

Full Length Research Article
Diagnostic accuracy of Calypte HIV-1 Urine EIA kit in Pakistan
Hasnain Javed1, Laiba NA1,2, Sobia Rizwan1, Warda Fatima2*
Adv. life sci., vol. 9, no. 3, pp. 313-317, October 2022
*– Corresponding Author: Warda Fatima (Email: warda.mmg@pu.edu.pk
Authors' Affiliations
2. Institute of Microbiology and Molecular Genetics, University of the Punjab, Lahore – Pakistan
[Date Received: 07/03/2022; Date Revised: 19/09/2022; Date Published: 31/10/2022]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: HIV is one of the major public health issues of modern world. The elevation in numbers calls for increased and efficient diagnostic testing protocols. A great number of HIV diagnostic tests have been approved and in use in the developed world but developing countries are still lagging in terms of testing HIV. These reasons are the motives behind this study which is aimed at testing the accuracy and use of Calypte HIV-1 Urine EIA in the Pakistani population.
Methods: 516 subjects are included in the study from different HIV centers of Pakistan. The test results of Calypte-HIV-1 Urine EIA were compared with the routinely used 3-kit method.
Results: The results exhibited 100% specificity but low sensitivity (74.67%). However, the positive predictive value and negative predictive value were 100% and 52.94%, respectively. Overall accuracy result for this kit was observed to be 81.40% for Calypte HIV-1 Urine EIA in the selected sample.
Conclusion: Pakistan has a low population prevalence of HIV and keeping in view of the WHO recommended guidelines for HIV testing, the use of Calypte HIV-1 Urine EIA is not ideal in the current scenario. Even though the test can be of great value in high prevalence populations and can be an excellent means of surveillance procedures, it is not as fit to be used in diagnostic settings in the current situation in developing countries.
Keywords: HIV diagnosis; public health; rapid testing; urine ELISA
Introduction![]()
HIV is one of the major public health concerns worldwide in the present day. According to global HIV and AIDS statistics provided by UNAIDS, 37.7 million people were living with HIV in 2020 out of which 1.5 million were newly diagnosed. Whereas the number of people who died from HIV-associated illness was 680 000 with 6.1 million people unaware of their HIV-related illness status [1]. In Pakistan, the prevalence of HIV infection is less than 0.1% of the population but 200,000 individuals were living with HIV in 2020 of which 25,000 were newly infected and 12% individuals were receiving Antiretroviral therapy (ART)ART[1]. As of June 2021, there were 46 912 active cases of AIDS in Pakistan as publicized by the National AIDS Control Program [2]. According to WHO, HIV has claimed the lives of 36.3 million people so far[3]In Pakistan, HIV is so far a “concentrated epidemic” confined to some critical population subgroups: People who inject drugs (PWID), Sex workers [Male (MSW), Female (FSW) and Transgender Sex workers (TGSW)], men involved in homosexual activities, and transgenders. The HIV prevalence observed in these groups is 21%, 3.8%, 3.7%, and 5.5% respectively [4].
There is a plethora of laboratory tests available to screen blood, diagnose infection, and track disease progression in HIV patients. Tests to detect HIV antibodies are divided into two types: screening assays, intended to detect all infected people, are highly sensitive, and confirmatory (supplemental) assays, which identify people who are not infected but have reactive screening test findings, are extremely specific. HIV testing is currently possible by using body fluids like oral fluid, blood, and urine [5]. Presently, diagnosis of HIV is done by serological tests (rapid test, enzyme immunoassays (EIA), agglutination tests, and detection of antiviral antibodies in the specimens by Western Blot), hematological viral load examinations, therapeutic chemistry, genotyping, and PCR [6]. Rapid testing methods are routinely employed for HIV diagnosis however as per recommendations the test results are evaluated by counter testing. Thus, EIA is counter-examined by Western Blot [7].
Usually, the distinctive symptoms of AIDS appear after a certain period; therefore, the patients with HIV remain ignorant of their clinical status [8]. Timely detection of HIV infection requires early awareness. This can help in delaying AIDS progression and avoid risk-behaviors that can lead to this state [5]. A window period exists before sero-conversion which in 95% of cases is of six months [9]. Standard HIV blood tests can detect antibodies 23- 39 days after infection, antigen/antibody tests require 18-45 days, while nucleic acid test (NAT) can tell if one has HIV infection 10-33 days after exposure [10]. The adoption of a third-generation immunoassay for HIV detection has shortened the time between infection and identification of antibodies. Most resource-limited nations are using the two-test system however, three test system is the actual WHO recommendation for countries with low population prevalence. These tests are to be run in chronological order. In addition to this, a parallel testing approach can also be adopted for HIV diagnostics but requires very high precision and skill [7].
In 1996, the first urine-based HIV test was approved in which ELISA is used to identify IgG antibodies to HIV-1 in urine samples [5,11]. HIV IgG ELISA test for urine is a non-intrusive, simple, and cost-efficient technique. The test can be performed at room temperature for longer periods without affecting its accuracy. Urine testing is appropriate for use in clinical and laboratory setting especially in underdeveloped countries. However, the validity of these positive screening tests is dependent on post confirmations with blood tests.
All these stated claims clarify the need to evaluate the use of urine immune assays for HIV diagnosis in Pakistan. The study is purposed at evaluating the sensitivity and specificity of urine immunoassay by making a comparison with the 03-kit method to validate the use of urine immunoassay in the Pakistani population. In addition to this, the research also aims at calculating the accuracy of the technique with Calypte HIV-1 urine EIA for use in this population.
Methods![]()
The study was conducted in Punjab AIDS Control Program-Advanced Diagnostic Laboratory, Primary and Secondary Healthcare Department, Government of the Punjab, Lahore, Pakistan. Study subjects were related to all over Punjab. All subjects were HIV-1 status positive, and some were on treatment. Informed consent was obtained, and pretest counseling was communicated to each patient. Whole blood was collected in sterile vacutainer with K2EDTA (3ml BD vial) and urine sample in sterile medical disposable 30 ml plastic urine container using standard protocols and stored at 2-8oC for further testing.
3-kit HIV Testing
03 HIV Kits were used concurrently for detection of serum IgG to HIV (Alere HIV Combo, Trinity Biotech Uni-GoldTM HIV, BIOLINE SD HIV1/2 3.0). The basic principle of the kits is based on the immune-chromatographic technique in which recombinant proteins represent the immune-dominant regions of the envelope protein of HIV-1 and HIV-2, gp41, gp120, and gp36 respectively are immobilized at the test region of the nitrocellulose strip. These proteins are also linked to colloidal gold and impregnated below the test region of the device. A narrow band of nitrocellulose membrane is also sensitized as a control region.
Urine HIV EIA
According to the manufacturer guidelines, urine samples were analysed for HIV antibodies using a commercially available assay (Calypte Biomedical Corporation, Alameda CA., USA, HIV-1 Urine EIA Cat. No. 40000, 480 tests kit). The Calypte HIV-1 Urine EIA is an enzyme immunoassay that employs a recombinant HIV-1 envelope protein to detect HIV-1 antibodies in human urine against the recombinant gp 160-envelope protein adsorbed into the wells of a micro-well plate. For each test run, appropriate positive and negative controls were included. By comparing the absorbance value of the specimen to a cut-off value- computed by adding the mean absorbance value of the negative calibrators to 0.180, the specimen was found to be reactive or non-reactive. Specificity, sensitivity, and predictive values with 95% confidence intervals (CI) of the urine IgG HIV-1 test kit were calculated using standard statistical techniques.
Results![]()
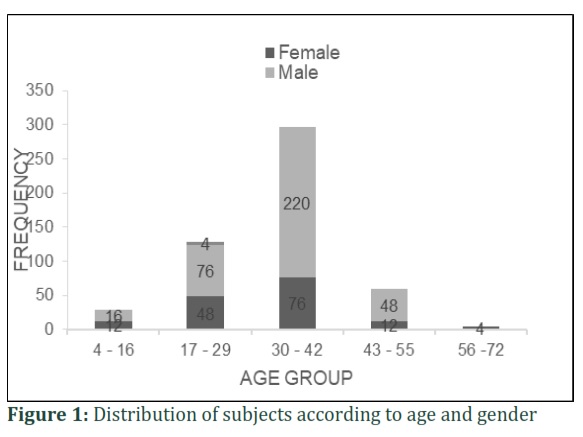
A total of 516 subjects, visiting HIV/AIDS treatment centers located in different districts of Punjab, Pakistan, participated in this study. Out of these 152(29.3%) were females, 360 (69.7%) were males, and 4 (0.77%) were transgender. The average age of subjects was 32.10 years (range 4-67 years) with 296(57.36%) participants belonging to the age group 30- 42 years(Figure 1). 276 (53.4%) were on ART while 240 (46.5%) subjects were treatment-naïve.
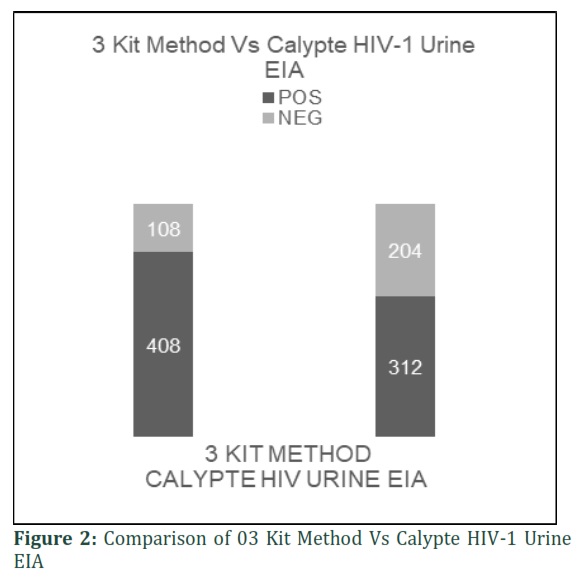
Blood samples of all study participants were evaluated for HIV-1 antibodies using three ELISA kits (based on different principles and antigens) as a gold standard. Overall, 408 subjects tested positive and 108 tested negatives for HIV on these kits. On 03 kit HIV testing method, 276 patient which were on ART treatment showed reactivity against serum IgG antibodies for HIV (100%) and none of them was HIV negative. In case of naïve patients and high risk groups suspected participants, 144 (60%) were determined to be HIV positive, and 96(40%) of participants were non-reactors. On Calypte HIV-1 Urine EIA test, 176 (63.76%) individuals that were on ART tested positive and 100 (36.23%) tested negative. However, among 240 antiretroviral-naïve/ high risk suspected participants HIV patients,132 (55%) and108 (45%) tested positive and negative, respectively.
However, when compared to the gold standard protocol, different results were observed. 312 (60.46%) of the patients tested positive on the Urine Elisa kit whereas 204 (39.53%) showed negative results. As 108 (52.9%) of the 204 individuals tested negative on both the urine Elisa kit and three serum ELISA test kits, they were termed true negatives. 96(47.5%) subjects were classified as false negatives since they only tested negative with the urine Elisa kit (Figure 2).
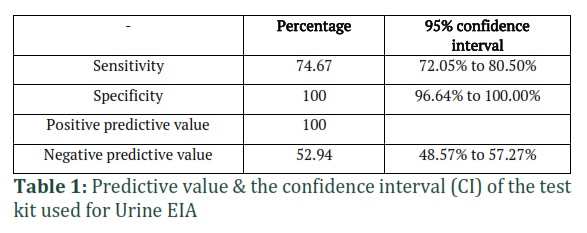
Calypte HIV-1 Urine EIA test was assessed for sensitivity and specificity. The sensitivity value turned out to be 76.47%, while 100% specificity was observed. Likewise, the positive predictive value was also 100%. However, the negative predictive value was 52.94% (95% CI 48.57% – 57.27%) and overall accuracy result for this kit was observed to be 81.40% (Table 1).
Figures & Tables
The elevated need for HIV-specific antibodies has highlighted the importance of diagnostic assays that can be utilized in a variety of settings [12]. The ideal alternative in resource-limited countries is the development of cost-efficient assays with accurate results. The most preferable option is the use of tests that require easily collectible samples while yielding accurate results at the same time [13]. The presence of HIV-specific antibodies in serum or plasma governed the use of these samples for HIV testing for a long time. Alternative non-invasive samples, such as urine or saliva have also been considered. US Food and Drug Administration has approved the use of oral testing devices because the assays have demonstrated excellent accuracy in many studies [14-16]. HIV testing employs specific antigens that are usually obtained from lysates in purified form, synthetic peptides, or recombinant technology. Sensitivity and specificity result due to these antigens. Because of their relatively easy technique, inherent high sensitivity, and suitability for testing large quantities of samples, ELISA tests are the most routinely used assays to screen for HIV infection [12]. Antibody titer or antibody avidity-based methodologies have been developed to identify newly infected people from those who have been infected for a long time [5,17].
In 1998, HIV testing from urine was first proposed. It was proposed due to the considerable benefits over other testing methods since urine is easy to collect, poses less risk of HIV transmission, better compliance, and reduced costs as compared to serum [18]. In many recent studies, Urine immunoassays have proved many benefits. The success of the method lies in its ease of use and safe disposal of the materials involved. The sample collection of urine analysis does not require specialized personnel and adds to the existing benefits of using the method. A study has elucidated the ability of this technique for the detection of HIV-1 despite the non-appearance of HIV-1 p24 antigen. Sensitivity and specificity testing of urine immunoassays have also exhibited promising results. However, this is not always the case as some studies have also reported weak results. Thus, the need is to use the urine immunoassays in a specific population after close evaluation of its validity testing in that particular population [7]. In 1996, the US Food and Drug Administration approved the Calypte Urine HIV-1 enzyme immunoassay (EIA) (Calypte Biomedical Corporation, Berkeley, CA, USA) for the detection of HIV-1 antibodies in urine, as well as the one-band gp160 WB confirmation test in 1998. Even though these tests are routinely used for screening in the United States [19], none of the currently available urine-based assays have been employed for epidemiological reasons in resource-limited countries. IgG antibody concentration in urine is about 1mg/L that is why fairly sensitive techniques are required to detect antibodies against HIV-1 in urine. To date, urine sample testing has relied on ELISA and Western blot techniques, although attempts are being undertaken to create simple/quick procedures for the detection of HIV antibodies in urine specimens [20].
The goal of this study was to see if this commercial urine-based test might be used as a screening tool for HIV infection in Pakistani populations at risk. It was observed that the concentration of antibodies is substantially low as compared to serum. Other factors may alter antibody concentrations in urine samples, causing a sample to be nonreactive to the screening and confirmation techniques utilized in the study, even though the sample was obtained from an HIV-positive individual. Urine collection after a very short period of the last urination can lead to false-negative results since it takes time for antibody levels to return to normal set point. Also, the intake of anti-diuretic, liquids in large amounts, and immuno-compromised status of an individual consequence into varied quantity of antibodies; hence, false-negative test results [13,19,21].
Although collecting urine samples is simple, sample processing necessitates the use of qualified personnel because urine ELISA is a sophisticated technique. Furthermore, in developing countries, urine collection facilities may not be accessible easily. Urine analysis also cannot be used for testing of subjects from remote sites due to the shorter shelf life of the sample. In Pakistan, HIV testing is still a centralized system and individuals from remote sites have no access to HIV testing facilities. This necessitates the use of specialized personnel for sample collection from those areas. Thus, the use of urine for testing those subjects will not serve any purpose with a centralized testing facility.
There have been a large number of studies that have elucidated good sensitivity and specificity of Calypte-HIV-1 testing. However, all these studies were set in high prevalence populations. Pakistan has an HIV population prevalence of less than 0.1% and does not fall under the recommended criteria of using urine-based assays [22]. In addition to these, all these studies have recommended the use of urine-based assays in epidemiological settings instead of diagnostic ones [20].
The comparison of Calypte HIV-1 urine enzyme immune assay with the 3-kit method yielded uneven results in our study. On one hand, high specificity was observed whereas sensitivity was considerably low. Same was the case with positive predictive value and negative predictive value where the latter was much lower than the former.
In our results, the urine ELISA kit correctly identified all the subjects without the disease i.e., excellent specificity was observed. It was 100% with 95% CI. These results were on par with the results of a similar kind of past study [23]. Positive predictive value (PPV) obtained in this research i.e., 100% with a confidence interval of 95% was also per previous investigations. WHO guidelines for diagnostic assays to be used in the developing world suggest a high sensitivity and specificity. Even though our test results yielded a high specificity, the outcome of low sensitivity makes these assays rather doubtful in our population settings [24]. Additionally, other studies have also discouraged the use of HIV-1 EIAs to be used as single confirmatory assays where low specificities were observed [25]. Thus, the results in our study, WHO recommendations, and previous studies are all suggestive of not using only this kit in these particular settings for diagnostic purposes.
The dire need for quick, efficient, and reliable testing protocols for HIV diagnosis demands increased research on the subject. Developing countries face many issues of limited resources and compromised health infrastructure; therefore, the use of any testing means should be in accordance with the set standards. Even though Calypte-HIV-1 Urine EIA is an ideal alternative of invasive techniques in high prevalence regions, its use in developing countries should be carefully analyzed. The research aimed at examining the test results of Calypte HIV-1 Urine EIA by comparison with a routinely used 03-kit method. The low sensitivity of the technique in our results, centralized system of testing, and low prevalence of HIV in the country suggest against the use of technique in daily diagnostic procedures.
![]()
Author Contributions
Laiba NA: Write the manuscript and Data Collection
Sobia Rizwan: Perform testing and arrangement of data
Warda Fatima: Data analysis and Proof read Manuscript.
![]()
The authors declare that there is no conflict of interest regarding the publication of this paper.
![]()
References
- UNAIDS (2021) Country factsheets, PAKISTAN 2020, HIV and AIDS Estimates
- NACP. Current Statistics (2021).
- WHO. HIV/AIDS (2021).
- UNAIDS. Global HIV & AIDS statistics — Fact sheet. (2021).
- Sahni A, Nagendra A, Roy P, Patrikar S. Usefulness of enzyme immunoassay (EIA) for screening of anti HIV antibodies in urinary specimens: a comparative analysis. medical journal armed forces india, (2014); 70(3): 211-214.
- Bystryak S, Bandwar RP, Ossina N. A pilot study to assess the performance of a rapid ultrasound particle agglutination method for the detection of HIV antibodies. Journal of Immunoassay and Immunochemistry, (2021); 17(9): 1-16.
- Alemnji G, Nkengasong JN, Parekh BS. HIV testing in developing countries: what is required? The Indian journal of medical research, (2011); 134(6): 779.
- Liblik K, Byun J, Saldarriaga C, Mendoza I, Baranchuk A (2022) HIV & Heart. Neglected Tropical Diseases and other Infectious Diseases affecting the Heart: Elsevier, (2016); 9(6): 125-136.
- Hovaguimian F, Günthard HF, Hauser C, Conen A, Bernasconi E, et al. Data linkage to evaluate the long-term risk of HIV infection in individuals seeking post-exposure prophylaxis. Nature communications, (2021); 12(1): 1-8.
- CDC (2021) Types of HIV Tests. Centers for Disease Control and Prevention.
- Hilton C, Sabundayo BP, Langan SJ, Hilton M, Henson C, et al. Screening for HIV infection in high-risk communities by urine antibody testing. Journal of acquired immune deficiency syndromes (1999), (2002); 31(4): 416-421.
- Bhatta M, Banerjee S, Nandi S, Dutta S, Saha MK. Performance of commercially available HIV in vitro diagnostic assays: A systematic review and meta-analysis. Journal of Clinical Virology, (2022); 146105047.
- Martinez P, de Lejarazu RO, Eiros J, De Benito J, Rodriguez-Torres A. Urine samples as a possible alternative to serum for human immunodeficiency virus antibody screening. European Journal of Clinical Microbiology and Infectious Diseases, (1996); 15(10): 810-813.
- Chamnanput J, Phanuphak P. Comparison of eight commercial test kits for detecting anti-HIV antibodies in saliva specimens. AIDS, (1993); 7(7): 1026.
- Frerichs RR, Htoon MT, Eskes N, Lwin S. Comparison of saliva and serum for HIV surveillance in developing countries. The Lancet, (1992); 340(8834-8835): 1496-1499.
- Jayashree S, Bhan M, Kumar R, Raj P, Glass R, et al. Serum and salivary antibodies as indicators of rotavirus infection in neonates. The Journal of infectious diseases, (1988); 158(5): 1117-1120.
- McFarland W, Kellogg TA, Louie B, Murrill C, Katz MH. Low estimates of HIV seroconversions among clients of a drug treatment clinic in San Francisco, 1995 to 1998. Journal of acquired immune deficiency syndromes (2000); 23(5): 426-429.
- Carducci A, Casini B, Morleo F, Giuntini A, Parenti M, et al. Comparison of three assays for HIV antibodies detection in urineto be applied to epidemiological setting. European journal of epidemiology, (1999); 15(6): 545-548.
- Urnovitz HB, Sturge JC, Gottfried TD, Murphy WH (1999) Urine antibody tests: new insights into the dynamics of HIV-1 infection. Oxford University Press.
- Feng G-j, Zheng C-q, Yu J, Yang L, Sun H, et al. Clinical Use of the Calypte~(TM) HIV-1 Urine EIA-PRC. Journal of Medern Laboratory Medicine, (2003).
- Connell J, Parry J, Mortimer P, Duncan R, McLean K, et al. Preliminary report: accurate assays for anti-HIV in urine. The lancet, (1990); 335(8702): 1366-1369.
- Taye B, Woldeamanuel Y, Kebede E. Diagnostic detection of human immunodeficincy virus type-1 antibodies in urine, Jimma Hospital, south west Ethiopa. Ethiopian Medical Journal, (2006); 44(4): 363-368.
- Almeda J, Casabona J, Matas L, González V, Muga R, et al. Evaluation of a commercial enzyme immunoassay for HIV screening in urine. European Journal of Clinical Microbiology and Infectious Diseases, (2004); 23(11): 831-835.
- Organization WH. HIV assays: operational characteristics (Phase 1). Report 15, Antigen/antibody ELISAs. (2004).
- Oelemann WM, Lowndes CM, Veríssimo da Costa GC, Morgado MG, Castello-Branco LRR, et al. Diagnostic detection of human immunodeficiency virus type 1 antibodies in urine: a brazilian study. Journal of Clinical Microbiology, (2002); 40(3): 881-885.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0