

Full Length Research Article
APOBEC3G Variant (rs6001417) CG and GG Genotypes and their protective feature against HIV-1 Infection in Pakistani Dwelled Community
Qaisar Ali2, Arshad Jamal1,2 , Sajjad Ullah2, Ahmed Bilal Waqar*2
Adv. life sci., vol. 8, no. 2, pp. 108-113, February 2021
*– Corresponding Author: Ahmed Bilal Waqar (Email: drabwaqar@yahoo.com)
Authors' Affiliations
2. Department of Medical Laboratory Sciences (DMLS), Faculty of Allied and Health Sciences, Imperial College of Business Studies Lahore – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: APOBEC3G (Apolipoprotein B mRNA-editing enzyme, catalytic polypeptide-like 3G) gene is one of the genetic host factors, have been linked with HIV-1 AIDS predisposing and protection in different residence populations. The investigation of genetic marker (APOBEC3G) variant (rs6001417) CC, CG and GG genotypes in Pakistan.
Methods: The extraction of DNA, the DNA Rapid Salting-out method was used. Then the observed DNA with electrophoresis technique referred for quantitative real-time PCR to identify the APOBEC3G variant rs6001417 genotypes and Taq Man genotyping.
Results: Three genotypes of rs6001417 (CC, CG and GG) were compared both in HIV-1 infected patients and healthy control groups (p=0.73, p=0.007, p=0.01 respectively). The rs6001417 CG and GG genotype demonstrated a significant involvement in both the healthy and infected individuals and portraying possible protective effect against HIV-1 infection with predictive value of 36.43% and 13.57% respectively.
Conclusion: APOBEC3G (rs6001417) CG and GG genotypes may have a protective feature in the progression of HIV-1 infection and we may use this as a preliminary predictive marker in the country for HIV-1 infected individuals as well.
Keywords: HIV-1; APOBEC3G; Predictive marker; Predictive value; Real-time PCR
Introduction![]()
HIV-1 infection is one of the global health problems, affecting almost 37.9 as million human population as of 2019 according to UNAIDS worldwide, with 3.1 million new cases reported every year [1-3, 40]. In recent past, HIV infection is highly prevalent in Sub-Saharan countries [4], however in Pakistan, currently it is one of the leading causes of morbidity and mortality as it hits approximately 160,000 infected individuals according to UN. Mostly HIV infection is being transmitted via contaminated blood and sexual contacts [5,6].
Immune related genetic mechanism can participate with the immune system while excluding a specific type of antigen from the body [7-11]. Recent findings portray that, both the host and viral genetics may have a substantial influence in the disease progression and protection [12-14]. In case of homozygous allelic variant of CCR5 protein has a substantial contribution in against the HIV infection [15,16]. Also, the ethnic background and DNA sequence similarity has a great role in the susceptibility and protection of a disease [17,19]. The only reason attracts researchers globally to study the genetic role in the progression of HIV infection.
In recent times, several studies have demonstrated that multiple host factors have influenced the pathogenesis of HIV-1/AIDS condition. These factors includes; APOBEC3G, Chemokine Receptor 5 (CCR-5), Dendritic Cell-Specific Intercellular adhesion molecule-3-Grabbing Non-integrin (DC-SIGN), Tripartite motif 5a (TRIM5a), Tetherin, and (SAM-domain HD-domain containing protein) SAMHD1 [5,20-23]. These are antagonized by accessory viral proteins [24,25].
Moreover, Apolipoprotein B mRNA editing enzyme catalytic polypeptide-like 3G (APOBEC3G) is an effective factor inside the host, which interferes with HIV-1 [22]. Virion infectivity factor (vif) which is structural part of HIV-1 is able to counteract APOBEC3G antiviral activity by targeting it for degradation in proteasomes [26,27]. Vif proteins derived from subtypes A, B, CRF01_AE, and CRF_02AG showed non-significant but some-what differential anti-APOBEC3G activity levels based on infectivity profiles while subtype C was highly significant [28,29]. The APOBEC3G protein was incorporated into newly synthesized viral particles, in the absence of the virion infectivity factor (vif), and deamination of cytosine (C) to uracil (U) made viral DNA mutated. APOBEC3G polymorphisms, such as (H186R) rs8177832, are supposed to be related with HIV-1 subtype B and C pathogenesis in different ethnic groups [7,30], however this association is not found in other populations [31-33]. These previous studies did not take the Circulating Recombinant Forms of HIV-1 into consideration, nor examine the effect of APOBEC3G polymorphisms in Asian Pakistani ethnic groups. The present study was conducted to understand and make clear the role of rs6001417, variants of APOBEC3G in HIV-1 infection in Pakistani population.
Methods![]()
Study population
A total of 240 subjects (100 patients and 140 healthy persons) were included in this study. Samples were collected from different HIV centers of Pakistan and processed at Imperial Diagnostics and Research Center, Lahore.
Sample collection, HIV-1 testing
Intravenous blood samples collected from HIV-1 infected subjects were genotyped using Real Time PCR Quantitative kit (SYBR GreenER) 100-rxn according to manufacturer’s instructions.
DNA extraction and genotyping
The DNA was extracted from blood by using the “DNA Rapid Salting-out” procedure which has characterized by Miller et al [34]. The extracted DNA was stored at -20oC till further processing. The concept of SNP was based on A3G variant rs6001417 along with the defense in contact with HIV-1 infection [30]. The rs6001417 in regard to A3G was genotyped by applying common SYBR GreenER SNP assay on the Fast Real-Time PCR Systems (Applied Biosystem Step One TM). PCR amplification was performed using the reverse and forward primers respectively Table 1. Every reaction was consisted of absolute amount of 25 µl, containing 10x PCR buffer 2.5 µl, Taq polymerase 0.5 µl, d-NTPs 1 µl, each primer 1 µl, genomic DNA 1 µl. The processing started by denaturation at 95℃, 30s of annealing at 55oC and 30s of extension at 68℃, in 35 cycles. The final extension was, at 72℃ for 7 minutes. After electrophoresis over a 2 percent agarose gel with 0.5 ug/ml ethidium bromide, the amplified product was examined on UV light.
Ethical considerations
The study was approved from the Institutional Ethical Committee of Imperial College of Business Studies and written consent from each participant was obtained.
Statistical analysis
The epidemiological data were recorded on a pre-designed form and handled within excel software. All calculations were performed by applying SPSS software version 20.0 statistical package. Data is expressed as Mean ± S.D and calibrations like diagnostic aspects has been calculated. Categorical variable was analyzed with X2 test. Hardy Weinberg equilibrium is also applied for Allele frequency. Contrasts to genotype placement of the groups were determined through the X2 trial. P<0.05 is considered as statistically significant.
Results![]()
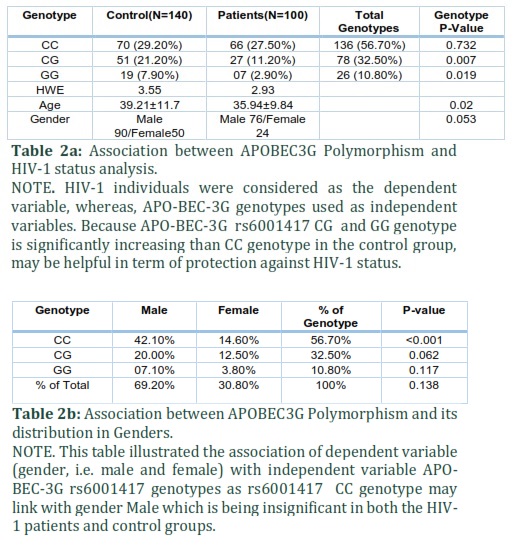
A total of 240 individuals were included into the study. Study population consisted of 100 HIV-1 infected patients and 140 healthy controls. Gender wise distribution, age of the cases and healthy groups have been defined in Table 2. The mean age of the study population was 39.21±11.7 in the healthy control group and 35.94±9.84 in the HIV-1 cases group. We found gender and age comparable variables among the two groups (P< 0.05). Genotype frequencies of the one APOBEC3G loci (rs6001417) for both the cases and controls were given correspondingly in Table 2.
1. Association between APOBEC3G variants and HIV-1 status
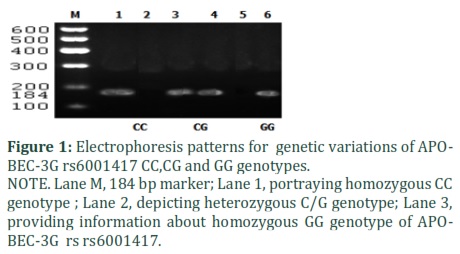
We analyzed and compared SNP rs6001417 genotypes ( CC, CG and GG) between cases and control groups by using P-value of > 0.05, as shown in Table 2. The electrophoresis pattern of APOBEC3G (rs6001417) CC, CG, and GG genotypes was shown in Figure 1.
1.1 APOBEC3G (rs6001417)
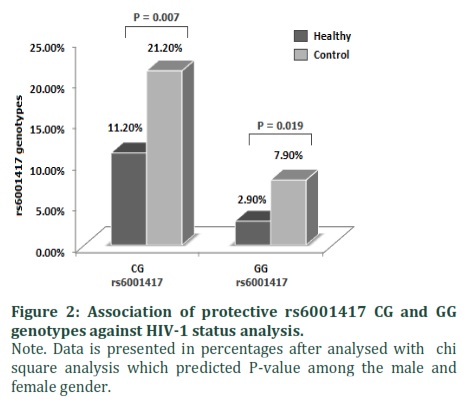
The genotype frequencies of APOBEC3G (rs6001417) CC, CG, and GG genotypes were 27.50%, 11.20%, 2.90% in the patient with HIV-1 group and 29.20%, 21.20%, 7.90% in the control group, respectively as shown in Table 1. Individuals account for HIV-1 infection has lower frequencies of the APOBEC3G (rs6001417) CG,GG genotypes than healthy individuals while CC in HIV-1 patients. Chi-square analysis provided information that rs6001417 CG and GG genotypes (51 (21.20%) vs 27 (11.20%) ; p=0.007 and 19 (7.90%) vs 07 (2.90%); p=0.019) reflect a significant variation between the two groups as shown in Figure 2. This analysis showed that subjects account for rs6001417 CG and GG genotype displays a protective role toward the HIV-1 infection.
2. Association of gender with protective and predisposing attaining APOBEG3G variants genotypes
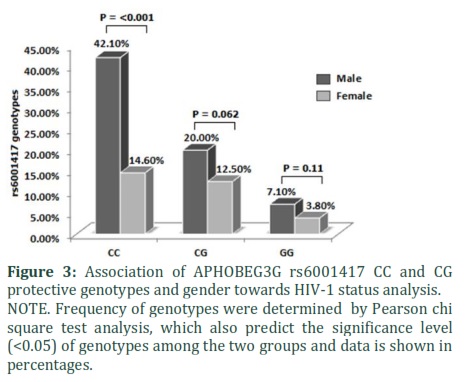
We found rs6001417 CC,CG and GG genotype frequencies and distribution as 42.10%, 20.00%, 07.10% and 14.60%, 12.50%, 3.80% in both male and female gender, respectively and had found comparable (P< 0.05) Table 2, Figure 3.
2.1 Analysis of gender with Protective (rs6001417) CG and GG genotypes
The rs6001417 CG and GG genotype had a comparable association in both the male and female studied population (20.00% vs 12.50%; P= 0.062 and 07.10% vs 3.80%; p=0.117) (Table 2). This analysis showed that, there is a comparable contribution of both male and female towards the protection in CG and GG individuals (reduces risk of being infected) of the HIV-1 studied population. Moreover, (rs6001417) CC genotype was more common in male than female in HIV-1 studied population and statistically significant (42.10% vs 14.60%; p <0.001) as shown in Table 2. These findings showed the maximum contribution by male gender towards the CC genotype which is being insignificant in both the HIV-1 cases and control groups. These comparisons were noticed in the HIV-1 studied population only.
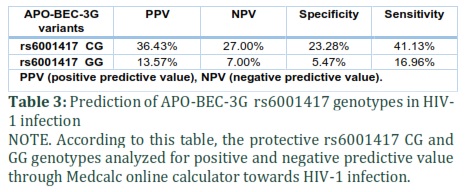
3. Predictive value of APOBEG3G (rs6001417) CG and GG genotypes
We have already discussed the protective rs6001417 CG, and GG genotypes for HIV-1 infection. In addition, we examined predictive value of these two genotypes as well. Both the rs6001417 CG and GG genotypes were found to be the protective genotypes, we also calculated positive predictive value (PPV) which was 36.43% and 13.57%, respectively as shown in Table 3.
Figures & Tables

Discussion![]()
Continual exposure to HIV infection does not certainly result in AIDS occurrence [35]. Multiple genetic and immune factors help in HIV acquirement, pathogenesis and AIDS progression at various stages of HIV life-cycle. So, HIV infection activates multiple intrinsic host factors that confer resistance to HIV pathogenesis, though the most important one is intrinsic inhibition to HIV infection by APOBEC3G genetic host factor [24,36]. APOBEC3G single nucleotide polymorphisms (SNPs) are of particular importance and its twenty-nine SNPs have been studied in American [37] and European [38] cohorts to reveal its influence on AIDS development and progression. We examined the frequency distribution of the variants rs6001417 of APOBEC3G gene in the population of Pakistan. Moreover, we studied the APOBEC3G gene polymorphism without the fact of that virion infectivity factor (vif), as it degrades the HIV-1 virus along with APOBEC3G gene [26,27].
The most common genotype was CC of APOBEC3G variants (rs6001417) followed by CG, GG , in the whole studied population. Furthermore, it was observed, that APOBEC3G rs6001417 CG and GG genotypes provide significant protection with 36.43% and 13.57% positive predictive value (PPV) respectively, towards HIV-1 infection. We have already reported predictive value in the treatment of HCV infection recently in which IL28B rs12979860 CT predicted 81.56% [39]. In a recently reported study from Pakistan, has shown that rs8177832 AA genotype has a predisposing role whereas, rs8177832 AG genotype portrayed a protective prediction against HIV-1 disease [40]. Recently a study conducted in Burkina Faso revealed that APOBEC3G GGT haplotypes for rs6001417 variants have an influential outcome by providing protection against HIV infection in comparison to other haplotypes. The results of the same study also demonstrated that individuals with haplotypes GGC has an increase of two- to five-folds in susceptiblity against the HIV infecton [41]. However, French cohort study showed a comparable association of APOBEC3G genetic variation, H186R, with the disease progression [31]. Interestingly, Tegwinde Rebeca Compaore et.al reported that rs6001417 GG and CG genotypes predicted protection and predisposing factor against the HIV-1 respectively, which is in line with our study that also showed both rs6001417 GG and CG genotypes with protective feature [42].
Moreover, in the recent past APOBEC3G was also studied with HBV infection, though a Moroccan based study where 179 chronic infected inviduals along with 216 control were involved concluded with comparable results after testing hypothesis [43]. But, this variation of the results might be due to the distinct level of population and genetic makeup. This gentic variation was noted as higher as 37%, 3% and 5% in African Americans, Europian Americans and europian, respectively [7]. Similarly, Single Nucleotide polymorphisms of APOBEC3G docking proteins such as Vif and CUL5 can also help in the progression of the disease [44].
According to our studied population, the effect of APOBEC3G rs6001417 CC (42.10% vs 14.60% ; P = <0.001) genotype with in gender as it found frequently in males compare to female. Therefore, the notion that the rs6001417 CT genotype may be supported by the male in term of protection or predisposing against HIV-1 infection is not supported by our results because we found this CT genotype insignificant (neither protective nor predisposing). Interestingly,we reported gender association in recent past with IL28B rs12979860 CT genotype against the spotaneous clearance of HCV infection, in which female gender supported CT genotype in term of spontaneous clearance of HCV infection [45]. To the best of our knowledge, no one has studied or reported the gender interaction with APOBEC3G gene polymorphism and HIV-1 infection. The limitations of this interaction, need further investigations as the sample size of our study was not enough and need further investigation in order to clarify the association.
APOBEC3G polymorphisms variants (rs6001417) CG and GG genotypes may play a vital role at biological level in the interaction of HIV-1 susceptibility to the host, however, extra efforts are required on a larger cohort of patients to elucidate the association.
Author Contributions
All authors contributed equally in preparation and publication of this manuscript.
The authors declare that there is no conflict of interest regarding the publication of this paper.
Acknowledgment
This work was supported by Çanakkale Onsekiz Mart University the Scientific Research Coordination Unit, Project number: 2008-44.
References![]()
- Barré-Sinoussi F, Chermann J-C, Rey F, Nugeyre MT, Chamaret S, et al. Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS). Science, (1983); 220(4599): 868-871.
- Celerino da Silva R, Victor Campos Coelho A, Rodrigues de Moura R, Claudio Arraes L, Andre Cavalcanti Brandao L, Lima Guimarães R, Crovella S. CUL5 and APOBEC3G polymorphisms are partially implicated in HIV-1 infection and antiretroviral therapy in a Brazilian population. Current HIV Research. 2017;15(4):245-57.
- Murray CJ, Ortblad KF, Guinovart C, Lim SS, Wolock TM, et al. Global, regional, and national incidence and mortality for HIV, tuberculosis, and malaria during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet, (2014); 384(9947): 1005-1070.
- Kharsany AB, Karim QA. HIV infection and AIDS in Sub-Saharan Africa: current status, challenges and opportunities. The open AIDS journal, (2016); 10: p34.
- Ali Q, Jamal A,, Ullah S, Waqar AB.Male predominant association with Apolipoprotein B mRNA-editing enzyme, catalytic polypeptide-like 3G variants (rs6001417, rs35228531, rs8177832) predict protection against HIV-1 infection. Advancement in life Science, (2020); 7(2): 91-97.
- Oberle CS, Joos B, Rusert P, Campbell NK, Beauparlant D, et al. Tracing HIV-1 transmission: envelope traits of HIV-1 transmitter and recipient pairs. Retrovirology, (2016); 13(1): p62.
- An P, Bleiber G, Duggal P, Nelson G, May M, et al. APOBEC3G genetic variants and their influence on the progression to AIDS. Journal of virology, (2004); 78(20): 11070-11076.
- An P, Penugonda S, Thorball CW, Bartha I, Goedert JJ, et al. Role of APOBEC3F gene variation in HIV-1 disease progression and pneumocystis pneumonia. PLoS genetics, (2016); 12(3): e1005921.
- Dunn GP, Bruce AT, Ikeda H, Old LJ, Schreiber RD. Cancer immunoediting: from immunosurveillance to tumor escape. Nature immunology, (2002); 3(11): p991.
- van Kooyk Y, Appelmelk B, Geijtenbeek TB. A fatal attraction: Mycobacterium tuberculosis and HIV-1 target DC-SIGN to escape immune surveillance. Trends in molecular medicine, (2003); 9(4): 153-159.
- D'Urbano V, De EC, Re M. Host restriction factors and Human immunodeficiency Virus (HIV-1): a dynamic interplay involving all phases of the viral life cycle. Current HIV research, (2018); 16(3): 184-207.
- Bataller R, North KE, Brenner DA. Genetic polymorphisms and the progression of liver fibrosis: a critical appraisal. Hepatology, (2003); 37(3): 493-503.
- Janssen R, Bont L, Siezen CL, Hodemaekers HM, Ermers MJ, et al. Genetic susceptibility to respiratory syncytial virus bronchiolitis is predominantly associated with innate immune genes. Journal of Infectious Diseases, (2007); 196(6): 826-834.
- Powell EE, Edwards‐Smith CJ, Hay JL, Clouston AD, Crawford DH, et al. Host genetic factors influence disease progression in chronic hepatitis C. Hepatology, (2000); 31(4): 828-833.
- Piacentini L, Biasin M, Fenizia C, Clerici M. Genetic correlates of protection against HIV infection: the ally within. J Intern Med, (2009); 265(1): 110-124.
- A Estrada-Aguirre J, G Cazarez-Salazar S, A Ochoa-Ramirez L, de J Acosta-Cota S, Zamora-Gómez R, et al. Protective effect of CCR5 Delta-32 allele against HIV-1 in Mexican women. Current HIV research, (2013); 11(6): 506-510.
- Kenny-Walsh E. The natural history of hepatitis C virus infection. Clinics in liver disease, (2001); 5(4): 969-977.
- Dolo A, Modiano D, Maiga B, Daou M, Dolo G, et al. Difference in susceptibility to malaria between two sympatric ethnic groups in Mali. The American journal of tropical medicine and hygiene, (2005); 72(3): 243-248.
- Perera FP. Molecular epidemiology: insights into cancer susceptibility, risk assessment, and prevention. JNCI: Journal of the National Cancer Institute, (1996); 88(8): 496-509.
- Duggal NK, Emerman M. Evolutionary conflicts between viruses and restriction factors shape immunity. Nature Reviews Immunology, (2012); 12(10): 687.
- Kagoné TS, Bisseye C, Méda N, Testa J, Pietra V, et al. A variant of DC-SIGN gene promoter associated with resistance to HIV-1 in serodiscordant couples in Burkina Faso. Asian Pacific journal of tropical medicine, (2014); 7: S93-S96.
- Harris RS, Liddament MT. Retroviral restriction by APOBEC proteins. Nature Reviews Immunology, (2004); 4(11): 868-877.
- Merindol N, Berthoux L. Restriction factors in HIV-1 disease progression. Current HIV research, (2015); 13(6): 448-461.
- Imran M, Manzoor S, Saalim M, Resham S, Ashraf J, et al. HIV-1 and hijacking of the host immune system: the current scenario. APMIS, (2016); 124(10): 817-831.
- Ayinde D, Casartelli N, Schwartz O. Restricting HIV the SAMHD1 way: through nucleotide starvation. Nature Reviews Microbiology, (2012); 10(10): 675-680.
- Mehle A, Strack B, Ancuta P, Zhang C, McPike M, et al. Vif overcomes the innate antiviral activity of APOBEC3G by promoting its degradation in the ubiquitin-proteasome pathway. Journal of Biological Chemistry, (2004); 279(9): 7792-7798.
- Farrow MA, Sheehy AM. Vif and Apobec3G in the innate immune response to HIV: a tale of two proteins. Future Micrbiology, (2008); 3(2): 145-154.
- Iwabu Y, Kinomoto M, Tatsumi M, Fujita H, Shimura M, et al. Differential anti-APOBEC3G activity of HIV-1 Vif proteins derived from different subtypes. Journal of Biological Chemistry, (2010); 285(46): 35350-35358.
- Binka M, Ooms M, Steward M, Simon V. The activity spectrum of Vif from multiple HIV-1 subtypes against APOBEC3G, APOBEC3F, and APOBEC3H. Journal of virology, (2012); 86(1): 49-59.
- Reddy K, Winkler C, Werner L, Mlisana K, Karim SA, et al. APOBEC3G expression is dysregulated in primary HIV-1 infection and a polymorphic variant influences CD4+ T cell counts and plasma viral load. AIDS (London, England), (2010); 24(2): p195.
- Do H, Vasilescu A, Diop G, Hirtzig T, Heath SC, et al. Exhaustive genotyping of the CEM15 (APOBEC3G) gene and absence of association with AIDS progression in a French cohort. Journal of Infectious Diseases, (2005); 191(2): 159-163.
- Valcke HS, Bernard NF, Bruneau J, Alary M, Tsoukas CM, et al. APOBEC3G genetic variants and their association with risk of HIV infection in highly exposed Caucasians. Aids, (2006); 20(15): 1984-1986.
- Kalam, I., Ullah, S., Ali, Q., Jamal, A. and Waqar, A.B., 2018. Impact of IL28B gene variants (rs12979860) in peg-IFN therapy against Chronic Hepatitis B Pakistani patients. Advancements in Life Sciences, 6(1), pp.11-18.
- Miller S, Dykes D, Polesky H. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic acids research, (1988); 16(3): p1215.
- Dean M, Carrington M, Winkler C, Huttley GA, Smith MW, et al. Genetic restriction of HIV-1 infection and progression to AIDS by a deletion allele of the CKR5 structural gene. Science, (1996); 273(5283): 1856-1862.
- McNab F, Mayer-Barber K, Sher A, Wack A, O'garra A. Type I interferons in infectious disease. Nature Reviews Immunology, (2015); 15(2): 87.
- An P, Bleiber G, Duggal P, Nelson G, May M, et al. APOBEC3G genetic variants and their influence on the progression to AIDS. Journal of Virol, (2004); 78(20): 11070-11076.
- Do H, Vasilescu A, Diop G, Hirtzig T, Heath SC, et al. Exhaustive genotyping of the CEM15 (APOBEC3G) gene and absence of association with AIDS progression in a French cohort. Journal Infection Diseases, (2005); 191(2): 159-163.
- Ali Q, Kalam I, Ullah S, Jamal A, Imran M, et al. Predictive value of IL-28B rs12979860 variants for peg-IFN, sofosbuvir plus ribavirin treatment of HCV infection in Pakistani population. Personalized medicine, (2018); 15(6).
- Iqbal K, Imran M, Ullah S, Jamal M, Waheed Y, et al. Correlation of apolipoprotein B mRNA-editing enzyme, catalytic polypeptide-like 3G genetic variant rs8177832 with HIV-1 predisposition in Pakistani Population. Current HIV research, (2018); 16(4): 297-301.
- Compaore TR, Soubeiga ST, Ouattara AK, Obiri-Yeboah D, Tchelougou D, et al. APOBEC3G Variants and Protection against HIV-1 Infection in Burkina Faso. PloS one, (2016); 11(1): p.e0146386.
- Compaore TR, Diarra B, Assih M, Obiri-Yeboah D, Soubeiga ST, et al. HBV/HIV co-infection and APOBEC3G polymorphisms in a population from Burkina Faso. BMC infectious diseases, (2016); 16(1): p336.
- Ezzikouri S, Kitab B, Rebbani K, Marchio A, Wain‐Hobson S, et al. Polymorphic APOBEC 3 modulates chronic hepatitis B in M oroccan population. Journal of viral hepatitis, (2013); 20(10): 678-686.
- De Maio FA, Rocco CA, Aulicino PC, Bologna R, Mangano A, et al. Effect of HIV-1 Vif variability on progression to pediatric AIDS and its association with APOBEC3G and CUL5 polymorphisms. Infection, Genetics and Evolution, (2011); 11(6): 1256-1262.
- Ali Q, Jamal A, Imran M, Ullah S, Kalam I, Ullah S, Waqar AB. Correlation of IL28B rs12979860 genotype and gender with spontaneous clearance of HCV infection: a Pakistani cross-section study. Personalized medicine. 2018 Nov;15(6):495-502.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0