

Full Length Research Article
Analysis of single nucleotide polymorphisms encompassing toll-like receptor (TLR) -7 (rs179008) and (TLR)-9 (rs352140) in systemic lupus erythematosus patients
Muhammad Adil Bashir1, Nadeem Afzal2, Hamdan Hamid1*, Muhammad Kashif1, Alishba Niaz3, Shah Jahan2
Adv. life sci., vol. 8, no. 2, pp. 103-107, February 2021
*– Corresponding Author: Hamdan Hamid (Email: kh.hamdan99@gmail.com )
Authors' Affiliations
2. University of Health Sciences, Lahore – Pakistan
3. Shaikh Zayed Medical College, Lahore – Pakistan
Editorial Note on Version of Record
This article has been corrected. See https://doi.org/10.62940/als.v13i0.4214 for more information.
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Multiple documentary evidence comprising genome wide association studies have established association of TLR7 and TLR9 gene polymorphisms with systemic lupus erythematosus (SLE). Present study was aimed to deduce and compare single nucleotide polymorphism (SNP) in TLR7 (rs179008) and TLR9 (rs352140) genes between local population of SLE patients and healthy controls.
Methods: A case control study; blood samples from 80 controls (Group1) and 80 SLE subjects (Group2) were collected in EDTA tubes and processed for the analysis of gene polymorphism of TLR7 (rs179008) and TLR9 (rs352140) by PCR-RFLP after DNA extraction. Complete blood counts were also determined. Statistical analysis was carried out using Chi-square test for SNPs analysis and allele frequencies between two groups. TLR 7 and TLR 9 genes polymorphism with SLE alongside clinical parameters were assessed.
Results: Genotypes of TLR7, AT and TT are not significantly associated with SLE. Whereas, TLR9 CT and TT genotypes, especially T allele are significantly associated with SLE reflecting noticeable interdependence of TLR9 gene polymorphism with respect to SLE subjects.
Conclusion: TLR9 (rs352140) gene variation might be a key factor to etiology and pathogenesis of SLE.
Keywords: Toll-like receptors; Restriction site; Single nucleotide polymorphism; Systemic lupus erythematosus
Introduction![]()
Systemic lupus erythematosus (SLE) is an autoimmune disease where autoantibodies are produced against self-nuclear and cytoplasmic constituents; specifically double stranded DNA (dsDNA). Autoantibodies react with self-antigens and form immune complexes which get deposited in tissues resulting in inflamed organs such as kidneys, joints, central nervous system, etc [1]. Worldwide it is more prevalent in females than males with a ratio of 9:1 [2].
Several environmental factors e.g. particulates in air pollution, ultraviolet light, infection and cross reactivity of antibodies with self-antigens lead to development of SLE [3]. Inappropriate regulation of lymphocyte production leads to a state of immunological hyperactivity that further converts to SLE [4]. Clearance of immune complexes, APC (antigen presenting cell), B cells, T cells signal transduction and toll-like receptors (TLRs)/interferon signaling pathways are three well established immunological pathways which account for the pathological process of SLE [3] [5,6].
Range of ligands including proteins, lipids and nucleic acids derived from both micro-organisms and endogenous tissues are recognized by TLR. After interaction with specific ligands, TLRs signal via recruitment of specific adapter protein channels. Those adapter proteins interact with interleukin 1 receptor domain that initiates a series of other signaling pathways followed by transcription activation factors that trigger gene expression of pro-inflammatory chemokines and cytokines as well as interferon regulatory factors [7,8]. Hyper activation of these receptors has been attributed to the pathogenesis of autoimmune disorders [9]. Ten human (TLR1 to TLR10) and twelve murine TLRs (TLR1 to TLR9, TLR11, TLR12 and TLR13) have been characterized [10]. Mice and human TLR7 and TLR9 are linked with autoimmune disorders e.g. SLE [11]. TLR7 and TLR9 recognize ssRNA and nonmethylated cytosine–phosphate–guanine (CpG) dinucleotide motifs located in bacterial, viral and fungal DNA [12,13]. Defective interferon/TLR signaling pathways induce immune complexes comprising of self-nucleic acid to interact with TLR7 and TLR9 within plasmacytoid dendritic cells and B cell endosomes leading to the secretion of type 1 interferon and (IL)-6 [14]. The combined activation of both B cell receptor and TLR leads to the proliferation of auto-reactive B-cells. Subsequent differentiation into plasmablasts and plasma cells result in secretion of autoantibodies [15].
The findings of various studies on TLR polymorphism and SLE are inconsistent and up to the best of our knowledge, there was no study from Pakistan on TLR in account to SLE. Therefore, present study was designed to determine TLR 7 (rs179008) and TLR 9 (rs352140) polymorphisms in SLE patients.
Methods![]()
It was a case control study that included age and gender matched 80 healthy individuals as controls (group 1) and 80 SLE patients (group 2). The study was approved by the ethical review committee of Fatima memorial hospital Lahore and University of Health Sciences (UHS) Lahore. It was carried out in the department of immunology at UHS. After the informed consent samples were collected from the patients who appeared in rheumatology clinic of Fatima memorial hospital and controls were recruited from healthy population of UHS. Convenaient sampling technique was applied.
Group I: Apparently, healthy controls.
Group II: SLE patients.
Inclusion criteria :
Control:
- Both male and female between 18-60 years of age.
- Healthy individuals.
Patients:
- Both male and female between 18-60 years of age.
- Diagnosed SLE patients based on ACR diagnostic criteria.
Exclusion criteria:
Subject with recent history of infection in last two weeks.
- Patients with autoimmune disease other than SLE
- Other chronic conditions (Diabetes mellitus)
- Malignancy
Sample processing and genotyping
DNA extraction from whole blood was carried out in the department of immunology UHS, Lahore. Complete blood counts were performed on sysmex XE-2100 instrument while ESRs were estimated on vesmatic cube30 instrument.
Extraction of DNA from whole blood was carried out using phenol and chloroform method [16]. Extracted DNA samples were stored at -20˚C until further processing. Polymorphism analysis of TLR7 (rs179008) and TLR9 (rs352140) was performed by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP). Primer pairs for TLR7 and TLR9 F:5′ TAACAACGAATAGGAAAATGC 3′, R:5′ GTTTTAGGAAACCATCTAGCC 3′ and F: 5′-GCAGCACCCTCAACTTCACC -3′, R: 5′-GGCTGTGGATGTTGTTGTGG -3′ were used for PCR respectively. PCR-amplified fragments of TLR7 were comprised of 369 base pairs (bp) and TLR9 possessed 360bp in length. Polymorphism analysis of TLR7 and TLR9 was conducted and genotype was assessed by restriction digestions of all the amplified DNA products with N1aIII and BstUI enzymes at 37ºC for 4 hours. Digested PCR products were electrophoresed on 1.5% TAE agarose gel for 40 minutes (90 volts) and visualized by ethidium bromide staining under UV. The digested product of TLR7 had 3 genotypes (AA), (AT), (TT) and similarly TLR9 had 3 genotypes (TT), (CC), (CT). TLR7 A allele was cleaved into 243bp and 126bp fragments while TLR7 T allele remained uncut. TLR9 C allele was cleaved into 227bp and 133bp fragments. TLR9 T allele remained uncut.
Statistical analysis
Statistical analysis was performed using SPSS version 20. Mean ± SD was given for quantitative variables such as age and hemoglobin. Using Chi-square test; polymorphisms were tested for deviation from Hardy–Weinberg equilibrium by comparing the observed and expected genotype frequencies. For SNP analysis, genotype and allele frequencies of TLR7 and TLR9 were compared between groups by Chi-square test, odds ratios (OR) and confidence intervals (CIs) were calculated using logistic regression. A p-value ≤ 0.05 was considered as statistically significant.
Results![]()
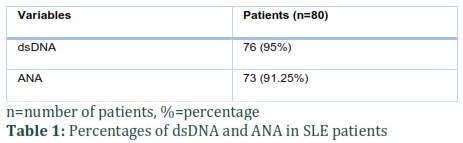
Subjects with SLE had mean (± SD) age of 30.72±7.77 years almost similar to the controls 30.70±7.65 years. Comparatively, there was no statistically significant difference between two groups (p=0.984). Among SLE patients 73 (91.25%) were positive for ANA whereas, 76 (95%) were positive for anti dsDNA antibodies: which is suggestive of diagnostic efficacy of anti dsDNA assay (Table 1).
Levels of hemoglobin in group 1 (controls) and group 2 (SLE patients) were 14.1 g/dl and 11.4g/dl respectively; statistically significant difference was detected (p<0.0001). The level of ESR was high in SLE patients (52.5 mm/hour) compared to controls (13.0 mm/hour) and there was statistically significant difference between the two groups (p<0.0001).
Polymorphism of TLR7 and TLR9 in SLE patients:
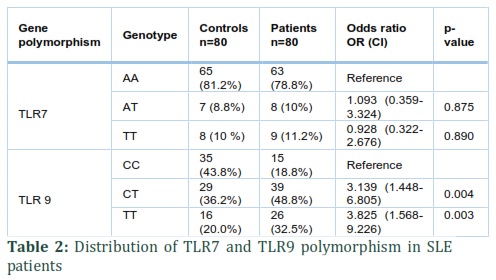
OR of TLR7 polymorphism for AT genotype was 1.093 and for TT it was 0.928 and no statistically significant association was found with respect to AT and TT genotypes with SLE (p=0.875 and TT=0.890 respectively). There was no significant association of TLR7 polymorphism with SLE (Table 2).
The OR of TLR9 polymorphism for CT genotype was 3.139 (95% confidence interval, p= 0.004) and for TT genotype it was 3.825 (95% confidence interval, p=0.003) which indicates that individuals with CT genotype of TLR9 polymorphism are three times, and those with TT genotype are almost four times more prone to develop SLE.
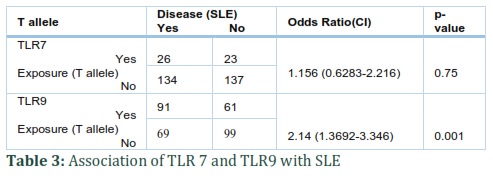
Association of T allele (TLR7 and TLR9) with SLE:
There is no statistically significant association (p=0.75) and presence of T allele is not associated with the onset of SLE in TLR7 (OR of 1.156 and confidence interval 0.6283-2.216). However the presence of T allele is positively associated (p=0.001) with the onset of SLE in TLR9 (OR: 2.14 and confidence interval: 1.3692-3.346) (Table 3).
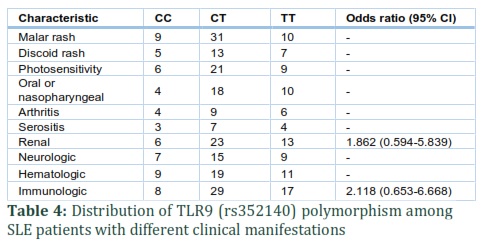
TLR9 (rs352140) polymorphism with different clinical manifestations of SLE:
Among patients with renal manifestation, frequency of CT and TT genotype was 23 and 13 respectively and it was associated with these genotypes but not significant (OR=1.862 [0.594-5.839]). Similarly, among patients with immunological manifestations, frequency of CT and TT genotype was 29 and 17 respectively and showed no association with these genotypes (OR=2.118 [0.653-6.668]) (Table 4).
Figures & Tables
Discussion![]()
In this study the relationship between two SNPs encoding genes i.e. TLR7 and TLR9 with occurrence of SLE was investigated. Mean (± SD) age of SLE subjects was 30.72 ± 7.77 which was in agreement with Rabbani et al, who reported mean age of 31 years [17]. Rubtsov et al, studied over expression of the genes mediating the formation of B Cells from partially non-ionized parts of the X chromosome known to contribute to the development of autoimmune condition in females [18].
In the present study ANA was detected in 91.25 % whether anti ds DNA antibodies were more frequent (95%) among diagnosed study subjects: which is suggestive of diagnostic efficacy of anti-ds DNA. Aforementioned study is in conformity with the study of Solangi et al, who documented 88.3% ANA in SLE patients. They also stated 96.81 % of anti dsDNA antibodies in SLE patients which is also supportive to the present study [19].
In the current study, hemoglobin in group I was 14.1 g/dl which is in normal range. The level of hemoglobin was 11.4g/dl in group II. These finding are in accordance with Voulgarelis et al, who reported hemoglobin as 9 to 11 g/dl [20]. Lam and Quah, deduced that low hemoglobin levels can be caused by impaired erythropoietin production by kidneys, loss of gastro-intestinal blood due to anti-inflammatory therapy, increased red cell destruction from hypersplenism or a drug-induced immune phenomenon [21].
Frequency of TT in group II was 26 (32.5%) whereas in group I it was 16 (20%), OR (95% CI) =3.825 (1.586-9.226), and p= 0.003. The frequency of CT in group II was 39 (48.8%) while in group I it was 29 (36.2%), OR (95%CI) =3.139 (1.448-6.805), and p=0.004. Increased OR was observed in SLE patients with TT compared to CC, which means that patients possessing T allele might be at risk for developing SLE. It supports Zhang et al, who reported TLR9 (rs351240) TT genotype, minor allele T and haplotype H3 increases susceptibility to SLE in northern Chinese population [22]. Xu et al, also documented that individuals with T allele at TLR9 (rs352140) have increased risk of SLE [23]. Another study by Nakano et al, divulged that extent of TLR9 mRNA in B cells was raised in SLE patients [24]. Piotrowski et al, showed that TLR9 (rs352140) polymorphism was not associated with SLE in Polish population [25]. Huang et al, showed polymorphism of TLR9 (rs187084) that is located in LD block with (rs352140) is associated with SLE in Taiwanese patients [26]. Similarly a study by Xu and Mu et al, revealed significant association of TLR9 (rs352140) with the susceptibility to SLE in Chinese population. They revealed high expression of TLR9 in SLE patients who had anti dsDNA antibody than patients who did not possess these antibodies [23,27]. A meta-analysis update by Lee et al, in Asian population projected association of TLR9 (rs352140) with SLE [28]. Elloumi et al, illustrated significant association of TLR9 (rs352140) with lupus nephritis patients [29].
Zhou et al, did not find a significant contribution of the TLR9 (rs352140) polymorphism to SLE development in Chinese Han population [30]. Moreover, a meta-analysis study in African, Asian and Caucasian cohorts by Lee et al, reflected lack of association between TLR9 (rs352140) alleles and SLE [31].
Patients displaying T/T and T/C genotypes are at substantial risk of acquiring renal disease in SLE. The study is in agreement with Piotrowski et al, who also established the same results [25]. Zhou and Piotrowski et al, observed that patients having same genotypes are at risk of developing renal disease. They also suggested TLR9 T/T and T/C genotypes are significantly related with immunological disorders and presence of anti-dsDNA antibodies in SLE patients [25,30]. Furthermore, Elloumi et al, illustrated significant association of TLR9 (rs352140) genotypes with renal manifestation as congruent with our findings [29]. The conflicts and deviations in the impressions of TLR9 polymorphisms and development to SLE alongside clinical expressions in several populations may be due to multiracial heterogeneity and vulnerability of population to different environmental factors.
Sanchez et al, Enevold et al, emphasized the role of TLR7 gene in the development of SLE. However, present study is in agreement with Sánchez et al, who conducted a case control study of 1107 healthy controls and 753 SLE patients and observed no association of TLR7 (rs179008) polymorphism with SLE in Spanish population [32,33]. Conversely, this study is not in agreement with Santos et al, who proved that T allele on the same loci remarkably raised the risk of SLE in Brazilian population [34]. That variation in result can be due to factors ranging genetic backgrounds, sample size and study designs.
This study is significant in the way that the findings are in particular to our local Pakistani cohorts and it will open a gateway for further understanding of disease pattern and advancements within this particular domain. SNP in TLR9 gene (rs351240) is associated with SLE while SNP in TLR7 (rs179008) is not associated with SLE in Pakistani population. Those findings may incorporate in better understanding of etiology and pathogenesis of SLE.
Limitation
We were unable to consider more study subjects due to time and financial constraints.
Author Contributions
Muhammad Adil Bashir: Study design, sample processing and analysis
Nadeem Afzal: Co-Supervisor and lead facilitator
Hamdan Hamid: Sample acquisition, processing and documentation
Muhammad Kashif: Results and discussion
Alishba Niaz: Statistical analysis
Shah Jahan: Result interpretation as principal investigator
The author declares that there is no conflict of interest regarding the publication of this paper.
References![]()
- Mortezagholi S, Babaloo Z, Rahimzadeh P, Namdari H, Ghaedi M, Gharibdoost F, et al. Evaluation of TLR9 expression on PBMCs and CpG ODN-TLR9 ligation on IFN-α production in SLE patients. Immunopharmacology and Immunotoxicology (2017); 39(1):11-8.
- Falasinnu, T, Chaichian, Y, Bass MB and Simard, JF. The representation of gender and race/ethnic groups in randomized clinical trials of individuals with systemic lupus erythematosus. Current rheumatology reports, (2018); 20(4): 20.
- Cha, HC, Chua, KH, Lim, SK and Phipps. ME. Insight into gene polymorphisms involved in toll-like receptor/interferon signalling pathways for systemic lupus erythematosus in South East Asia. Journal of Immunology Research, (2014); 529167.
- Wang, D, Zhang C, Zhou Z and Pei F. TLR9 polymorphisms and systemic lupus erythematosus risk: an update meta-analysis study. Rheumatology International, (2016); 36: 585.
- Devaraju P, Gulati R, Antony PT, Mithun CB, Negi VS. Susceptibility to SLE in South Indian Tamils may be influenced by genetic selection pressure on TLR2 and TLR9 genes. Molecular Immunology, (2015); 64(1): 123–126.
- Zhang J, Zhu Q, Meng F, Lei H, Zhao Y. Association study of TLR-9 polymorphisms and systemic lupus erythematosus in Northern Chinese Han population. Gene, (2014); 533: 385-388.
- Kieser KJ, Kagan JC. Multi-receptor detection of individual bacterial products by the innate immune system. Nature Reviews Immunology, (2017); 17(6): 376-90.
- Kawai T, Akira S. TLR signaling. Seminars in Immunology, (2007); 19: 24–32.
- Takeda K, Kaisho T, and Akira S. Toll-like receptors. Annual Review of Immunology, (2003); 21:335–376.
- Dhupal M, Oh JM, Tripathy, DR, Kim, SK, Koh, SB and Park, KS. Immunotoxicity of titanium dioxide nanoparticles via simultaneous induction of apoptosis and multiple toll-like receptors signaling through ROS-dependent SAPK/JNK and p38 MAPK activation. International journal of nanomedicine, (2018); 13: 6735
- Weidenbusch M, Kulkarni OP and Anders HJ. The innate immune system in human systemic lupus erythematosus. Clinical Science, (2017); 131(8): 625-634.
- Ramirez-Ortiz ZG, Specht CA, Wang JP, Lee CK, Bartholomeu DC, Gazzinelli RT, et al. Toll-like receptor9-dependent immune activation by unmethylated CpG motifs in Aspergillus fumigatus DNA. Infection Immunology, (2008); 76: 2123–2129.
- Santiago-Raber M-L, Baudino L, Izui S. Emerging roles of TLR7 and TLR9 in murine SLE. Journal of Autoimmunity, (2009); 33(3–4): 231–238.
- Lande R, Gregorio J, Facchinetti V, Chatterjee B, Wang YH, Homey B, et al. Plasmacytoid dendritic cells sense self-DNA coupled with antimicrobial peptide. Nature, (2007); 449: 564–569.
- Banchereau, J and Pascual, V. Type I interferon in systemic lupus erythematosus and other autoimmune diseases. Immunity, (2006); 25(3): 383-392.
- Carpi M F, Pietro FD, Vincenzetti F, Mignini S, Napolioni F and Valerio. Human DNA extraction methods: patents and applications. Recent Patents on DNA & Gene Sequences, (2011); 5(1): 1-7.
- Rabbani MA, Siddiqui BK, Tahir MH, Ahmad B, Shamim A, Shah S MA, et al. Systemic lupus erythematosus in Pakistan. Lupus, (2004); 13(10): 820-825.
- Rubtsov AV, Rubtsova K, Fischer A, Meehan RT, Gillis JZ, Kappler JW, et al. Toll-like receptor 7 (TLR7)-driven accumulation of a novel CD11c⁺ B-cell population is important for the development of autoimmunity. Blood, (2011); 118(5): 1305-15.
- Solangi, GA, Zuberi BF, Shaikh SA, Mirza MA. Systemic lupus erythematosus at Karachi and Larkana: A comparative study of 94 patients. Journal of the College of Physicians and Surgeons Pakistan, (2001); 11(6): 371-373.
- Voulgarelis M, Giannouli S, Tasidou A, Anagnostou D, Ziakas PD, Tzioufas AG. Bone marrow histological findings in systemic lupus erythematosus with hematologic abnormalities: a clinic-pathological study. American Journal of Hematology, (2006); 81(8): 590-7.
- Lam SK, Quah TC. Anemia in systemic lupus erythematosus. Journal of the Singapore Paediatric Society, (1990); 32(3-4): 132-136.
- Zhang J, Zhu Q, Meng F, Lei H, Zhao Y. Association study of TLR-9 polymorphisms and systemic lupus erythematosus in northern Chinese Han population. Gene, (2014); 533(1): 385–388.
- Han JW, Zheng HF, Cui Y, Sun LD, Ye DQ, Hu Z, et al. Genome-wide association study in a Chinese Han population identifies nine new susceptibility loci for systemic lupus erythematosus. Nature Genetics, (2009); 41: 1234-1237.
- Nakano S, Morimoto S, Suzuki J, Nozawa K, Amano H, Tokano Y, et al. Role of pathogenic auto-antibody production by toll-like receptor 9 of B cells in active systemic lupus erythematosus. Rheumatology (Oxford) 2008;47(2):145–149.
- Piotrowski P, Lianeri M, Wudarski M, Olesińska M, Jagodziński PP. Contribution of STAT4 gene single – nucleotide polymorphism to systemic lupus erythematous in the Polish population. Molecular Biology Reports, (2012); 39: 8861-66.
- Huang CM, Huang PH, Chen CL, Lin YJ, Tsai CH, Huang WL, et al. Association of toll-like receptor 9 gene polymorphism in Chinese patients with systemic lupus erythematosus in Taiwan. Rheumatology International, (2012); 32(7): 2105–2109.
- Mu R, Sun XY, Lim LT, Xu CH, Dai CX, Su Y, et al. Toll-like receptor 9 is correlated to disease activity in Chinese systemic lupus erythematosus population. Chinese Medical Journal, (2012); 125(16): 2873–2877.
- Lee YH, Choi SJ, Ji JD, Song GG. Association between toll-like receptor polymorphisms and systemic lupus erythematosus: a meta-analysis update. Lupus, (2016); 25(6): 593-601.
- Elloumi N, Fakhfakh R, Abida O, Ayadi L, Marzouk S, Hachicha H, et al. Relevant genetic polymorphisms and kidney expression of Toll-like receptor (TLR)-5 and TLR-9 in lupus nephritis. Clinical and Experimental Immunology, (2017); 190(3): 328-339.
- Zhou XJ, Lv JC, Cheng WR, Yu L, Zhao MH, Zhang H. Association of TLR9 gene polymorphisms with lupus nephritis in a Chinese Han population. Clinical and Experimental Rheumatology, (2010); 28(3): 397–400.
- Lee YH, Choi SJ, Ji JD, Song GG. Association between toll-like receptor polymorphisms and systemic lupus erythematosus: a meta-analysis update. Lupus, (2016); 25(6): 593-601.
- Sanchez M, Giordani L, Libri I, Quaranta MG, Mattioli B, Viora M. IFN-alpha amplifies human naive B cell TLR-9-mediated activation and Ig production. Journal of Leukocyte Biology, (2009); 86(2): 261-71.
- Enevold C, Nielsen CH, Jacobsen RS, Hermansen ML, Molbo D, Avlund K, et al. Single nucleotide polymorphisms in genes encoding toll-like receptors 7, 8 and 9 in Danish patients with systemic lupus erythematosus. Molecular Biology Reports, (2014); 41(9): 5755-63.
- Dos Santos BP, Valverde JV, Rohr P, Monticielo OA, Brenol JC, Xavier RM, et al. TLR7/8/9 polymorphisms and their associations in systemic lupus erythematosus patients from southern Brazil. Lupus, (2012); 21(3): 302-309.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0![]()