

Review Article
Clinical Guidelines for Management of Acute Painful Episodes of Vaso-Occlusive Crisis in Children with Sickle Cell Disease
Nawaf Alanazi
Adv. life sci., vol. 8, no. 3, pp. 221-227, July 2021
*– Corresponding Authors: Nawaf Alanazi (Email: alanazina@ksau-hs.edu.sa)
Authors' Affiliations
Dean / Assistant Professor, College of Applied Medical Sciences
King Saud bin Abdulaziz University for Health Sciences (www.ksau-hs.edu.sa)
King Abdulaziz Medical City, Ministry of National Guard Health Affairs
Kingdom of Saudi Arabia
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
Sickle cell disease (SCD) is an inherited disease resulted due to a single mutation in beta globin gene. It changes normal red blood cells into sickle-shaped cells, just rendering their ability to carry oxygen to tissues and cells. SCD involves many fatal clinical complications including very painful vaso-occlusive crisis (VOC), the later caused by sickled erythrocytes-mediated ischemic tissue injury and obstruction of blood flow that leads. Pain in VOC is caused by hypoxia, acidosis, fever, infections, dehydration, obstructive sleep apnea, abrupt changes in weather (hot / cold), menstruation and pregnancy etc. Pain in VOC is very severe and is associated with many other life-threatening clinical complications. Therefore, it is needed be managed as early as possible, otherwise persistent pain can weaken patients physically and psychologically. There are no specific laboratory indicators for VOC and diagnosis is made on the basis of history and physical examination. We formulated clinical guidelines for the management of acute painful crisis (VOC) in sickle cell patients based upon updated published medical literature, in addition to our experience of treating sickle cell patients King Abdulaziz National Guards Hospital, Al-Ahsa, Saudi Arabia, which is its application to an Asian publication. This report describes details of these clinical guidelines for management of acute painful vaso-occlusive crisis in sickle cell patients.
Keywords: Sickle cell disease; Vaso-Occlusive Crisis; Acute pain management; Pediatric
Introduction![]()
Sickle cell disease (SCD) is an autosomal recessive disorder caused by a single gene mutation that transforms normal red blood cells into sickle-shaped cells [1]. It leads to many fatal clinical complications including vaso-occlusive crisis (VOC) [2]. The sickled erythrocytes cause ischemic tissue injury by obstructing blood flow that leads to VOC [3]. The reduction in blood flow due to sickle-shaped erythrocytes causes hypoxia and acidosis that promotes the process of sickle-cell formation and ischemic tissue injury.
Intensity and duration of VOC varies not only between different patients but even in same patient during different episodes of VOC [4]. Pain in VOC is caused by hypoxia, acidosis, fever, infections, dehydration, obstructive sleep apnea, abrupt changes in weather (hot / cold), menstruation and pregnancy [3]. Abdominal pain and pain in bones like in back, extremities and swelling of finger and toe joints (dactylitis or hand-foot syndrome) are mostly experienced due to VOC [5]. The bone pain is the most common manifestation and may be accompanied by inflammation, redness, warmth and low fever. Bone pain may be symmetrical (affecting the similar joints on left and right side of the body), asymmetrical (pain affecting bone/joint of one side of the body) or migratory (pain spreading from one joint to the other). Dactylitis is more common in SCD patients with age of 3 years and below while older patients present with abdominal and back pain [6]. Although abdominal pain, if present in SCD children, is mild, but it may be accompanied with other manifestations like pelvic inflammatory disease, urinary tract infection, cholecystitis, pancreatitis, appendicitis, splenic sequestration, liver sequestration, pneumonia and chest crisis and it is necessary to rule-out these complications [4]. Moreover, in case of severe painful crisis, patients may experience acute chest syndrome due to sickling in the small blood vessels of the lungs [7, 8]. It may involve the most devastating central nervous system complications including overt stroke in 10% SCD children and silent cerebral infarcts in about 35% SCD patients [9]. CNS manifestations lead to many neuropsychological complications. Therefore, it is necessary to rule out these complications in SCD children presented with painful VOC.
Due to its severity and/or its association with many other serious clinical manifestations, treatment for pain in VOC should started as soon as diagnosis is made, otherwise persistence of pain can weaken patients physically and psychologically [3, 4]. There are no specific laboratory features indicative of VOC and therefore diagnosis is merely made on the basis of history and physical examination [10, 11]. At King Abdulaziz National Guards Hospital Al-Ahsa, we developed some clinical guidelines for the management of acute painful crisis (VOC) in sickle cell patients. These guidelines are based upon our experience of managing VOC in sickle cell patients and other published guidelines from prestigious health centers in North America. Below we are presenting an outline of these guidelines.
Methods![]()
Literature Search Strategy and Selection Criteria
We utilized different databases like PubMed (NCBI), Scopus, Google scholar and google to search the articles and published material related to our review paper. Different keywords utilized to search data were “Sickle cell disease, Vaso-Occlusive Crisis, Acute Pain, management and Pediatric”. Original peer / reviewed articles, review articles, meta-analysis and clinical trials were considered for this review was addressing clinical management of acute pain in SCD patients with VOC. Case studies were excluded.
Discussion![]()
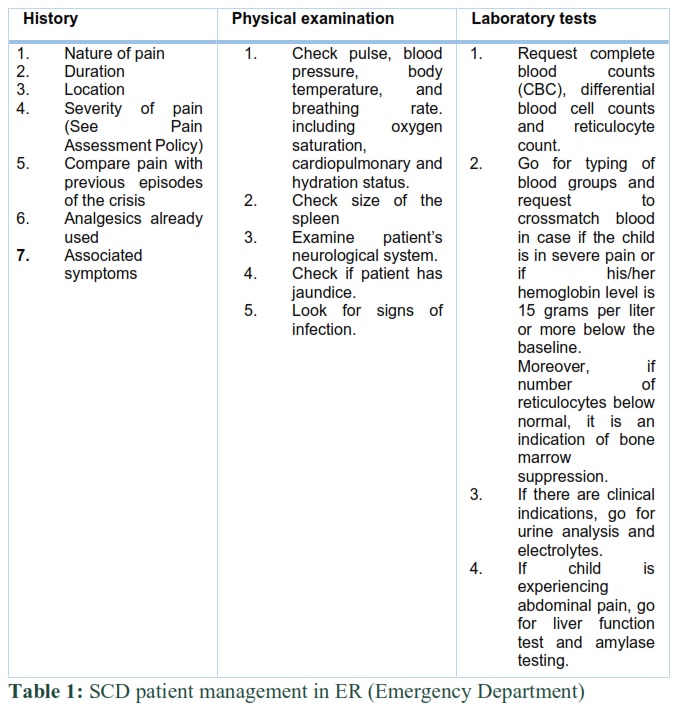
SCD patient management in ER (Emergency Department) (Grade C) [12]
ER assessment of SCD patients with fever: If SCD patient has consistent fever of 38.5 °C, transfer patient on ER bed and follow “Clinical Guidelines for Fever Management”. Carry out a thorough assessment of the patient after administration of antibiotics (Appendix 1).
ER assessment of SCD patients without fever: Transfer SCD patient without fever to a BED at the earliest. Take brief history and carry out physical examination concurrently with measures as given in Table 1. If child is having fever, respiratory illness or/and fever, go for x-ray of the chest as well as monitor his/her oxygen (O2) saturation. If patient is complaining of severe respiratory distress, request for arterial blood gas (ABC) level testing additionally [13, 14].
If you find patient febrile (feverish), dehydrated or complaining of moderate to severe pain, insert an intravenous (I.V.) catheter. Page and inform the Hematology consult service if available. Hematology consultant should examine all SCD patients who are have serious condition and should arrange their proper follow-up. Following are criteria to see if any patient has serious illness:
- Patients in shock (i.e. life-threatening medical condition) with symptoms are very low blood pressure etc.
- Patients with aplastic crisis, acute splenic sequestration crisis, sepsis, meningitis, stroke etc.
- Decompensating patients, for example, patients who progressing into chest crisis etc.
- Patients showing oxygen saturation less than 90% while breathing room air.
In case of fever, acute chest crisis, gallstones etc., please follow other guidelines of “Sickle Cell Management Protocols” specific to these complications [14-16].
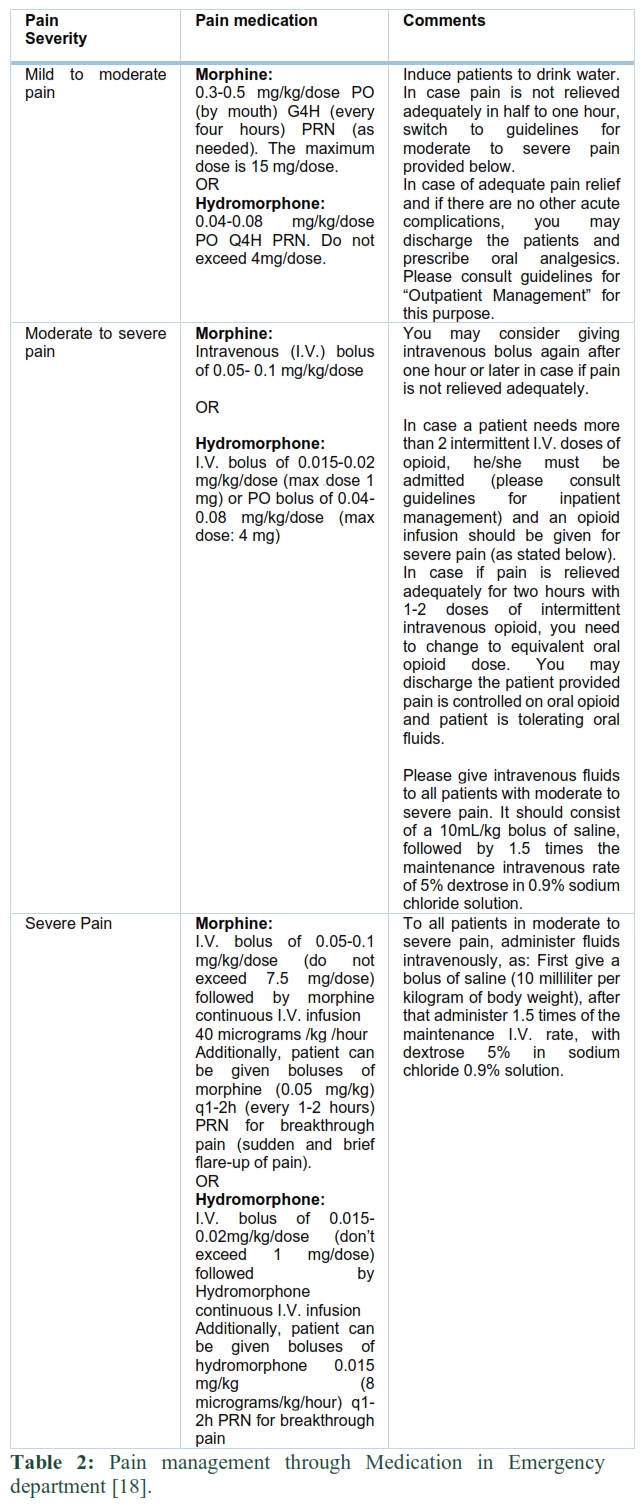
Pain management through Medication in Emergency department (ER)
Please adopt protocols provided in table 2 to manage pain, depending upon pain severity [17, 18].
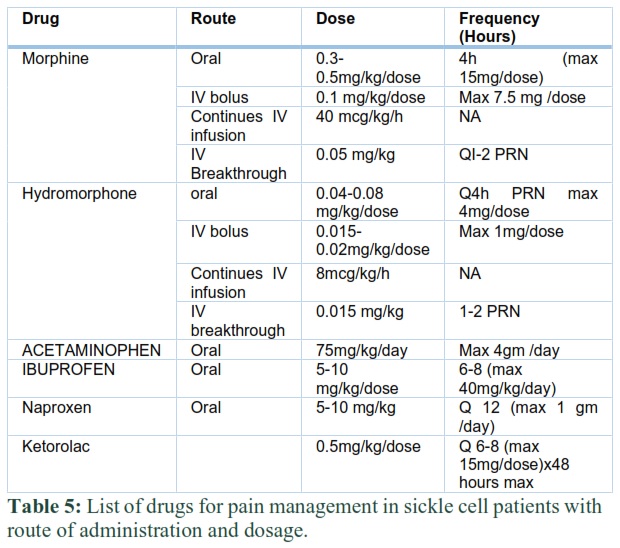
Adjunct pain relief management: For mild, moderate and severe pain, Acetaminophen 75 mg/kg/day PO (maximum dose 4g/day) and an non-steroidal anti-inflammatory drug (NSAID) can be given as adjunct pain relief medication along with morphine, unless there are any contraindications to their use. Before using NSAIDs, assess renal function and consult with pharmacist if you find results abnormal [17].
Recommended NSAIDs include:
Ibuprofen: For children 6 months-12 years old: 5-10 mg/kg/dose PO q6-8h (orally, every 6-8 hours); Not to exceed 40 mg/kg/day or 2400 mg/day.
Naproxen: 10-20 mg/kg/day PO divided BID (orally, twice daily); Not to exceed 1 g/day).
Ketorolac: 0.5 mg/kg/dose intravenous (I.V.) q6-8h (every 6-8 hours); Not to exceed 15 mg/dose), maximum for 48 hours and after that change switch to ibuprofen or naproxen.
Pain management for Indoor patients [18-20]
You need to admit patient if pain is inadequately controlled with oral analgesics or in case of other complications such as fever, dehydration etc.
Patients should be admitted to hospital ward only under General Pediatrics Service.
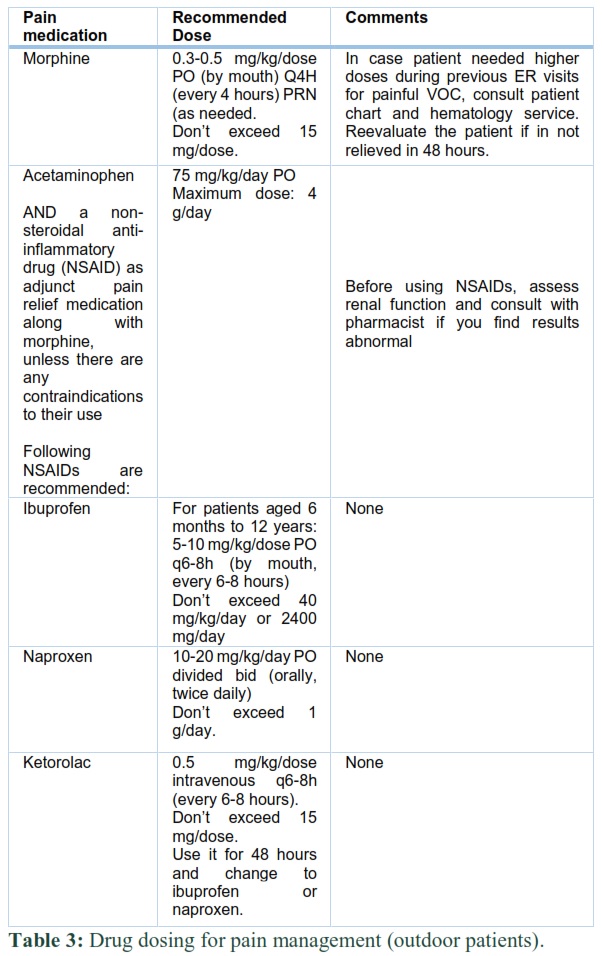
Pain management through Medication for outdoor patients [18, 19]
- Prescribe oral morphine dose that adequately relieved pain as stated in 2.1.7 (don’t exceed 15 mg/dose). In case patient needed higher doses during previous ER visits for painful VOC, consult patient chart and hematology service. Reevaluate the patient if in not relieved in 48 hours.
- For mild, moderate and severe pain, Acetaminophen 75 mg/kg/day PO (maximum dose 4g/day) AND a non-steroidal anti-inflammatory drug (NSAID) can be given as adjunct pain relief medication along with morphine, unless there are any contraindications to their use. Please consult table 3 for dosing.
Patients are needed to be observed closely for signs of deterioration and are required to be monitored continuously with cardiac and oxygen (O2) saturation, for vital signs every four hours, for fluid input and output as well as daily weight. It is required to carry out assessment of patient’s comfort level every 4 hours. This assessment is also required before as well as after every treatment provided for pain management and even after any non-pharmacological management of with pain.
If patient is hospitalized with chest and back pain, refer to him/her to Physiotherapy. It is recommended for physiotherapist to determine if incentive spirometry (10 breaths every 1-2 hours while awake) is appropriate for older children (8 years or older). For younger children, physiotherapist should motivate them use bubbles for deep breathing. The physiotherapist should also encourage walking without any support (ambulation) and any other activities keeping in consideration patient’s tolerance. Per recommendations of physiotherapists, other health professionals involved should also promote child’s mobility [13].
Referral of the patient to Physiotherapy is required if he/she is showing significant decrease in mobility or restricted joint movement.
To improve patient comfort level, non-pharmacological interventions such as massage, heating pads, warm baths, and other such methods should be utilized. It is advisable for “Child Life representative” to recommend structured daily activity for the patient. Use of Imagery and distraction prove to be helpful.
In case if pain is not relieved even after using analgesics or if any pain-related are encountered, consultation with Pain Management Team is highly recommended.
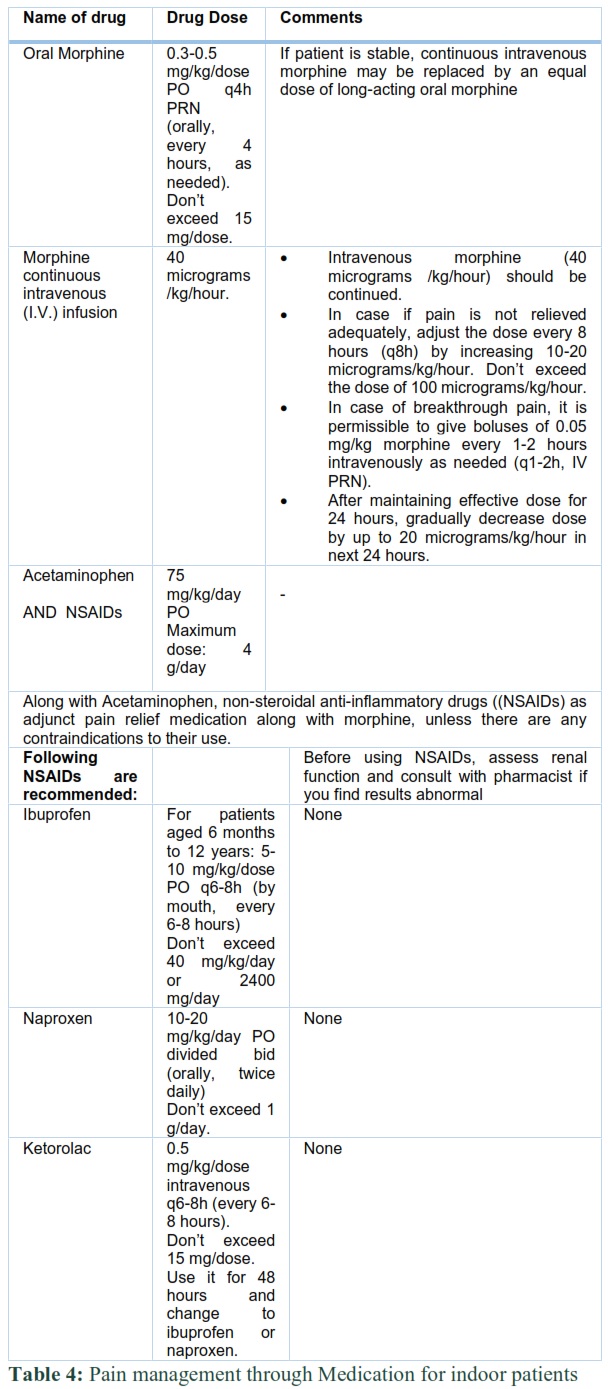
Give patient boluses of morphine intravenously for breakthrough pain (consult table 4 for exact doses). After maintaining effective dose for 24 hours, gradually decrease dose by up to 20 micrograms/kg/hour in next 24 hours. If patient is stable, continuous intravenous morphine may be replaced by an equal dose of long-acting oral morphine (consult table 4 for exact doses).
Step-down therapy: For those patients who are comfortable, it is recommended to change to oral analgesics (morphine 0.3-0.5 mg/kg/dose orally every 4 hours as needed (PO, q4h, PRN prn). Don’t exceed 15 mg/dose (consult table 4 for exact doses).
For mild, moderate and severe pain, Acetaminophen 75 mg/kg/day PO (maximum dose 4g/day) AND a non-steroidal anti-inflammatory drug (NSAID) can be given as adjunct pain relief medication along with morphine, unless there are any contraindications to their use (consult table 4 for exact doses).
In case of pain persisting for more than 24-48 hours in patients older than 6 years of age, using Patient Controlled Analgesia (PCA) pump is recommended [21-23]. Similarly, utilize a PCA pump for any child already treated with a PCA pump or for children who did not achieve adequate analgesia. A PCA pump has capability to deliver a continuous infusion as well as intravenous boluses of morphine or any other medication per patient need and a required dose and interval of medication can be pre-programmed by the prescriber (physician) and therefore chances of overdosing are negligible if PCA pump is used. Please contact (through pager) the Pain Management Team to get PCA pump and they can set it at its basal rate, bolus rate, and lockout time. It is mandatory to observe patients carefully for opioid toxicity when patients are on morphine. The indications of opioid toxicity include hypotension, bradycardia, drowsiness, coma, pinpoint pupils, cold clammy skin, and hypoventilation. It is required to regularly monitor and record patient's heart rate, respiratory rate and oxygen saturation while observing patient for opioid toxicity.
Use of stool softeners: If the patient does not have diarrhea, it is required to administer him/her a stool softener such as Docusate Sodium (5 mg/kg/day for children). You administer it in three equal doses or as a single daily dose. Adult daily dose is 100-200 mg.
Use of antihistamines: For patients with pruritus, prescribe antihistamines PRN (as needed).
Hydration: For hydrating patients, fluids should be continually given intravenously or orally at 1-1.5 times the maintenance rate. Fluid maintenance rate can be calculated using specific charts and formulas provided in medical literature [24, 25].
Oxygen: Systematic use of oxygen is not recommended for VOC in sickle cell patients, based upon many studies and reports. Nevertheless, SCD children with VOC may develop hypoxia that can promote sickling process. Accordingly, it is highly recommended to regularly monitor oxygen saturation in such patients and if patients have indications of hypoxemia, oxygen should be provided [26, 27].
Use of Corticosteroids: For sickle cell patients, effectiveness of corticosteroids as an adjunct therapy for reducing pain duration is not clear. Therefore, it is recommended to avoid using corticosteroids routinely unless data from some new clinical trials supports their use [27].
Guidelines foe discharge patients:
The patients can be discharged in following cases:
- If patients are tolerating fluids and medications orally.
- If there is adequate pain relief using oral medications.
- If all concurrent problems of the patient are resolved.
Sickle cell disease (SCD) is an familial disorder resulted due to a single mutation in beta globin gene. It leads to many fatal clinical complications including painful vaso-occlusive crisis (VOC), requiring acute clinical management. VOC pain is caused by hypoxia, acidosis, fever, infections, dehydration, obstructive sleep apnea, abrupt changes in weather (hot / cold), menstruation and pregnancy etc. Pain in VOC is very severe and leads to many other life-threatening clinical complications if not timely diagnosed and properly treated. Nevertheless, there are clear laboratory indicators for VOC. We formulated clinical guidelines for the management of acute painful crisis (VOC) in sickle cell patients by utilizing published clinical data as well as our experience of treating sickle cell patients at a tertiary care hospital in Al-Ahsa, Saudi Arabia, as it fits Asian populations better. This article describes details of these clinical guidelines for management of acute painful vaso-occlusive crisis in sickle cell patients. It details practical clinical measures to be taken by medical specialists in different fields of medicine and their associated healthcare staff to treat painful VOC in sickle cell patients.
Important notes:
- Please consider allergies, drug effects, side effects and contra-indications prior to administration.
- Patients on regular opiates should receive stool softeners.
None.
References ![]()
- Piccin A, Murphy C, Eakins E, Rondinelli MB, Daves M, Vecchiato C, et al. Insight into the complex pathophysiology of sickle cell anaemia and possible treatment. European Jouranl of Haematology (2019);102(4): 319-330.
- Faes C, Ilich A, Sotiaux A, Sparkenbaugh EM, Henderson MW, Buczek L, et al. Red blood cells modulate structure and dynamics of venous clot formation in sickle cell disease. Blood (2019);133(23): 2529-2541.
- Darbari DS, Sheehan VA, Ballas SK. The vaso-occlusive pain crisis in sickle cell disease: Definition, pathophysiology, and management. European Jouranl of Haematology. (2020); 105(3): 237-246.
- Niccoli AA, Altini C, Nappi AG, Lavelli V, Ferrari C, Marzullo A, et al. Sickle cell diseases: What can nuclear medicine offer? Hell Journal of Nuclear Medicine (2019); 22(1): 2-3.
- Opoka RO, Ndugwa CM, Latham TS, Lane A, Hume HA, Kasirye P, et al. Novel use Of Hydroxyurea in an African Region with Malaria (NOHARM): a trial for children with sickle cell anemia. Blood (2017); 130(24): 2585-2593.
- Takahashi T, Okubo Y, Handa A. Acute chest syndrome among children hospitalized with vaso-occlusive crisis: A nationwide study in the United States. Pediatric Blood Cancer (2018); 65(3): e26885.
- Nur E, Gaartman AE, van Tuijn CFJ, Tang MW, Biemond BJ. Vaso-occlusive crisis and acute chest syndrome in sickle cell disease due to 2019 novel coronavirus disease (COVID-19). Amercan Journal of Hematology (2020); 95(6): 725-726.
- Estcourt LJ, Kimber C, Hopewell S, Trivella M, Doree C, Abboud MR. Interventions for preventing silent cerebral infarcts in people with sickle cell disease. Cochrane database of systematic reviews. (2020); 4(4): CD012389.
- Patel DK, Mohapatra MK, Thomas AG, Patel S, Purohit P. Procalcitonin as a biomarker of bacterial infection in sickle cell vaso-occlusive crisis. Mediterranean Journal of Hematology and Infectious Diseases, (2014); 6(1): e2014018.
- Lovett PB, Sule HP, Lopez BL. Sickle Cell Disease in the Emergency Department. Hematology Oncology Clinics of North America, (2017); 31(6): 1061-1079.
- Simon E, Long B, Koyfman A. Emergency Medicine Management of Sickle Cell Disease Complications: An Evidence-Based Update. Journal of Emergency Medicine, (2016); 51(4): 370-381.
- Bellet PS, Kalinyak KA, Shukla R, Gelfand MJ, Rucknagel DL. Incentive spirometry to prevent acute pulmonary complications in sickle cell diseases. New England Journal of Medicine (1995); 333(11): 699-703.
- Yawn BP, Buchanan GR, Afenyi-Annan AN, Ballas SK, Hassell KL, James AH, et al. Management of sickle cell disease: summary of the 2014 evidence-based report by expert panel members. The Journal of the American Medical Association (2014); 312(10): 1033-48.
- Wing R, Dor MR, McQuilkin PA. Fever in the pediatric patient. Emergency Medicine Clinics of North America (2013); 31(4): 1073-96.
- Subramaniam S, Chao JH, Chaudhari P. Managing acute complications of sickle cell disease in pediatric patients [digest]. Pediatric Emergency Medicine Practice (2016);13(11 Suppl Points & Pearls): S1-S2.
- Puri L, Nottage KA, Hankins JS, Anghelescu DL. State of the Art Management of Acute Vaso-occlusive Pain in Sickle Cell Disease. Paediatric Drugs (2018); 20(1): 29-42.
- Brandow AM, DeBaun MR. Key Components of Pain Management for Children and Adults with Sickle Cell Disease. Hematology Oncology Clinics of North America (2018); 32(3): 535-550.
- Frei-Jones MJ, DeBaun MR. Personal pain action plans for children and adolescents with sickle cell disease. In Acute Pain: Causes, Effects And Treatment. Nova Science Publishers, Inc. (2009) p. 213-220.
- Miller ST, Kim HY, Weiner D, Wager CG, Gallagher D, Styles L, Dampier CD; Investigators of the Sickle Cell Disease Clinical Research Network (SCDCRN). Inpatient management of sickle cell pain: a 'snapshot' of current practice. American Journal of Hematology (2012); 87(3): 333-6.
- Santos J, Jones S, Wakefield D, Grady J, Andemariam B. Patient Controlled Analgesia for Adults with Sickle Cell Disease Awaiting Admission from the Emergency Department. Pain research & management (2016); 32(18):186.
- Melzer-Lange MD, Walsh-Kelly CM, Lea G, Hillery CA, Scott JP. Patient-controlled analgesia for sickle cell pain crisis in a pediatric emergency department. Pediatric Emergency Care. (2004); 20(1): 2-4.
- Turaç A, Rumeli Atıcı Ş. Cocuklarda OHA, Etkinliğini HKAY, Değerlendirmesi K. [Evaluation of the effectiveness of patient-controlled analgesia in children with sickle cell anemia from the perspective of healthcare professionals and parents]. Agri : Agri (Algoloji) Dernegi'nin Yayin organidir = The journal of the Turkish Society of Algology (2016); 28(3): 150-154.
- Pecker LH, Lanzkron S. Sickle Cell Disease. Annals of internal medicine, (2021); 174(1):1-16.
- Chesney RW. The maintenance need for water in parenteral fluid therapy. Pediatrics (1998); 102(2 Pt 1): 399-400.
- Okomo U, Meremikwu MM. Fluid replacement therapy for acute episodes of pain in people with sickle cell disease. Cochrane Database Systematic Reviews (2017); 7(7): CD005406.
- Howard J, Lee SA, Inusa B, Cheng MYE, Bavenjit C, Reading IC, et al. Prevention of Morbidity in Sickle Cell Disease (POMS2a)-overnight auto-adjusting continuous positive airway pressure compared with nocturnal oxygen therapy: a randomised crossover pilot study examining patient preference and safety in adults and children. Trials (2019); 20(1): 442.
- Osunkwo I, O'Connor HF, Saah E. Optimizing the management of chronic pain in sickle cell disease. Hematology American Society of Hematology Educational Program (2020); 2020(1): 562-569.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0