

Full Length Research Article
Mutational analysis of exons 5-9 of TP53 gene in breast cancer patients of Punjabi ethnicity
Haleema Sadia1, Mukhtar Ullah1, Asma Irshad2, Kausar Malik3, Waqas Ahmad3, Rais Ahmed4, Muhammad Umer Khan5, Sana Ashiq1, Ali Akbar6, Atta-ur Rehman7, Shahid Raza8, Kashif Iqbal Sahibzada9
Adv. life sci., vol. 9, no. 1, pp. 18-23, May 2022
*– Corresponding Author: Haleema Sadia (Email: sadiahaleema377@gmail.com)
Authors' Affiliations
2. Department of Life Sciences, University of Management Sciences, Lahore – Pakistan
3. National Centre of Excellence in Molecular Biology, University of The Punjab Lahore – Pakistan
4. Department of Microbiology, CUVAS, Bahawalpur – Pakistan
5. University Institute of Medical Laboratory Technology, University of Lahore, Lahore – Pakistan
6. Department of Microbiology, University of Balochistan – Pakistan
7. College of Animal Husbandry and Veterinary Science, Abdul Wali Khan University Mardan – Pakistan
8. ORIC, Lahore Garrison University, Lahore – Pakistan
9. Institute of Biochemistry and Biotechnology. University of the Punjab, Lahore – Pakistan
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Breast cancer is a multifactorial disease that is influenced by many genes-environment and gene-gene interactions. It emerges due to the perturbations in the tumor suppressor genes. One of these genes is TP53. The TP53 gene plays a crucial role in regulating normal cell proliferation. However, this gene is commonly mutated in different human cancers.
Methods: In the current study, we determined the role of TP53 mutation in breast cancer in the Punjabi ethnic group/patients of Pakistan. This study was undertaken to determine mutation in the hotspot region of TP53 in breast cancer patients. A total of 30 modified radical mastectomies (MRM) tissue biopsies were collected from different hospitals located in Lahore city of Pakistan. Histopathological analysis was performed to determine the cancer type, stage and grade followed by DNA extraction and sequencing to evaluate mutation in the hotspot region of TP53 gene. Sequencing data was visualized with Bio-edit 7.2.5 and chromas.
Results: According to the Nottingham scoring system 70% patients have grade 3 tumors, followed by grade 2 (23%), grade 4 (6%) and grade-1 (3%). Sanger sequencing analysis of exon 5-9 of TP53 show no mutation. However, many noise mutations were there, which are discussed in detail. This study also shed light that how a genetic analyzer’s results can be correctly analyzed and to avoid false reporting of any mutation which could be a disaster for mis diagnosis of disease. Besides this, a new recipe with very low volume for sequencing PCR ingredients was introduced which could reduce the cost of sequencing.
Conclusion: The present study suggests that there might be no correlation between TP53 exon 5-9 mutation and breast cancer in the Punjabi ethnic group of Pakistan. However, more studies are required to investigate mutation in the other exons of TP53 gene in large patients’ cohort.
Keywords: Breast cancer; TP53 mutation; Punjabi ethnicity
Introduction![]()
Globally, breast cancer is the second most common each year, affecting 2.1 million women [1]. In the Asian region, the mortality rate is 44%. In the year 2018, approximately 46.3% of breast cancer cases reported in both genders [2]. However, the risk rate in men is about 1 in 1000 [3].
In the developed countries only 89% of females survive for five years after cancer detection [4] however, the survival rate is very low in underdeveloped countries due to lack of advanced health facilities and late-stage diagnosis. Breast tumors can be classified into different types and grades on the basis of tumor site and size. According to the American Cancer Society, the most common breast cancer is Ductal Carcinoma in Situ (DCIS), Invasive Ductal Carcinomas (IDC), Invasive Lobular Carcinomas (ILC), and Inflammatory Breast Carcinoma (IBC). Similarly, there are different grades of breast cancer depending on the tumor size. Commonly tumor is graded from 1 to 4. This depends on the cells that how quickly divide. The cell division is mainly controlled by TP53 gene. The TP53 gene is one of the most investigated and frequently mutated gene in human carcinoma [5]. Mutations mostly occurs in the hotpot regions. These regions located in the in codon 175, 245, 248, 273 and 282 of TP53. Mutation in these codons impaired the binding which leads to disruption in normal cellular processes [6].
The present study was designed to check alteration in the exon 5-9 of TP53 gene in breast cancer patients in the Punjabi ethnic group which are the largest ethnic group in Pakistan. This study shed light on the role of exon5-9 of TP53 in breast cancers.
Methods![]()
A total of thirty MRM specimens were taken in two separate vials of 10% formalin and RNA later. Samples collected for the histological purpose were kept at room temperature to preserve the tumor cell morphology, while the other samples were stored at -80oC. Histological analysis was performed in Fatima memorial hospital Lahore using the established H & E staining protocol [7]. The ethical protocols were strictly followed. The ethical review board approved the study.
DNA Extraction
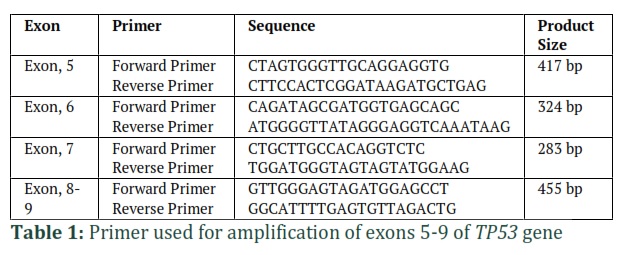
The Tiangen DNA extraction kit was used for the isolation of DNA from specimens. DNA purity and quantification were measured by Nano-Drop 1000 USA. Primers for exons five and six were designed using snap gene 3.3.3 software while for exon 7-9 already reported primers were used [8]. The primers were designed to bind 50 bp away from the coding region. All the sequences of primers are given in table 1.
Gel Electrophoresis
PCR amplified exons were examined on 1.4% w/v Sea Kem LE agarose gel (Lonza, Rockland, ME, USA). The gel was prepared in 0.5X Tris-Borate-EDTA buffer. 2 µl of PCR products were loaded on the gel. The gel was observed by using the Bio-Rad Gel Doc (BIO-RAD, Hercules, CA, USA). The rest of the PCR products were purified and proceed for sequencing PCR.
Sequencing PCR
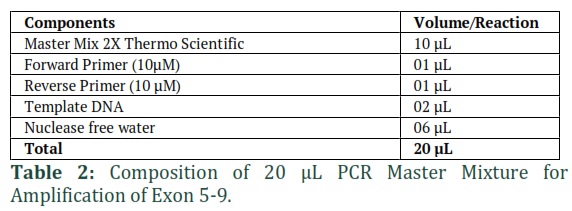
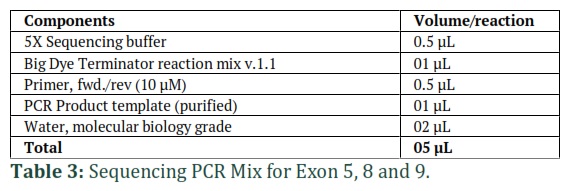
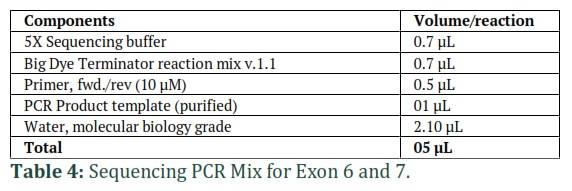
The sequencing PCR was performed in 5 µl reaction volume. 5X Sequencing buffer (Life Technologies, Carlsbad, CA, USA) was used. The reaction was performed with either forward or reverse primer and the DNA concentration was 5-10ng and the recipe of the sequencing reaction are given in the Table 3 and 4. The sequencing PCR consisted of the following cyclic conditions: one cycle at 96°C for 3 minutes, 30 cycles at 96°C for 30 seconds, 50°C for 15 seconds, 60°C for 4 minutes and one cycle of 60°C for 4 minutes.
Capillary Electrophoresis
After sequencing PCR, the amplicons were purified before capillary electrophoresis. For this purpose, 2 µL of 3 mM sodium acetate and 2 µL of 125 mM EDTA and 25µL absolute ethanol were added in each well of the 96 well plate. The plate was vortexed, incubated for 30 minutes at room temperature and then centrifuged at 3000 rpm for 25 minutes at 4°C. Finally, 70% ethanol, 50 µL added and at 4°C centrifuged for fifteen minutes at 3000 rpm. Then the product was air-dried. Thirteen microliters (13 µl) formamide was added and heat shocked for 5 minutes at 97°C. The plate analyzed ABI 3730 genetic analyzer (GA). Sequencing data were analyzed with Bio-edit 7.2.5 and Chromas 2.62.
Results
![]()
Most of the patients were at advanced cancer stage
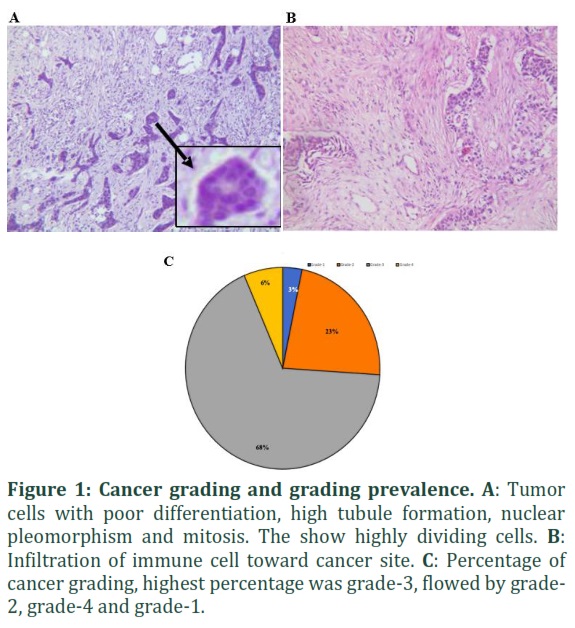
According to the histopathological analysis most of the patient’s samples were diagnosed with advanced cancer stage. The cancer grading was done according to the Nottingham grading system. According to this system, the cancer is graded on basis of three main characteristics, i.e., tubule formation, nuclear pleomorphism and mitotic activity. Each of these characteristics is scored from 1 to 3. The initial stage of cancer, which is close to normal cell morphology is scored as 1 while the cancer cells that possess extremely abnormal are scored as 3. In our study, most of the patient sample showed the highest level of tubule formation and nuclear pleomorphism while mild to moderate level of mitosis. Tubule formation and nuclear pleomorphism have scored 3 while mitosis was scored 1 and 2 respectively. In figure 1A, the cancer was grade 3. The cancerous cells showed poor differentiation. The tubule formation and nuclear pleomorphism were scored 3 as the worst while the mitosis scored 2 as a moderate level of cell division (fig. 1A). Furthermore, the infiltration of immune cells was also higher in grade 3 cancer patients which showed a high level of inflammation (Fig. 1B).
The high number of immune cells at the infected site correct the cancer stage. In the current study, most of the patient’s sample showed scores 3+3+2 respectively. According to the Nottingham grading system, the higher percentage (70%) of the patients had grade -3 followed bygrade2 (23.33%), grade 4 (6.66%) and only 3.3% of patient had grade 1 tumor (Fig. 1C). All these data suggest that most of the patients diagnosed when the cancer cells grow into an advance stage. This is due to lack of awareness, social problem and late-stage diagnosis.
Exon 5-9 mutation has no link with breast cancer in Punjabi ethnicity
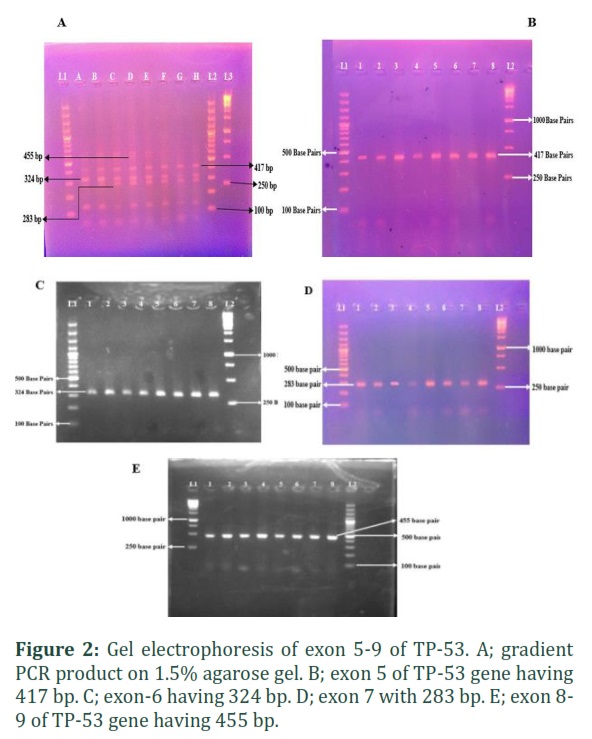
After histopathological confirmation of cancer, we checked whether there is any correlation between a mutation in exon 5-9 of TP53 and breast cancer in the patients of Punjabi ethnicity. For this purpose, we extracted DNA from the tissue biopsy which was reconfirmed by histological analysis (fig. 1). Exons 5-9 of the TP53 gene were amplified using different annealing temperatures. The amplicon size of each primer pairs was confirmed through gel electrophoresis. All the primers bind 30 to 50 bp upstream and downstream of each exon. To amplify all the exons, we performed gradient PCR for all primers and noted the best annealing temperature. The size of each exon was confirmed according to the expected product size (fig. 2A). After gradient PCR each exon amplified separately for further downstream analysis. The primers used to amplify 417 bp of exon 5 (Fig 2B) 324 bp of exon- 6 (Fig. 2C), 283 bp of exon-7 (Fig. 2D) and 455 bp of exon 8-9 (Fig. 2E). Exons 8 and 9 were amplified with single primer pair because both exons are small and close to each other. After successful amplification and confirmation of exon through gel electrophoresis. We sequenced all the exons with a single primer either forward or reverse. Sequencing data were analyzed through bio edit and chromas. The electropherogram of all the sequences was inspected thoroughly. Samples showed too much noise and overlapping electropherogram were re-sequenced either forward or reverse primer. The sequence was blasted using the NCBI blast tool for aligning to reference gene sequence. We found many mismatches in the aligned sequence. However, when we read and analyzed the electropherogram of the sequence. We suspected that the mismatch might be due to misread by a genetic analyzer. Therefore, either we sequenced the sample reverse primer or compare the electropherogram peak with corresponding nucleotide reads.
Analysis of Mismatches
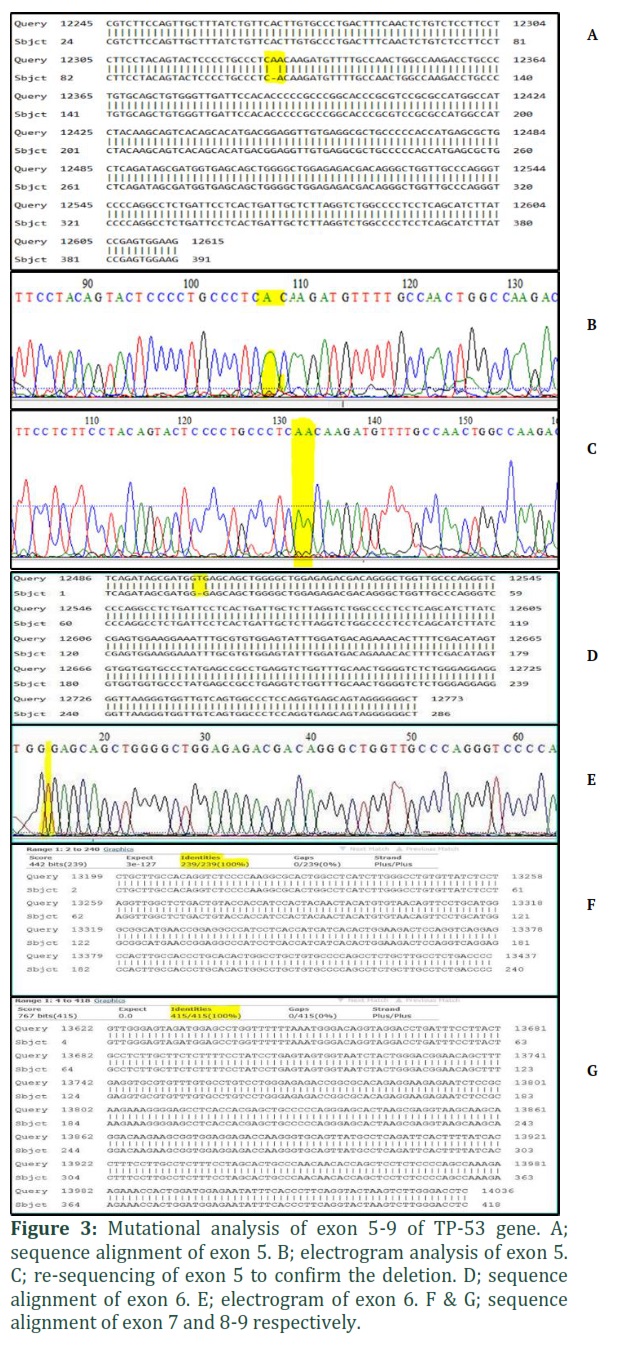
The analysis of the peak of that sequence was done by using the BioEdit software which revealed the presence of mismatches. The software showed any mismatch in nucleotides, but when we analyzed carefully either the sequence or the peaks of electropherograms, indeed it was miss reading of the genetic analyzer but not a mutation in the exons (fig. 3).
Similarly, when we aligned exon-5 sequence with reference sequence (NC_000017). In the alignment at position 12330 revealed a deletion of adenine (Fig 3A). Further through the software analysis, it shows a wide adenine peak (fig 3B). We suspected that this might be due to misreading of the sequence. When we repeated the same sample with reverse primers and shows two adjacent adenines with sharp peaks (fig. 3C) at the same place and there was deletion. Overall, this figure suggests that machine mixed the sequence and read as single nucleotide. In similar context another exon-6 sequence showed a deletion of thymine at position 12500 bp when aligned with reference sequence (fig. 3D). Again, when we checked the electropherogram of the same sequence in Bio edit software. The peak of the thymidine was present, but the software couldn’t read the nucleotide sequence (Fig. 3E), which indicate the error of genetic analyzer. The same sequence was reconfirmed with both forward and reverse primers. Contrary to exon-5 and exon-6 misreading, the other exons show 100% similarity with a reference sequence (fig. 3F & 3G). All these results suggest that there might be no correlation between mutation in exon 5-9 of TP53 and breast cancer in Punjabi ethnic group of Pakistan. However, more studies are required to investigate mutation in TP53 gene in large patient cohort. Apart from this, reporting any mutation we should pay great attention and re-confirm with different tools otherwise fall mutation could be disaster for miss diagnosis of the disease.
Figures & Tables
Discussion![]()
The p53 is the tumor suppressor gene located at 17p13 of chromosome 17. Its size is approximately 20 kilobase [9]. It is composed of three hundred and ninety-three amino acids and contains 11 exons [10]. The deletion or dislocation in this gene region most commonly associated with breast cancers [11]. The homozygous deletion occurs in less percentage as compared to the heterozygous loss at the gene location [12, 13]. It provides presumptive evidence of the TP53 gene involvement in causing breast cancer but does not exclude other cancer suppressor genes [14] as the p53 gene is not mutated in all sporadic cancers [15]. There is various evidence that suggests that exon 5-9 have many missense mutations in it [16]. Many studies prove that it has some variations among different ethnic groups. A study reported that the pattern of mutation in Japanese women is different as compared to their American and European counterparts [17]. Base on such evidence we proposed the current study to investigate the role of mutation in exon-5 to exon-9 of TP53 gene in breast cancer patients. The result could increase our understanding of breast cancer in South Asia especially in Pakistan.
In the present study, we couldn’t found a significant relation between exon 5-9 mutation and breast cancer patients. Our results are closely related to the finding of Rashid et al. They studied sporadic and familial breast cancer. They found only one patient out of 67, who had germ line mutation in TP53 [18].
Similarly, Roy and colleagues report the same results from West Bengal, India [19]. Their results are consistent with our finding. They studied mutation in exon 5-7 in the Indian population. They couldn’t find any significant mutation in exon 5-7 in breast cancer patients. They emphases that it could be different in different ethnic groups [20]. Another study by Miller et al suggested that high genomic variability among different ethnic group make them prone to breast cancer. According to their finding that the Vietnamese and Korean population have a low risk of breast cancer as compared to the black American and white non-Hispanic population [21]. Overall, this suggests that breast cancer couldn’t be limited to some cancer specific genes, but the etiology is quite diverse and could be different in different ethnic groups.
Very recently, Bataillon et al., conducted a study to investigate the role of TP53 mutation and breast cancer. They did the sequencing of 50 different genes in 10 out of 13 low-grade breast carcinomas. Interestingly they couldn’t find any single mutation in TP53 gene [22]. In contrast, a similar study conducted by Akhter et al, in the Bangladeshi cohort. They performed a targeted sequencing screen of the novel mutations in the genes of breast cancer patients. They screened the two exonic regions of TP53 gene. They found one frame shift insertion in exon-5 and another missense mutation in exon-7. This result suggests that mutation might be specific to ethnicity because they found two mutations large homogenous population [23]. Taking all the results together we couldn’t rollout the importance of TP53 in breast cancer, however, the mutation pattern could be different in different ethnic groups.
In the present study, we couldn’t find a single mutation in exons 5-9 of the TP53 gene in breast cancer patients of Punjabi ethnicity of Pakistan. The exons 5-9 might have no role in breast cancer progression of the Punjabi ethnic group. There is a need to study a large cohort, including familial cancers and sporadic breast cancer patients.
Author Contributions
HS designed and supervised the study. MU did the experiments, data analysis and wrote the first draft of manuscript, WA, AT critically reviewed, made corrections, and wrote the discussion part. MUK, TN, AA, SR, KI, RA, KM, AI, HS and KM helped in sample collection, histopathological analysis, demographic data collection, paper write up, editing and review procedure of the study.
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
- Nakayama M, Hong CP, Oshima H, Sakai E, Kim SJ, Oshima M. Loss of wild-type p53 promotes mutant p53-driven metastasis through acquisition of survival and tumor-initiating properties. Nature communications, (2020); 11(1): 1-4.
- Ferlay J, Colombet M, Soerjomataram I, Siegel R, Torre L, Jemal A. Global and regional estimates of the incidence and mortality for 38 cancers: GLOBOCAN 2018. Lyon: International Agency for Research on Cancer. World Health Organization, (2018).
- Hoffman J, Fejerman L, Hu D, Huntsman S, Li M, John EM, et al. Identification of novel common breast cancer risk variants at the 6q25 locus among Latinas. Breast Cancer Research, (2019); 21(1): 1-12.
- Kamangar F, Dores GM, Anderson WF. Patterns of cancer incidence, mortality, and prevalence across five continents: defining priorities to reduce cancer disparities in different geographic regions of the world. Journal of clinical oncology, (2006); 24(14): 2137-50.
- Gottlieb E, Vousden KH. p53 regulation of metabolic pathways. Cold Spring Harbor perspectives in biology, (2010); 2(4): a001040.
- Baugh EH, Ke H, Levine AJ, Bonneau RA, Chan CS. Why are there hotspot mutations in the TP53 gene in human cancers?. Cell Death & Differentiation, (2018); 25(1): 154-60.
- Mateen I, Irshad S. Mutational analysis of p53 gene in sporadic breast carcinoma. Pakistan Journal of Biochemistry and Molecular Biology, (2015); 48(3): 79-83.
- Liu Y, Bodmer WF. Analysis of P53 mutations and their expression in 56 colorectal cancer cell lines. Proceedings of the National Academy of Sciences, (2006); 103(4): 976-981.
- Lamb PE, Crawford LI. Characterization of the human p53 gene. Molecular and cellular biology, (1986); 6(5): 1379-1385.
- Levine AJ, Perry ME, Chang A, Silver A, Dittmer D, Wu M, et al. The 1993 Walter Hubert Lecture: the role of the p53 tumour-suppressor gene in tumorigenesis. British journal of cancer, (1994); 69(3): 409-416.
- Callahan R, Cropp CS, Merlo GR, Liscia DS, Cappa AP, Lidereau R. Somatic mutations and human breast cancer. A status report. Cancer, (1992); 69(S6): 1582-1588.
- Singh S, Simon M, Meybohm I, Jantke I, Jonat W, Maass H, et al. Human breast cancer: frequent p53 allele loss and protein overexpression. Human genetics, (1993); 90(6): 635-640.
- Muller PA, Vousden KH. p53 mutations in cancer. Nature cell biology, (2013); 15(1): 2-8.
- Kerangueven F, Eisinger F, Noguchi T, Allione F, Wargniez V, Eng C, et al. Loss of heterozygosity in human breast carcinomas in the ataxia telangiectasia, Cowden disease and BRCA1 gene regions. Oncogene, (1997); 14(3): 339-347.
- Carey LA, Perou CM, Livasy CA, Dressler LG, Cowan D, Conway K, et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. Jama, (2006); 295(21): 2492-2502.
- Hollstein M, Sidransky D, Vogelstein B, Harris CC. p53 mutations in human cancers. Science, (1991); 253(5015): 49-53.
- Biggs PJ, Warren W, Venitt S, Stratton MR. Does a genotoxic carcinogen contribute to human breast cancer? The value of mutational spectra in unravelling the aetiology of cancer. Mutagenesis, (1993); 8(4): 275-283.
- Rashid MU, Gull S, Asghar K, Muhammad N, Amin A, Hamann U. Prevalence of TP53 germ line mutations in young Pakistani breast cancer patients. Familial cancer, (2012); 11(2): 307-311.
- Roy AG, Sarkar BN, Roy R, Rao VR, Bandyopadhyay AR. Absence of p53 gene mutations in exons 5-7 among breast cancer patients of Bengalee Hindu caste females, West Bengal, India. Asian Pacific Journal of Cancer Prevention, (2012); 13(9): 4477-4479.
- Das SK, Dhanya L, Varadhan S, Mukherjee S, Vasudevan DM. Effects of chronic ethanol consumption in blood: a time dependent study on rat. Indian Journal of Clinical Biochemistry, (2009); 24(3): 301-306.
- Miller BA, Kolonel LN. Racial/ethnic patterns of cancer in the United States: 1988-1992. US Department of Health and Human Services, National Institute of Health, (1996); 96.
- Bataillon G, Fuhrmann L, Girard E, Menet E, Laé M, Capovilla M, et al. High rate of PIK 3 CA mutations but no TP 53 mutations in low‐grade adenosquamous carcinoma of the breast. Histopathology (2018); 73(2): 273-283.
- Akter H, Sultana N, Martuza N, Siddiqua A, Dity NJ, Rahaman MA, et al. Novel mutations in actionable breast cancer genes by targeted sequencing in an ethnically homogenous cohort. BMC medical genetics, (2019); 20(1): 1-8.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0