

Full Length Research Article
Assessing the life quality in a Moroccan population of diabetics by the General Quality of Life Questionnaire SF36
Fatima Zahra Kehailou*, Mohammed Jabari, Ali Labriji, Souad El Amrani, Said Aatil, Houriya Mestaghanmi
Adv. life sci., vol. 7, no. 4, pp. 270-276, August 2020
*- Corresponding Author: Fatima Zahra Kehailou (Email: fati.kehailou@gmail.com)
Authors' Affiliations
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The quality of life assessment reflects the impact of chronic diseases on patients. The objective of our study is to assess the life quality of diabetic patients and to determine the factors that affect it.
Methods: A cross-sectional study was conducted in 2019 in the Hygiene Service of the Sidi-Othmane district (Casablanca) in 526 diabetic patients. Quality of life was estimated using the SF-36 questionnaire to determine factors that affect mental or physical health. We used Pearson's correlation test for continuous variables and ANOVA for discontinuous variables.
Results: Our patients have an average of life quality considering PCS and MCS respectively (38.47 ± 9.28; 41.15 ± 10.55). Association analyses showed on the one hand associations between the PCS and the gender (p = 0.0001), professional activity (p = 0.0001), marital status (p = 0.0001) and with chronic complications (p = 0.0001). On the other hand, between physical activity and PCS (p = 0.0001) and with MCS (p = 0.0001), between the level of instruction and the PCS and MCS dimensions respectively (p = 0.0001; p = 0.011) between acute complications and PCS and MCS dimensions respectively (p = 0.0001; p = 0.001). The correlation study showed inverse correlations between PCS and age (p = 0.0001), the diabetes duration (p = 0.0001), HbA1c (p = 0.037), and BMI (p = 0.008), and between MCS, and BMI (p = 0.0001).
Conclusion: The presence of one of these factors (female, advanced age, high diabetes duration, complications, and unbalanced diabetes, low level of education, physical inactivity, and professional inactivity) leads to poor life quality.
Keywords: Diabetes; Life quality; Physical health; Mental health
Introduction![]()
Diabetes is a chronic disease recognized as a global epidemic and devastating by its social and economic consequences. It is due either to a genetic or acquired deficiency from the production of insulin by the pancreas, or to resistance to the insulin action. This deficiency causes a chronic increase in blood sugar, which in the long run leads to lesions affecting several devices or systems, especially the vessels and nerves [1]. The global prevalence of diabetes is 463 million according to the International Diabetes Federation (IDF) in 2019. The latter predicts 700 million diabetics by 2045 [2]. In Morocco, the statistics are alarming. In 2016, according to the latest WHO estimates, the prevalence of diabetes reached 12.4% among people aged 20 and over [1]. While in 2018, according to the Ministry of Health, more than 2 million people aged 25 and over have suffered from diabetes and 50% of whom are unaware of their disease [3]. Diabetes is considered one of the deadliest diseases in the world. According to the WHO, one person dies of diabetes every 6 seconds or 1.5 million deaths worldwide, more than AIDS, tuberculosis or malaria [4]. Nationally, the mortality rate from diabetes is 6.3% of all recorded deaths [3]. Unbalanced or unbalanced diabetes is associated with short- and long-term complications. Diabetes is also a major cause of blindness, kidney failure, cardiovascular disease, stroke, and lower limb amputation, according to WHO [1].
Diabetes and its complications are a major economic burden on the patient, his family, and the health care system. According to the International Diabetes Federation, overall health care costs for the treatment of this disease reached USD 727 billion in 2017, an increase of 8% over previous statistics published in 2015 [2]. Diabetes requires a need for ongoing care and follow-up. Its impact is of such magnitude that it affects the patient both physically, psychologically, and emotionally [5]. It is for these reasons that the management of these patients must include not only homeostasis, the treatment of somatic complications, but also the evaluation of individual patient satisfaction which results in an improvement in their quality of life [6].
Quality of life is a new concept defined by WHO as "An individual's perception of his or her place in life, in the context of the culture and value system in which he lives, in relation to his goals and expectations, its standards and concerns"[7]. Quality of life is a multidimensional concept that includes many indicators specifically related to a person’s health, such as satisfaction, freedom of choice, lifestyle, and mental behavior [8,9].This assesses the physical, psychological, and social impact of the disease on the patient’s life. Indeed, the factors that can influence life quality are numerous: age and sex, socioeconomic factors (occupational status, marital status, etc.), the impact of complications and several other factors. They significantly modulate one’s perception of one’s life quality and health [10]. The evaluation of the life quality of diabetics requires an appropriate and validated scale. Several scales of measurement can be used to assess the life quality of diabetics (SF-36 (Short Form 36 items), DQOL (Diabetes Quality Of Life), ADDQoL (Audit Diabetes Dependant Quality of Life) and EQ-5D (EuroQol 5 dimensions). These instruments are increasingly integrated into population surveys.
The Medical Outcome Study-Short Form-36 (SF-36) is one of the generic life quality scales that can be used in clinical practice and research to assess and monitor the health status of the population [11]. It was developed by Warne and Sheirbonen 1992 in the United States [12]. This scale is frequently used in studies and surveys because of its brevity, high reproducibility, validity, and sensitivity to change [13].The SF-36 is a short questionnaire that generates scores on eight health dimensions.
In Morocco, few studies on the life quality of type 1 and type 2 diabetics have been conducted. Thus, this study will allow:
- To follow the progress of the health status of these patients
- To adapt their care, considering the different dimensions of physical and mental health,
- To improve their life quality.
Methods![]()
Type of study
This is a cross-sectional descriptive study through a questionnaire on a population of 526 diabetic patients, enrolled and monitored in the Hygiene Service of the Sidi-Othman district in Casablanca. These diabetic patients receive anti-diabetic medication assistance, as well as weekly follow-up. This locality represents a single district among sixteen in the municipality of Casablanca and has a population of 220,047 inhabitants according to the 2014 general census of the Kingdom of Morocco [14].
At this service, followed diabetics represent 3% of the population of this district. This approximately reflects the real prevalence of diagnosed diabetes in this territory of the municipality of Casablanca (4.9%) [15]. The objective of our work is to assess the life quality of diabetic patients through the SF-36 scale and to measure the impact of different parameters related to diabetic disease.
Study population
Diabetic patients were recruited to the Hygiene Service of the Sidi-Othman district between February and October 2019.
Inclusion criteria
Diabetics over 18 years old recorded and / or monitored by the Hygiene Service of the district of Sidi Othmane and diagnosed for at least one year.
Exclusion criteria
Pregnant women and patients under 18 years old are excluded from this study.
Variables studied
The data was collected using an anonymous questionnaire. Several variables were studied that were grouped into two sections.
The first was socio-demographic, economic, clinical and biological data in addition to those related to the lifestyle
- Socio-demographic data: age, gender, marital status and lifestyle.
- Socio-economic data: the patient's occupation, education level and medical coverage.
- Clinical data: Type of diabetes, diabetes duration, associated pathologies and complications related to diabetes.
- Biological data (HbA1c, FBG, blood pressure). The blood sugar was measured by an extra One Call glucometer. Blood pressure and pulse with an Omron M6 Comfort blood pressure monitor. HbA1c was dosed in private laboratories for medical analysis.
- Health-related data (Physical activity practice and tobacco and alcohol consumption)
The second, related to the evaluation of the quality of life of patients by the SF36 scale. It involves calculating the scores for the dimensions of physical and mental health.
General Quality of Life Questionnaire SF36:
The SF-36 questionnaire is generic. It includes 36 items that are divided into 8 dimensions:
- Physical Functioning or PF
- Role Physical or RP
- BodilyPainor BP
- General Healthor GH
- Vitality or VT
- Social Functioning or SF
- Mental Health or MH
- Role Emotional or RE
Translation and cross-cultural adaptation of the questionnaire
We have made two translations of this scale from French to Moroccan Arabic dialect by two teams of translators fluent in both languages. We then compared the two translations in the presence of investigators not involved in the translation. After discussion, dimension by dimension of the two translated versions, a final version adapted to Moroccan culture was prepared.
The latter was then counter-translated by two teams who spoke French fluently and did not know the original version of the scale. This resulted in two versions which were ultimately compared to the original version.
The pre-final version of the questionnaire was validated on 50 selected diabetic patients, of different age groups and different intellectual levels. Investigators thoroughly discussed all questions with respondents and made sure that they were all understood. After this pre-test, changes were made to the pre-final version, after which the final version was worked out. The questionnaire was administered directly by the investigators to 526 diabetic patients from the Hygiene Service of the Sidi Othmane district (Casablanca), after signing an informed consent and informing the objectives of the study. The proportion of patients who agreed to answer the questionnaire was 98%.
Score calculations
Scores on this scale were calculated according to Ware and his collaborators [12]. According to these authors, the score of each dimension varies from 0 to 100. Scores of 100 indicate good lifestyle and/or good health. On the other hand, a score to 0 indicates poor lifestyle and/or poor health. Several items are grouped together to form the score of each dimension. The dimensions themselves can be grouped together to form a Physical Component Score (PCS) and Mental Component Score (MCS)[16].
Statistical analysis
The IBM SPSS version 23 was used to analyze the data collected. The results were expressed on mean and standard deviation (Mean ±SD) for all the variables studied. The calculation of the different health scores was done using a data sheet that we modeled on MS-Access, which allowed the automatic calculation of scores by dimension (scores between 0 and 100).
To identify the various factors affecting physical (PCS) and mental health (MCS), we studied the association between SF-36 scores and socio-demographic, socioeconomic and clinical characteristics by the ANOVA (Analysis of variance) for continuous
variables and the Pearson test for discontinuous variables. Statistical significance wasp<0.05.
The quotient of the sums of the squares of the factors and of the total deviations (eta-squaredη²) was calculated. It allows to easily defining the association ratio which is always between 0 and 1. The interpretation of this index was made according to Cohen (1988) [17].
Ethical considerations
To respect the ethical dimension, several elements were considered (respect for the anonymity of the questionnaire, informed consent, informing patients of the objectives of the study, discretion in the processing of information). The study was conducted in accordance with the revised Helsinki declarations. It was also approved by the Ethics Committees of Marrakech and Casablanca, Morocco.
Results![]()
Socio-demographic and socio-economic data
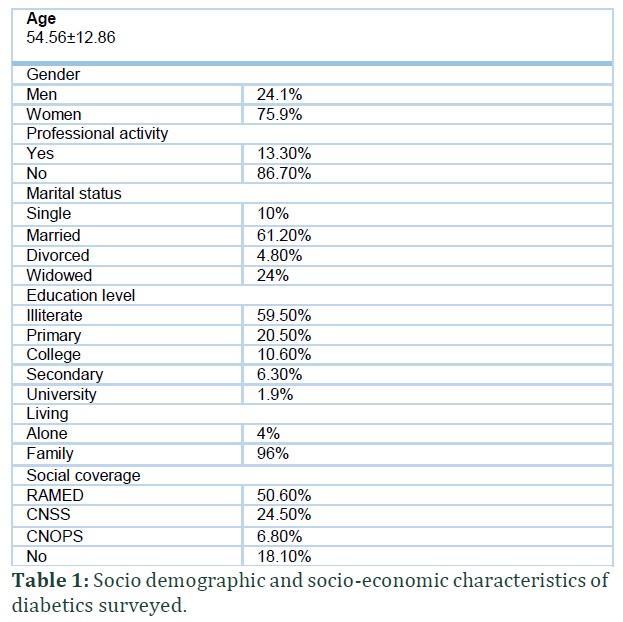
This study involved 526 patients, of whom 75.9% are women and 24.1% are men. The mean age was 54.56 ± 12.86 years. 61.2% of the population were married, 24% widowed, 10% single while only 4.8% were divorced. According to the level of education, 59.5% were illiterate, 20.5% had attended primary school and 16.9% had a secondary level (College: 10.6%; High school: 6.3%), while only 1.9% had completed a university course. In terms of employment, 86.7% of patients were unemployed (without occupation, housewives, retirees and students), compared to 13.3% who are in work. In terms of living, 96% of diabetics lived as a family, while 4% lived alone. For medical coverage, 50.6% had the RAMED, 24.5% had CNSS; 6.8% had the CNOPS and 18.1% of patients had no medical coverage (Table 1).
Clinical, biological and lifestyle data
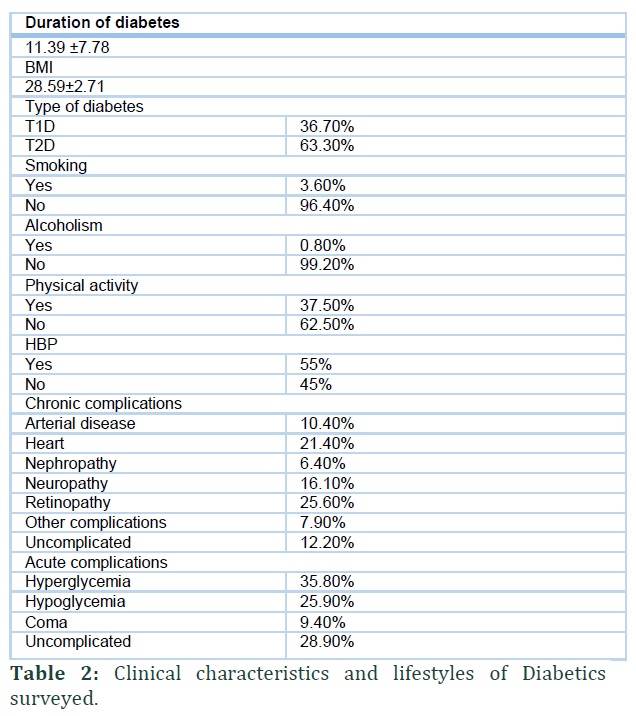
For the clinical characteristics of the population, 63.3% have type 2 diabetes (T2D) and 36.7% have type 1 diabetes (T1D), with an average diabetes duration of 11.39±7.78 years. Mean body mass index (BMI) of the participants was 28.59±2.71kg/m². High blood pressure was present in 55% of diabetics. The most common chronic complication was retinopathy, followed by heart disease, neuropathy, arterial disease, and kidney disease respectively (25.6%; 21.4%; 16.10%; 10.4%; 6.4%). We also noticed that hyperglycemia was the most common acute complication in our diabetics (35.8%) followed by hypoglycemia (25.9%) and coma (9.4%), while 28.90% have no complications (Table 2).
Evaluation of the lifestyle of diabetics by the SF-36
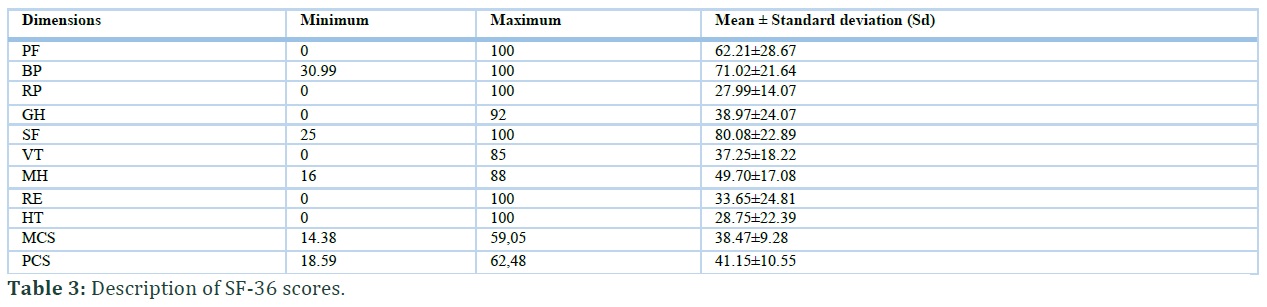
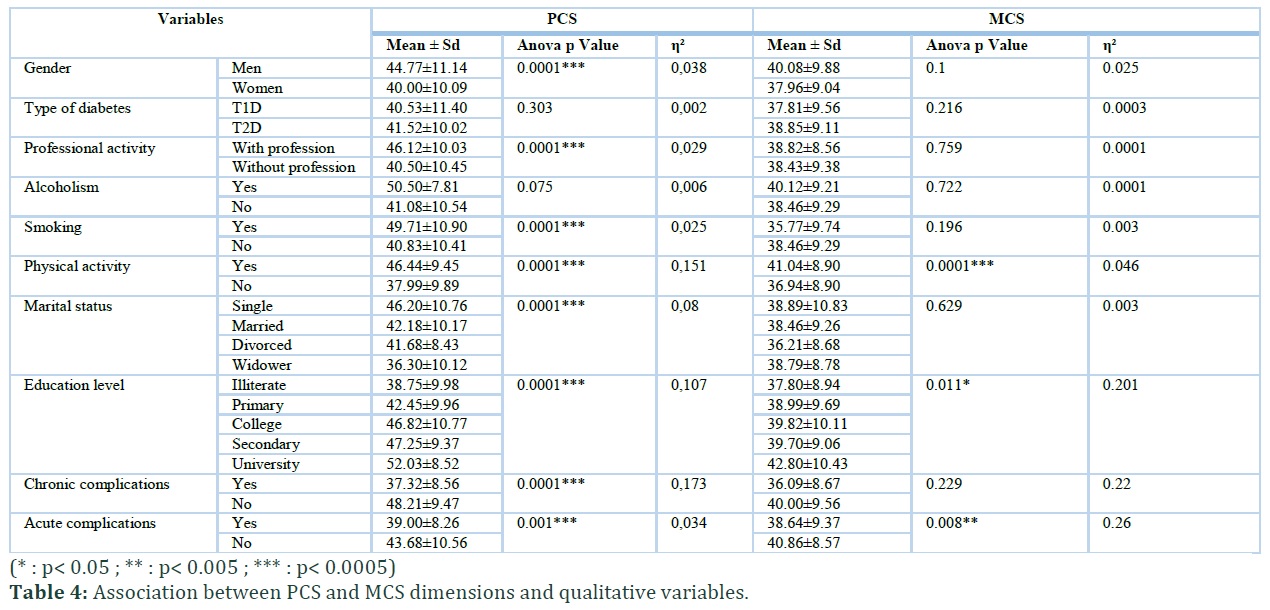
Mean SF-36 scores were: 62.21±28.67for PF, 27.99±14.07 for RP, 33.65±24.81 for RE, 37.25±18.22 for vitality VT, 49.70 ±17.08 for MH, 71.02 ±21.64 for BP, 38.97±24.07for GH, 28.75±22.39 for HT, and 80.08±22.89 SF. For the MCS, the mean was 38.47 ±9.28, with a minimum score of 14.38 and a maximum score of 59.05. For the PCS, the mean was 41.15±10.55, with a minimum score of 18.59 and maximum score of 62.48 (Table 3). The PCS and MCS dimensions of diabetics were associated with physical activity (p = 0.0001; p = 0.0001), educational attainment (p = 0.0001; p = 0.011) and acute complications (p = 0.0001; p = 0.008). The square eta shows a strong association with the PCS and MCS dimensions and the level of education respectively (η² = 0.107, η² = 0.201), with PCS and physical activity (η²= 0.151) and with MCS and acute complications (η² = 0.26). On the other hand, a mean association was observed between MCS and physical activity (η² = 0.046) and between PCS and acute complications (η² = 0.034). In addition, the PCS was weakly associated with gender (p = 0.0001; η² = 0.038), professional activity (p = 0.0001; η² = 0.029), moderately associated with smoking (p = .0001; η² = 0.025) and marital status (p = 0.0001; η² = 0.08) while it is strongly associated with chronic complications (p = 0.0001; η² = 0.173) (Table 4).
The correlation study generally shows an inverse correlation between PCS, age (p = 0.0001; r² = 0.361), the duration of diabetes (p = 0.0001; r² = -0.205), blood pressure (p = 0.001; r² = -0.181) HbA1c (p = 0.037; r² = -0.104) and BMI (p = 0.008; r² = -0.024). Therefore, the more these parameters increase, the more the physical health deteriorates. In contrast, for MCS, we found only the correlation with blood pressure (p = 0.0001; r² = 0.317) and BMI ( p = 0.0001; r² = -0.152 ) (Table 5).
Figures & Tables

Discussion![]()
Although many studies have been carried out to assess the lifestyle of diabetes patients worldwide, in Morocco they are few. In our study, we recruited 526 diabetic patients followed by the Hygiene Service of the Sidi-Othmane district, for the evaluation of their lifestyle. To do this, we used the SF 36 scale, which is considered the most important generic lifestyle instrument for diabetics and allows for two scores: a mental quality score and a quality of physical life score. The physical component score (PCS = 41,15) and the mental component score (MCS = 38.47) of our population are according with the results of Abouothman who assessed the lifestyle of a population of type 2 diabetics residing in the Marrakech region and who observed that the physical and mental summary scores were (PCS = 39.6) (MCS = 38.9)[18]. On the other hand, our results are slightly lower than those observed in metropolitan France by Bourdel-Marchasson (PCS =57.6) [19], in Greece by Papadopoulos(PCS = 60.4; MCS = 64.7) [20] and Sweden by Svedbo-Engstrom (PCS = 48.35; MCS = 49.8) [21].
Our study showed a significant decrease of PCS in diabetic women compared to men (40.00 vs 44.77; p = 0.0001). This result is like that observed by Al-Shehri who reported a PSC score of 47.8 for men and 41.2 for women (p <0.001) [22]. In contrast, the Hanninen study in Finland showed no association between PCS and gender [23].
Many studies have shown that the lifestyle of women with diabetes is more impaired than that of men. It is therefore set that women are more affected by diabetes [24,25]. A similar finding was observed by Shaheen who noted in Pakistan in the hospital setting that the lifestyle of diabetics is significantly associated with sex, and that the general health status of men is more stable than that of women [26].This could be explained by the fact that women tend to have more depression and anxiety compared to men and that they have less confidence in
their ability to manage their disease which tends to have a poor glycemic balance, a greater number of complications and more discomfort concerning leisure [27].
In this study we found that the BMI of our population tend toward obesity, and an inverse correlation between BMI and PCS and MCS scores. This shows that an increase in BMI leads to a deterioration in the quality of life. In addition, Murray reported that in general, obese patients tend to decrease their quality of life compared to those of non-obese [28]. A similar result was observed by Eckert who noticed that patients with type 2 diabetes and grade 2 obesity have a lower lifestyle than overweight and obese grade 1 patients [29].
The age of the patient and the duration of diabetes are found to be associated with decreased lifestyle in diabetics. In this study, patients with longer duration of diabetic and / or older age had weaker PCS scores (p = 0.0001; r² = -0.205; r² = -0.361). Similar results were observed by Woodcock and Gulliford in England who found that the increasing duration of diabetes was related to the deterioration in scores for most dimensions of the SF-36 [30,31]. In addition, Shaheen observed a better physical score in 2014 in men aged 40 years and in diabetics with duration of diabetes of 5 to 10 years [26].
In our study, we observed a significant increase (p = 0.0001) in PCS and MCS quality of life scores. The practice of physical activity could therefore be as an improving factor in the lifestyle of diabetics. A similar result was observed by Eckert who noticed that quality of life decreased with decreased physical activity practice in all scores of SF-36 [29]. In addition, Al-Shehri and collaborators found that 30 minutes of physical exercise for 3 days or more each week produced positive changes in most dimensions of SF-36 and much more with the mental dimension MCS [22].
We found an association between the PCS and professional activity (p = 0.0001), and on the other hand between the level of education and the PCS and MCS scores (p = 0.0001; p = 0.011). This result is according with that of Larsson and Clouet who showed that low socio-economic status due to inactivity and low level of education (illiterate people) is associated with poor lifestyle [32,33].
In our study, we showed an association between PCS and marital status (p = 0.0001), the lowest scores were observed in divorcees and widowers in both sexes. It therefore looks that marital status could be a good predictor of health status. Several authors have suggested the association between these two factors. A better lifestyle is associated with a decrease in mortality and allows for good marital relationships, thereby reducing the chance of rupture [34].
In our study, to measure the increased level of HbA1c, there was a decrease in the quality of life in our study for the PCS (p = 0.037). The results of an American study confirm our results, with higher SF-36 scores in those with low HbA1c levels than in those with high HbA1c levels [35].
A highly significant association was observed between lifestyle and complications of diabetes (chronic and acute) on the PCS (p = 0.0001; p = 0.001). For MCS, the association is found only for acute complications. According to several studies that revealed that diabetic patients had poor lifestyle compared to non-diabetic patients [36,37].
Our study showed a higher prevalence of cardiovascular disease, retinopathy, hypertension, neuropathy and kidney disease. These results are according with those of Al-Shehri which showed that complications of diabetes were reported in 72.6% of cases, 13.9% with cardiovascular disease, 22.2% with hypertension, and 47.2% with retinopathy [22]. Although Lloyd has shown that the slight presence of complications in diabetics has a significant impact on lifestyle [38]; this could be explained by the lack of health education, awareness and patient care.
We also observed an association between HTA and PCS and MCS scores respectively (p = 0.001; p = 0.0001), a similar result was observed by Shaheen who noted that VT was better in non-hypertensive subjects compared to hypertensive subjects [26].
This study provides important data on the quality of life of diabetics, thus establishing reference points for future comparisons with other patient groups. Nevertheless, she presents some limitations, mainly related to the cross-sectional nature of the study which limits the causal interpretation of the results. It was also conducted in a single center, which may limit its generalizability. It is therefore desirable to do others large-scale studies, to properly assess the quality of life of Moroccan diabetics. In parallel to the statistical tool, lifestyle assessment tools (generic or specific) help to understand and highlight the factors influencing this parameter and to help take appropriate corrective action. For example, our study showed that our diabetic patients have an average lifestyle by considering both MCS and PCS scores on the SF-36. Factors that significantly decrease their lifestyle are: Women, advanced age, physical inactivity, inactivity, low level of education, duration of diabetes, glycemic imbalance, as well as complications.
Treating physicians must therefore take all these factors into account so that they can improve the care of their patients and achieve better control of their diabetes and promote a better lifestyle by creating care and rehabilitation services that are still scarce.
Authors' Contribution
Fatima Zahra Kehailou: conception, follow-up of diabetics, data collection and capture, analysis, and interpretation of results, writing of the manuscript.
Mohammed Jabari: therapeutic follow-up of diabetics, conception, analysis, and interpretation of the results, writing and validation of the final version of the manuscript.
Houriya Mestaghanmi: conception, analysis, and interpretation of the results, writing and validation of the final version of the manuscript.
Ali Labriji: statistical analysis of data, interpretation of results.
Souad El Amrani: interpretation of the results, validation of the final manuscript
Said Aatil: data collection.
All the authors contributed to the conduct of this work. All authors also state that they have read and approved the final manuscript
The authors declare that they have no competing interests.
Acknowledgement
This work would never have been possible without the precious help of Borough Council President Sidi Othmane and the staff of his Hygiene Service. We would also like to thank the students of the Faculty of Sciences ben M'Sik for having contributed to the realization of the survey on the quality of life of diabetics.
References![]()
- World Health Organization WHO. Global report on diabetes, (2016) [Online]. Available: https://apps.who.int/iris/handle/10665/204871
- Atlas Diabetes. International Diabetes Federation IDF, 9th edn. Brussels, Belgium, (2019) [Online]. Available: https://www.diabetesatlas.org/
- Ministry of health. Communiqué: Célébration de la journée mondiale du diabète, Morocco, (2016) [Online]. Available: https://www.sante.gov.ma/Pages/Communiques.aspx?IDCom=165
- Atlas Diabetes. International Diabetes Federation IDF, 8th edn. Brussels, Belgium, (2017) [Online]. Available: https://www.idf.org/e-library/epidemiology-research/diabetes-atlas/134-idf-diabetes-atlas-8th-edition.html
- Lyhyaoui O (2011) Evaluation de la qualité de vie liée à la santé chez les diabétiques de type 2: University Sidi Mohammed Ben Abdellah. Faculty of Medicine and Pharmacy, Fes, Morocco
- Azanmasso H, Tchonda E, Alagnide E, Lahrabli S, Diagne N-S, et al. Qualité de vie des patients diabétiques en Afrique : à propos d’une étude bi-centrique. Médecine des Maladies Métaboliques, (2015); 9(6): 603-609.
- Group W. Study protocol for the World Health Organization project to develop a Quality of Life assessment instrument (WHOQOL). Quality of Life Research, (1993); 2(2): 153-159.
- Ware JE, Gandek B. Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project. Journal of Clinical Epidemiology, (1998); 51(11): 903-912.
- Alonso J, Ferrer M, Gandek B, Ware JE, Aaronson NK, et al. Health-related quality of life associated with chronic conditions in eight countries: Results from the International Quality of Life Assessment (IQOLA) Project. Quality of Life Research, (2004); 13(2): 283-298.
- El Emrani L, Bendriss A, M S. Assessment of health-related quality of life in the population of Tetouan (Morocco) using the SF-36: the influence of level of education and marital status. International Journal of Innovation and Applied Studies. International Journal of Innovation and Applied Studies (2014); 7(2): 815-822.
- Brazier JE, Harper R, Jones NM, O'Cathain A, Thomas KJ, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. British Medical Journal, (1992); 305(6846): 160-164.
- Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Medical Care, (1992); 30(6): 473-483.
- Ware JE, Jr., Gandek B, Kosinski M, Aaronson NK, Apolone G, et al. The equivalence of SF-36 summary health scores estimated using standard and country-specific algorithms in 10 countries: results from the IQOLA Project. International Quality of Life Assessment. Journal of Clinical Epidemiology, (1998); 51(11): 1167-1170.
- Office of the High Commissioner of the plan (HCP). General population and Habitat census note of presentation of the first results., greater Casablanca region, Kingdom of Morocco, (2014). [Online]. Available: https://www.HCP.Ma/reg-Casablanca/attachment/673642/.
- National Fund of social welfare agencies (Cnops).Etude surla population diabétique assurée par la CNOPS(2008-2013) Kingdom of Morocco, Department of studies and Actuariate, (2014). [Online]. Available: http://www.cnops.org.ma/sites/default/files/Etude_Diabete_periode_2008_2013_CNOPS.pdf.
- Ware JE, Snow KK, Kosinski M, Gandek B, New England Medical Center H, et al. SF-36 health survey : manual and interpretation guide. Health Institute, New England Medical Center, Boston. (1993).
- Cohen J. Statistical Power Analysis for the Behavioral Sciences (2e édition). Hillsdale, New Jersey : Lawrence Erlbaum Associates. (1988). .
- Abouothman S (2014) Évaluation de la qualité de vie des patients diabétiques de type 2 au niveau de la région de Marrakech: University Cadi Ayyad, Faculty of Medicine and Pharmacy, Marrakech, Morocco.
- Isabelle Bourdel-Marchasson, Aurore Tulon, Marie-Line Erpelding, Pierre Lecomte, Patrick Vexiau, et al. Quality of life in type 2 diabetic patients living in metropolitan France: multiple factors associated. ENTRED 2007. Bulletin Epidémiologique Hebdomadaire, (2001); 2(25): 15-20.
- Papadopoulos AA, Kontodimopoulos N, Frydas A, Ikonomakis E, Niakas D. Predictors of health-related quality of life in type II diabetic patients in Greece. BMC Public Health, (2007); 7186.
- Svedbo Engström M, Leksell J, Johansson U-B, Borg S, Palaszewski B, et al. Health-related quality of life and glycaemic control among adults with type 1 and type 2 diabetes – a nationwide cross-sectional study. Health and Quality of Life Outcomes, (2019); 17(1): 141.
- Al-Shehri AH, Taha AZ, Bahnassy AA, Salah M. Health-related quality of life in type 2 diabetic patients. Annals of Saudi Medicine, (2008); 28(5): 352-360.
- Hänninen J, Takala J, Keinänen-Kiukaanniemi S. Quality of life in NIDDM patients assessed with the SF-20 questionnaire. Diabetes Research and Clinical Practice, (1998); 42(1): 17-27.
- Senez B, Felicioli P, Moreau A, Goaziou M-FL. Quality of life assessment of type 2 diabetic patients in general medicin. Presse Médicale, (2004); 33(3): 161-166.
- Kazemi-Galougahi MH, Ghaziani HN, Ardebili HE, Mahmoudi M. Quality of life in type 2 diabetic patients and related effective factors. Indian Journal of Medical Sciences (2012); 66(9-10): 230-237.
- Shaheen F, Basit A, Riaz M, Fawwad A, Hakeem R, et al. Assessing health related quality of life in diabetic subjects by SF 36 questionnaire in a tertiary care diabetes unit of Karachi, Pakistan. . International Journal of Advanced Research, (2014); 6(6): 13-17.
- Moreau A, Senez B, Felicioli P, Goaziou M-FL. Évaluation de la qualité de vie des patients diabétiques de type 2 en médecine générale. Presse Médicale, (2003); 17(608): 1-5.
- Finkelstein MM. Body mass index and quality of life in a survey of primary care patients. Journal of Family Practice, (2000); 49(8): 734-737.
- Eckert K. Impact of physical activity and bodyweight on health-related quality of life in people with type 2 diabetes. Diabetes, Metabolic Syndrome and Obesity, (2012); 5303-311.
- Woodcock AJ, Julious SA, Kinmonth AL, Campbell MJ. Problems with the performance of the SF-36 among people with type 2 diabetes in general practice. Quality of Life Research, (2001); 10(8): 661-670.
- Gulliford MC, Mahabir D. Relationship of health-related quality of life to symptom severity in diabetes mellitus: a study in Trinidad and Tobago. Journal of Clinical Epidemiology, (1999); 52(8): 773-780.
- Larsson D, Lager I, Nilsson PM. Socio-economic characteristics and quality of life in diabetes mellitus–relation to metabolic control. Scandinavian Journal of Public Health, (1999); 27(2): 101-105.
- Clouet F, Excler-Cavailher G, Christophe B, Masson F, Fasquel D. [Type 2 Diabetes and Short Form 36-items Health Survey]. Diabetes & Metabolism, (2001); 27(6): 711-717.
- Ikeda A, Iso H, Toyoshima H, Fujino Y, Mizoue T, et al. Marital status and mortality among Japanese men and women: the Japan Collaborative Cohort Study. BMC Public Health, (2007); 773.
- Liu H. Till Death Do Us Part: Marital Status and U.S. Mortality Trends, 1986 – 2000. Journal of Marriage and Family, (2009); 71(5): 1158-1173.
- Wee HL, Cheung YB, Li SC, Fong KY, Thumboo J. The impact of diabetes mellitus and other chronic medical conditions on health-related Quality of Life: is the whole greater than the sum of its parts? Health Qual Life Outcomes, (2005); 32.
- Poljicanin T, Ajduković D, Sekerija M, Pibernik-Okanović M, Metelko Z, et al. Diabetes mellitus and hypertension have comparable adverse effects on health-related quality of life. BMC Public Health, (2010); 1012.
- Lloyd A, Sawyer W, Hopkinson P. Impact of long-term complications on quality of life in patients with type 2 diabetes not using insulin. Value Health, (2001); 4(5): 392-400.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0

