

Full Length Research Article
Rh alleles and phenotypes among Saudi women in Hail Region, Saudi Arabia
Jerold C. Alcantara1, Tessie Y. Alcantara1, Khalid F. Al Shaghdali 1, Fawaz D. Al Shammari*1, Fahad Ghali M. Al Shammari2
Adv. life sci., vol. 8, no. 2, pp. 114-118, February 2021
*– Corresponding Author: Fawaz D. Al Shammari (Email: fawazaboff@gmail.com)
Authors' Affiliations
2. Clinical Laboratory Department, Hail Maternity and Children Hospital – Saudi Arabia
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The Rh system is considered as the most complex among the human blood group systems, with 61 antigens identified to date. This study aimed to provide preliminary data on the distribution of Rh alleles and phenotypes among Saudi women and compare them with other ethnic groups.
Methods: This retrospective cross-sectional study was conducted among Saudi women who visited the Maternity and Children Hospital of Hail from November 2019 to March 2020. A fully automated blood bank analyzer was used in determining the Rh subgroups (D, C, c, E, e) and phenotypes. Inferential statistics and chi-square tests were used appropriately for comparisons.
Results: The study included a total of 500 Saudi female patients. The most prevalent antigen found was the “e” antigen, while phenotype CcDee has shown to have the highest frequency. A significant difference exists in comparison with the other studies from various ethnic groups.
Conclusions: The prevalence and distributions of Rh alleles and phenotypes among Saudi women were revealed in this study. The findings showed that Rh alleles and phenotypes are diverse across various races and regions globally.
Keywords: Rh allele; Rh phenotype; Rh system; Saudi Arabia
Introduction![]()
The Rh system is considered as the most complex human blood group, with 61 antigens identified to date [1]. The D antigen, which is the most immunogenic of all antigens, underscores its clinical importance. In addition, clinically important Rh antibodies are relatively common in pregnancy, and patients requiring transfusion [2]. Additional four antithetical Rh antigens – C and c, and E and e comprise the system’s principal antigens. Among the 61 Rh antigens that have been characterized, these five antigens account mainly of the clinically significant antibodies of the Rh system [1-3].
Routine donor and patient typing results in the detection of D only. However, the majority of Rh incompatibilities are mainly caused by the five principal antigens [4,5] Rh-negative recipients that are transfused with Rh-positive blood are likely to develop anti-D in more than 50% of cases [1,6]. The prevalence of alloimmunization in Rh-negative females with Rh-positive fetus was a significant risk before the availability of Rh Immune Globulin (RhIg) prophylaxis [1]. The increasing number of multi-transfused patients in our society reflects the prevalence of red cell alloantibodies. Factors such as the need for transfusion for certain diseases, the growing disparity of red cell antigen distribution between red cell donor and recipient population, and immunogenicity of particular blood group antigen increase the tendency of alloantibody development [7,8]. To resolve or confirm antibody identification, testing the other common antigens is performed. Antibodies of the Rh system are considered clinically significant that can cause hemolytic disease of the fetus and new-born (HDFN) and transfusion reactions [1].
Determination of Rho status, including weak D in obstetric patients, is critical [2]. They are valuable in transfusion centers both in routine and advanced clinical practice [9-11]. Distributions of blood groups varies across different races. Certain ethnic groups may possess distinctive blood groups and can display disparity in prevalence among other groups worldwide [8]. In a study which comprises of 600 Saudi nationals in Riyadh, it was identified that DCcee (28.7%) among the RhD positive, and dccee (13.7%) among the RhD negative blood donors, were the most common phenotypes [9].
Presently, a minimal number of studies on Rh antigens and phenotypes, specifically among Saudi women, are available in the Kingdom. Our study aimed on providing preliminary data on the Rh alleles and phenotypes among the Saudi women population. These data could be valuable in the Identification of the distinct Rh phenotypes or subgroups in the Hail population. Knowledge of their distribution can also aid in finding antigen-negative blood for alloimmunized patients.
Methods![]()
This is a retrospective cross-sectional study conducted on a hospital-based Blood Bank of Maternity and Children Hospital in Hail, Saudi Arabia, from November 2019 to March 2020. The study population comprises of 500 Saudi women of different age groups ranging from age 18-55 that were randomly selected. Rh subtyping and phenotyping were performed using the TangoTM Optimo, a fully automated blood bank analyzer. An EDTA anticoagulated blood (3 ml) sample was used in the analysis. The principle is based on microplate hemagglutination that detects the corresponding red cell antigens. The antigens on the red cell precisely react with the corresponding antibodies on the wall cavities. Agglutination indicates a positive reaction, while a negative reaction shows non-agglutination.
Collected data were entered and analyzed using SPSS v 20.0. Variables such as Rh antigens, alleles, and phenotypes were observed and expressed as frequencies and percentages. Statistical tools like the chi-square tests and inferential statistics were employed to compare the antigens prevalence and their distributions from the different ethnicities.
The study protocol was reviewed and approved by the ethics committee of the College of Medicine, University of Hail, Saudi Arabia. Further, written permission was obtained from the laboratory director of Maternity and Pediatric Hospital in Hail.
Results![]()
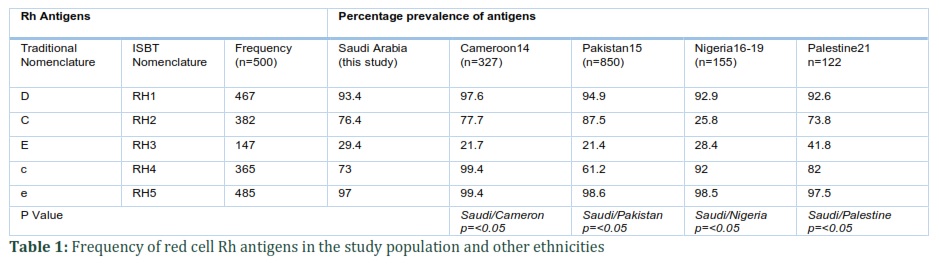
The study included a total of 500 Saudi female patients. Of which 93.4% (467) was RhD positive, while 6.6% (33) was determined as RhD negative. The overall prevalence rate of the other Rh antigens C, E, c, and e were 76.4%, 29.4%, 73%, and 97%, respectively (Table1), where antigen e (97%) as the most prevalent while antigen E (29.4%) as least antigens observed. Moreover, among the RhD positives in the study population, the most frequent was antigen e (97%), while antigens c and e was determined to be present in all RhD-negatives. Table 1 shows the prevalence of antigens in the study population.
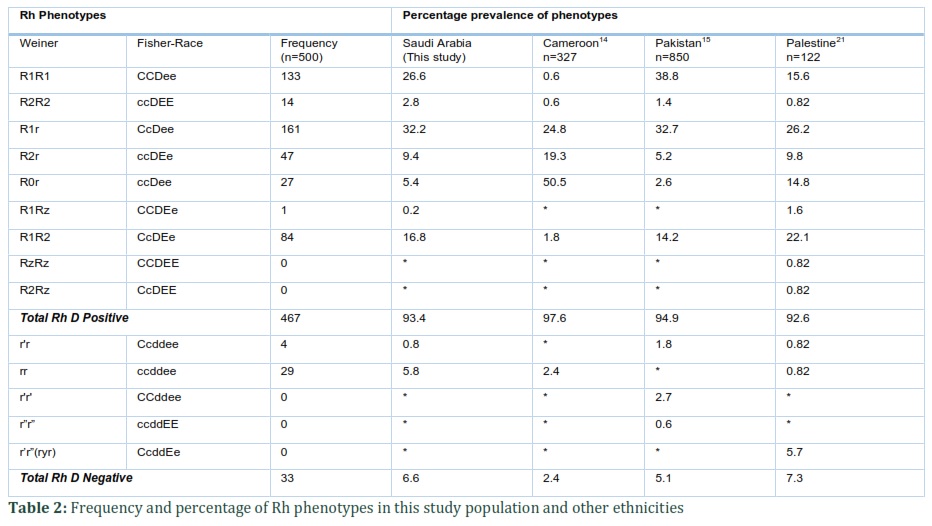
Overall, CcDee (32.2%) was found to be the commonest phenotype observed in our population, followed by CCDee (26.6%), while the least common was Ccddee, which accounts for 0.8% and CCDEe for 0.2%. Among the RhD positives, the CcDee phenotype has the highest rate, while ccddee phenotype among the RhD negatives (Table 2). Noticeably, some phenotypes were not present in the study population but existed in other ethnicities. A comparison of Rh phenotype frequencies with those other ethnic populations is presented in Table 2.
Figures & Tables
Discussion![]()
Determining the minimum level of stocks and the blood products that is required most in a given population is crucial. Antigens on red cells are highly variable. It is, therefore, essential for the transfusion institute to assess and define the frequencies of antigens to ensure transfusion safety [12,13].
After an extensive search, the authors believed that no data exist or study conducted on this subject from this region, mainly among women. We compared our data with those other international data and similar studies outside and within the Kingdom [13-19]. The results of this study found out that they were fairly consistent with the other studies.
The RhD positive in this study was 93.4%, while 6.6% was RhD negative. This result is consistent with the study of Talib et al. [13] among Saudi obstetric patients in Riyadh and other studies of different ethnicity (Table 1). However, differences were observed in the frequency of the other Rh antigens as compared to other studies [14-16,18,19]. The prevalence of C antigen in this study was found to have minor differences among other studies but substantially higher than the study from Nigeria. However, the lower frequency was observed on c antigen as compared to the study from Cameroon, Nigeria, and Palestine (Table1). The prevalence of E and e antigen in this study was found to be consistent with the data published internationally (English) [8,20] and with the other ethnic populations. Furthermore, we also observed the distribution of the other four (4) Rh antigens according to D status. It was found that the proportions of D positive and D negative individuals vary according to their positivity or occurrences.
For instance, there was a higher positivity of C antigen (81.2%) among D positive individuals as compared to D negative individuals (12%). In contrast, all D negative individuals in the study population were positive for c antigen (D−c+ = 100%, D+c+ = 71.3%). Similarly, antigen E positivity differs depending on their D status (D+E+ = 31.3% D−E+ = 0). But for the distribution of e antigen, there were no substantial difference in terms of RhD status (D+e+ = 97%, D−e+ = 100%). These patterns of findings were similar to the studies conducted among blood donors in Saudi Arabia [9,20]. A similar pattern was also observed from the studies made to other ethnic groups (Table 1).
Distribution of Rh phenotype varies across the racial and geographical location. The commonest phenotype found in this study was CcDee (R1r). Similarly, the study of Elsayid et al9 in Riyadh derived the same findings. Furthermore, the results of this study agree with the international published data among Caucasians and Blacks but not with Asians (CCDee, R1R1) [7,21]. Conversely, Rh phenotype distributions among other ethnicities (Table 2) differ from our study. CCDee (R1R1), ccDee (R0r), and CcDee (R1r) were commonest and leading phenotypes found in Pakistan, Cameroon, and Palestine, respectively. Noticeably, there were also differences observed among the D negative phenotypes. Our study agrees with the findings of Elsayid et al. [9] among blood donors that ccddee (rr) as the commonest. A similar result was also noted in Cameroon while Pakistan and Palestine study revealed that CCddee (r’r’) and CcddEe (r’r”) as the commonest phenotypes, respectively.
Alloimmunization is an existing problem and remains a challenge to transfusion safety and practice. It is one of the most relevant post-transfusion complications associated with transfusion delays, HDFN, and hemolytic transfusion reactions, which can be fatal in some cases [22]. Antibodies of the Rh system are commonly associated with alloimmunization. The study of Klapper et al. [23] observed that females are more likely to develop alloimmunization than males. It is believed that females, especially in developing countries, are anemic, and pregnancy is an important risk factor for alloimmunization [24]. In the study of Singer et al [25], it was demonstrated that transfusions involving blood that are matched phenotypically for the Rh system, was proven effective in the prevention of alloimmunization than bloods that are matched phenotypically for the ABO-D system only. In Western countries like France, Norway, and Finland, blood transfusion of non-phenotyped is prohibited in women of childbearing age [26,27].
Regular phenotyping not only limits the possibility of alloimmunization, especially among women in the reproductive age, but also creates a simple database of all common and unusual phenotypes that would be readily available when needed. When choosing the most appropriate reagents and phenotyping techniques, and in developing strategies for genotyping, knowledge on the variants in a specific population is critically vital [28]. The data generated in this study is useful in mapping the Rh phenotypic profile among women, finding antigen-negative compatible blood for alloimmunized patients, and in preparation of indigenous panel cells.
The prevalence and distributions of Rh alleles and phenotypes among Saudi women were revealed in this study. The findings showed that a diversity of Rh alleles and phenotypes exist across various races and regions globally. A larger scale of the population on this subject is recommended to establish a comprehensive database to define distinctly the Rh phenotypic profile of the population, which would be essential in the formulation of guidelines on testing and transfusion of blood among women in the reproductive age.
Author Contributions
J.C.A., T.Y.A. and F.D.A. conceived and designed the experiments; J.C.A., T.Y.A., K.A. and F.G.A. performed the experiments; J.C.A., T.Y.A. F.D.A. and K.A. organized drafting and analysis; F.D.A., J.C.A. and F.G.A. contributed figures and revised the article; J.C.A. and K.A. revised the paper; J.C.A. F.D.A., K.A., F.G.A. wrote the paper.
The authors declare that there is no conflict of interest regarding the publication of this paper.
References![]()
- Denomme GA WCTRSiMF, BJ. Grossman, CD Hillyer & CM Westhoff (Edition). Technical Manual 18th edition. Maryland: American Association of Blood Banks. (2014); pp: 317-321..
- Johnson ST WM. The Rh Blood Groups System’ in DM. Harmening (Eds). Modern Blood Banking and Transfusion Practices 6th ed. (2012); pp: 160-161.
- Rh DG. RHAG blood group systems. Human blood groups 3rd Ed Oxford (UK): Wiley-Blackwell, (2013); 185.
- Frohn C, Dumbgen L, Brand JM, Gorg S, Luhm J, et al. Probability of anti-D development in D- patients receiving D+ RBCs. Transfusion, (2003); 43(7): 893-898.
- Klein, H. G. "Immunology of red cells In: Klein HG, Anstee DJ., editors. Mollison's blood transfusion in clinical medicine. Oxford." (2005): 48-113.
- Achargui S, Zidouh A, Abirou S, Merhfour FZ, Monsif S, et al. [Identification of alloantibodies and their associations: Balance sheet of 3 years at the Regional Center of Blood Transfusion in Rabat/Morocco and difficult in transfusion management]. Transfusion Clinique et Biologique, (2017); 24(4): 422-430.
- Reid, Marion E., Christine Lomas-Francis, and Martin L. Olsson. The blood group antigen factsbook. Academic press, 2012.
- Daniels G. Human Blood Groups (2nd edn). Transfusion Medicine, (2004); 14(4): 326-326.
- Elsayid M, Al Qahtani FS, Al Qarni AM, Almajed F, Al Saqri F, et al. Determination of the frequency of the most immunogenic Rhesus antigens among Saudi donors in King Abdulaziz Medical City – Riyadh. Journal of Natural Science, Biology and Medicine, (2017); 8(1): 56-59.
- Levine P, Stetson RE. An unusual case of intra-group agglutination. Journal of the American Medical Association, (1939); 113(2): 126-127.
- Scott ML. The complexities of the Rh system. Vox Sanguinis, (2004); 87 Suppl158-62.
- Mazières S, Temory SA, Vasseur H, Gallian P, Di Cristofaro J, et al. Blood group typing in five Afghan populations in the North Hindu‐Kush region: implications for blood transfusion practice. Transfusion Medicine, (2013); 23(3): 167-174.
- Talib ZM, Al-Nuaim LA, El-Hazmi MA, Warsy AS. Blood groups in Saudi obstetrics patients. Saudi Medical Journal, (1998); 19(3): 260-264.
- Francoise NS DT, Bernanrd CC, Rene E. Erythrocyte alloimmunization, Rhesus and Kell phenotype for women of childbearing age in Yaounde. Journal of Medical Research (2018); 4(1): 20-23.
- Mahmood R, Alam M, Altaf C, Abbasi A, Malik H. Phenotypic profile of Rh blood group systems among females of child-bearing age in Pakistan. Hematology & Transfusion International Journal, (2018); 6(1): 00148.
- Erhabor O, Adamu KS, Yakubu A, Shehu C, Hassan M. Singh S.. Rh (D) Phenotype among Pregnant Women in Sokoto, North Western Nigeria. Implications on Haemolytic Disease of the New-Born and Haemolytic Transfusion Reaction. Health Science Research, (2014); 1(2): 19-24.
- Osaro E, Ladan MA, Zama I, Ahmed Y, Mairo H. Distribution of Kell phenotype among pregnant women in Sokoto, North Western Nigeria. The Pan African Medical Journal, (2015); 21,(1).
- Jeremiah ZA, Biribo AA, Adias TC, Uko EK. Uncommon Rh phenotypes in a cross section of Nigerian antenatal women: implications for molecular genotyping of blood groups. Journal of Blood Disorders and Transfusion, (2012); 10: 001.
- El-Wahhab Skaik YA. The Rh allele frequencies in Gaza city in Palestine. Asian Journal of Transfusion Science, (2011); 5(2): 150-152.
- Mustafa MHI, Elmisbah TE, Salim A, Ahmed MAM, Babiker S, et al. RHD and RHCE frequencies and gene complexes among major tribes of Turabah Province, Saudia Arabia. International Journal of Multidisciplinary and Current Research, (2014); (2), 2573-578.
- Wagner FF, Kasulke D, Kerowgan M, Flegel WA. Frequencies of the blood groups ABO, Rhesus, D category VI, Kell, and of clinically relevant high-frequency antigens in south-western Germany. Infusion Therapy and Transfusion Medicine, (1995); 22(5): 285-290.
- Dinardo CL. Red blood cell alloantibodies and autoantibodies: different presentation, same physiopathology. Hematology, Transfusion and Cell Therapy, (2018); 40(2): 99-100.
- Klapper E, Zhang Y, Figueroa P, Ness P, Stubbs J, et al. Toward extended phenotype matching: a new operational paradigm for the transfusion service. Transfusion, (2010); 50(3): 536-546.
- Sood R, Makroo RN, Riana V, Rosamma NL. Detection of alloimmunization to ensure safer transfusion practice. Asian Journal of Transfusion Science, (2013); 7(2): 135-139.
- Singer ST, Wu V, Mignacca R, Kuypers FA, Morel P, et al. Alloimmunization and erythrocyte autoimmunization in transfusion-dependent thalassemia patients of predominantly asian descent. Blood, (2000); 96(10): 3369-3373.
- Da Rocha Lopes, L. "Genetic determinants and genotype-phenotype associations in hypertrophic cardiomyopathy-Contribution of a high-throughput sequencing approach." PhD dissertation., UCL (University College London), 2015.
- Peyrard T, Rouger P, Transfusion and obstetrical safety of people with a rare blood group; Hématologie, (2010); 16(2): 143-55.
- El Housse H, El Wafi M, Ouabdelmoumene Z, Zarati F, Alid R, et al. Comprehensive phenotypic and molecular investigation of RhD and RhCE variants in Moroccan blood donors. Blood Transfusion, (2019); 17(2): 151-156.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0