

Full Length Research Article
Diagnostic accuracy of chest computed tomography for detecting COVID-19 pneumonia in low disease prevalence area: A local experience
Mounir Benmessaoud*, Ahmed Dadouch, Maghnouj Abdelmajid, Anass Abir, Youssef el-Ouardi, Assiya Lemmassi, Khalid Nouader, Inssaf Chibani
Adv. life sci., vol. 8, no. 4, pp. 355-359, December 2021
*– Corresponding Author: Mounir Benmessaoud (Email: mounir.benmessaoud@usmba.ac.ma )
Authors' Affiliations
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The role of computed tomography (CT) was crucial in detecting coronavirus disease 2019, their diagnostic performances were evaluated frequently in the high disease prevalence regions. In contrast, limited studies assessed the accuracy of chest CT in low disease prevalence areas.
Methods: A retrospective study was conducted at a single center from April 3 to October 16, 2020. The data were collected manually involving age, gender, symptoms, chest CT and RT-PCR results. Patients included were all suspected cases diagnosed by both chest CT and RT-PCR. The confidence intervals (95%) were estimated using the Wilson method.
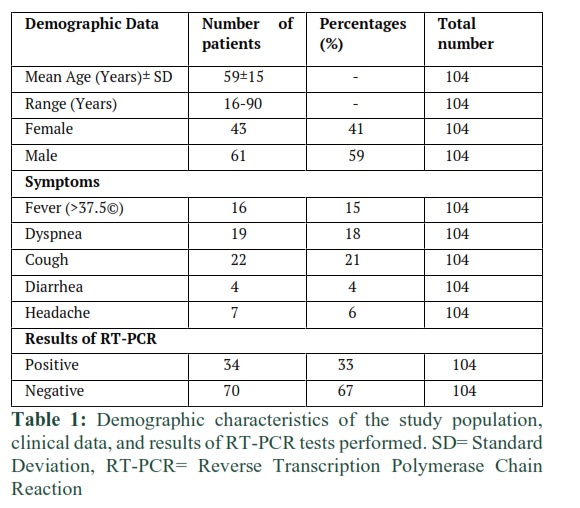
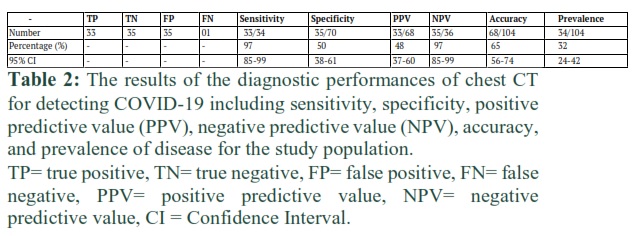
Results: A total of 104 patients (mean age 59±15 years, 61 males) were included. 6/104(15%) were presented with fever, 22/104(21%) with cough, 19/104(18%) with dyspnea, 4/104(4%) with diarrhea, and 7/104(6%) with headache. Regarding reverse transcription-polymerase chain reaction (RT-PCR) tests, 34 cases were positive and 70 were negatives. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy of chest CT using RT-PCR as a reference were 97% (33/34,95%CI; [85-99%]), 50% (35/70,95%CI; [38-61%]), 48% (33/68,95%CI; [37-60%]), 97% (35/36,95%CI; [85-99%]) and 65% (68/104,95%CI; [56-74%]), respectively.
Conclusion: Chest CT is an important tool that contributed to the treatment decision of the high-suspected cases, as an early intervention before the confirmation with RT-PCR.
Keywords: COVID-19; Chest Computed Tomography; Diagnostic Accuracy
Introduction![]()
The first outbreak of the novel coronavirus was in Wuhan, China in December 2019 [1], its spread was very fast and widely extended across different countries in the world. For the African nations especially in Morocco, the first confirmed case of COVID-19 was declared on 2 March 2020 by the health authorities [2]. Nowadays, more than 474 966 confirmed cases were reported in Morocco (February 06, 2021) [3]. Further, during the period ranging from March 2, 2021, to May 28, 2021, the total COVID-19 related deaths were 202 cases and a mortality rate of 2.6% [4].
The diagnosis of COVID-19 infection is based on reverse transcription-polymerase chain reaction (RT-PCR) as a reference standard according to the international recommendations [5]. Therefore, three Moroccan centers were considered at the beginning of the epidemic as the national referral institutions, which were charged to perform the RT-PCR assays in the whole country. However, the big challenge was the prior detecting of the COVID-19 infection, to control the widespread of the virus among Moroccan regions. Thus, the number of laboratories was increased progressively from 3 to more than 24 over 4 months period including public and private centers.
Following the first protocol of diagnosis and treatment of the novel virus declared by the Moroccan health ministry, the chest X-ray was recommended to be performed systematically for each patient suspected of COVID-19 [6]. This procedure was considered to detect chest abnormalities that may be caused by the virus infection and to eliminate the other pulmonary diseases that could affect the health of patients. Thus, identify at an early stage any factor of comorbidity.
The period of process testing with the RT-PCR method was ranging from 2 days to 4 days, including the collection of several swabs samples for each day, transportation, and the analyzing time in the referral laboratories. This long process of detecting requires another intervention as computed tomography (CT) technique, which was necessary to confirm primarily the positivity or negativity of the high suspected patients.
On one hand, the role of chest CT was crucial in diagnosing the COVID-19 as a complementary tool of the RT-PCR technique [7, 8]. The sensitivity, specificity, and accuracy of chest CT were estimated in China by Tao et al, which were 97%, 25% and 68%, respectively [8]. On the other hand, another investigation concluded that in low prevalence disease regions (<10%), there is no benefit of using CT as a tool for detecting the COVID-19 [9]. The debate about the diagnostic performance of chest CT remains an open and uncompleted issue, especially with the significant differences reported in study’s findings, and the lack of reports investigated from the low prevalence countries. Therefore, the purpose of the present study was to assess the diagnostic accuracy of chest CT for detecting COVID-19 pneumonia using the RT-PCR findings as a reference and taking into consideration the low disease prevalence in Morocco.
Methods![]()
Clinical data and design study
This retrospective study was conducted at a single center from April 3 to October 16, 2020, excluding June and July months. The data were collected manually involving age, gender, symptoms, chest CT acquisition parameters, chest CT and RT-PCR results. The patients included were all suspected patients diagnosed by both chest CT and RT-PCR during the period mentioned above. While we excluded patients who were tested only by RT-PCR.
The administration permission for data collection was obtained and the informed consent of participating patients was waived due to the retrospective anonymized data collection.
CT acquisition parameters
The patients admitted in this center were scanned by using Hitachi model scanner 16-slice and the chest CT was performed without venous contrast and with the following scans parameters: tube voltage: 120kV, scan time: 0.75s, slice thickness: 3.75mm, collimation: 1.25 x 16, table pitch: 1.0625 and field of view: 350mm x 350mm.
CT image analysis
The analysis of chest CT images was performed by two radiologists with experience of more than 8 years in CT.
Statistical analysis
The statistical analysis of data was performed using SPSS Software (Version 20.0). The descriptive statistics were used to determine means, standard deviation, and ranges. The confidence intervals (95%) were estimated using the Wilson method.
The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of chest CT screening were estimated by using the formulas (1), (2), (3), (4), and (5), respectively. While the disease prevalence in the included population was evaluated by the formula (6) [10, 11].
Sensitivity = True Positive / (True Positive + False Negative) (1)
Specificity = True Negative / (True Negative + False Positive) (2)
PPV= (Sensitivity ×Prevalence) / (Sensitivity × Prevalence) +[(1 – Specificity)×(1- Prevalence)] (3)
NPV= Specificity× (1- Prevalence) / Specificity× (1- Prevalence) +[(1 – Sensitivity)× Prevalence] (4)
Accuracy = (True Positive + True Negative) / Total population (5)
Prevalence= (True Positive + False Negative) / Total population (6)
Results
![]()
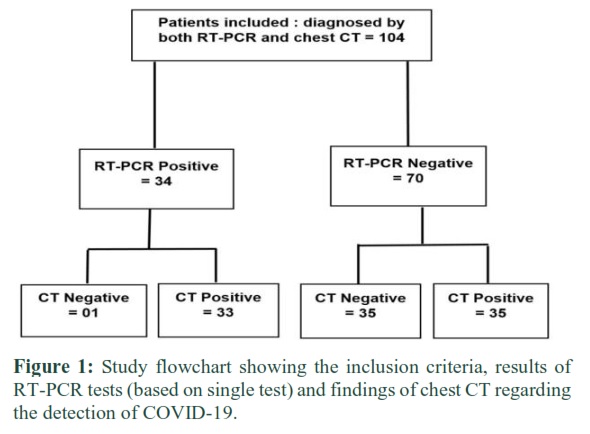
A total of 104 patients were included in this study, 36% (38/104) of whom were presented with different symptoms as follows: 16/104 (15%) fever, 22/104 (21%) cough, 19/104 (18%) dyspnea, 4/104 (4%) diarrhea, 7/104 (6%) headache, and the data of 64% (66/104) were unavailable. The mean age of the sample was 59± 15 years, ranging between 16 years and 90 years. While 41% (43/104) of the patients included were females and 59% (61/104) were males. Clinical and demographic data were reported in table 1 and the flowchart of the present study is summarized in figure 1.
Of the total sample included, 34 cases were positive, and 70 cases were negatives regarding the RT-PCR assays. Thus, the true and false values of chest CT were provided as follows: 33 true positive, 35 true negatives, 35 false positive, and 1 case with a false negative CT. Otherwise, of 68 cases with positive CT findings, 43 (63%) were recorded with the proportions of lungs affected. The repartitions were as follows: 16% (7/43) with <25%, 32% (14/43) with 25-50%, 37% (16/43) with 50-75%, and 14% (6/43) with >75% of lungs affected.
The performance estimation of chest CT in detecting COVID-19 was based on the sensitivity, specificity, PPV, NPV, and accuracy indicators, which were assessed by considering the RT-PCR as a reference standard or the gold standard at present in diagnosing COVID-19 pneumonia. The sensitivity, specificity, and accuracy of chest CT estimated were 97% (95%CI, [85-99%]), 50% (95%CI,[38-61%]) and 65% (95%CI,[56-74%]), respectively as shown in table 2.
The PPV and NPV were evaluated with caution and took into consideration the disease prevalence of our study population by using Bayes’ theorem. The PPV, NPV and prevalence were 48% (95%CI, [37-60%]), 97% (95%CI, [85-99%]) and 32% (95%CI, [24-42%]), respectively (Table 2).
Figures & Tables
Discussion![]()
The diagnostic performances of chest CT in differentiating COVID-19 pneumonia have been reported by several studies, which were almost documented from the high prevalence disease countries or regions, such as China, Italy, and France [8, 12, 13]. By contrast, a few reports were published from non-high-epidemic area in terms of disease prevalence [14]. The results of a meta-analysis study published by KIM et al [9], were our first inspiration source to investigate more about the diagnostic performance in low prevalence region as Morocco. Therefore, the purpose of the present study was to assess the diagnostic performance of chest CT in diagnosing COVID-19 using the RT-PCR findings as a reference and taking into account the low disease prevalence in Morocco.
The sensitivity, specificity, PPV, and NPV are applicable only for the population from which they are estimated. The sensitivity and specificity are the intrinsic characteristics of a diagnostic test and they are independents of disease prevalence. In contrast, the PPV and NPV are very influenced by the disease prevalence level of the population studied [10]. Thus, in two different sites with different disease prevalence, the predictive values of CT in diagnosing COVID-19 will be different by site [10]. It is important to note that the patients included in the present study were scanned at the initial presentation as an emergency examination. Furthermore, the suspected patients who were discharged from the hospital with a negative RT-PCR were controlled at home during 14 days period to exclude complications or development of other symptoms of COVID-19 infection. The sensitivity of chest CT at the initial presentation was investigated by Fang et al, They reported that the sensitivity of chest CT in diagnosing COVID-19 at initial patients’ presentation was higher than that of RT-PCR(98% vs 71%, p< 0.001) [15]. On one side, the use of RT-PCR as a reference to estimate the performance of chest CT is a universal approach considered by several studies. However, the number of RT-PCR tests used as the final reference remains an important source of differences between studies and may affect the accuracy of RT-PCR results. In our study, the sample collection for RT-PCR testing was based on the nasopharyngeal swabs uniquely without using any other swabs such as throat or sputum swabs. Thus, the presence of COVID-19 infection in the suspected swabs was confirmed or ignored by a single test of RT-PCR. In contrast, the other countries performed two(or more than 2) virological tests consecutive to declare the positivity or negativity of swabs tested. Therefore, the accuracy of RT-PCR tests may affect the assessment of the diagnostic performance of chest CT in the detection of COVID-19 pneumonia. On the other side, the time of testing the cases is an important factor that can affect the results of RT-PCR. Yu et al reported that after 5-6 days of onset, COVID-19 infection is detected with high probability in nasopharyngeal swabs [16]. So, if we tested the patients by two tests consecutive (or more) separated in time, we increase the probability of detecting the infection, then decrease the false negative results of RT-PCR. As reported by Ducray et al, the false negatives tests of RT-PCR decrease the PPV of chest CT [17]. That may explain the low PPV (48%) of chest CT obtained in our investigation, especially we used a single test of RT-PCR as a reference. The majority (70) of patients included in this study were recorded in August, September, and October months, they were presented with severe illness and symptoms. Of 68 cases with positive chest CT, 43 cases were collected with the proportions of lungs affected, the first group involved 22 cases with >50% of lungs affected, 16 were true positive CT and 6 false positive CT using RT-PCR results as the standard reference. For the second group, 21 cases with <50% of lungs affected including 13 false positive CT and 8 true positive CT using RT-PCR findings. In this context, Ducray et al concluded that for patients with severe illness, there is a low probability of having false negatives CT, which increases the values of NPV estimated in the sample [17]. The higher value of NPV (97%) documented in this study may be due to the reason mentioned above. Besides, it is known that the predictive values of a diagnostic test are influenced by the disease prevalence in the population tested. In Other Words, the low prevalence disease decreases the PPV and increases the NPV [18]. Thus, the low PPV (48%) and high NPV (97%) estimated in our population study were highly impacted by the low prevalence of disease assessed (32%). At present, the COVID-19 infection increases to evolve many peoples in Morocco. Thus, the request for RT-PCR analysis will be increased dramatically. Therefore, the use of CT as a diagnostic tool of COVID-19 is necessary for the suspected cases and for the confirmed positive patients under treatment to control their evolution. The limitations of the present study were the following: First, the pre-objective of this study was to conduct a multi-center investigation but the access to other centers was limited and not authorized. Second, the presence or absence of COVID-19 infection was confirmed by a single test of RT-PCR which was used as a reference. In contrast, it is recommended to perform more than two tests to assure the accuracy of RT-PCR. Third, the number of cases included was limited due to that the chest CT scan was undergone only for the high suspected patients. Fourth, the procedure of administration permission for data collection was complicated and time–consuming. Fifth, the data archiving in the center was based on handwriting papers due to that the electronic archiving system is not available. The chest CT was required for the high suspected and complicated patients who were admitted with severe illness and with abnormalities in chest X-ray images. Thus, the chest CT was an important tool that contributed to the treatment decision of the high suspected cases, as an early intervention before the confirmation with RT-PCR results. Otherwise, the findings of the present study shed light on the efficacy of chest CT in diagnosing COVID-19 pneumonia in the low prevalence area in Morocco.
Author Contributions
Study concepts and design: Dadouch Ahmed, Maghnouj Abdelmajid, Benmessaoud Mounir
Literature research: Benmessaoud Mounir , El-ouardi Youssef
Data collection: Benmessaoud Mounir , Abir Anass, Nouader Khalid, Chibani Inssaf
Analysis and/or interpretation of data: Dadouch Ahmed, Benmessaoud Mounir, Abir Anass
Statistical analysis: Benmessaoud Mounir, Lemmassi Assiya
Drafting the manuscript: Benmessaoud Mounir, Lemmassi Assiya
We have read and understood ALS policy on declaration of interests and declare that we have no competing interests.
References![]()
- Huang C, Wang Y, Li X, Ren L, Zhao J, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet, (2020); 395(10223): 497–506.
- Moroccan health ministry Web site. http://www.covidmaroc.ma/Documents/COM/.Accessed April 30, 2020.
- Moroccan health ministry Web site. http://www.covidmaroc.ma/Documents/BULLETIN/. Accessed February 06, 2021.
- Cherradi Y. About the Moroccan strategy in the fight against Covid-19 before lockdown ease period. Journal of Medical and Surgical Research, (2020); 737:40.
- Interim Guidance: Healthcare Professionals 2019-nCoV | CDC; (2020).
- Moroccan health ministry Web site. http://www.covidmaroc.ma/Documents/2020/coronavirus/PS/covid-19. Accessed May,04 2020.
- Li Y, Xia L. Coronavirus disease 2019 (COVID-19): Role of chest CT in diagnosis and management. American Journal of Roentgenology, (2020); 214(6): 1280–1286.
- Ai T, Yang Z, Hou H, Zhan C, Chen C, Lv W, Tao Q, Sun Z, Xia L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology, (2020); 296(2): E32–E40.
- Kim H, Hong H, Ho Yoon S. Diagnostic performance of ct and reverse transcriptase polymerase chain reaction for coronavirus disease 2019: A meta-analysis. Radiology, (2020); 296(3): E145–E155.
- Eng J, Bluemke D A. Imaging publications in the COVID-19 pandemic: Applying new research results to clinical practice. Radiology, (2020); 297(1): E228–E231.
- Alberg A J, Park J W, Hager B W, Brock M V, Diener-West M. The use of “overall accuracy” to evaluate the validity of screening or diagnostic tests. Journal of General Internal Medicine, (2004); 19(5 PART 1): 460–465.
- Falaschi Z, Danna P S C, Arioli R, Pasché A, Zagaria D, et al. Chest CT accuracy in diagnosing COVID-19 during the peak of the Italian epidemic: A retrospective correlation with RT-PCR testing and analysis of discordant cases. European Journal of Radiology, (2020); 130(July): 109192.
- Herpest G, Lederlin M, Naudin M, Ohana M, Chaumoitre K, et al. Efficacy of Chest CT for COVID-19 Pneumonia Diagnosis in France. Radiology, (2021); 298(2): E81–E87.
- Himoto Y, Sakata A, Kirita M, Hiroi T, Kobayashi K, et al. Diagnostic performance of chest CT to differentiate COVID-19 pneumonia in non-high-epidemic area in Japan. Japanese Journal of Radiology, (2020); 38(5): 400–406.
- Fang Y, Zhang H, Xie J, Lin M, Ying L,Pang P, Ji W. Senivity of Chest CT for COVID.19: Comparasion to RT-PCR. Radiology, (2020); 296: 15–17.
- Yu F, Yan L, Wang N, Yang S, Wang L, et al. Quantitative detection and viral load analysis of SARS-CoV-2 in infected patients. Clinical Infectious Diseases, (2020); 71(15): 793–798.
- Ducray V, Vlachomitrou A S, Bouscambert-Duchamp M, Si-Mohamed S, Gouttard S, et al. Chest CT for rapid triage of patients in multiple emergency departments during COVID-19 epidemic: experience report from a large French university hospital. European Radiology, (2020);31(2): 795–803.
- Ranganathan P, Aggarwal R. Common pitfalls in statistical analysis: Understanding the properties of diagnostic tests – Part 1. Perspectives in Clinical Research, (2018); 9(1) : 40–43.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0