

Full Length Research Article
Isolation and characterization of Vancomycin resistant Staphylococcus aureus (VRSA) from Intensive Care Units (ICU) of different hospitals in Lahore, Pakistan
Sana Riaz1, Abid Hussain1,2, Muhammad Sohail1,2, Shafiq UR Rehman1, Numan Javed1, Zaigham Abbas1*
Adv. life sci., vol. 8, no. 3, pp. 339-344, December 2021
*– Corresponding Author: Zaigham Abbas (Email: zaigham.mmg@gmail.com)
Authors' Affiliations
2. Faculty of Rehabilitation & Allied Health Sciences, Riphah International University, QIE Campus Lahore – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Nosocomial infections present a major threat because of the increased prevalence of clinical cases appearing among both developed as well as developing countries thus resulting in an alarming condition. This descriptive study was designed to determine the prevalence of hospital acquired vancomycin resistant Staphylococcus aureus (VRSA) in intensive care units (ICU) of different hospitals of Lahore.
Methods: Sixty three swab samples were collected from different local hospitals in Lahore. The study was conducted at the Department of Microbiology and Molecular Genetics, University of the Punjab, Lahore from 2013 to 2014. Methicillin sensitive Staphylococcus aureus (MSSA), Methicillin resistant Staphylococcus aureus (MRSA) and VRSA were isolated and confirmed using Clinical & Laboratory Standard Institute (CLSI), 2015 guidelines. vanA gene was amplified to determine the molecular basis of resistance of all VRSA isolates by using strain of S. aureus (ATCC 29213) as a gold standard.
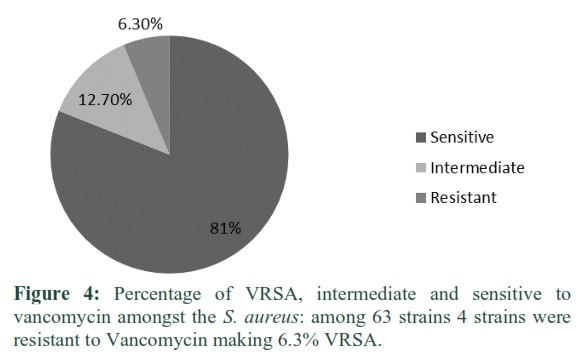
Results: Prevalence of VRSA is comparatively low in the hospital settings of Lahore than MRSA. Out of sixty three S. aureus, four (6%) isolates were VRSA positive, and eight isolates (17%) showed intermediate resistance. The absence of vanA gene in VRSA showed that mechanism of resistance is other than vanA gene transfer.
Conclusions: Presence of VRSA in hospital settings is alarming for health care workers, patients and researchers and it also highlights the importance of alternative medicines to cure infections.
Keywords: Vancomycin, Methicillin resistance, Staphylococcus aureus, Plasmids
Introduction![]()
Emergence of antibiotics resistance is the major public health concern. Methicillin resistant Staphylococcus aureus (MRSA) is considered as superbug that is responsible for community associated as well as nosocomial infections [1,2] and it is continuously causing different types of ailments worldwide [3]. MRSA is responsible for wide categories of infections that are ranging from minor skin infections to major disorders that can lead to death of the patient.
Coagulase negative Staphylococcus aureus (CoNS) and Staphylococcus aureus (S. aureus) both were sensitive to glycopeptides, except few reports of vancomycin resistant Staphylococcus aureus (VRSA), Vancomycin intermediate S. aureus (VRSA) and vancomycin resistant CoNS [4,5]. Frequent use of vancomycin for multiple infectious agents other than MRSA is the reason of emerging resistance for vancomycin. VRSA are resistant to most of the available antibiotics, limiting the options for therapy. Introduction of VRSA is alarming for medical community due to life threating infections caused by S. aureus in hospitalized and non-hospitalized patients [6,7].
VRSA strains have been found to have thicker cell walls than the sensitive strains [8]. Usually vancomycin is trapped in the outer layers and sequestered by the bacteria that results in resistance [9,10]. Exchange of genetic material between Enterococci and Staphylococci is well documented and consequence of this is VRSA [11]. It has been suggested that patients at risk for VRSA are co-infected or co-colonized with Vancomycin resistant Enterococci (VRE) and MRSA, which enables transfer of vanA gene from VRE to MRSA in a biofilm environment leading to a VRSA strain [12]. While inappropriate and suboptimal level of vancomycin is also the contributing factor for VRSA [13].
The vanH, vanA and vanX proteins play a significant role in the expression of vancomycin reduced susceptibility, while vanY has role in encoding of D,D-carboxypeptidase and the consequences are increased glycopeptides resistance. Another protein vanZ also mediates teicoplanin-like antibiotic resistance, while the mechanism of such resistance is unclear yet [14-16]. The vanA type expressed reduced vancomycin susceptibility which is intervened through an alternative mechanism producing cell wall antecedent terminus in D-Alanyl-D-lactate, indicating decreased glycopeptides attachment and downshifting of the cell wall production via housekeeping enzymes in the cell [14-16].
The aim of this study was to determine the prevalence of hospital acquired VRSA in intensive care units (ICU) of different hospitals of Lahore, to characterize VRSA on the basis of vanA gene and also to compare the epidemiology of MRSA and VRSA.
Methods![]()
A descriptive study was conducted at the Department of Microbiology and Molecular Genetics, University of the Punjab from 2013 to 2014 after approval from institutional ethical review committee. Swab samples were collected from various surfaces (cardiac monitors, ventilators, suction pump, door handles, floor, beds and side tables), personnel and patient skin or nares of ICU of different hospitals (Sheikh Zaid Hospital, Services Hospital, Ghurki Hospital and Lady Aitchison Hospital) in Lahore. All samples were inoculated on Blood, MacConkey and Chocolate agar plates. All plates were incubated at 37Cº for 24 hours. After incubation, the plates were examined for the growth and Gram’s staining was performed. Gram positive cocci in clusters were inoculated on blood agar for identification and purification [17].
Presumptive identification and confirmation of S. aureus and then MRSA was done following the CLSI guidelines [18]. Various biochemical tests including Catalase, Coagulase (slide and tube method) were performed for preliminary identification. Isolated colonies were inoculated on MSA (Mannitol Salt Agar) and DNase for confirmation [19]. MRSA was detected on the basis of resistance to oxacillin & cefoxitin by disc diffusion method [20]. The antimicrobial susceptibility was determined by the Kirby-Bauer disk diffusion method according to the guidelines recommended by CLSI. S. aureus (ATCC® 29213) was used as positive control during identification and antimicrobial sensitivity testing [18].
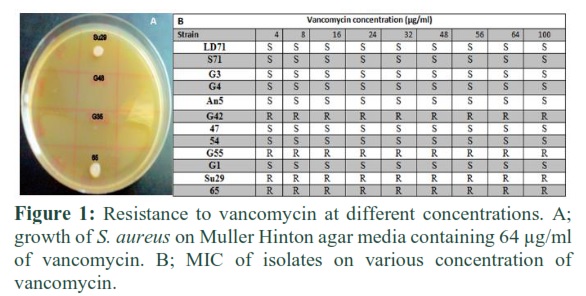
Agar plate dilution method was used for minimum inhibitory concentration (MIC) determination. Antibiotic was dissolved in solvent (distilled water) and added to molten Mueller Hinton agar. Mueller Hinton medium plates were prepared containing different concentration of vancomycin; 4µg/ml, 8µg/ml, 16µg/ml, 24µg/ml, 32µg/ml, 48µg/ml, 56µg/ml, 64µg/ml and 100µg/ml. Standard bacterial inoculum of 0.5 McFarland standard prepared in 0.9% NaCl was used [21].
Genomic DNA was isolated as described by Ausubel, et.al., with minor modifications [22]. Plasmid DNA was extracted and stored at -20°C [23]. Gel electrophoresis was performed to visualize the genomic and plasmid DNA [24]. PCR was performed to amplify vanA using following reported primers [25].
FP-vanA: 5’- ATGAATAGAATAAAAGTTGCAATAC-3’ (Forward Primer)
RP-vanA: 5’ –CCCCTTTAACGCTAATACGAT-3’ (Reverse Primer)
PCR amplification was performed in a 50µl reaction mixture containing genomic DNA (100ng), 25pmol vanA gene primer (10 µl), 10X PCR buffer (5µl), 25mM MgCl2 (3µl), 250mM dNTPs mixture (4µl) and 5 units of Taq DNA polymerase (0.5 µl) in a total volume of 50 µl. The amplification was programmed in the thermocycler (Bioer xp cycler) as follow: preheating for 1 minute at 95Co (initial denaturation), 35 cycles each for 20 seconds at 95Co (denaturation), 25 seconds at 55 Co and 20 seconds at 72Co (extension) and a final extension at 72Co for 2 minutes. The resulting PCR products were run on 1% agarose gels, stained with ethidium bromide and visualized on UV illuminator [26].
Results![]()
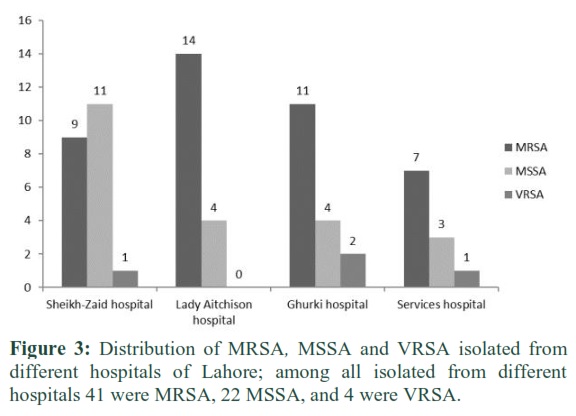
S. aureus strains were isolated from ICUs of different, public as well as private hospitals (Sheikh-Zaid hospital, Lady Aitchison, Ghurki trust teaching hospital and Services hospital) of Lahore. These strains were isolated from non-living surfaces such as; cardiac monitors, ventilators, suction pump, door handles, floor, beds and side tables as well as living surfaces such as; patient skin and nares, personnel skin and nares. By using CLSI guidelines for the identification and confirmation of bacterial resistance, sixty three (63) strains of S. aureus were isolated, among these forty one (41) on the basis of Cefoxitin (30µg); zone of inhibition ≤ 24 mm confirmed MRSA among these four (04) strains were further confirmed as VRSA rest of the strains twenty two (22) were MSSA.
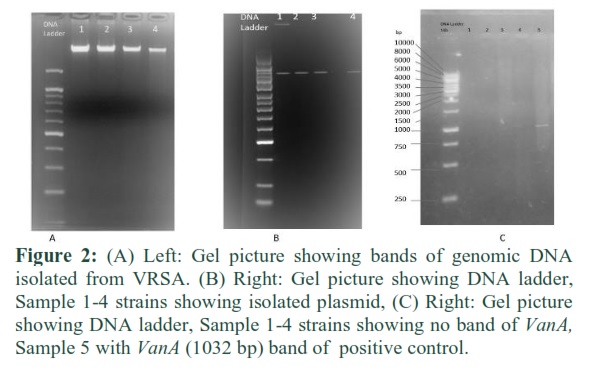
Antibiotic susceptibility test was performed using CLSI guidelines; results showed 41 strains Cefoxitin resistant, which confirmed MRSA and remaining were MSSA. Except 12 isolates, all were vancomycin sensitive. Four (04) were vancomycin resistant and eight (08) showed intermediate level of resistance. MIC was determined by using agar dilution method and it confirmed the results of agar diffusion test as 08 isolates showed intermediate level of resistance and 4 were vancomycin resistant and their MICs were > 100µg/ml. MRSA are more prevalent than VRSA in health care settings. MIC of Staphylococcus sp. strains against vancomycin was determined by agar dilution method by following CLSI guidelines (Figure 1). Out of 12 strains, 4 (33.33 %) were having MICs <100ug/ml. The MIC of vancomycin <4µg/mL is susceptible, 8-16µg/mL is intermediate and MIC > 32µg/mL are resistant Staphylococcus sp.[27]. Genomic and plasmid DNA of VRSA was extracted and processed for the amplification of vanA gene. There was no amplification of vanA gene in the four strains of VRSA shown in figure 2 (A,B&C).
Figures & Tables
Discussion![]()
Prevalence of Methicillin resistant S. aureus isolates collected from various hospitals in Lahore and the prevalence of VRSA is described in Figure 3. As the present study revealed an increased prevalence of methicillin resistant S.aureus, the vancomycin was recommended as drug of choice to treat MRSA. Therefore vancomycin intermediate S. aureus and vancomycin resistant S. aureus strains were developed. MSSA is most frequently isolated from Sheikh Zayed Hospital, MRSA from Lady Aitchison Hospital and VRSA from Ghurki Hospital Lahore. No VRSA was isolated from Lady Aitchison hospital as shown in Figure 3. Most of pathogens isolated in this study were sensitive to vancomycin (81%) and only 6.30 % were resistant to vancomycin as shown in Figure 4. The occurrence of multidrug resistant MRSA has been increased because of insufficient information about drugs in the community, lack of awareness, low economic status, increased availability of antibiotics and improper dose of antimicrobials, anti-microbial prophylaxis, high number of individuals with weak immune system, the common utilization of obtrusive techniques, devices and lacking of contamination control measures [28,29].
Development of vancomycin tolerance has become a serious issue in health care settings to treat multidrug resistant S. aureus and MRSA [30]. The present study revealed Staphylococci in different locations inside the ICUs of health care settings. Masaki also demonstrated [31] comparable results to our study, who isolated 19 clinical MRSA strains from the clinical floor. In an alternate study, Brady isolated 25 MRSA strains from hospital cots, showing the existence of this microbe on distinctive locations [32]. Another study was conducted which reported that health care experts again contaminate their hands throughout interferences of patient treatment by touching things, for example, a computer mouse, caution catches and pens before administering the patients [33]. Many microbes can also be transferred via nonliving things like soap dispensers, tables, telephones, sphygmomanometers, monitors and bedside bars [34].
We suppose the probability of vancomycin tolerance vanA gene transfer from vancomycin resistant Enterococci spp. to Staphylococci spp. according to in vitro exchange of vanA gene from Enterococcus spp. to S. aureus [35]. In fact the vanA, vanR, vanS, vanH and vanX genes are quite important for the VanA phenotype to be expressed, reported in past studies [36]. VRSA isolates additionally have been discovered to have thicker cell wall compared to sensitive ones [37]. In the case of hetero vancomycin intermediate S. aureus, they also show thickened cell wall resistance mechanism having high cell wall murein content. It is demonstrated that vancomycin molecules are trapped in the external layers and are sequestered by the bacteria that result in resistance [38].
Another resistance mechanism proposed for VRSA is transfer of hereditary material from one bacterial spp. to another. It was proposed that individuals with high risk for VRSA have co-infection and co-colonization of VRE and VRSA, which helps in transfer of vanA gene from vancomycin resistant Enterococci to MRSA in a biofilm environment developing it into VRSA [39].
Only a few reports are present regarding detection of VRSA – in health care settings all over the world and some of these VRSA strains are community associated [35]. In the present study vanA gene of VRSA was amplified but no amplification of vanA gene indicated absence of gene in these isolates. It confirms the presence of other mechanism of resistance independent of vanA gene, which needs further investigations. Expectancy of development and prevalence of VRSA in all groups is very crucial to be considered. Suitable contamination control measures, appropriated antimicrobial management, hygienic settings and awareness in individuals can help to control the rise and transmission of antimicrobial tolerant microorganisms such as VRSA. There ought to be a consistently checking of the reduced susceptibility example of the multi-drug resistant S. aureus. There is great need to take measures to control VRSA infection; otherwise it can play havoc in hospital settings as well as in community at large.
Author Contributions
Sana Riaz performed experimentation, Abid Hussain performed data analysis and manuscript preparation, Muhammad Sohail helped in sample collection and experimentation, Shafiq UR Rehman Supervision and manuscript revision, Numan Javed Supervision and manuscript revision, Zaigham Abbas Supervision Data analysis and manuscript revision.
Acknowledgement
University of the Punjab, Lahore is highly acknowledged for providing financial support during the study.
None.
References![]()
- McMaster J, Booth MG, Smith A, Hamilton K. Meticillin-resistant Staphylococcus aureus in the intensive care unit: its effect on outcome and risk factors for acquisition. Journal of Hospital Infection, (2015); 90(4): 327-332.
- Khokhlova OE, Hung WC, Wan TW, Iwao Y, Takano T, et al. Healthcare- and Community-Associated Methicillin-Resistant Staphylococcus aureus (MRSA) and Fatal Pneumonia with Pediatric Deaths in Krasnoyarsk, Siberian Russia: Unique MRSA's Multiple Virulence Factors, Genome, and Stepwise Evolution. Plos One, (2015); 10(6).
- Rivera AM, Boucher HW. Current concepts in antimicrobial therapy against select gram-positive organisms: methicillin-resistant Staphylococcus aureus, penicillin-resistant Pneumococci, and vancomycin-resistant Enterococci; 2011. Elsevier. pp. 1230-1243.
- Srinivasan A, Dick JD, Perl TM. Vancomycin resistance in Staphylococci. Clinical microbiology reviews, (2002); 15(3): 430-438.
- Tenover FC. Vancomycin-resistant Staphylococcus aureus: a perfect but geographically limited storm? Clinical Infectious Diseases, (2008); 46(5): 675-677.
- Denys GA, Relich RF. Antibiotic Resistance in Nosocomial Respiratory Infections. Clinics in Laboratory Medicine, (2014); 34(2): 257-270.
- Limbago BM, Kallen AJ, Zhu W, Eggers P, McDougal LK, et al. Report of the 13th vancomycin-resistant Staphylococcus aureus isolate from the United States. Journal of clinical microbiology, (2014); 52(3): 998-1002.
- Daum RS, Gupta S, Sabbagh R, Milewski WM. Characterization of Staphylococcus aureus isolates with decreased susceptibility to vancomycin and teicoplanin: isolation and purification of a constitutively produced protein associated with decreased susceptibility. The Journal of Infectious Diseases, (1992); 166(5): 1066-1072.
- Cui L, Murakami H, Kuwahara-Arai K, Hanaki H, Hiramatsu K. Contribution of a thickened cell wall and its glutamine nonamidated component to the vancomycin resistance expressed by Staphylococcus aureus Mu50. Antimicrobial Agents and Chemotherapy, (2000); 44(9): 2276-2285.
- Billot-Klein D, Gutmann L, Bryant D, Bell D, Van Heijenoort J, et al. Peptidoglycan synthesis and structure in Staphylococcus haemolyticus expressing increasing levels of resistance to glycopeptide antibiotics. Journal of Bacteriology, (1996); 178(15): 4696-4703.
- Clewell DB, Francia MV, Flannagan SE, An FY. Enterococcal plasmid transfer: sex pheromones, transfer origins, relaxases, and the Staphylococcus aureus issue. Plasmid, (2002); 48(3): 193-201.
- Finks J, Wells E, Dyke TL, Husain N, Plizga L, et al. Vancomycin-resistant Staphylococcus aureus, Michigan, USA, 2007. Emerging Infectious Diseases, (2009); 15(6): 943-945.
- De Vriese AS, Vandecasteele SJ. Vancomycin: the tale of the vanquisher and the pyrrhic victory. Peritoneal Dialysis International, (2014); 34(2): 154-161.
- Lee WG, Huh JY, Cho SR, Lim YA. Reduction in glycopeptide resistance in vancomycin-resistant Enterococci as a result of vanA cluster rearrangements. Antimicrobial Agents and Chemotherapy, (2004); 48(4): 1379-1381.
- Depardieu F, Podglajen I, Leclercq R, Collatz E, Courvalin P. Modes and modulations of antibiotic resistance gene expression. Clinical Microbiology Reviews, (2007); 20(1): 79-114.
- Arthur M, Quintiliani R, Jr. Regulation of VanA– and VanB-type glycopeptide resistance in Enterococci. Antimicrobial Agents and Chemotherapy, (2001); 45(2): 375-381.
- Cappuccino JG, Sherman N. Basic Laboratory Techniques for Isolation, Cultivation, and Cultural Characterization of Microorganisms. Microbiology: A Laboratory Manual, (2013); 11: 1-560 Pearson Education Limited, United Kingdom.
- Institute CaLS (2015) CLSI 2015: Antimicrobial Susceptibility Testing. USA: Wayne, Pennsylvania.
- Gemmell CG, Edwards DI, Fraise AP, Gould FK, Ridgway GL, et al. Guidelines for the prophylaxis and treatment of methicillin-resistant Staphylococcus aureus (MRSA) infections in the UK. Journal of Antimicrobial Chemotherapy, (2006); 57(4): 589-608.
- Fernandes CJ, Fernandes LA, Collignon P. Cefoxitin resistance as a surrogate marker for the detection of methicillin-resistant Staphylococcus aureus. Journal of Antimicrobial Chemotherapy, (2005); 55(4): 506-510.
- Soriano A, Marco F, Martínez JA, Pisos E, Almela M, et al. Influence of Vancomycin Minimum Inhibitory Concentration on the Treatment of Methicillin-Resistant Staphylococcus aureus Bacteremia. Clinical Infectious Diseases, (2008); 46(2): 193-200.
- Ausubel F, Brent R. Kingston, RE, Moore, DD, Seidman, JG, Smith, JA and Struhl, K.(eds) 1987. Current Protocols in Molecular Biology, (1987); 18.5.
- Bimboim H, Doly J. A rapid alkaline extraction procedure for screening recombinant plasmid DNA. Nucleic Acids Research, (1979); 7(6): 1513-1523.
- Green MR, Hughes H, Sambrook J, MacCallum P. "Molecular cloning: a laboratory manual." Molecular Cloning: a Laboratory Manual. (2012). 1890-1890. CSHL Press, United States.
- Miele A, Bandera M, Goldstein BP. Use of primers selective for vancomycin resistance genes to determine van genotype in Enterococci and to study gene organization in VanA isolates. Antimicrobial Agents and Chemotherapy, (1995); 39(8): 1772-1778.
- Miele A, Bandera M, Goldstein BP. Use of primers selective for vancomycin resistance genes to determine van genotype in enterococci and to study gene organization in VanA isolates. Antimicrobial Agents and Chemotherapy, (1995); 39(8): 1772-1778.
- Tenover FC, Biddle JW, Lancaster MV. Increasing resistance to vancomycin and other glycopeptides in Staphylococcus aureus. Emerging infectious diseases, (2001); 7(2): 327.
- Carbon C. MRSA and MRSE: is there an answer? Clinical Microbiology and Infection, (2000); 617-22.
- Onanuga A, Temedie TC. Multidrug-resistant intestinal Staphylococcus aureus among self-medicated healthy adults in Amassoma, South-South, Nigeria. Journal of Health, Population, and Nutrition, (2011); 29(5): 446.
- Tiwari HK, Sen MR. Emergence of vancomycin resistant Staphylococcus aureus (VRSA) from a tertiary care hospital from northern part of India. BMC Infectious Diseases, (2006); 6(1): 156.
- Maki H, McCallum N, Bischoff M, Wada A, Berger-Bächi B. tcaA inactivation increases glycopeptide resistance in Staphylococcus aureus. Antimicrobial Agents and Chemotherapy, (2004); 48(6): 1953-1959.
- Brady RA, Leid JG, Kofonow J, Costerton JW, Shirtliff ME. Immunoglobulins to surface-associated biofilm immunogens provide a novel means of visualization of methicillin-resistant Staphylococcus aureus biofilms. Applied and Environmental Microbiology, (2007); 73(20): 6612-6619.
- Lam MW, Young CJ, Brain RA, Johnson DJ, Hanson MA, et al. Aquatic persistence of eight pharmaceuticals in a microcosm study. Environmental Toxicology and Chemistry, (2004); 23(6): 1431-1440.
- Karabey S, Ay P, Derbentli S, Nakipoglu Y, Esen F. Handwashing frequencies in an intensive care unit. Journal of Hospital Infection, (2002); 50(1): 36-41.
- Whitener CJ, Park SY, Browne FA, Parent LJ, Julian K, et al. Vancomycin-resistant Staphylococcus aureus in the absence of vancomycin exposure. Clinical Infectious Diseases, (2004); 38(8): 1049-1055.
- Woodford N, Adebiyi A-MA, Palepou M-FI, Cookson BD. Diversity of VanA glycopeptide resistance elements in Enterococci from humans and nonhuman sources. Antimicrobial Agents and Chemotherapy, (1998); 42(3): 502-508.
- Daum RS, Gupta S, Sabbagh R, Milewski WM. Characterization of Staphylococcus aureus isolates with decreased susceptibility to vancomycin and teicoplanin: isolation and purification of a constitutively produced protein associated with decreased susceptibility. Journal of Infectious Diseases, (1992); 166(5): 1066-1072.
- Billot-Klein D, Gutmann L, Bryant D, Bell D, Van Heijenoort J, et al. Peptidoglycan synthesis and structure in Staphylococcus haemolyticus expressing increasing levels of resistance to glycopeptide antibiotics. Journal of Bacteriology, (1996); 178(15): 4696-4703.
- Finks J, Wells E, Dyke TL, Husain N, Plizga L, et al. Vancomycin-resistant Staphylococcus aureus, Michigan, USA, 2007. Emerging Infectious Diseases, (2009); 15(6): 943-945.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0