

Full Length Research Article
Molecular genetic analysis of the m.A3243G mutation of the tRNALeu (UUR) gene in a population of Moroccan deaf diabetics
Taha Rhouda1☽, Fatima Zahra Kehailou1*☽, Fatima Zahra EL Mskini1, Ali Labriji2, Mohammed Jabari3, Houriya Mestaghanmi1
Adv. life sci., vol. 9, no. 1, pp. 111-115, May 2022
* – Corresponding Author: Fatima Zahra Kehailou (Email: fati.kehailou@gmail.com)
☽ – These authors contributed equally to this work.
Authors' Affiliations
2. Modelling, Analysis and Simulation Laboratory. Department of Mathematics and Computer Science. Faculty of Sciences Ben M’Sik. Casablanca – Morocco
3. Division of Hygiene, Prevention and Environment, Wilaya of de la Region of Casablanca-Settat, Ministry of the Interior, Casablanca – Morocco
Editorial Note on Version of Record
24 June 2025: This article has been corrected. See https://doi.org/10.62940/als.v13i0.4242 for more information.
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The mitochondrial DNA (mtDNA) m.A3243G mutation of the tRNALeu (UUR) gene presents clinically heterogeneous phenotypes and is often responsible for diabetes, with or without deafness syndrome. The aim of this study was to search for this pathogenic mutation in 3 diabetics with bilateral deafness and a family history of diabetes.
Methods: mtDNA was extracted from the patients’ whole blood. After PCR amplification, the DNA was sequenced and analyzed.
Results: The sequencing results showed the absence of the most common mtDNA mutation m.A3243G in diabetic families with individuals who suffer from hearing loss.
Conclusions: The m.A3243G mutation in the mitochondrial tRNALeu (UUR) Leu gene was not found to be a common cause of type 2 diabetes and deafness. These results suggest that there may be genetic causes for this phenotype.
Keywords: Diabetes; Deafness; M.A3243G Mutation; Mitochondrial DNA
Introduction![]()
Diabetes mellitus is a multifaceted disease that affects a huge extent of the global population. It is associated with environmental and/or genetic risk factors, caused by mutations in the nuclear DNA (nDNA) [1] as well as in genes of the mitochondrial genome (mDNA) [2].
According to several studies, genetic determinism in diabetes mellitus is very important, as it is estimated that the risk of developing the disease is 30% with one parent with type 2 diabetes and 70% if both parents are affected. The most common mitochondrial mutation m.A3243G is associated with maternally inherited diabetes and deafness (MIDD) [3,4]. The m.A3243G mutation is located at the Leu transfer RNA (UUR) gene [5] and expresses variable clinical manifestations [6]. The patient could present only with Type 2 Diabetes Mellitus (T2DM) with or without deafness, when the mutation is present at relatively low levels of heteroplasmy (10% to 30%) [7]. However, at levels above 70%, the mutation does not lead to diabetes, but rather to more severe symptoms, such as cardiomyopathy, or mitochondrial encephalomyopathy [5].
The mitochondrial genome is transmitted from the mother because the mitochondria of the spermatozoa are selectively destroyed and eliminated after fertilization [8]. Thus, only the mitochondria of the mother’s oocyte are retained, which will be passed on from one generation to the next. Previous research has shown suggested that spontaneous mutations can occur in mitochondrial disease families, albeit the mechanism is unknown [9,10].
Diabetes and deafness can have a variety of clinical manifestations. Although there is a considerable association between the level of heteroplasmy and illness severity, some phenotypic characteristics can be explained by this correlation.[11,12] , other regulatory factors, such as additional mitochondrial DNA mutations, could also influence the clinical features with the m.A3243G mutation [10,13,14].
Generally, the m.A3243G mutation is a mutation routinely sought in diabetes mellitus associated with sensorineural hearing loss, but other mtDNA mutations are rarely identified [15]. In the present study we sought to determine whether this m.A3243G mutation is significantly associated with established diabetes mellitus in a population of Moroccan deaf diabetics.
Methods![]()
This study was conducted at the Ben M’sik Faculty of Sciences “Laboratory of Physiopathology and Molecular Genetics” (LPGM)., in collaboration with the Division of Hygiene, Prevention and Environment of Greater Casablanca (Morocco). The participants were male and had a mean age of 83.67±8.02 years. They were bilaterally deaf and had a family history of diabetes.
This study was approved by the ethics committees for Biomedical Research of the Faculties of Medicine and Pharmacy of Casablanca and Marrakech. The study was carried out in accordance with the Helsinki ethical guidelines. All ethical dimensions were respected (respect for the anonymity of the participants and discretion in data processing). Told agreement was acquired from the three deaf diabetes patients who were included in this study after they were informed of the study’s goals.
Sample collection
After the clinical examination of the patients, 2-3 ml of whole blood from each participant was taken and collected in EDTA tubes and a dry tube. The EDTA tube was used for DNA extraction and HbA1c measurement, while the dry tube was reserved for blood glucose measurement. The glucose-oxidase/peroxidase enzymatic method was used to determine fasting blood glucose (FBG) by the kit (biosystems Glucose). The principle of the assay lies in the oxidation of glucose by-glucose oxidase, leading to the formation of gluconic acid and hydrogen peroxide. The 4-hydroxyaminophenazone sodium present in the reagent is oxidized by the hydrogen peroxide, in the presence of the peroxidase to form a stable red quinone complex. The pink colouration developed is proportional to the glucose concentration. The absorbance of the standard and sample was determined against the blank at 500 nm.
The glycated hemoglobin (HbA1c) was determined by enzymatic method (Biolabo HbA1c ENZYM) and the concentration of Hemoglobin is expressed as %, using an appropriate calibration curve.
DNA extraction and sequencing
The protocol followed for whole blood DNA extraction was that described by the manufacturer of the Promega kit. The extracted DNA samples were kept at 20°C and subsequently sent to the Laboratory of Genomic Analysis of the National Centre for Scientific and Technical Research (CNRST) in Rabat for sequencing. NANODROP 8000 (Thermo Scientific) was used to quantify DNA and the DNA concentrations after assay were between 22.72ng/ μl and 364.2ng/µl. Polymerase Chain Reaction (PCR) was performed using a primer pair flanking the region with the m.A3243G mtDNA mutation. the primers designs were performed with Primer Express 2;0 software (applied Biosystems, Foster City, CA).
– F: 5′ GTCCTAAACTACCAAACCTGC 3′
– R: 5’AAGGGTTGTAGTAGCCCGTAG 3′
PCR reactions were performed by Kit (Bioline MyTaq DNA polymerase). Each tube contained 5μl of buffer, 1μL of F-primer (10 μM), 1μL of R-primer (10 μM), 0.2μl of Taq DNA polymerase (5U/ μL), 1 μl of DNA, addition of H2O until the final volume of 25 μl. The PCR was carried out in an ABI “Verity” thermal cycler using the following program: 95°C, 2 minutes; (95°C, 30 seconds; 50°C, 30 seconds; 72°C, 30 seconds) 35 cycles; 72°C, 3 minutes.
The amplified PCR products were visualized by electrophoresis on the Bio Analyzer “Qiaxcel”, on a 1% agarose gel. The Sephadex G50 Superfine kit (SIGMA ALDRICH) was used to purify them, and the 3130XL sequencer was used to sequence them.
Genetic sequence analysis
The sequences were aligned to the Human Mitochondrial DNA Reference Sequence NC_012920.1, using the Nucleotide BLAST (Basic Local Alignment Search Tool) program and the position of the desired mutation was located. A reading of the sequencing chromatogram was performed, using Chromas 2.6.6 software, as well as a sequence scan for other mutations.
Statistical analysis
The data was imported into Microsoft Office Excel 2016 and analyzed using SPSS Version 23 software (Statistical Package for the Social Sciences).
Results![]()
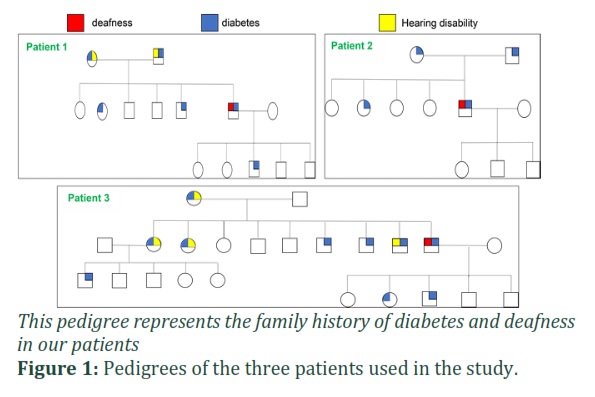
FBG of the participants was 1.8±0.3g/l and glycosylated Hemoglobin (HbA1c) was 8.7±2.4%. Sequencing results showed that there was no pathogenic mutation of mtDNA m.A3243G in our sample. The clinical characteristics of the 3 deaf diabetic subjects are presented in Table 1. All patients had a strong family history of diabetes but not deafness (Fig 1). It should be noted that the parents of patients 1 and 3 had hearing problems with diabetes, while patient 2 nobody has deafness or hearing problems.
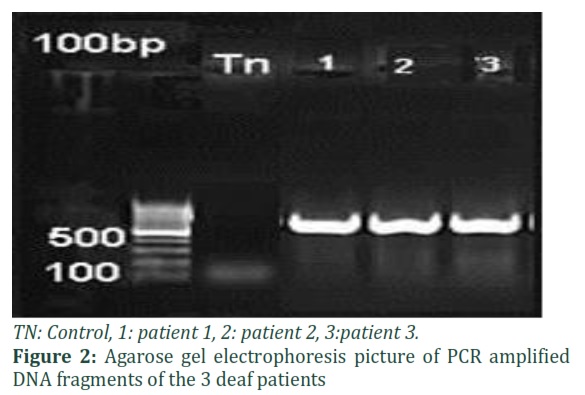
The tRNALeu (UUR) gene in the 3 deaf diabetic subjects was amplified (Fig 2) and sequenced. After careful sequence analysis, we were unable to identify the m.A3243G mutation (Fig 3). Bidirectional DNA sequencing confirmed our sequencing results. Next, we performed comparative analyses of the patient’s sequences with the reference sequence before confirming the sequencing results.
Figures & Tables


Discussion![]()
Mitochondrial diseases are a group of diseases that can affect several organs and then subjects of all ages; their physiopathology involves mutations in mitochondrial DNA (mtDNA) and nuclear genes (nDNA) [16] . They can affect the endocrine glands, gonads, brain, bone marrow, eyes, ears, peripheral nerves, muscles, etc. [16]. Indeed, they are the site of many oxidative metabolic reactions including the production of energy in the form of adenosine triphosphate (ATP). The diagnosis of mitochondriopathies becomes difficult due to the wide range of phenotypes encompassing almost all organ dysfunction [16,17]. Although some clinical manifestations are limited to a single organ, most patients have multiple systemic involvements [16,18,19]. In our study, the 3 selected patients belong to diabetic families with deafness, one of whom had a mother who was blind. Indeed, a mitochondrial DNA mutation can affect the sensory organs of sight and hearing. It can have deleterious effects on energy metabolism, as neurosensory cells are rich in mitochondria and this is proportional to their energy consumption [20]. Various studies have shown a relationship between mutations in mitochondrial genes and diabetes [15]. In addition to environmental factors, genetic factors are a major risk factor and key players in the development of type 2 diabetes.
The most common mutation associated with mitochondrial diabetes is m.A3243G, which is located at the tRNALeu (UUR) of mtDNA. This mutation decreases the binding of the amino acid to its tRNALeu (UUR) , resulting in reduced synthesis of proteins essential for oxidative phosphorylation and consequently impaired mitochondrial ATP production [21,22], as well as decreased glucose-stimulated insulin secretion by pancreatic cells [22].
Our study showed the absence of the pathogenic m.A3243G mutation in the mitochondrial DNA tRNALeu (UUR) in the 3 deaf diabetic subjects and revealed no significant variants in the tRNA-Leu gene. These results are in agreement with those obtained in 6 subjects from a Pakistani family with a mitochondrial diabetes phenotype [23]. This suggests the involvement of other underlying genetic causes in the development of diabetes, as the mitochondrial genome is susceptible to various pathogenic mutations, which would therefore require sequencing of the entire mtDNA [23].
Similarly, Zambelli et al. discovered that 65 local Caucasian diabetics with a mother history of diabetes, four of whom were deaf, did not have the harmful m.A3243G mutation [24]. Also, the study by Mkaouar-Rebai et al. found the absence of the m.A3243G mutation in Tunisian diabetics [25], while the study by Bouhaha et al. showed a low frequency of 1.07% in the latter [26]. This trend was also observed in Indonesia [27] and Pakistan [28]. These results can be explained by the fact that the prevalence of this mutation is about 1.5% in the world diabetic population [21].However, some studies in Japan [29] and Egypt [30] have shown the presence of the m.A3243G mutation. The m.A3243G mutation is considered a cause of maternally transmitted diabetes and deafness in the Egyptian population, with a percentage of 7.3% in all diabetic individuals and a percentage of 30% in diabetics with deafness [30]. According to the literature, mitochondrial diabetes mellitus affects roughly 1.5 percent of diabetics with insulin and non-insulin dependent diabetes, about 6% of diabetics with a maternal history of diabetes, and 60% of diabetics with deafness. [24]. It has been claimed that mitochondrial single nucleotide polymorphisms are related to T2DM, but they seem to differ considerably between regions and populations [31]. Our results did not show an m.A3243G mutation in deaf diabetics. Although previous studies and clinical observations have shown that mitochondrial dysfunction has some role in the progression of type II diabetes, the m.A3243G mutation cannot be as the main cause of deafness in diabetics. Therefore, the involvement of other genetic variants in the etiology of maternal hereditary diabetes can be suggested. A thorough study of deafness-related mutations at the nuclear genome level may be necessary.
Authors’ Contribution
FZK: design, monitoring of subjects, participation in data acquisition, extraction and analysis of the DNA sequence, statistical analysis, analysis and interpretation of results, drafting of manuscript.
TR: conception, supervision of the project, analysis and interpretation of the results, writing and validation of the final version of the manuscript.
HM: design, analysis and interpretation of results, supervision of the project, drafting and validation of the final version of the manuscript.
MJ: therapeutic follow-up of diabetics, validation of the final version of the manuscript.
Ali Labriji: Statistical analysis
FZE: Extraction and analysis of the DNA sequence.
All authors contributed to the realization of this work. All authors also declare to have read the final draft and given his or her approval.
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
- Bouatia-Naji N, Bonnefond A, Froguel P. Inputs from the genetics of fasting glucose: lessons for diabetes. Medical Sciences (Paris), (2009); 25(11): 897-902.
- Schaefer AM, Walker M, Turnbull DM, Taylor RW. Endocrine disorders in mitochondrial disease. Molecular and Cellular Endocrinology, (2013); 379(1-2): 2-11.
- van den Ouweland JM, Lemkes HH, Ruitenbeek W, Sandkuijl LA, de Vijlder MF, et al. Mutation in mitochondrial tRNA(Leu)(UUR) gene in a large pedigree with maternally transmitted type II diabetes mellitus and deafness. Nature Genetics, (1992); 1(5): 368-371.
- Murphy R, Turnbull DM, Walker M, Hattersley AT. Clinical features, diagnosis and management of maternally inherited diabetes and deafness (MIDD) associated with the 3243A>G mitochondrial point mutation. Diabetic Medicine, (2008); 25(4): 383-399.
- Goto Y, Nonaka I, Horai S. A mutation in the tRNA(Leu)(UUR) gene associated with the MELAS subgroup of mitochondrial encephalomyopathies. Nature, (1990); 348(6302): 651-653.
- Wallace DC. A mitochondrial paradigm of metabolic and degenerative diseases, aging, and cancer: a dawn for evolutionary medicine. Annual Review of Genetics, (2005); 39359-407.
- van den Ouweland JM, Lemkes HH, Trembath RC, Ross R, Velho G, et al. Maternally inherited diabetes and deafness is a distinct subtype of diabetes and associates with a single point mutation in the mitochondrial tRNA(Leu(UUR)) gene. Diabetes, (1994); 43(6): 746-751.
- Biousse V, Brown MD, Newman NJ, Allen JC, Rosenfeld J, et al. De novo 14484 mitochondrial DNA mutation in monozygotic twins discordant for Leber’s hereditary optic neuropathy. Neurology, (1997); 49(4): 1136-1138.
- Yamamoto M. Did de novo MELAS common mitochondrial DNA point mutation (mtDNA 3243, A–>G transition) occur in the mother of a proband of a Japanese MELAS pedigree? Journal of the Neurological Sciences, (1996); 135(1): 81-84.
- Jiang Z, Zhang Y, Yan J, Li F, Geng X, et al. De Novo Mutation of m.3243A>G together with m.16093T>C Associated with Atypical Clinical Features in a Pedigree with MIDD Syndrome. Journal of Diabetes Research, (2019); 20195184647.
- Laloi-Michelin M, Meas T, Ambonville C, Bellanné-Chantelot C, Beaufils S, et al. The clinical variability of maternally inherited diabetes and deafness is associated with the degree of heteroplasmy in blood leukocytes. The Journal of Clinical Endocrinology & Metabolism, (2009); 94(8): 3025-3030.
- Ohkubo K, Yamano A, Nagashima M, Mori Y, Anzai K, et al. Mitochondrial Gene Mutations in the tRNALeu(UUR) Region and Diabetes: Prevalence and Clinical Phenotypes in Japan. Clinical Chemistry, (2001); 47(9): 1641-1648.
- Corona P, Antozzi C, Carrara F, D’Incerti L, Lamantea E, et al. A novel mtDNA mutation in the ND5 subunit of complex I in two MELAS patients. Annals of Neurology, (2001); 49(1): 106-110.
- Bindoff LA, Engelsen BA. Mitochondrial diseases and epilepsy. Epilepsia, (2012); 53 Suppl 492-97.
- Tabebi M, Mkaouar-Rebai E, Mnif M, Kallabi F, Ben Mahmoud A, et al. A novel mutation MT-COIII m.9267G>C and MT-COI m.5913G>A mutation in mitochondrial genes in a Tunisian family with maternally inherited diabetes and deafness (MIDD) associated with severe nephropathy. Biochemical and Biophysical Research Communications, (2015); 459(3): 353-360.
- Jardel C, Rucheton B. Diagnostic des maladies mitochondriales. Revue Francophone des Laboratoires, (2018); 2018(501): 36-48.
- McFarland R, Taylor RW, Turnbull DM. A neurological perspective on mitochondrial disease. The Lancet Neurology, (2010); 9(8): 829-840.
- Auré K, Jardel C, Lombès A. [Mitochondrial diseases: molecular mechanisms, clinical presentations and diagnosis investigations]. Annales de Pathologie, (2005); 25(4): 270-281.
- Auré K, Ogier de Baulny H, Laforêt P, Jardel C, Eymard B, et al. Chronic progressive ophthalmoplegia with large-scale mtDNA rearrangement: can we predict progression? Brain, (2007); 130(Pt 6): 1516-1524.
- Alonso L (2016) Déficits de la chaîne respiratoire mitochondriale avec instabilité de Œ ADN mitochondrial : identification de nouveaux gènes et mécanismes: Université Côte d’Azur, 2016. Français. ffNNT : 2016AZUR4101ff. fftel-01466739f. 132 p.
- Gerbitz KD, van den Ouweland JM, Maassen JA, Jaksch M. Mitochondrial diabetes mellitus: a review. Biochimica et Biophysica Acta, (1995); 1271(1): 253-260.
- Hsouna S, Ben Halim N, Lasram K, Arfa I, Jamoussi H, et al. Association study of mitochondrial DNA polymorphisms with type 2 diabetes in Tunisian population. Mitochondrial DNA, (2015); 26(3): 367-372.
- Abrar S, Muhammad K, Zaman H, Khan S, Nouroz F, et al. Molecular genetic analysis of Type II diabetes associated m.3243A>G mitochondrial DNA mutation in a Pakistani family. Egyptian Journal of Medical Human Genetics, (2017); 18(3): 305-308.
- Zambelli A, Vidal-Rioja L. Lack of association between mitochondrial DNA mutation np3243 and maternally inherited diabetes mellitus. Clinical Biochemistry, (1999); 32(1): 81-82.
- Mkaouar-Rebai E, Tlili A, Masmoudi S, Belguith N, Charfeddine I, et al. Mutational analysis of the mitochondrial tRNALeu(UUR) gene in Tunisian patients with mitochondrial diseases. Biochemical and Biophysical Research Communications, (2007); 355(4): 1031-1037.
- Bouhaha R, Abid Kamoun H, Elgaaied A, Ennafaa H. A3243G mitochondrial DNA mutation in Tunisian diabetic population. Tunisie Medicale, (2010); 88(9): 642-645.
- Ishak AR, Puspitaningrum R, Utari RD, Ferania M, Adhiyanto C, et al. Mutation of mtDNA ND1 Gene in 20 Type 2 Diabetes Mellitus Patients of Gorontalonese and Javanese Ethnicity. HAYATI Journal of Biosciences, (2014); 21(4): 159-165.
- Khan N, Ullah H, Raziq A, Khan A, Khan M. Molecular genetic analysis of leucine tRNA in relevance to type 2 diabetes mellitus. Clinical Diabetology, (2020); 9(3): 167-173.
- Yorifuji T, Fujimaru R, Hosokawa Y, Tamagawa N, Shiozaki M, et al. Comprehensive molecular analysis of Japanese patients with pediatric-onset MODY-type diabetes mellitus. Pediatric Diabetes, (2012); 13(1): 26-32.
- FawziO A, Za H, AbdelKawyS I, Al-DiwanyO I, Adela M, et al. Mitochondrial Mutation In Egyptian Patients With Type 2 Diabetes Mellitus. The Egyptian Journal of Hospital Medicine, (2006); 23245-256.
- Liao WQ, Pang Y, Yu CA, Wen JY, Zhang YG, et al. Novel mutations of mitochondrial DNA associated with type 2 diabetes in Chinese Han population. The Tohoku Journal of Experimental Medicine, (2008); 215(4): 377-384.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0