

Full Length Research Article
An Investigation into the Evaluation of the Satisfaction with Prenatal Care Services among Pregnant Women Attending Healthcare Centers during Pregnancy in the Capital of Lorestan Province, Iran
Khatereh Anbari1, Amir Hossein Yousefvand2, Pardis Qanadi2, Firouz Amraie3*
Adv. life sci., vol. 9, no. 2, pp. 224-230, July 2022
*– Corresponding Author: Firouz Amraie (Email: amraeifirouz@gmail.com)
Authors' Affiliations
2. Student of Medicine, Lorestan University of Medical Sciences, Khorramabad – Iran
3. Instructor, School of Medicine, Lorestan University of Medicine Sciences, Khorramabad – Iran
Editorial Expression of Concern
20 June 2025: Following publication of this paper, the internal audit (consequent to concerns on quality raised by Web of Science) notified Advancements in Life Sciences about suspected plagiarism. By this Editorial Expression of Concern, we alert the scientific community of the errors as we reconcile the records.
Editorial Note
25 June 2025: While rerunning the Turnitin originality analysis, a similarity index of 49% was found for this article (40% from a single source). Editorial board of Advancements in Life Sciences has started the process of retracting this article due to the above post-publication findings. The process shall be concluded after registering responses from the authors. Meanwhile, full text of the article shall remain unavailable for citations (this notice has been updated following insights derived from relevant COPE cases and the industry standards). Show of cause notice has also been issued to the concerned editorial team member.
Rescinded: Editorial Expression of Concern
23 July 2025: Editorial expression of concern issued on 20 June 2025 is hereby rescinded on account of author's explanation of the found similarity. Author's justification reads "I would like to sincerely confirm that the similarity identified—specifically with the article titled “Evaluation of the Utilization Rate of and Satisfaction with Prenatal Care among Pregnant Women Referred to Khorramabad Therapeutic Health Centers in 2020”—is indeed the result of a technical issue. This manuscript had been previously submitted to another journal (name redacted), but it was withdrawn before publication due to author request and lack of final confirmation from the editorial process. It appears that despite the withdrawal, a version of the manuscript file may have inadvertently remained accessible through the journal’s backend server or archive, leading to the match found in the Turnitin similarity analysis. As such, I respectfully confirm that the current article submitted to Advancements in Life Sciences is our original and unpublished work, and that the detected similarity stems from the aforementioned technical lapse, not from any form of unethical duplication".
Concluding remarks: The inquiry team concurs with the authors as it could not find the article highlighted in the Turnitin Originality Analysis report either in the other journal's referred issue or elsewhere on the internet. With this rescinding note, a signed declaration from authors is also being made available here. Editorial office may be contacted for more details, if required.
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Pregnancy period is one of the most important periods for mother and infant, and the maternal and fetal health during this period is of paramount importance. This study aimed to evaluate the satisfaction with prenatal (also known as antenatal) care services among pregnant women attending healthcare centers in the capital of Lorestan province (Khorramabad, west Iran).
Methods: This cross-sectional (descriptive-analytical) study evaluated the satisfaction with benefitting from prenatal care services among pregnant women in the last months of pregnancy. The research sample was selected using a multistage sampling method involving a combination of stratified, cluster, and random sampling. The required data were gathered using a three-part questionnaire, including information regarding demographic survey questions, information about the extent to which pregnant women in Khorramabad benefit from prenatal care services, and the degree of pregnant women's satisfaction with prenatal care. Independent t-test and one-way analysis of variance (ANOVA) were used to analyze the data.
Results: According to the obtained results, the mean score of benefiting from and satisfaction with prenatal care services was high. The difference in the score of benefitting from services was statistically significant in terms of type of pregnancy and a history of stillbirth (p <0.05). The number of children, occupation, and type of pregnancy were statistically significant, and these factors produced the mean satisfaction score (p <0.05).
Conclusion: To increase the rate of benefiting from and satisfaction with prenatal care services among pregnant women, the health authorities of the region should take effective practical and educational measures to improve the quality-of-care delivery, train health service providers, and complete and equip prenatal centers.
Keywords: Satisfaction; Care; Pregnant women; Healthcare centers
Introduction![]()
As one of the indicators of quality of health services, patients' satisfaction has received lots of attention from many healthcare organizations today [1]. The importance of satisfaction issue in a healthcare provision system rises as experiencing the illness and the necessity of following up the treatment and care process increase the patients’ vulnerability and further their need for comprehensive support [2]. The association between the patient’s health status and satisfaction with healthcare services has been investigated in several studies [3]. Pregnancy care plays a key role in a healthy lifestyle during pregnancy and includes specific periodic checkups during this period. Prenatal care is essential for the health and well-being of the mother and fetus.
Pregnancy care is of significant importance. Proper fetal growth and maintaining maternal and fetal health are dependent on prenatal care. Part of this care includes proper nutrition and healthy eating habits prior to and during pregnancy. However, the other part of this care depends on regular examinations done by the physician, and laboratory and clinical screenings leading to risk attenuation for the fetus [4].
Receiving inadequate or a low rate of prenatal care is one of the causes of maternal or fetal mortality [5]. Research studies show that prenatal care in women causes a healthy and good pregnancy experience for women and promises having healthy children in the future [6]. Quality improvement of midwifery care is one of the important parts of prenatal care [6]. Mothers who are more satisfied with care quality during this period experience a better pregnancy [6].
In case of benefiting from prenatal care, the overall fetal mortality rate is 2.7 per 1000 live births and it reaches 14.1 per 1000 live births when no prenatal care is received [7].
The quality of prenatal care services is of paramount importance. Inadequate care is the cause of abortion and intrauterine fetal demise [8]. A significant reduction was observed in preterm births or low-birth-weight infants among women with prenatal care [8]. However, the quality of midwifery care is poor and undesirable in many countries, including Iran [8].
One of the most important aims of healthcare providers is to satisfy patients, especially pregnant women. Assessment of healthcare recipients' (pregnant women) satisfaction is one of the important items of healthcare quality that results in the birth of a healthy child [9]. Given the importance of prenatal care and its effect on maternal health and the birth of a healthy infant, quality improvement of healthcare, especially throughout pregnancy, is of significant importance. Quality improvement of health services is impossible without paying attention to the demands of services recipients [10].
Healthy women are the main pillars of any society and maintaining the health of pregnant women is among the most important priorities of healthcare providers. Healthcare services recipients are themselves capable of evaluating the quantity and quality of care services. These recipients' expectations and needs can thus be used in evaluating healthcare services [11].
Control and evaluation of healthcare services is the first necessary step toward provision of proper services, and clients' satisfaction rate is one of the most important factors in evaluation of healthcare services. As the provision of healthcare services is not desirable in some cases, investigation of the status of services provision to pregnant mothers and their needs and expectations can contribute to improving the quality of services [12]. The results from a study indicated that most of the pregnant women were satisfied with the provision of prenatal care [13,14]. Another study showed that the mean level of satisfaction in the experimental group was significantly higher than that in the control group [15-18].
The purpose of the present epidemiological study was to evaluate the pregnant women's satisfaction with and benefiting from the prenatal care services in the capital of Lorestan province (west Iran).
Methods![]()
The data of the present epidemiological (descriptive-analytical) study were collected using a survey. The studied population consisted of women who were in the eighth and ninth months of pregnancy attending healthcare centers in the capital of Lorestan province (west Iran). The research sample was selected using a multistage integrative sampling method (stratified, cluster, and random sampling).
The target healthcare centers were investigated in different regions of the capital of Lorestan province (north, south, and central regions). The comprehensive health center was selected as the head cluster for each region. Three to five comprehensive health centers were then randomly selected from each region and consecutive sampling was performed among pregnant women in each sampling center. Considering p = 48%, z (1-a/2) = 1.96, and d = 0.06, the final sample size was calculated 266 (considering the cluster sampling error, it was multiplied by 1.2 and the final sample size was calculated 319).
The required data were gathered using a three-part questionnaire. The first part included information regarding age, education level, place of residence, occupation, as well as the history of fertility and pregnancy, i.e., age of pregnancy, number of children, order of pregnancy, type of pregnancy, history of abortion and stillbirth, etc. The second part of the questionnaire included information on benefiting from prenatal care. A positive answer was given a score of 1 and a negative answer was given a score of 0. The third part of the questionnaire was related to the evaluation of clients' satisfaction. A standard 20-item questionnaire was used to evaluate the clients' satisfaction rate regarding different issues (items included physical space, physical and geographical access, waiting time to receive service, staff behavior, personnel and center cleanliness, confidentiality and respect for privacy, emotional support, adequacy of the center's welfare facilities, and the extent to which the personnel meet clients' needs, etc.). The Lawshe test was used to examine the content and face validity of the questionnaire. Cronbach's coefficient α was used to estimate the degree of reliability (α =0.91). Descriptive statistics methods (ratios, percentage, mean and standard deviation) were used to describe data, and the statistical data analysis was performed using independent t-tests, one-way ANOVA and linear regression analysis via SPSS software version 19.
Inclusion criteria were being pregnant (eighth and ninth months of pregnancy) and residing in the capital of the province. Exclusion criteria were not willing to participate in the study.
Results
![]()
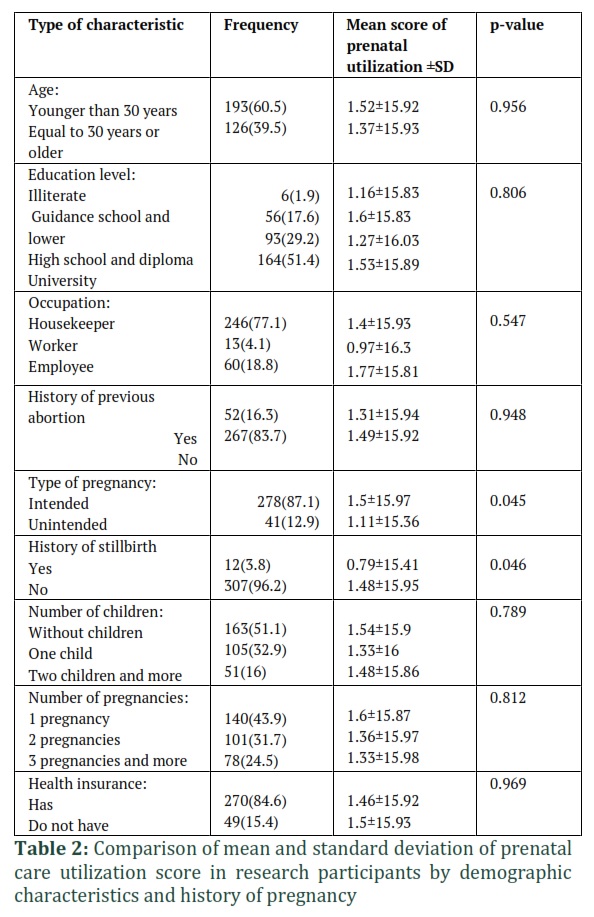
Considering the research findings, 60% of the respondents were in the age group under 30 years, 51% had academic education, 77% were housekeeper, 53% lived in a family of two persons, 51% had no children, 44% had experienced 1 pregnancy, 87% had intended pregnancy, 84% had no history of abortion and 96% had no history of stillbirth in previous pregnancies; moreover, 85% were under the coverage of health insurance (Table 2).
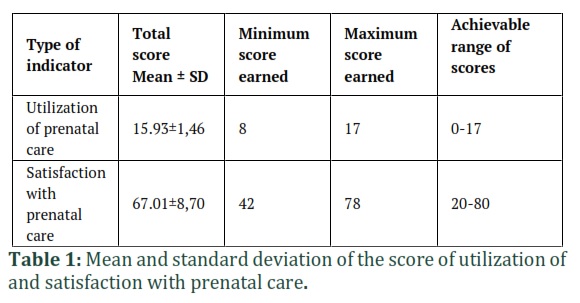
The mean score of prenatal care utilization and satisfaction with prenatal care showed the high rate of utilization of and satisfaction with prenatal care (given the scores domain) in the research participants (Table 1).
The best status is related to the items: recording the health history by the center staff at the first visit (100%) and the request for medical tests at the first visit (100%), and the worst status was related to receiving prenatal counseling from the center personnel (71.8%), recording medical history and previous pregnancy history (80%), education on non-smoking and alcohol during pregnancy (84%) and education on the number of hours required for sleeping and taking a rest (87.8%).
The worst status was related to the item: the status of satisfaction with waiting more than 15 minutes for service provision (lowest score), and after that the item: opportunity and likelihood of training by experts and midwives in training groups in the presence of other pregnant women, as well as the item: satisfaction with the extent to which the care providers attempt to get clients engaged in decision making process. Moreover, the research participants were most satisfied with being carefully listened by staff about the clients' concerns, and the provision of high quality and clear information about prenatal care by the care provider.
By using independent t-test, it was found that the difference in the utilization score was not statistically significant by age (Pv=0.956), history of previous abortion (Pv=0.948) and history of being or not being under the coverage of health insurance (Pv=0.969). The difference in the health services utilization score was statistically significant between the subjects in terms of the type of pregnancy (Pv=0.045) and a history of stillbirth (Pv=0.046); and the utilization rate of prenatal care was lower in persons with a history of stillbirth and unintended pregnancy. Additionally, according to one-way ANOVA results, the difference in the utilization score was not statistically significant between the studied pregnant women based on their occupation (Pv=0.542), education level (Pv=0.806), number of children (Pv=0.789), and number of pregnancies (Pv=0.812) (table 2).
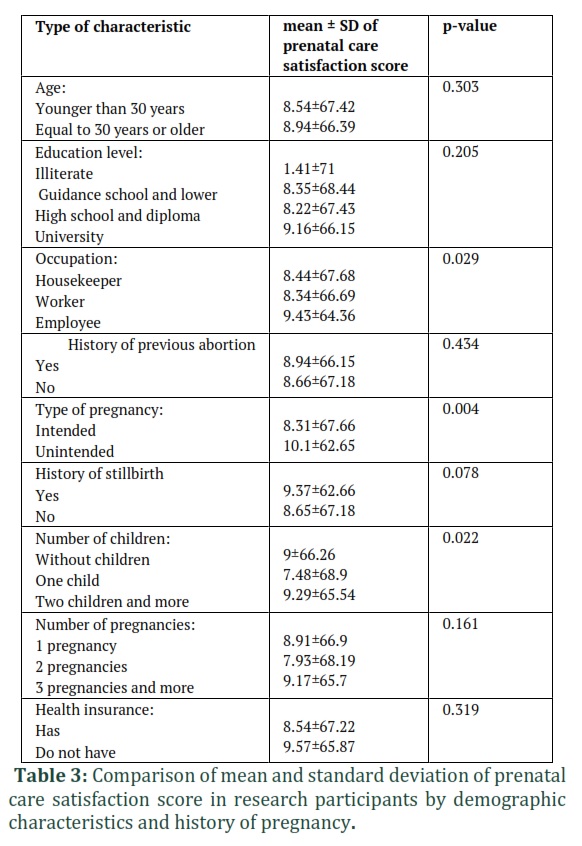
Based on the result of statistic calculation independent t-test, it was found that the difference in the mean score of satisfaction was not statistically significant between the study subjects by age (Pv=0.303), the education level (Pv=0.205), a history of previous abortion (Pv=0.434), a history of stillbirth (Pv=0.078), and a history of being or not being under the coverage of health insurance (Pv=0.319). However, according to the results of independent t-test, the difference in the mean score of satisfaction was statistically significant (Pv=0.004) between the study subjects by the type of pregnancy (intended or unintended). Additionally, according to one-way ANOVA results, the difference in the mean score of satisfaction with prenatal care was statistically significant (Pv=0.029) in terms of occupation, and the housewives scored higher than any other occupational group. According to one-way ANOVA results, the difference in the score of satisfaction was not statistically significant based on the education level (Pv=0.205) and the number of pregnancies (Pv=0.161). Finally, the difference in the mean score of participants' satisfactions was statistically significant based on the number of children (Pv=0.022) (Table 3).
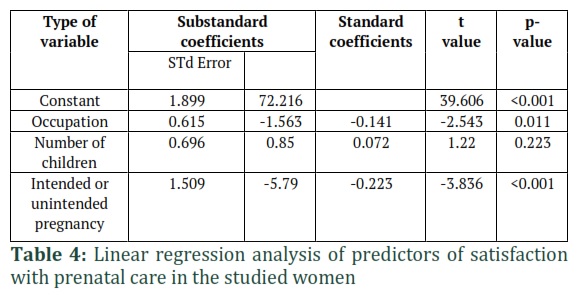
In linear regression analysis to investigate the predictive factors of satisfaction with prenatal care services in the subjects, the relationship between the number of children and the level of satisfaction that was significant in the univariate test was not statistically significant in the multivariate test (Pv = 0.223).
But the relationship between occupation and the level of satisfaction with prenatal care (Pv=0.011), as well as the relationship between the type of pregnancy in terms of being intended or unintended and the level of satisfaction with prenatal care (Pv<0.001) significant in univariate analysis also became significant in multivariate analysis using linear regression. Therefore, occupation and type of pregnancy were predictors of satisfaction with prenatal care in the studied women.
Figures & Tables
Discussion![]()
The best empirical therapy should include According to the obtained results, the mean score of health-promoting behaviors was 122.6. The present study showed that most of the youth under study had a moderate performance level regarding health-promoting behaviors. The results of a study on health-promoting behaviors in students of Birjand University of Medical Sciences indicated that the performance level was moderate in students [19]. The results of our study regarding the status of health-promoting behaviors are similar to those obtained in a study by Rastegar et al., and in agreement with the results of a study conducted in Mashhad. The study conducted in Mashhad showed the moderate performance level of health volunteers regarding the adoption of health-promoting behaviors [20]. The high score obtained for the spiritual growth aspect and the low score for physical activity are consistent with the results of the study by Rastegar et al. [19]. Considering the health-promoting behaviors among nurses in selected military hospitals in the study by Kalroozi et al., the highest and the lowest mean score was related to the spiritual growth aspect and physical activity, respectively [21]. The lowest score obtained for physical activity was reported in the studies by Wittayapun et al. [22], Asgarshahi et al. [23], and Modanloo et al., [24]. Among the outcomes of today’s generation is the lack of proper physical activity. One of the reasons for this problem is the constant use of computers and mobile phones. The other reason is less inclination to exercise. A total of 43.6% of participants in our study showed a poor level of performance. The results of our study showed that practice of stress management behaviors was found to be poor in 48.6% of participants. This can be attributed to the lack of effective coping skills to control stressors. In this study, there was a moderate correlation between nutrition behaviors and performance of 79.6% of the studied youth. This finding is in a similar vein with those obtained by Raiyat et al. [25] and Fathi et al., [26]. The family characteristics, parental and friends' dietary patterns, as well as the socio-economic status and advertisements affect the dietary patterns and nutrition behaviors of the youth.
The difference in physical activity dimension was statistically significant between girls and boys. Quintiliani showed that the prevalence of unhealthful behaviors regarding the physical activity dimension was significantly higher in women than in men [27]. The lower level of physical activity reported in women as compared to the men is in agreement with findings of the study by Moieni [28] and other studies [29,30]. Considering health promoting behaviors in health workers, a significant relationship was observed between gender and health promoting behaviors [31].
In a study by Khazaie et al., [19] and another study conducted in Hong Kong, women scored higher on interpersonal relationships than men [32]. We showed that the health responsibility score was higher in women than in men. The level of responsibility in men was also reported to be higher in studies abroad [7, 33]. No significant relationship was observed between age and health-promoting behaviors in study of Rastegar et al., and the same occurred in our study. In a study by Al-kandari et al., an inverse relationship was reported between age and health-promoting lifestyle [34]. A study by Lim et al., on Korean women showed that there is a significant relationship between marital status and health-promoting lifestyle [35]. This was in agreement with our study. In agreement with our study, Kalroozi et al., reported higher scores on health promotion in married people as compared to the single people [21]. Mainly, higher education level makes clearer the importance of health to people more than before. Norouzinia et al., reported the health-promoting behaviors in students of Alborz University. They stated that education is among factors affecting health behaviors and the mean score of health behaviors in students at higher education levels was significantly higher than in other students [36]. Taiwan adolescents with high health literacy are more likely to perform health-promoting behaviors [37]. Households and employees scored significantly higher on health-promoting behaviors than those with other occupations probably due to having sufficient accuracy in housewives or higher education in employees. A significant relationship was also observed between the type of job and following up a health-promoting lifestyle in a study by Torche [38].
Pregnancy is one of the most important periods for mother and baby [39-44]. Health care systems for women, men and children are one of the most important health issues that improve the health of society by managing diseases [45-54]. The lifestyle of the youth living in the capital of Lorestan province regarding the adoption of health-promoting behaviors has a semi-desirable-undesirable status. Major policymakers and community health officials can improve the physical, mental, and social health of youth by formulating educational programs.
Author Contributions
The author declares that there is no conflict of interest regarding the publication of this paper.
References
- Ren XS, Kazis L, Lee A, Rogers W, Pendergrass S. Health status and satisfaction with health care: a longitudinal study among patients served by the Veterans Health Administration. American Journal of Medical Quality, (2001); 16(5): 166-173.
- Lohr KN, Medicare: a strategy for quality assurance. Washington, D.C: National Academy Press; 1990.
- Blumenthal D. Quality of health care, part 1: Quality of care—what is it? New England Journal of Medicine, (1996); 335: 891– 894.
- Tabrizi JS, Qolipour K, Alipour R. Farahbakhsh M. Asqari Jafarabadi M. Haqaei H. The prenatal care quality from the perspective of pregnant women in healthcare centers and stations in Tabriz. 2010. Hospital Quarterly, (2013): 4(12):9-18.
- Alexander GR, Korenbrot CC. The role of prenatal care in preventing low birth weight. The future of children, (1995); 103-120.
- Orvos H, Hoffmann I, Frank I, Katona M, Pál A, et al. The perinatal outcome of pregnancy without prenatal care: A retrospective study in Szeged, Hungary. European Journal of Obstetrics & Gynecology and Reproductive Biology, (2002); 100(2): 171-173.
- Stringer M. Issues in determining and measuring adequacy of prenatal care. Journal of Perinatology, (1998); 18(1): 68-73.
- Briese V, Voigt M, Hermanussen M, Wittwer-Backofen U. Morbid obesity: Pregnancy risks, birth risks and status of the newborn, Comparative Human Biology. UK: Appleton and Lange; 2009.p. 220-29.
- Araban M, Karimi M, Tavousi M, Shamsi M, Rostam Niakan Sh, Khazaeian S. Simbar M. Evaluation of the quality of midwifery care provided to women hospitalized in the maternity ward of selected hospitals in Yazd. Journal of Shahid Beheshti University of Medical Sciences, 2013; 23 (81): 19-26.
- Aemi SZ, Dadgar S, Pourtaghi F, Hoseini Z, Moghadam Z. The effect of exercise program using elastic band in improving the old women's health. Iranian Journal Of Obstetrics, Gynecology And Infertility, (2016); 18(177): 20-25.
- Jafarnejad F, Kazemeini H, Mazloum R, Emami Moghadam Z, Sefidgaran A. Study on the effect of colporrhaphy on women’s sexual function and satisfaction. The Iranian Journal of Obstetrics, Gynecology and Infertility, (2013); 16(59): 14-23.
- Esfandyari Nejad P, Najar S, Afshari P, Yaralizadeh M, Nezamivand Chegini S. Evaluation of pregnant women's satisfaction of presented prenatal care at Ahvaz health care centers. The Iranian Journal of Obstetrics, Gynecology and Infertility, (2016); 19(31): 13-22.
- Faghani Aghoozi M, Amerian M, Mohammadi S, Yazdanpanah A, Azarabadi S. A review of the quality of midwifery care in Iran. Education & Ethic In Nursing, (2020); 9(1): 52-62.
- Masoumi SZ, Shobeiri F, Karimi S, Roshanaei G. The Effect of Delivery Preparation Counselling on the Pregnant Women’s Satisfaction in the Educational-Medical Fatemieh Hospital in Hamadan in 2015. Journal of Sabzevar University of Medical Sciences, (2016); 23(4): 578-589.
- Hakari D, Mohammadzadeh R, Velayati A, Zareie S. A survey of prenatal care quality in Tabriz therapeutic-health centers. Woman and Study of Family, (2012); 5(18): 157-178.
- Geng X, Wang X, Zhou G, Li F, Li Y, et al. A randomized controlled trial of psychological intervention to improve satisfaction for patients with depression undergoing TKA: a 2-year follow-up. The Journal of Bone and Joint Surgery, (2021); 103(7): 567-574.
- Jin H, Lin W, Lu L, Cui M. Conventional thyroidectomy vs thyroid thermal ablation on postoperative quality of life and satisfaction for patients with benign thyroid nodules. European Journal of Endocrinology, (2021); 184(1): 131-141.
- Usmani SZ, Mateos M-V, Hungria V, Iida S, Bahlis NJ, et al. Greater treatment satisfaction in patients receiving daratumumab subcutaneous vs. intravenous for relapsed or refractory multiple myeloma: COLUMBA clinical trial results. Journal of Cancer Research and Clinical Oncology, (2021); 147(2): 619-631.
- Khazaie T, Khazaie T, Kianfar S. Health-promoting behavior factors among students of Birjand University of Medical Sciences. Iranian Journal of Health Education and Health Promotion, (2015); 3(2): 125-132.
- Rastegar M, Zendehtalab H, Yavari M, Mazlom S. Health-promoting lifestyle and its related factors among health volunteers Mashhad in 2015. Journal of Torbat Heydariyeh University of Medical Sciences, (2015); 3(3): 55-48.
- Kalroozi F, Pishgooie S, Taheriyan A, Khayat S, Faraz R. Health-promoting behaviours and related factors among nurses in selected military hospitals. Military Caring Sciences, (2015); 1(2); 73-80.
- Wittayapun Y, Tanasirirug V, Butsripoom B, Ekpanyaskul C. Factors affecting healthpromoting behaviours in nursing students of the Faculty of Nursing, Srinakharinwirot University, Thailand. Journal of Public Health, (2010); 40(2): 215-225.
- Asgarshahi M, Mazlomi Mahmoudabad S, Fazelpour SH. the status of healthpromoting behaviours Teachers. Journal of Yazd University of Medical Sciences. 2013; 21(3): 12-51.
- Modanloo S, Bagheri Nesami M, Khalili R, Araghiyan F, Ismaili M. Survey of relationship between public health and demographic factors associated with in nurses. 2nd Global Conference on Health Promotion Strategies and Challenges 2011:70 .
- Raiyat A, Nourani N, Samiei Siboni F, Sadeghi T, Alimoradi Z. Health improving behaviors in students of Qazvin secondary schools. Journal of Health and Hygiene, (2012); 3(3): 46-51.
- Fathi Y, Barati M, Ramhormozi SM, Ranaei A, Ayobi E. Assessment of health promoting behaviors and its relation to general self-efficacy among college students in Hamadan. [MSc Thesis]. Hamadan University of Medical Sciences and Health Services. 2009.
- Quintiliani L, Allen J, Marino M, KellyWeeder S, Li Y. Multiple health behavior clusters Among female college students. Patient Education and Counseling, (2010); 79 (1): 134–7.
- Moieni B,dashti S, Teymoori P, Kafami V, Mousali AA, Sharifi M, Akbarzade M, Maleki H. Survey the Health-promoting behaviors among high school students in Hamadan in 2013. Pajouhan Scientific Journal, (2015); 13(3): 49-57.
- Allahverdipour H, Bazargan M, Farhadinasab A, Moeini B. Correlates of video games playing among adolescents in an Islamic country. BMC Public Health, (2010); 10(3): 28-36.
- Hakim A, Khashei N, Latifi SM, DarrehGhaedi F. Evaluation of Daily Physical Activity in Adolescents of 14-20 Years Old in Ahvaz in 2016. Journal of Pediatric Nursing, (2017); 3(3): 1-8.
- Abdolkarimy M, Zareipour M, Mahmoodi H, Dashti S, Faryabi R, et al. Health promoting behaviors and their relationship with self-efficacy of health workers. Iran Journal of Nursing, (2017); 30(105): 68-79.
- Lee RL, Loke AJ. Health-promoting behaviors and psychosocial well-being of university students in Hong Kong. Public Health Nursing, (2005); 22(3): 209-20.
- Larouche R. Determinants of college students' healthpromoting lifestyles. Clinical excellence for nurse practitioners: the international journal of NPACE, (1998); 2(1): 35-44.
- Al‐Kandari F, Vidal VL, Thomas D. Health‐promoting lifestyle and body mass index among College of Nursing students in Kuwait: A correlational study. Nursing & Health Sciences, (2008); 10(1): 43-50.
- Lim YM, Sung MH, Joo KS. Factors affecting health-promoting behaviors of community-dwelling Korean older women. Journal of gerontological nursing, (2010); 36(10): 42-50.
- Norouzinia R, Aghabarari M, Kohan M, Karimi M. Health promotion behaviors and its correlation with anxiety and some students’ demographic factors of Alborz University of Medical Sciences. Journal of Health Promotion Management, (2013); 2(4): 39-49.
- Chang LC. Health literacy, self‐reported status and health promoting behaviours for adolescents in Taiwan. Journal of Clinical Nursing, (2011); 20(1‐2): 190-196.
- Torche F. Social status and cultural consumption: The case of reading in Chile. poetics, (2007); 35(2-3): 70-92.
- Zanzal Ra'ad Al-dorri A, Ibraheem Salih N, Saleh Khuder H. Serological Detection of Helicobacter pylori Infection in Pregnant Women Related to ABO Blood Group. Archives of Razi Institute, (2022); 77(2): 591-597.
- Shamkhi G, Alkhuzai R, Al-Shukr N. Molecular Genotyping of Chlamydia trachomatis in Iraqi Married Pregnant and Non-Pregnant Women. Archives of Razi Institute, (2022); 77(2): 761-769.
- Leman MA, Claramita M, Rahayu GR. Predicting factors on modeling health behavior: a systematic review. American Journal of Health Behavior, (2021); 45(2): 268-278.
- Rao S, Anthony ML, Chowdhury N, Kathrotia R, Mishra M, et al. Molecular characterization of lung carcinomas: A study on diagnostic, predictive, and prognostic markers using immunohistochemical analysis at a Tertiary Care Center in Uttarakhand, India. Journal of Carcinogenesis, (2021); 20: 17.
- Fatemi M, Mohammadi Bavani M, Mohammadi A, Navidpour S, Rafinejad J. A Comparative Morphometric Study on Odontobuthus bidentatus and Odontobuthus doriae (Scorpionida: Buthidae) in Iran. Archives of Razi Institute, (2022); 77(2): 899-905.
- Kodori M, Nikmanesh B, Hakimi H, Ghalavand Z. Antibiotic susceptibility and biofilm formation of bacterial isolates derived from pediatric patients with cystic fibrosis from Tehran, Iran. Archives of Razi Institute, (2021); 76(2): 397.
- Naeimipour F, Rezaie S, Bayat M. Subtilisin Gene Activity in Dermatophytes: A study on the Presence of the Subtilisin Gene in Trichophyton verrucosum and Microsporum gypseum in Clinical and Nonclinical Samples in Tehran, Iran. Archives of Razi Institute, (2021); 76(2): 253.
- Babazadeh M, Noormohammadi Z, Esmaelizad M, Goudarzi H. Molecular Identification of Mycoplasma agalactiae in Iran Based on P30 Gene. Archives of Razi Institute, (2021); 76(1): 61.
- Wissmann R, Zhan C, D'Amica K, Prakash S, Xu Y. Modeling the Population Health Impact of ENDS in the US. American Journal of Health Behavior, (2021); 45(3): 588-610.
- Kumar V, Kumar A. Self-reliance in advanced diagnostic imaging for accessible, affordable, and quality health care in India. Journal of Natural Science, Biology and Medicine, (2021); 12(2): 129-129.
- Matuan A, Palutturi S, Arifin M, Daud A, Moedjiono A. Factors Affecting Provision of Basic Immunization for Infants at Popukoba Health Center, Jayawijaya, Papua. Journal of Natural Science, Biology and Medicine, (2021); 12(3).
- Grace SM, Barr-Anderson DJ, Fulkerson JA. Exploring Associations of Household Chaos and Child Health Behaviors in Rural Families. American journal of health behavior, (2022); 46(1): 49-59.
- JaKa MM, Dinh JM, McCann P, Katz AS, Kottke TE, et al. Promoting Fish Consumption Messages: Perspectives of Hmong Women of Childbearing Age. American Journal of Health Behavior, (2021); 45(5): 867-878.
- Jalil AT, Al-Khafaji AHD, Karevskiy A, Dilfy SH, Hanan ZK. Polymerase chain reaction technique for molecular detection of HPV16 infections among women with cervical cancer in Dhi-Qar Province. Materials Today: Proceedings, (2021).
- Jalil AT, Kadhum WR, Faryad Khan MU, Karevskiy A, Hanan ZK, et al. Cancer stages and demographical study of HPV16 in gene L2 isolated from cervical cancer in Dhi-Qar province, Iraq. Applied Nanoscience, (2021); 1-7.
- Soltanbeigi A, Dastyar N, Khajoei Nejad F, Shokri S. Medicinal Herbs Affecting Cancers in Iran and the World. Plant Biotechnololgy Persa, (2022); 4(1): 1-3.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0