singapore is the country with the highest HDI of 0.932. According to HDI, Southeast Asian countries were classified in three categories of human develop level as follow: three countries in very high human develop category, includes Singapore, Brunei, Malaysia; one country in high category, includes Thailand; seven countries in medium category, includes Philippines, Indonesia, Viet Nam, Timor-Leste, Lao People’s Democratic Republic, Cambodia and Myanmar.
Evaluating the association between incidence-ASR, mortality-ASR and HDI
The result of correlation analysis showed the moderate positive correlation between incidence-ASR and HDI (r = 0.625) (Fig. 3, Table 5). This correlation was statistically significant (p = 0.04). In addition, the analysis result showed the weak positive correlation between mortality-ASR and HDI (r = 0.38). However, this correlation was not statistically significant (p = 0.26) (Fig. 4, Table 5). The analyzed results of relationship between incidence-ASR, mortality-ASR with HDI components were shown in Table 5. As the results, there were positive correlation between incidence-ASR, mortality with HDI components, includes Life expectancy at birth, mean year of schooling and GNI/capita. However, only the relationship between incidence-ASR with GNI/capita was statistically significant (p = 0.02).
Figures & Tables

Discussion![]()
Nasopharyngeal cancer is a rare cancer among other populations in the world, except for high incidence and mortality in Asia. Many studies on the etiology of nasopharyngeal cancer have strongly suggested it has a remarkable ethic and distinct geographical distribution [1-5,16,17]. Overall, 34,681 new cases and 22,231 deaths attributed to nasopharyngeal cancer in Southeast Asian countries in 2018. Among them, three highest incidences of nasopharyngeal cancer are as follows: (1) Indonesia: 17,992 cases; (2) Viet Nam: 6,212 cases; (3) Philippines: 2,913 cases. Three highest mortality of nasopharyngeal cancer are as follows: (1) Indonesia: 11,204 cases; (2) Viet Nam: 4,232 cases; (3) Philippines: 1,899 cases. So that, the high incidence of nasopharyngeal cancer in human medium develop counties is higher than high and very high develop countries (Table 1, 4), and this is distributed to environment with a high relative of risk factors related to the carcinogenesis, less budget allocations for health care and public health sectors, includes population incomes, educations and health services [2,3,18]. Due to lack of health service and the diagnosis of most of cases were on the advantage stage, the high mortality was observed more in these areas.
In this study, the significant positive correlation was found between incidence-ASR, mortality-ASR with HDI (Table 5). Notably, based on the HDI, Singapore, Brunei and Malaysia were classified as highly developed countries (HDI ≥ 0.80). However, the higher incidence-ASR, mortality-ASR of those countries were found, compared to other high or medium human develop countries, such as Thailand, Indonesia, Viet Nam, Myanmar, etc. (Table 2, 3; Fig. 3, 4). Among them, Brunei, highest incidence-ASR of 9.9, and mortality-ASR of 5.8 were recorded, compared to the incidence-ASR of 1.5 and mortality-ASR of 0.84. Furthermore, only a significant positive relationship was observed between incidence-ASR with HDI component: GNI/capita. Overall, it could be explained by the greater westernization effect, meant that the tobacco and air pollution were serious, due to the industrialization and consumption [7,19,20]. Additionally, the systems of epidemiological research and record in the medium human development level could be generally less robust, and it remains uncertain whether this observation could be attributed to reporting bias [7,19].
Nasopharyngeal cancer is gravitated to Asian region, includes Southeast Asian countries. The high incidence and mortality were related to medium human development countries, includes Philippines, Indonesia, Viet Nam, Timor-Leste, Lao People’s Democratic Republic, Cambodia and Myanmar. It was significant positive correlation between HDI with incidence-ASR, mortality-ASR. However, this ecological study was focused on the Southeast Asian countries, thus, further studies are recommended in other regions of Asia in order to find out the ecology of nasopharyngeal cancer in Asia.
Authors' Contribution
Both authors contributed equally to this study, drafting and publication of the manuscript.
The authors declare that there is no conflict of interest regarding the publication of this paper.
References![]()
- Tsao SW, Yip YL, Tsang CM, Pang PS, Lau VM, Zhang G, et al. Etiological factors of nasopharyngeal carcinoma. Oral Oncology, (2014); 50(5):
- Mahdavifar N, Towhidi F, Makhsosi BR, Pakzad R, Moini A, Ahmadi A, et al. Incidence and Mortality of Nasopharynx Cancer and Its Relationship With Human Development Index in the World in 2012. World Journal of Oncology, (2016); 7(5-6): 109-118.
- Mahdavifar N, Ghoncheh M, Mohammadian-Hafshejani A, Khosravi B, Salehiniya H. Epidemiology and Inequality in the Incidence and Mortality of Nasopharynx Cancer in Asia. Osong Public Health and Research Perspectives. (2016); 7(6): 360-372.
- Lao TD, Nguyen DH, Nguyen TM, Le TAH. Molecular Screening for Epstein-Barr virus (EBV): Detection of Genomic EBNA-1, EBNA-2, LMP-1, LMP-2 among Vietnamese Patients with Nasopharyngeal Brush Samples. Asian Pacific Journal of Cancer Prevention, (2017); 18(6):1675-1679.
- Lao TD, Le THA. Hypermethylated dna as biomarker for nasopharyngeal cancer detection. Asian Journal of Pharmaceutical and Clinical Research, (2018); 11(9):68-71.
- Chen CJ, Liang KY, Chang YS, Wang YF, Hsieh T, Hsu MM, et al. Multiple risk factors of nasopharyngeal carcinoma: Epstein-Barr virus, malarial infection, cigarette smoking and familial tendency. Anticancer Research, (1990); 10(2B): 547-553.
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. International Journal of Cancer, (2015); 136(5): E359-386.
- Yu MC, Ho JH, Lai SH, Henderson BE. Cantonese-style salted fish as a cause of nasopharyngeal carcinoma: report of a case-control study in Hong Kong. Cancer Research, (1986); 46(2): 956-961.
- Soheylizad M, Khazaei S, Jenabi E, Delpisheh A, Veisani Y. The Relationship Between Human Development Index and Its Components with Thyroid Cancer Incidence and Mortality: Using the Decomposition Approach. International Journal of Endocrinology, (2018); 16(4): e65078.
- Ghislandi S, Sanderson WC, Scherbov S. A Simple Measure of Human Development: The Human Life Indicator. Population and Development Review, (2019); 45(1): 219-233.
- Franceschi S, Wild CP. Meeting the global demands of epidemiologic transition – the indispensable role of cancer prevention. Molecular Oncology, (2013); 7(1): 1-13.
- Kiadaliri AA. Gender and social disparities in esophagus cancer incidence in Iran, 2003-2009: a time trend province-level study. Asian Pacific Journal of Cancer Prevention, (2014); 15(2): 623-627.
- Ghoncheh M, Mohammadian-Hafshejani A, Salehiniya H. Incidence and Mortality of Breast Cancer and their Relationship to Development in Asia. Asian Pacific Journal of Cancer Prevention, (2015); 16(14): 6081-6087.
- Global cancer observatory. Available from: http://gco.iarc.fr/
- Human Development Indices and Indicators: 2018 Statistical Update. Available from: http://hdr.undp.org/en/2018-update.
- Pakzad R, Mohammadian-Hafshejani A, Ghoncheh M, Pakzad I, Salehiniya H. The incidence and mortality of lung cancer and their relationship to development in Asia. Translational Lung Cancer Research, (2015); 4(6): 763-774.
- Thompson LD. Update on nasopharyngeal carcinoma. Head & Neck Pathology, (2007); 1(1): 81-86.
- Young LS, Dawson CW. Epstein-Barr virus and nasopharyngeal carcinoma. Chinese Journal of Cancer, (2014); 33(12): 581-590.
- Thun MJ, DeLancey JO, Center MM, Jemal A, Ward EM. The global burden of cancer: priorities for prevention. Carcinogenesis, 2010; 31(1): 100-110.
- Wong MCS, Lao XQ, Ho KF, Goggins WB, Tse SLA. Incidence and mortality of lung cancer: global trends and association with socioeconomic status. Scientific Reports, (2017); 7: 14300.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0
![]()