

Review Article
A review on Aluminum phosphide (Rice Tablets) Poisoning; From Exposure to the Applicable and New Strategies of Clinical Management
Aliasghar Manouchehri1, Shiva Ghareghani2, Shabnam Shamaei3, Maede Nilechi4, Fatemeh Bossaghzadeh5*
Adv. life sci., vol. 8, no. 4, pp. 326-332, December 2021
*– Corresponding Authors: Fatemeh Bossaghzadeh (Email: bossaghzadeh.f@ymail.com)
Authors' Affiliations
2. Department of Pharmacology, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran
3. Department of Chemistry, Khorramabad Branch, Islamic Azad University, Khorramabad, Iran
4. Department of Biology, Science and Research Branch, Islamic Azad University, Tehran – Iran
5. Department of Biology, Dezful Branch, Islamic Azad University, Dezful – Iran
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
Rice tablets (especially aluminum phosphide) as a solid fumigant pesticide is one of the major areas of interest within the field of pesticide poisoning due to high fatality. It is commonly used in grain storage places including silos, warehouses, and grain transporting systems such as ships to control damages of pests and rodents. Unfortunately, it is considerably consumed for suicidal purpose in developing countries because of the ease of access. Aluminum phosphide (ALP) has been conceived as the most mortal one among others and accounts for many deaths each year. ALP toxicity is associated with phosphine gas liberation which is highly toxic and may cause various toxicities in all body organs, especially in cardiovascular and respiratory systems. As there is no certain antidote to prevent human's death, hence having thorough information about this pesticide is required. Thus, in this article physiochemical features of rice tablets, various toxicological, clinical/pathological impacts of ALP on human body and also applicable and new strategies of its managements have been highlighted. Eventually, gathering all published information about ALP intoxication till date demonstrated that restricted preventative measures plus early and improved management protocols can limit the organ injuries and mortality.
Keywords: Phosphine; Rice tablet; Aluminum phosphide; Human poisoning; Pesticide; Toxicity of ALP; Management strategies
Introduction![]()
Metal phosphides are one of the most widely used groups of pesticide agents used for safe storage and transportation of rice and grains in developing countries because of agricultural revolutions and pest controls [1]. Among all members belonging to metal phosphides including aluminum, magnesium, calcium, and zinc phosphite, aluminum phosphide (ALP) has been conceived as the most fatal one [2]. As it is readily available in low to middle-income countries (such as Asian markets), deliberate and accidental poisoning of this pesticide has been identified as the most lethal poisoning due to its high mortality [3].
In spite of the fact that the use of aluminum phosphide has been forbidden in many countries (such as Iran), it is sold illegally in some markets usually in the form of 3g tablets, which is referred to as rice tablet, with different brand names [4,5]. Although Most reports of ALP intoxication are associated with young adult populations from rural Asian areas, also there has been some phosphine poisoning reports in European countries including Germany [6,7], UK. [8], France [9], and Denmark [10] over the last three decades. In regard to large burden of pesticide and fumigant poisoning in developing countries (such as India and Iran), it is becoming extremely difficult to say that ALP poisoning happens accidentally. Self-poisoning by pesticides has become increasingly prevalent response due to ease of availability in some developing countries. Researchers have maintained that most of the self-harm cases do not plan to commit a suicide leading to die, but as they are unaware of destructive and deadly effects of some pesticides (such as ALP) have unplanned die [11]. However, it is worth to say that it seems phosphine poisoning predominantly occurs unintentionally in developed countries.
Methods![]()
Search strategy and selection criteria
A literature search of this narrative review was conducted by key terms of “aluminum phosphide”, “rice tablet”, “human poisoning”, “mechanism of ALP poisoning”, “new strategies for treatment of ALP poisonings”, “organ toxicity in ALP toxication”, “routs of exposure to ALP” in Google Scholar and Pub Med databases and all the relevant articles were selected. The selected articles were reviewed for contents and the articles with duplicated information were excluded.
Discussion![]()
Physio-chemical features of rice tablets
ALP, the active component of rice tablet, is a solid fumigant formulated by ammonium carbonate with ratio of 56: 44% to prevent probable combustion of diphosphine gas (which is produced as a result of phosphine gas interactions with atmospheric moisture) during transportation or storage [12,13]. ALP interacts with atmospheric moisture and liberates phosphine gas which is the leading cause of rice tablet poisoning and death in pests and human as well [1]. Moreover, there is an evidence demonstrating that the release of phosphine gas elevates in acidic environments [3]. Equation of ALP reaction to moisture and hydrochloric acid:
ALP + 3H2O Al (OH)3 + PH3
ALP + 3 HCL AlCl3 + PH3
The physical features of rice tablets are addressed in table 1.
Routs of Exposure and Toxicity Levels
According to numerous researches done by scholars, rice tablet toxicities originate from three main routs including (I) direct oral consumption, (II) inhalation of air containing phosphine, and hardly ever (III) absorption via skin or eyes. However, absorption through oral ingestion has been regarded as the most common cause of toxicity. In the literature on ALP poisoning, human lethal dose has been determined about 150- 500 mg (depending on the exposure of tablet to moisture and expiry date) [14]. Furthermore, the recommended workplace exposure limit for people working at ALP manufacturing industries, grain storage warehouses, and ships has been suggested to be below 0.3 ppm [15].
Mechanisms of Toxicity in Human Body
As soon as ALP contacts to the gastro-intestinal moisture and stomach hydrochloric acid, the release of phosphine gas (PH3) occurs in gastrointestinal tract and cytochrome oxidase blocks and inhibition of oxidative phosphorylation begin. Hence, some sensitive organs requiring more oxygen including brain, kidney, heart, lungs and liver are more vulnerable to these toxic effects which may contribute to histopathological alters and cell death [3,16]. It certainly appears to be the case that the valence of hemoglobin hem component alters as a result of the cytochrome oxidase blocks. Moreover, it has been demonstrated that extra-mitochondrial liberation of free oxygen radicals and oxidative stress stemming from cytochrome oxidase blocks may lead to lipid peroxidation and protein denaturation of the cell membrane in several organs. So, any organ could be affected via ALP intoxication [17-19].
Acute Toxicity
Non-specific clinical features of ALP poisoning remain controversial, because it mainly relies on way of exposure, dose, and duration of exposure. Different clinical signs of acute toxicity relating to each exposure rout are listed in table 2.
Chronic Toxicity
Respiratory symptoms entailing chest pain, cough, mandibular necrosis (known as phossy jaw), and dyspnea frequently happens as a result of low-level respiratory poisoning in chronic mode. Besides, it has been reported that prolonged exposure to 0.4 ppm phosphine gas through skin can contribute to dermatitis alterations. This kind of intoxication may occur in storage facility workers [1].
Organ Toxicity
Earliest organs commonly involved in rice tablet poisoning are gastrointestinal and respiratory systems in oral and inhalational routs of exposure, respectively. however, there has been much discussion as to the ALP poisoning effects on various human organs and evidence seems to be supporting ALP rice tablets could be affected any organ [1].
Cardiovascular toxicity is the leading cause of High morbidity and mortality in patients with ALP poisoning. Electrocardiographic evidence shows that sinus tachycardia is the most common rhythm abnormality on
electrocardiogram (ECG) in the first 3-6 hour. However, dysrhythmia, ST-T wave changes (6-12 hours) and arrhythmias occur respectively as the subsequent
complications [2,21-23]. In fact, Siwach et al. (1998) have been maintained that malignant arrhythmias such as supraventricular and ventricular tachycardia may involve 86.7 % cases (46.7% and 40% respectively). Moreover, 23.3% of ALP-poisoned patients are vulnerable to ventricular fibrillation, but arterial fibrillation may occur in 20% of them [24]. The most common clinical toxic impacts and symptoms of ALP on different organs including cardiovascular, respiratory, nervous, gastrointestinal, and renal systems etc. are addressed in table 3.
How to diagnose ALP poisoning?
ALP intoxication may be misdiagnosed because of metabolic abnormalities, inflammation and also sepsis, thus appropriate history and clinical suspicious are needed. According to the fact that other metal phosphides create the same symptoms in less intense, differentiation of ALP to others requires precise and detailed history and also biochemical testing by hydrochloric acid, ammonium hydroxide, and ammonium chloride [40,44]. Silver nitrate (0.1 NAgNO3) saturated paper can be prescribed for diagnose of ALP poisoning in doubtful cases. If there is a phosphine in breath, silver nitrate paper will turn to black due to the silver phosphate formation. Furthermore, it can be diagnosed by heating gastric aspirated samples above 50˚C in order that phosphine could be released above the flask. Then, these fumes can be detected by silver nitrate papers [45,46]. It has been proved that quantitative methods are the most reliable ones for differentiation. With reference to this fact, gas chromatography with nitrogen phosphorus detector is the most sensitive and specific test which is accessible for phosphine detection [47].
Management/Treatment Strategies
There is no need for any confirmatory test to start the treatment of ALP-Poisoned patient and it should be done immediately after any clinical suspicious history, because early identification plays a key role when encountering to phosphine gas contributing to organ failure and further complications. ALP-poisoning managements can be categorized in the following 3 parts:
Reducing the Toxin exposure
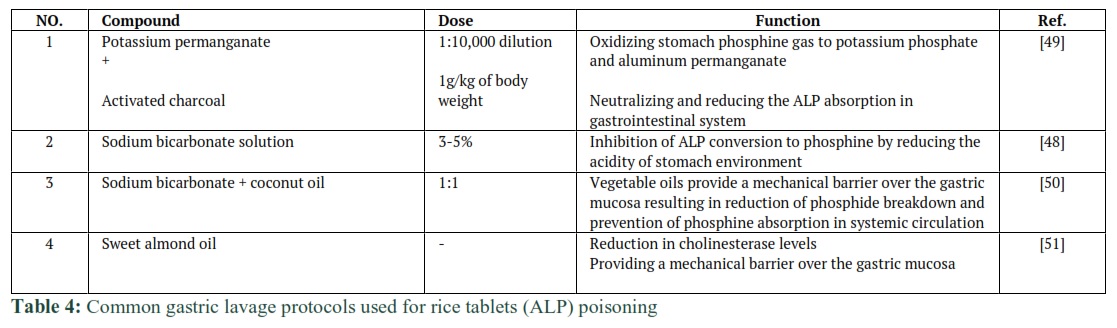
The respiratory poisoned victims (which are mostly workers of ALP-related industries or warehouses and grain storage silos) should be transfer from the offending environment to outdoor. Besides, gut decontamination in the form of gastric lavage within the first hour of toxin ingestion plays a crucial role in poisoning management. There are two challenges with ALP (rice tablets) poisoning gastric lavage [48]: (I) water cannot be used for this situation due to the avoiding phosphine gas formation, (II) it is very important to protect the patient 's air way from direct contact of stomach liquid containing acid and phosphine gas.
Various gastric lavage protocols have been suggested by scholars over the last three decades which are reported in table 4.
Increasing the Toxin Excretion
Elevating phosphine excretion via urine and lungs is a classic concern in ALP intoxication. Traditionally, researchers have subscribed to the belief that phosphine excretion via urine can be occurred by proper intravenous hydration and also dopamine infusion in renal dose. Moreover, elevation of respiratory rate in patients supported by mechanical ventilation may be helpful in phosphine excretion via lungs [12].
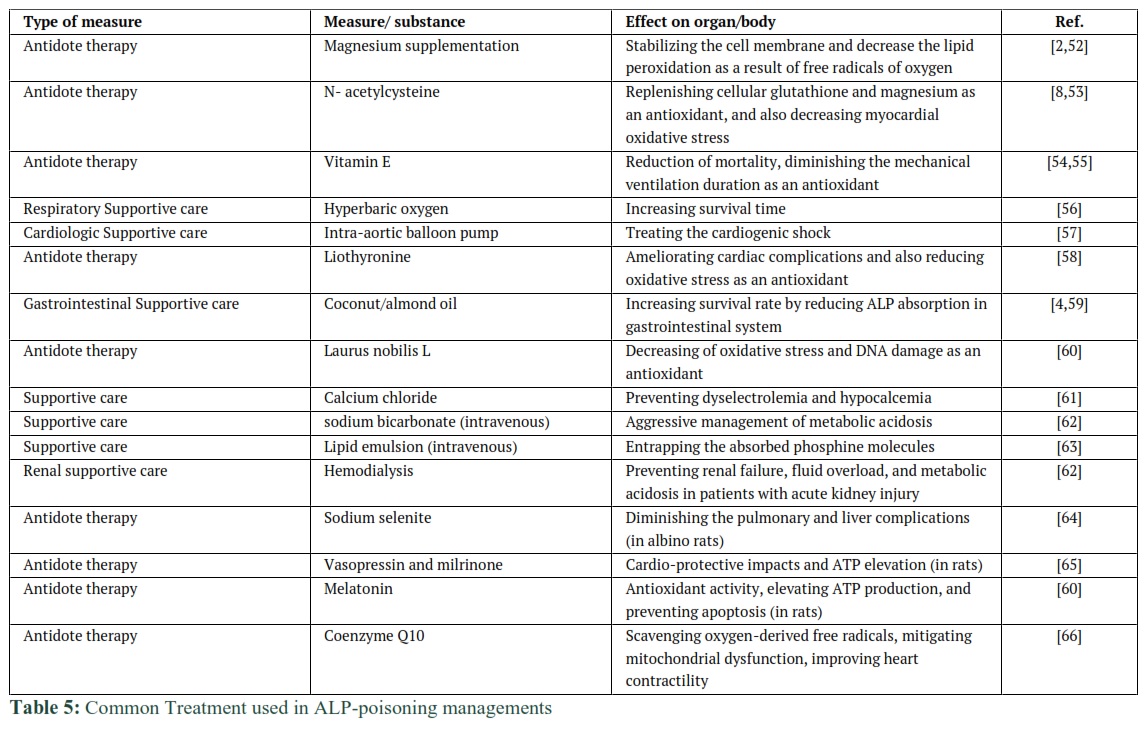
Supportive Treatments Done for Each Organ
Generally, supportive treatment has a vital role in ALP-poisoning management and has been widely recognized as the most effective treatment in poisoning emergencies for decades. Thus, in this article the most common measures have been done recently to save the patient's life and also prevent the organ failure are listed in table 5. However, toxins and chemicals and medicines have harmful effects on human health (67-71) Medicinal plants that can reduce the toxic effects of chemicals and side effects of drugs and chemicals can be used in the form of natural antioxidants (72-79).



Despite the absence of specific (100% effective) antidote, still there is a lack in preventative restricted rules to forbid the misuse of ALP tablets in general population. In this condition, it seems that the most effective measures are preventative ones including limitation of its selling to public, using non-fatal alternatives instead of ALP, training of general population and appropriate documentation as well. Beside these preventative measures, it is worth to mention that time plays a crucial role in management/treatment of the poisoned patients and their life saving. Because, early and correct diagnose can help with being able to select early, effective and improved clinical management strategies resulting in reduction in the case fatality rates. At the end, in order to decline the overall incidence of successful suicide or any unintended poisoning much needs to be done, especially in developing countries, by national governments.
All authors contributed equally.
The authors have no conflict of interests.
References ![]()
- Garg KK. Review of aluminum phosphide poisoning. International Journal of Medical Science and Public Health, (2020); 9(7).
- Gupta S, Ahlawat SK. Aluminum phosphide poisoning—a review. Journal of Toxicology: Clinical Toxicology, (1995); 33(1): 19-24.
- Amiri H, Vaseie L, Habibollahi P, Ghodrati N. Rice tablet: An overview to common material in Iran. Journal of Research in Clinical Medicine, (2016); 4(2): 77-81.
- Mehrpour O, Jafarzadeh M, Abdollahi M. A systematic review of aluminium phosphide poisoning. Archives of Industrial Hygiene and Toxicology, (2012); 63(1): 61-73.
- Mehrpour O, Aghabiklooei A, Abdollahi M, Singh S. Severe hypoglycemia following acute aluminum phosphide (rice tablet) poisoning; a case report and review of the literature. Acta Medica Iranica, (2012); 568-571.
- Alter P, Grimm W, Maisch B. Lethal heart failure caused by aluminium phosphide poisoning. Intensive care medicine, (2001); 27(1): 327-327.
- Lauterbach M, Solak E, Kaes J, Wiechelt J, Von Mach M-A, et al. Epidemiology of hydrogen phosphide exposures in humans reported to the poison center in Mainz, Germany, 1983–2003. Clinical toxicology, (2005); 43(6): 575-581.
- Bogle R, Theron P, Brooks P, Dargan P, Redhead J. Aluminium phosphide poisoning. Emergency Medicine Journal, (2006); 23(1): e03-e03.
- Anger F, Paysant F, Brousse F, Normand IL, Develay P, et al. Fatal aluminum phosphide poisoning. Journal of analytical toxicology, (2000); 24(2): 90-92.
- Andersen T, Holm J. Poisoning with aluminum phospholipide used as a poison against moles. Ugeskrift for laeger, (1996); 158(38): 5308-5309.
- Gunnell D, Eddleston M. Suicide by intentional ingestion of pesticides: a continuing tragedy in developing countries. International journal of epidemiology, (2003); 32(6): 902-909.
- Hashemi-Domeneh B, Zamani N, Hassanian-Moghaddam H, Rahimi M, Shadnia S, et al. A review of aluminium phosphide poisoning and a flowchart to treat it. Archives of industrial hygiene and toxicology, (2016); 67(3): 183-193.
- Shadnia S, Soltaninejad K. Spontaneous ignition due to intentional acute aluminum phosphide poisoning. The Journal of emergency medicine, (2011); 40(2): 179-181.
- Sudakin D. Occupational exposure to aluminium phosphide and phosphine gas? A suspected case report and review of the literature. Human & experimental toxicology, (2005); 24(1): 27-33.
- Pepelko B, Seckar J, Harp PR, Kim JH, Gray D, et al. Worker exposure standard for phosphine gas. Risk Analysis: An International Journal, (2004); 24(5): 1201-1213.
- Neil MJ, Smith A, Heckelman PE. The Merck Index. Encyclopedia of Chemicals, Drugs and Biologicals, 14th edition, Merck Research Laboratories, USA, (2006); 140.
- Price NR, Mills KA, Humphries LA. Phosphine toxicity and catalase activity in susceptible and resistant strains of the lesser grain borer (Rhyzopertha dominica). Comparative Biochemistry and Physiology Part C: Comparative Pharmacology, (1982); 73(2): 411-413.
- Chugh S, Arora V, Sharma A, Chugh K. Free radical scavengers & lipid peroxidation in acute aluminium phosphide poisoning. The Indian journal of medical research, (1996); 104190-193.
- Dua R, Gill KD. Aluminium phosphide exposure: implications on rat brain lipid peroxidation and antioxidant defence system. Pharmacology & toxicology, (2001); 89(6): 315-319.
- Moghadamnia AA. An update on toxicology of aluminum phosphide. DARU journal of Pharmaceutical Sciences, (2012); 20(1): 1-8.
- Katira R, Elhence G, Mehrotra M, Srivastava S, Mitra A, et al. A study of aluminum phosphide (AlP) poisoning with special reference to electrocardiographic changes. The Journal of the Association of Physicians of India, (1990); 38(7): 471-473.
- Bhasin P, Mital H, Mitra A. An echocardiographic study in aluminium phosphide poisoning. J Assoc Physicians India, (1991); 39851.
- Soltaninejad K, Beyranvand M-R, Momenzadeh S-A, Shadnia S. Electrocardiographic findings and cardiac manifestations in acute aluminum phosphide poisoning. Journal of forensic and legal medicine, (2012); 19(5): 291-293.
- Siwach S, Singh H, Katyal V, Bhardwaj G. Cardiac arrhythmias in aluminium phosphide poisoning studied by on continuous holter and cardioscopic monitoring. The Journal of the Association of Physicians of India, (1998); 46(7): 598-601.
- Chhina RS, Thukral R, Chawla LS. Aluminum phosphide-induced gastroduodenitis. Gastrointestinal endoscopy, (1992); 38(5): 635-636.
- Verma S, Ahmad S, Shirazi N, Barthwal S, Khurana D, et al. Acute pancreatitis: A lesser-known complication of aluminum phosphide poisoning. Human & experimental toxicology, (2007); 26(12): 979-981.
- Madan K, Chalamalasetty SB, Sharma M, Makharia G. Corrosive-like strictures caused by ingestion of aluminium phosphide. NATIONAL MEDICAL JOURNAL OF INDIA, (2006); 19(6): 313.
- Nijhawan S, Rastogi M, Tandon M, Mathur A, Rai R. Aluminum phosphide-induced esophageal stricture: an unusual complication. Endoscopy, (2006); 38(S 2): E23-E23.
- Chugh S, Ram S, Mehta L, Arora B, Malhotra K. Adult respiratory distress syndrome following aluminium phosphide ingestion. Report of 4 cases. The Journal of the Association of Physicians of India, (1989); 37(4): 271-272.
- Saleki S, Ardalan FA, Javidan-Nejad A. Liver histopathology of fatal phosphine poisoning. Forensic science international, (2007); 166(2-3): 190-193.
- Khosla S, Chugh S, Nand N, Saini R. Systemic involvement in aluminium phosphide poisoning (a report of 10 cases). The Journal of the Association of Physicians of India, (1986); 34(3): 227-230.
- Proudfoot AT. Aluminium and zinc phosphide poisoning. Clinical toxicology, (2009); 47(2): 89-100.
- Soltaninejad K, Nelson LS, Khodakarim N, Dadvar Z, Shadnia S. Unusual complication of aluminum phosphide poisoning: Development of hemolysis and methemoglobinemia and its successful treatment. Indian journal of critical care medicine: peer-reviewed, official publication of Indian Society of Critical Care Medicine, (2011); 15(2): 117.
- Singh S, Singh D, Wig N, Jit I, Sharma B-K. Aluminum phosphide ingestion—a clinico-pathologic study. Journal of Toxicology: Clinical Toxicology, (1996); 34(6): 703-706.
- Mehrpour O, Dolati M, Soltaninejad K, Shadnia S, Nazparvar B. Evaluation of histopathological changes in fatal aluminum phosphide poisoning. Indian Journal of Forensic Medicine &Toxicology, (2008); 2(2): 34-36.
- Mehrpour O, Neumann N, Ng P. Is cytochrome oxidase inhibition the primary mechanism in aluminum phosphide poisoning? Expert opinion on drug metabolism & toxicology, (2019); 15(8): 613-614.
- Kalra G, Anand I, Jit I, Bushnurmath B, Wahi P. Aluminium phosphide poisoning: haemodynamic observations. Indian heart journal, (1991); 43(3): 175-178.
- Mehrpour O, Shadnia S, Soltaninezhad K, YAGHMAEI A. Evaluation of electrolytes and blood glucose level in aluminum phosphide poisoning. (2009).
- Singh B, Gupta S, Minocha S, Aggarwal N. Hypoglycaemia in aluminium phosphide poisoning. The Journal of the Association of Physicians of India, (1994); 42(8): 663-663.
- Mehrpour O, Keyler D, Shadnia S. Comment on Aluminum and zinc phosphide poisoning. Clinical toxicology, (2009); 47(8): 838-839.
- Singh R, Singh R, Singh U. Hypermagnesemia following aluminum phosphide poisoning. International journal of clinical pharmacology, therapy, and toxicology, (1991); 29(2): 82-85.
- Chugh S, Kamar P, Sharma A, Chugh K, Mittal A, et al. Magnesium status and parenteral magnesium sulphate therapy in acute aluminum phosphide intoxication. Magnesium research, (1994); 7(3-4): 289-294.
- Mostafazadeh B, Pajoumand A, Farzaneh E, Aghabiklooei A, Rasouli MR. Blood levels of methemoglobin in patients with aluminum phosphide poisoning and its correlation with patient’s outcome. Journal of Medical Toxicology, (2011); 7(1): 40-43.
- Chugh S, Aggarwal H, Mahajan S. Zinc phosphide intoxication symptoms: analysis of 20 cases. International journal of clinical pharmacology and therapeutics, (1998); 36(7): 406-407.
- Chugh S, Ram S, Chugh K, Malhotra K. Spot diagnosis of aluminium phosphide ingestion: an application of a simple test. The Journal of the Association of Physicians of India, (1989); 37(3): 219-220.
- Chan L, Crowley R, Delliou D, Geyer R. Phosphine analysis in post mortem specimens following ingestion of aluminium phosphide. Journal of analytical toxicology, (1983); 7(4): 165-167.
- Council NR, Levels CoAEG (2008) Phosphine and Eight Metal Phosphides Acute Exposure Guideline Levels. Acute Exposure Guideline Levels for Selected Airborne Chemicals: Volume 6: National Academies Press (US).
- Maitai C, Njoroge D, Abuga K, Mwaura A, Munenge R. Investigation of possible antidotal effects of activated charcoal, sodium bicarbonate, hydrogen peroxide and potassium permanganate in zinc phosphide poisoning. East and Central African Journal of Pharmaceutical Sciences, (2002); 5(2): 38-41.
- Pajoumand A, Jalali N, Abdollah M, Shadnia S. Survival following severe aluminium phosphide poisoning. Journal of Pharmacy Practice and Research, (2002); 32(4): 297-299.
- Bajwa SJS, Bajwa SK, Kaur J, Singh K, Panda A. Management of celphos poisoning with a novel intervention: A ray of hope in the darkest of clouds. Anesthesia, essays and researches, (2010); 4(1): 20.
- Saidi H, Shojaie S. Effect of sweet almond oil on survival rate and plasma cholinesterase activity of aluminum phosphide-intoxicated rats. Human & experimental toxicology, (2012); 31(5): 518-522.
- Chugh S, Kolley T, Kakkar R, Chugh K, Sharma A. A critical evaluation of anti-peroxidant effect of intravenous magnesium in acute aluminium phosphide poisoning. Magnesium research, (1997); 10(3): 225-230.
- Kim KS, Suh GJ, Kwon WY, Kwak YH, Lee K, et al. Antioxidant effects of selenium on lung injury in paraquat intoxicated rats. Clinical Toxicology, (2012); 50(8): 749-753.
- Bazmi E, Mousavi F, Giahchin L, Mokhtari T, Behnoush B. Cardiovascular complications of acute amphetamine abuse: cross-sectional study. Sultan Qaboos University Medical Journal, (2017); 17(1): e31.
- Halvaei Z, Tehrani H, Soltaninejad K, Abdollahi M, Shadnia S. Vitamin E as a novel therapy in the treatment of acute aluminum phosphide poisoning. Turkish journal of medical sciences, (2017); 47(3): 795-800.
- Saidi H, Shokraneh F, Ghafouri H-B, Shojaie S. Effects of hyperbaric oxygenation on survival time of aluminum phosphide intoxicated rats. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences, (2011); 16(10): 1306.
- Siddaiah LM, Adhyapak SM, Jaydev SM, Shetty GG, Varghese K, et al. Intra-aortic balloon pump in toxic myocarditis due to aluminum phosphide poisoning. Journal of medical toxicology, (2009); 5(2): 80-83.
- Goharbari M, Taghaddosinejad F, Arefi M, Sharifzadeh M, Mojtahedzadeh M, et al. Therapeutic effects of oral liothyronine on aluminum phosphide poisoning as an adjuvant therapy: A clinical trial. Human & experimental toxicology, (2018); 37(2): 107-117.
- Shadnia S, Rahimi M, Pajoumand A, Rasouli M-H, Abdollahi M. Successful treatment of acute aluminium phosphide poisoning: possible benefit of coconut oil. Human & experimental toxicology, (2005); 24(4): 215-218.
- Karimani A, Mohammadpour AH, Zirak MR, Rezaee R, Megarbane B, et al. Antidotes for aluminum phosphide poisoning–An update. Toxicology reports, (2018); 51053-1059.
- Gurjar M, Baronia AK, Azim A, Sharma K. Managing aluminum phosphide poisonings. Journal of emergencies, trauma and shock, (2011); 4(3): 378.
- Memiş D, Tokatlıoglu D, Koyuncu O, Hekimoglu S. Fatal aluminium phosphide poisoning. European journal of anaesthesiology, (2007); 24(3): 292-293.
- Baruah U, Sahni A, Sachdeva HC. Successful management of aluminium phosphide poisoning using intravenous lipid emulsion: Report of two cases. Indian journal of critical care medicine: peer-reviewed, official publication of Indian Society of Critical Care Medicine, (2015); 19(12): 735.
- Moghadam Nia A, Firooz Jahi A, Javadian S, Dibavand N. Aluminium phosphide poisoning in mice and the procedure for its managements. Journal of Babol University of Medical Sciences, (2000); 2(4): 25-33.
- Abdolghaffari AH, Baghaei A, Solgi R, Gooshe M, Baeeri M, et al. Molecular and biochemical evidences on the protective effects of triiodothyronine against phosphine-induced cardiac and mitochondrial toxicity. Life sciences, (2015); 13930-39.
- Marashi SM, Majidi M, Sadeghian M, Jafarzadeh M, Mohammadi S, et al. Protective role of coenzyme Q10 as a means of alleviating the toxicity of aluminum phosphide: An evidence-based review. Tzu Chi Medical Journal, (2015); 27(1): 7-9.
- Manouchehri AA, Pirhadi M, Parsaei P, Alikord M, Safian Boldaji H. A review of aflatoxin M1 in milk and dairy products and new procedure for evaluating aflatoxin M1. J Chem Health Risks, (2021); 11(0): 0-0.
- Bahmani M. A new method for promoting biologic synthesis and reducing the size of titanium dioxide nanoparticles (Tio2 NPs) synthesized by Origanum vulgare. Plant Biotechnol Persa, 2019); 1 (1):10-12.)
- Pirhadi M, Shariatifar N, Bahmani M, Manouchehri AA. Heavy metals in wheat grain and its impact on human health: A review. J Chem Health Risks, (2021); 10.22034/jchr.2021.1924307.1269.
- Karimian M. Natural remedies for vascular diseases. Plant Biotechnol Persa, (2019); 1 (1):1-3.
- Manouchehri A, Shakib P, Biglaryan F, Nazer M, Darvishi M. The most important medicinal plants affecting bee stings: A systematic review study. Uludag Aricilik Dergisi, (2021); 21(1): 91-103.
- Zhang Y, Mahdavi B, Mohammadhosseini M, Rezaei-Seresht E, Paydarfard S, Qorbani M, Karimian M, Abbasi N, Ghaneialvar H, Karimi E. Green synthesis of NiO nanoparticles using Calendula officinalis extract: Chemical charactrization, antioxidant, cytotoxicity, and anti-esophageal carcinoma properties. Arabian Journal of Chemistry, (2021); 14(5):103-105.
- Ma D, Han T, Karimian M, Abbasi N, Ghaneialvar H, Zangeneh A. Immobilized Ag NPs on chitosan-biguanidine coated magnetic nanoparticles for synthesis of propargylamines and treatment of human lung cancer. International Journal of Biological Macromolecules, (2020); 165: 767-775.
- Abbaszadeh S, Andevari AN, Koohpayeh A, Naghdi N, Alizadeh M, Beyranvand F, Harsej Z. Folklore medicinal plants used in liver disease: A review. Int J Green Pharmacy, (2018); 12(3): 463-472.
- Solati K, Karimi M, Rafieian-Kopaei M, Abbasi N, Abbaszadeh S, Bahmani M. Phytotherapy for wound healing: The most important herbal plants in wound healing based on iranian ethnobotanical documents. Mini-Reviews in Medicinal Chemistry, (2021); 21(4): 500-519.
- Abbasi N, Khalighi Z, Eftekhari Z, Bahmani M. Extraction and phytoanalysis of chemical compounds of Eucalyptus globulus leaf native to Dehloran, Ilam province, Iran by HS-SPME and GC-MS. Advances in Animal and Veterinary Sciences, (2020); 8(6): 647-652.
- Aidy A, Karimi E, Ghaneialvar H, Mohammadpour S, Abbasi N. Protective effect of Nectaroscordum tripedale extract and its bioactive component tetramethylpyrazine against acetaminophen-induced hepatotoxicity in rats. Advances in Traditional Medicine, (2020); 20(3): 471-477.
- Abbaszadeh S, Rashidipour M, Khosravi P, Shahryarhesami S, Ashrafi B, Kaviani M, Sarabi MM.Biocompatibility, cytotoxicity, antimicrobial and epigenetic effects of novel chitosan-based quercetin nanohydrogel in human cancer cells. International Journal of Nanomedicine, (2020); 15: 5963-5975.
- Abbasi N, Khosravi A, Aidy A, Shafiei M. Biphasic response to luteolin in MG-63 osteoblast-like cells under high glucose-induced oxidative stress. Iranian Journal of Medical Sciences, (2016); 41(2): 118-125.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0