

Full Length Research Article
Serum Interleukin-17 and its Correlation with Anti-CCP antibodies, Vitamin D3, and Obesity in Rheumatoid Arthritis women Patients
Raghda Rafiq Qadir, Bushra Hussain Shnawa*
Adv. life sci., vol. 9, no. 3, pp. 347-355, October 2022
*– Corresponding Author: Bushra Hussain Shnawa (Email: Bushra.shnawa@soran.edu.iq)
Authors' Affiliations
[Date Received: 28/08/2022; Date Revised: 04/10/2022; Date Published: 31/10/2022]
Editor's Note: Metadata of this publication modified on 20 April 2023.
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease. Members of the IL-17 cytokine family have various biological functions, including enhancing defense against multiple pathogens while promoting inflammatory pathology during autoimmune disease. Additionally, it has been suggested that vitamin D may be connected to the etiology of RA. Therefore, this study aimed to assess serum IL-17 and vitamin D3 concentrations in RA women and determine how these levels relate to anti-CCP, obesity, and age.
Methods: This work included eighty women aged between (22-60) years. Sixty were afflicted with RA and attended the department of rheumatology and medical rehabilitation centre for rheumatic diseases at Rzgary teaching hospital-Erbil, Iraq, compared to twenty healthy women. The concentrations of Anti-CCP antibodies as a diagnostic test, Vitamin D3 and IL-17, were assessed by ELISA. The Mann-Whitney U test and normality were applied for the statistical analysis of the results. Also, the relationship between the study parameters was examined using Pearson's correlation. The ideal cutoff value for IL-17 with the highest sensitivity and specificity was detected using a Receiver Operating Characteristic (ROC) Curve.
Results: This study revealed that serum IL-17 levels were significantly higher in RA women than in the control group (p < 0.001) and that serum VD3 levels were significantly lower in RA women than in healthy controls. Seropositive anti-CCP Ab was found in about 42% of RA patients. The pro-inflammatory IL-17 serum level was positively correlated with vitamin D, age, and obesity in RA women. The best IL-17 cutoff for predicting the presence of RA was 69.5 pg/ML, with a sensitivity of 96% and a specificity of 75%.
Conclusion: In patients with RA, vitamin D deficiency was common and correlated with age. Consequently, a high level of suspicion is needed when assessing at-risk patients, particularly women who complain of vitamin D deficiency.
Keywords: Rheumatoid arthritis; Interleukin-17; Vitamin D3; Anti-CCP; Obesity; Women
Introduction![]()
Guo et al. [1] stated that rheumatoid arthritis (RA) is a chronic systemic autoimmune joint condition that mainly affects the lining of synovial joints and is linked to socioeconomic issues, premature death, and progressive disability. Additionally, it is categorized as an erosive disease that causes joint deformity and the loss of physiological functions [2]. RA disease affects around 1% of the population, with a women-to-men ratio of about 2.5–1. According to Smolen et al. [3], RA is more common in older people and primarily affects women between the ages of 40 and 60. Several risk factors, including a family history of RA or other autoimmune diseases, smoking, environmental factors, ageing, and viral infections, are linked to an increased risk for RA [4,5].
Along with the production of autoantibodies, which harms the synovial membrane and joints, a strong inflammatory immune response causes RA to develop. Activation of inflammation increases cytokines, chemokines, and inflammatory reactants such as C-reactive protein (CRP). Also, an increase in inflammation causes a series of immune responses. Consequently, autoantibodies are overproduced, elevating immunoglobulin M (RF) and anti-CCP. Hence, CRP, RF, and anti-CCP represent RA's inflammatory and immune response products and are known diagnostic blood biomarkers [6-9]. The global prevalence of RA from 1980 to 2019 reached 460 per 100,000 people, with differences according to geographical site and study approach [10]. Based on the production of antibodies to rheumatoid factor and citrullinated protein antigens (ACPA), rheumatoid arthritis patients can be classified into two types. Approximately two-thirds of RA patients are seropositive for the antibody, and these individuals typically exhibit more severe symptoms. ACPAs and RF are frequently found in the blood long before any indications of joint inflammation, suggesting that autoimmunity triggering may happen somewhere other than the joints, for instance, in the lung [11]. Numerous immunomodulatory molecules, mostly cytokines produced by the immune cells, facilitate RA’s pathogenesis, resulting in disease treatment and management complications. Even though the exact aetiology of RA is still unknown, current publications indicate that T-helper cells (Th17) may have a crucial role in its pathogenesis. IL-17 is a cytokine produced by Th17 cells and may also have a considerable role in the development of RA [12]. (TH17) is a group of CD4+ effector T cells dissimilar to TH1 and TH2 cells due to their capability to produce interleukin IL-17. Some human autoimmune diseases, primarily TH1- or TH17-mediated, such as rheumatoid arthritis and psoriasis, have been linked to the pathogenic effects of TH17 lymphocytes. Scientific facts suggest that TH1 and TH17 cells are shared in the pathogenesis of RA [13]. The high expression of IL-10 in colorectal cancer patients’ sera proves its usefulness for detecting patients’ prognoses [14].
Vitamin D is a significant endocrine mediator with immunomodulatory characteristics. In the last 20 years, it has been found to have a close relationship with immune responses. It is understood that vitamin D possesses a pleiotropic anti-inflammatory action and directly contributes to the expression of vitamin D receptors on various immune cells. This conclusion, along with the discovery that low vitamin D levels and vitamin D deficiency are frequent in RA patients, proposes that vitamin D can act as a preventative factor against the disease [15-17]. Vitamin D possesses an immunomodulatory and anti-inflammatory role, and its deficiency has been correlated with many autoimmune syndromes, including RA. Its deficiency is more prevalent in RA patients and may be one of the reasons for the disease’s development [18].
This work aimed to evaluate the serum levels of IL-17 and Vitamin D3 in RA-affected women and explore their relationships with anti-CCP, obesity, and patient age in Iraqi RA women. This study is the first investigation on IL-17 levels in female RA patients in Kurdistan, Iraq.
Methods![]()
Study Subject
Female rheumatoid arthritis patients aged between (22-60 years) were eligible for this study compared to the age and sex-matching healthy control women.
Samples selection and collection
Peripheral blood samples were taken from sixty post-diagnosed female patients afflicted with RA and attending the rheumatology department and medical rehabilitation center of biological therapy for the rheumatic disease at Rzgary teaching hospital-Erbil from November 2021 to January 2022. Associated hospital staff, a rheumatologist, and patient permission were obtained before sample collection, and the patient signed a consent form. For healthy controls, peripheral blood samples from twenty age and sex-matching individuals were randomly selected from healthy women. Three ml of peripheral blood was drawn from patients and healthy controls and put in a serum separation tube (gel tube). After allowing the blood specimens to clot for 30 minutes at room temperature, the sera were separated by centrifuging the samples for 15 minutes at 3000 rpm [19]. Three aliquots of serum were prepared for each sample by transferring 0.7 mL of serum into 1.5 mL Eppendorf tubes. The serum samples were kept at -20°C till further analysis. Enzyme-linked immunosorbent assay (ELISA) was used to detect anti-CCP, interleukin -17, and vitamin D3 in the sera of RA patients as well as healthy control (HC) groups. To confirm their diagnosis, all participants completed a questionnaire about their health status. The questionnaire asked about age, BMI, drug type, time since diagnosis of the disease, and family history.
Estimation of serum cyclic citrullinated peptide IgG antibody (CCPA)
The serum level of IgG antibodies to specific cyclic citrullinated peptides was measured by ELISA (DIAGNOSTIC AESKULIZA CCP, REF 3166, 55234 Wendelsheim- Germany55234) following the manufacturer's instructions. The ELISA standard curve was created to estimate the tested sample by plotting the OD values on the Y-axis and calibration concentrations (U/ml) on the X-axis.
Estimation of Vitamin D3
The serum level of human Vitamin D3 was assessed by the Human Vitamin D Direct AccuBind ELISA kit (Monobind Inc, Lake Forest, CA 92630, USA, product code: 9425-300) based on the competitive ELISA method following the kit's manufacturer's instructions. The ELISA standard curve was drawn by plotting the OD values on the Y-axis and calibration concentrations(pg/ml) on the X-axis to calculate the VD3 concentration of tested samples using EXCEL 2016.
Estimation of Interleukin-17
The serum level of interleukin 17 (IL-17) in the study subjects was estimated by ELISA. A human IL-17 ELISA Kit was used based on the Sandwich method (SUN LONG BIOTECH/CHINA, Catalogue number: SL0978Hu) following the directions provided by the kit's manufacturer. The ELISA standard curve was drawn by plotting the OD values on the Y-axis and calibration concentrations(pg/ml) on the X-axis to assess the concentration of tested samples.
Statistical Analysis
The initial normality and non-parametric test (Mann-Whitney U test) were performed to analyze the data statistically. Pearson's correlation was applied to determine the tested parameters' correlation. The receiver operating characteristic (ROC) curve was established. The area under the curve (AUC) was evaluated to compare the diagnostic efficacy of each value to predict the presence of RA. All statistics and graphics were created using Excel 2016 and the GraphPad Prism 8.05 program.
Results![]()
Study subject demography and clinical characteristics
Demographic and clinical data, including age, Body Mass Index (BMI), family history of patients, and patient treatment usage, were presented in Table1. The findings revealed that the mean age for the RA and HC groups was 47.27 ± 1.187 and 44.15±2.27, respectively. The distribution of age among RA patients showed that (41.7%) of RA patients were within the third group (42-51 years), which had the highest number, including 25 RA women, followed by the fourth group (52-61) with 21 patients, whereas a low number of patients were observed in the first group (22-31 years), including 3 (5%) patients.
The present outcomes demonstrated that 45.0% (27) of RA women were within the normal weight category, including (18.5-24.9), as well as 36% of RA patients, which included (22) were overweight compared to the healthy control group, where the majority of them tended to be normal weight. A person's BMI was determined using the equation (BMI = kg /m2), where kg is their weight in kilograms and m2 is their height in meters squared. The duration of the disease in patients was 12 ± 216 years and ranged between ( 1-39) years.
The present study showed that 51.7% (31) of RA patients had a family history of the disease, while 48.3% (29) of RA patients showed no family history of RA disease. Also, 51.7% (31) of RA patients have a family history of the disease, while 48.3% (29) do not. Patients with first-degree relatives with RA (mother, sister, or brother) made up 46.7% of the total (28), while patients with second-degree relatives (grandparents, aunts, and uncles) with RA made up only 5% of the total (3).
According to their doctor's diagnosis and tests, 45% (27 RA patients out of 60) of the study's RA women took vitamin D3 due to vitamin D deficiency. While 33 RA patients, or 55% of the study's patients, did not receive vitamin D3. Moreover, present results revealed that 68.3% (45) of RA patients took biological therapy while 31.7% (19) did not. As well as the majority of RA patients, 86.7% (52) received Anti-Rheumatoid drugs, while only 13.3% (8) did not. Biological therapy was an Enbrel injection. Physicians also recommended antirheumatic medications, such as methotrexate and hydroxychloroquine, as Disease-Modifying Antirheumatic Drugs (DMARD).
Serological study
For the serological study, sixty RA female patients and twenty HC were enrolled to estimate the serum Anti-CCP level, serum Vitamin D3, and IL- 17 (table 1).
Estimation of cyclic citrullinated peptide antibody IgG (Anti-CCP)
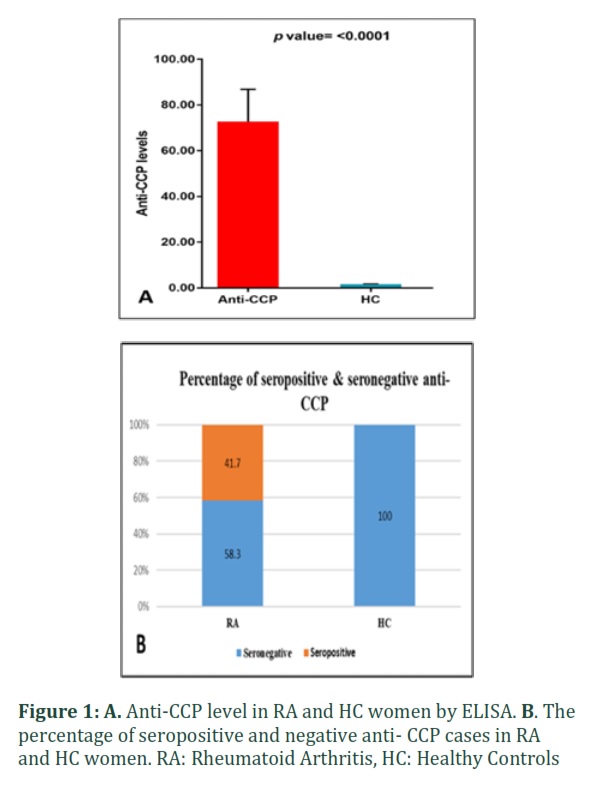
As shown in Figure 1, A, the current findings showed that Anti-CCP levels were significantly higher in the RA group compared to the HC group (p< 00001), means and ranges were 72.77 ± 14.08 (0.9768- 320.2) and 1.629 ± 0.1440 (0.9819- 3.421) pg/ml, respectively). The mean CCP level in the -ve cases was 2.719 ± 0.3276 U/ml. The study results of the seropositivity and sero-negativity of RA women concerning CCP levels revealed that 41.7% of RA patients were positive for CCP, and the mean level was 170.9 ± 21.94 U/ml, leaving 58.3% of RA patients as negative cases. The mean concentration for HC was 1.629 ± 0.144 U/ml, and all samples tested negative for CCP, which is 100%, as shown in Figure1 B.
Estimation of serum Vitamin D3 concentrations in RA patients
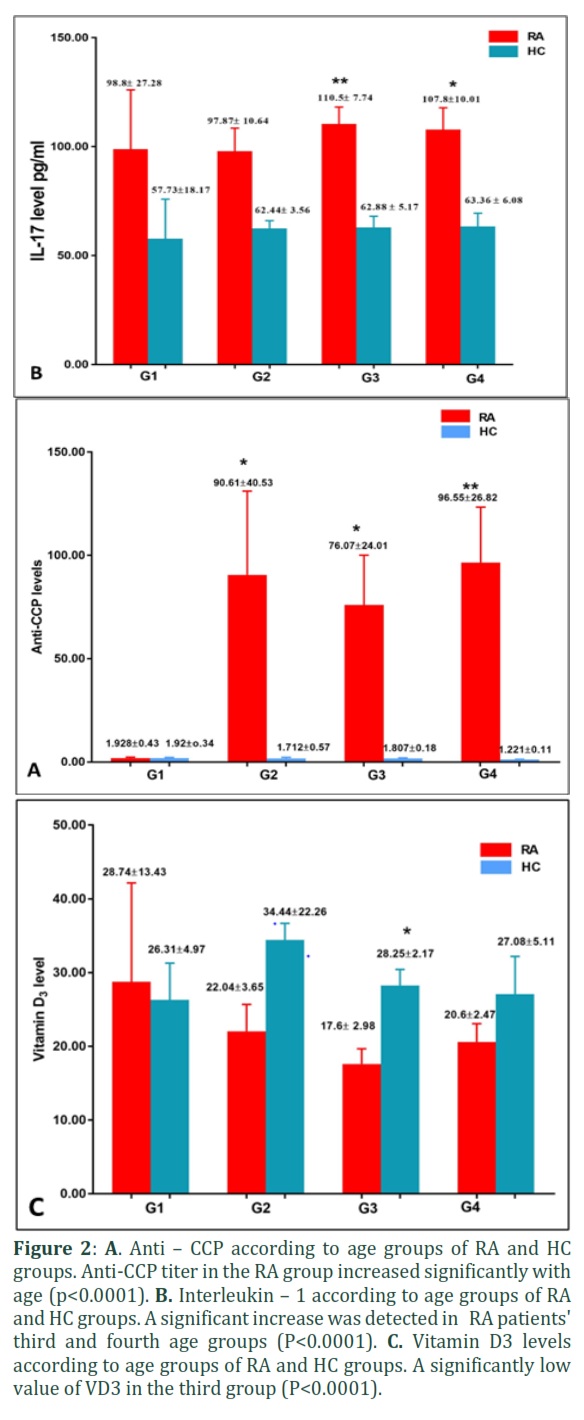
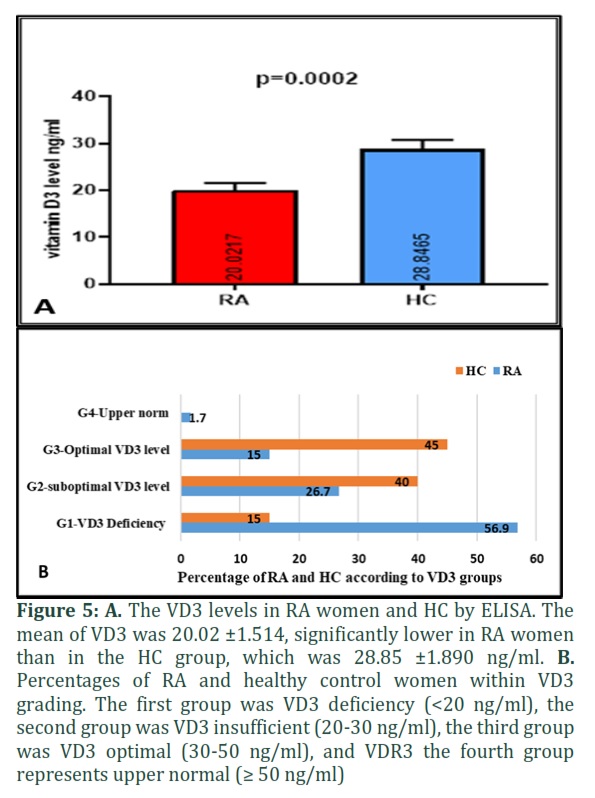
The present results demonstrated that the level of vitamin D3 was significantly decreased (p =0.0002) in RA women compared to HC. The means and range were 20.02 ±1.514 ng/ml (2.304-54.84 ng/ml) and 28.85 ±1.890 ng/ml (3.113 -39.54ng/ml) ng/ml, respectively. Furthermore, the Vitamin D3 levels of study subjects were divided into four groups depending on the kit concentration range. The first group was VD3 deficiency (< 20 ng/ml), the second group was VD3 suboptimal (20-30 ng/ml), the third group was VD3 optimal (30 – 50 ng/ml) and the fourth group of upper normal (≥ 50 ng/ml). Most RA patients suffered from VD3 deficiency (VD group 1), which comprised 56.9% counts 34 of all patients, and the mean VD3 level was 12.10 ± 0.9216 ng/ml. RA patients with suboptimal VD3 levels (VD group 2) included 26.7 %, which counts 16 patients with a VD3 level mean of 24.23±0.7050 ng/ml. 15.0%, which measures nine patients with an optimal level of VD3 (38.57± 2.083 ng/ml), and finally, just one of them (1.7 %) had an overdose of VD3 level with a mean of 54.84 ± 0.000. In healthy control, about half of the HC individuals who were 45% counted nine in the third group with a VD3 mean of 35.29 ± 1.136 ng/ml, while 40 % of those who counted eight had a suboptimal level of VD3 (27.23±0.5558 ng/ml). Only 15% of HC had VD3 deficiency levels with a mean of (13.80± 5.368 ng/ml). In contrast to the other age groups, the third group of RA women displayed a low significant value of V D3 (P<0.0001).
Serum IL-17 levels in RA and HC subjects
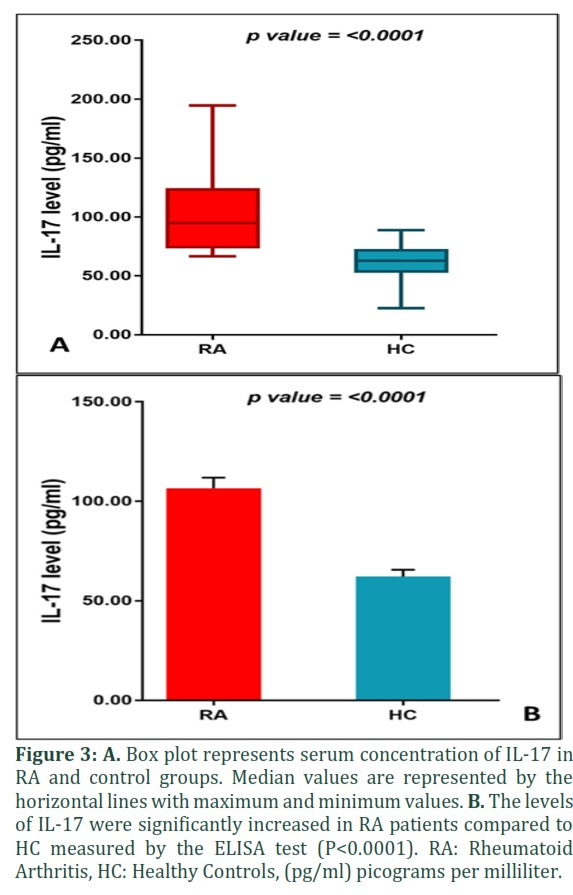
The current findings showed a significant rise in IL-17 levels in the RA group in comparison to HC (p<0.0001). The means and ranges were 106.6 ±5.221 (66.620-194.7) and 62.16 ± 3.419 (22.48-88.80) pg/ml, respectively, as illustrated in Figures 3-A and B. Patients in the third and fourth age groups had levels of Il-17 that were significantly higher than those in other age groups, as shown in Figure 2- B.
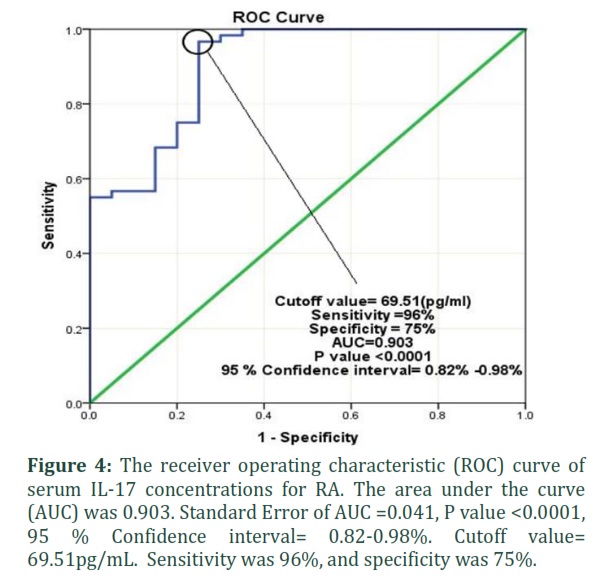
The ROC curve was performed to evaluate the best serum IL-17 cutoff value that can predict a diagnosis of RA. As depicted in Figure 4, the Cutoff value was 69.51 (pg/mL), sensitivity was 96%, and specificity was 75%.
Pearson's correlation between Vitamin D3 level and age groups
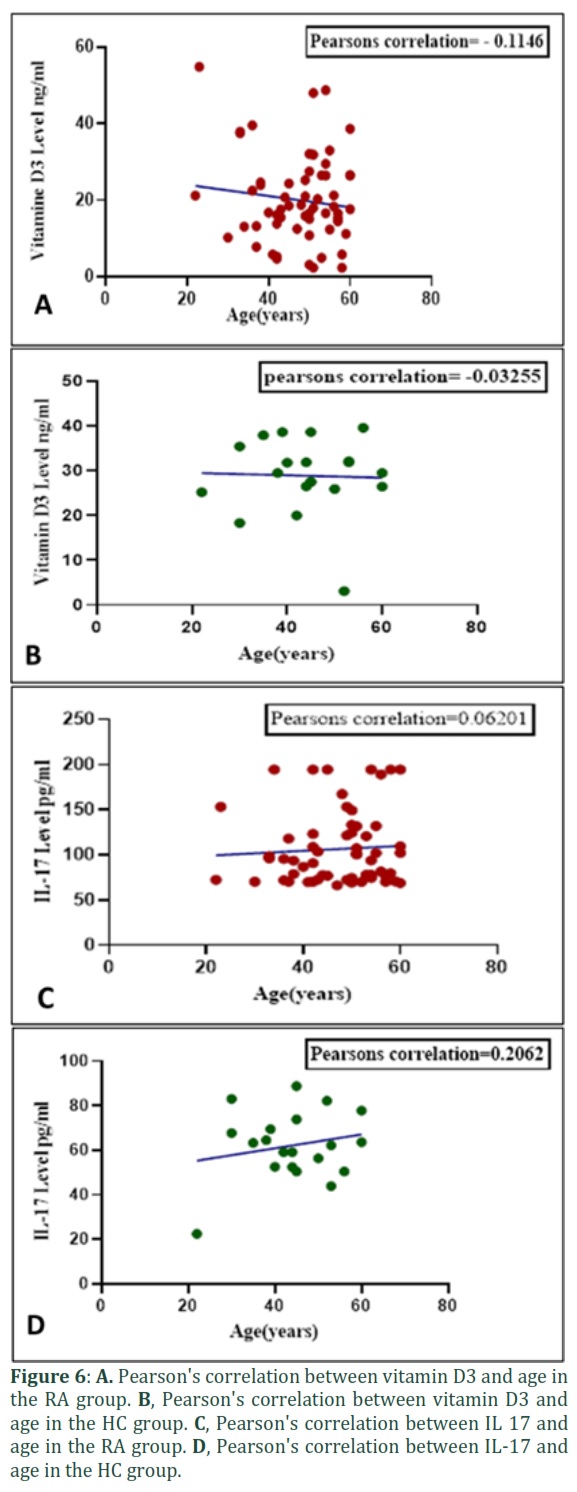
Figures 6- A and B depict the relationship between the age of the RA group and HC and their vitamin D3 levels. A non-significant negative correlation was observed between Vitamin D3 serum levels and the age of RA and HC women. Pearson's correlation was -0.1146 and -0.0325, respectively.
Pearson's correlation between IL-17 levels and age groups
Figures 6- C and D depict the relationships between IL-17 levels, RA patient ages, and HC. A non-significant weak positive association was detected between IL-17 serum levels and ages of RA and HC groups; the Pearson's correlations were 0.062 and 0.206, respectively.
Pearson's correlation between IL-17 levels and Vitamin D3
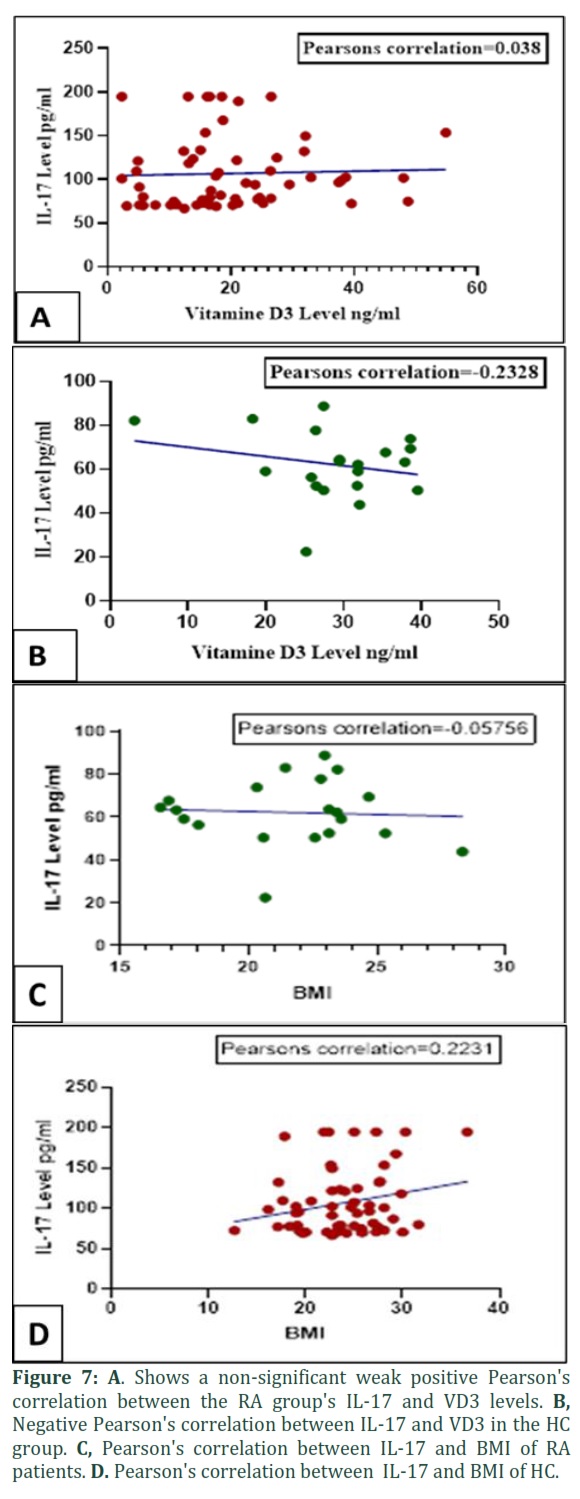
The correlation between the study subject's vitamin D3 level and IL-17 level revealed a non-significant weak positive relationship between these parameters in the RA group, in which Pearson's correlation was 0.038. In contrast, the HC group's Pearson's correlation value was negative – 0.2328 between the two parameters, as shown in Figures 7- A and 7- B. Figure 7- C & D depicts the interaction between the IL-17 concentration and BMI of the RA and HC groups. In the group of RA women, there was a non-significant weak positive association between IL-17 level and BMI. In contrast, a non-significant weak negative relationship in the HC group was found. Pearson's correlation was 0.2231 and – 0.05756, respectively.
Figures & Tables

This study found that in Kurdistan, Iraq, the mean age of female RA patients was 47.27 ± 1.187. Most patients were in the third age group (42-51) and the fourth age group (52-61). This result is consistent with Khadim and Al-Fartusie's finding [20] that RA patients in Iraqi women had a mean age of 48.56. In addition, a recent retrospective study of RA patients in Iraq found that their average age was 48.34 ± 11.7 years (range: 23-95 years) and that they were females (82.7 %). Seventy-six per cent of those patients demonstrated seropositivity for ACCP antibodies [21]. The tendency of rheumatoid arthritis disease to affect older adults is well-described in Iraq. Hussein et al. [22] also found that most patients were between 40 and 59 years old.
The present study showed that 51.7% (31) of RA patients have a family history of this disease, while 48.3% (29) of RA patients showed no family history. Patients with a first-degree relative who had RA represented 46.7% (28) and patients with second-degree relatives with RA comprised only 5% (3). Recently, Gr et al. [23] concluded that higher seropositive of Anti-CCP in RA patients' asymptomatic first-degree relatives (AFDR) might increase the risk of developing RA soon. Therefore, all AFDRs should be screened for early detection, and positive cases must be followed up.
Sera negative and positive Anti- CCP cases were described and mentioned in many studies; according to our findings, 41.7% of RA patients tested positive for anti-CCP, while 58% of RA patients tested negative. Another study mentioned that 81 (70.4%) of the RA samples had anti-CCP antibodies [24]. Previous investigations proved that ACPA-positive individuals experienced more active symptoms during follow-up than ACPA-negative patients [25]. As a result, ACPA was recommended in the 2009 RA diagnostic standards based on the available evidence [26]. Anti-CCP is more sensitive than RF and may detect RA disease earlier in its progression. Since it correlates well with disease activity, anti-CCP should be chosen over RF. However, it is ineffective in controlling the disease’s extra-articular manifestation (EAM) [23]. According to recent studies [21,27,28], (RA patients who are seropositive for RF or anti-CCP antibodies are thought to have more aggressive symptoms than seronegative patients.
Women with RA frequently lack adequate amounts of vitamin D. Our research found that the mean levels of vitamin D3 in RA patients were significantly lower than those in healthy controls; these values were 20.02 ± 1.514 ng/ml and 28.85 ± 1.890 ng/ml, respectively. This study revealed that most RA patients suffered from VD3 deficiency, which includes 56.9% of RA cases. Previously, in research conducted in Erbil, Iraq [29]. They found that 70% of the studied RA cases had Vitamin D3 deficiency. Another study suggested that hypovitaminosis D is a common risk factor for many autoimmune diseases, including RA, because VD3 is responsible for regulating immune response and boosting the immune system, as mentioned [30]. Meena et al. [18] concluded that Vitamin D deficiency is more prevalent in RA patients and may be one of the reasons for developing or worsening symptoms. Women with RA had lower basal serum levels of 25(OH)D than healthy controls, which is consistent with our observations, and also seems to be an environmental risk factor for RA [31]. Similarly, at least in postmenopausal women, vitamin D intake and the risk of RA were negatively correlated [32,33].
Our results showed a significant increase in IL-17 levels in the RA group compared to HC, with a mean of 106.6 ±5.221and 62.16 ± 3.419, respectively. This result agrees with [34,35], Who documented a significant difference between the serum IL-17 levels in the RA patients and the control group. They proposed that serum IL-17 levels might be a key indicator of RA disease activity. Moreover, the present findings point out that the AUC of IL-17 for diagnosing RA was 0.903. The 95% confidence interval of 0.82- 0.98%, with high sensitivity of 96% and specificity of 75%, suggests that the serum levels of IL-17A can potentially be a biomarker for RA.
Similarly, Qu et al. [34] concluded that IL-17 has better sensitivity and specificity than IL-10 for diagnosing RA. In addition, a recent study proved that IL-17A has potential efficiency as a biomarker for disease activity in RA [36]. Rheumatoid arthritis is one autoimmune disease for which IL-17 has been linked to its pathogenesis.
Nevertheless, in vivo and in vitro results depict that IL-17A is one of the causes that spread local inflammation in the synovium, particularly in RA [37]. Suppression of interleukins is beneficial in controlling some diseases. It has been believed that suppression of IL-31 may be a helpful way to treat inflammatory cases [38]. New strategies are required to precisely control IL-17-mediated immunopathology in a chronic autoimmune disorder [39].
This work revealed that serum IL-17 levels were significantly higher in RA women than in the control group (p < 0.001). Vitamin D deficiency was prevalent in RA patients and correlated positively with anti-CCP and inversely with the age. Consequently, a high level of suspicion is needed when assessing at-risk patients, particularly women who complain of vitamin D deficiency. Moreover, IL-17 has good sensitivity and specificity, which helps to raise the diagnostic bar for RA and serves as a guide for the disease's pathogenesis, diagnosis, and treatment. Further studies with more cases of RA and analyzing the IL-17 level in the synovial fluid are needed to validate the study's findings.
Author Contributions
RR Qadir carried out the experimental work and BH Shnawa designed and supervised this study.
![]()
The authors declare that there is no conflict of interest in this work.
![]()
References
- Guo Q, Wang Y, Xu D, Nossent J, Pavlos NJ, et al. Rheumatoid arthritis: pathological mechanisms and modern pharmacologic therapies. Bone research, (2018); 6(1): 1-14.
- Liu J, Gao J, Wu Z, Mi L, Li N, et al. Anti-citrullinated protein antibody generation, pathogenesis, clinical application and prospects. Frontiers in Medicine, (2022); 2853.
- Smolen J, Aletaha D, McInnes I. Therapies for bone R. Lancet, (2016); 30173-30178.
- Bullock J, Rizvi SA, Saleh AM, Ahmed SS, Do DP, et al. Rheumatoid arthritis: a brief overview of the treatment. Medical Principles and Practice, (2018); 27(6): 501-507.
- Smith MH, Berman JR. What Is Rheumatoid Arthritis? JAMA, (2022); 327(12): 1194-1194.
- Choy EH, Panayi GS. Cytokine pathways and joint inflammation in rheumatoid arthritis. New England Journal of Medicine, (2001); 344(12): 907-916.
- Muller S, Radic M. Citrullinated autoantigens: from diagnostic markers to pathogenetic mechanisms. Clinical reviews in allergy & immunology, (2015); 49(2): 232-239.
- Mun S, Lee J, Park A, Kim H-J, Lee Y-J, et al. Proteomics approach for the discovery of rheumatoid arthritis biomarkers using mass spectrometry. International journal of molecular sciences, (2019); 20(18): 4368.
- Mun S, Lee J, Park M, Shin J, Lim M-K, et al. Serum biomarker panel for the diagnosis of rheumatoid arthritis. Arthritis Research & Therapy, (2021); 23(1): 1-10.
- Almutairi K, Nossent J, Preen D, Keen H, Inderjeeth C. The global prevalence of rheumatoid arthritis: a meta-analysis based on a systematic review. Rheumatology international, (2021); 41(5): 863-877.
- Malmström V, Catrina AI, Klareskog L. The immunopathogenesis of seropositive rheumatoid arthritis: from triggering to targeting. Nature Reviews Immunology, (2017); 17(1): 60-75.
- Yap H-Y, Tee SZ-Y, Wong MM-T, Chow S-K, Peh S-C, et al. Pathogenic role of immune cells in rheumatoid arthritis: implications in clinical treatment and biomarker development. Cells, (2018); 7(10): 161.
- Annunziato F, Cosmi L, Liotta F, Maggi E, Romagnani S. Type 17 T helper cells—origins, features and possible roles in rheumatic disease. Nature Reviews Rheumatology, (2009); 5(6): 325-331.
- Hamad RS, Shnawa BH, Al-Ali SJ. Correlation between IL-10 as Cancer Biomarker and Demographic Characteristics of Colorectal Cancer Patients. Pharmaceutical Research International, (2021); 33(26B).
- Jeffery LE, Raza K, Hewison M. Vitamin D in rheumatoid arthritis—towards clinical application. Nature Reviews Rheumatology, (2016); 12(4): 201-210.
- Bragazzi NL, Watad A, Neumann SG, Simon M, Brown SB, et al. Vitamin D and rheumatoid arthritis: an ongoing mystery. Current opinion in rheumatology, (2017); 29(4): 378-388.
- Romão VC, Fonseca JE. Etiology and risk factors for rheumatoid arthritis: a state-of-the-art review. Frontiers in Medicine, (2021); 8.
- Meena N, Chawla SPS, Garg R, Batta A, Kaur S. Assessment of vitamin D in rheumatoid arthritis and its correlation with disease activity. Journal of natural science, biology, and medicine, (2018); 9(1): 54.
- Shani WS, Shnawa B H, Waheda N E. Levels of Immunoglobulins and complements in sera of patients with toxoplasmosis. Basrah Journal of Scienec (B) Vol, (2012); 30(1): 72-77.
- Khadim R, Al-Fartusie F. Evaluation of Liver Function and Lipid profiles in Iraqi patients with Rheumatoid Arthritis; 2021. IOP Publishing. pp. 012040.
- Ridha A, Hussein S, AlJabban A, Gunay LM, Gorial FI, et al. The Clinical Impact of Seropositivity on Treatment Response in Patients with Rheumatoid Arthritis Treated with Etanercept: A Real-World Iraqi Experience. Open Access Rheumatology: Research and Reviews, (2022); 14113.
- Hussein RH, MezherAl-Rayahi IA, Taha K. Rheumatoid factor isotypes in a sample of Iraqi rheumatoid arthritis patients. J Glob Pharma Technol, (2018); 10141-145.
- Gr P, Dihingia P, Jha AK, Gadgade A, Agarwal D. Rheumatoid Arthritis Co-relation with Anti-CCP Antibodies with special reference to its Prevalence in Asymptomatic First-Degree Relatives. Mediterranean Journal of Rheumatology, (2022); 33(1): 42.
- Dhaouadi T, Chahbi M, Haouami Y, Sfar I, Abdelmoula L, et al. IL-17A, IL-17RC polymorphisms and IL17 plasma levels in Tunisian patients with rheumatoid arthritis. PLoS One, (2018); 13(3): e0194883.
- Rönnelid J, Wick MC, Lampa J, Lindblad S, Nordmark B, et al. Longitudinal analysis of citrullinated protein/peptide antibodies (anti-CP) during 5 year follow up in early rheumatoid arthritis: anti-CP status predicts worse disease activity and greater radiological progression. Annals of the rheumatic diseases, (2005); 64(12): 1744-1749.
- Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis & rheumatism, (2010); 62(9): 2569-2581.
- Choi S-T, Lee K-H. Clinical management of seronegative and seropositive rheumatoid arthritis: a comparative study. PLoS One, (2018); 13(4): e0195550.
- Martinez-Prat L, Nissen MJ, Lamacchia C, Bentow C, Cesana L, et al. comparison of serological biomarkers in rheumatoid arthritis and their combination to improve diagnostic performance. Frontiers in immunology, (2018); 91113.
- Hamad BA. Relationship between vitamin D3 level and rheumatoid arthritis patients attending Rizgary Teaching Hospital in Erbil city. Zanco Journal of Medical Sciences (Zanco J Med Sci), (2017); 21(2): 1736-1742.
- Sukharani N, Dev K, Rahul F, Bai P, Ali A, et al. Association between rheumatoid arthritis and serum vitamin D levels. Cureus, (2021); 13(9).
- Harrison SR, Li D, Jeffery LE, Raza K, Hewison M. Vitamin D, autoimmune disease and rheumatoid arthritis. Calcified tissue international, (2020); 106(1): 58-75.
- Merlino LA, Curtis J, Mikuls TR, Cerhan JR, Criswell LA, et al. Vitamin D intake is inversely associated with rheumatoid arthritis: results from the Iowa Women's Health Study. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology, (2004); 50(1): 72-77.
- Dupuis ML, Pagano MT, Pierdominici M, Ortona E. The role of vitamin D in autoimmune diseases: could sex make the difference? Biology of sex differences, (2021); 12(1): 1-12.
- Qu C, Hou Y, Bi Y, Han Q, Jiao C, et al. Diagnostic values of serum IL-10 and IL-17 in rheumatoid arthritis and their correlation with serum 14-3-3η protein. Eur Rev Med Pharmacol Sci, (2019); 23(5): 1899-1906.
- Atwa SE, Azab MM, Mohamed MS. Serum Interleukin-17 Level in Patients with Rheumatoid Arthritis and its Relation to Disease Activity. Zagazig University Medical Journal, (2020); 26(1): 87-93.
- Dissanayake K, Jayasinghe C, Wanigasekara P, Sominanda A. Potential applicability of cytokines as biomarkers of disease activity in rheumatoid arthritis: Enzyme-linked immunosorbent spot assay-based evaluation of TNF-α, IL-1β, IL-10 and IL-17A. PloS one, (2021); 16(1): e0246111.
- Robert M, Miossec P. IL-17 in rheumatoid arthritis and precision medicine: from synovitis expression to circulating bioactive levels. Frontiers in medicine, (2019); 5364.
- Shnawa BH, Al-Ali SJ, Ahmad HF, Essa SA. An Investigative Study of Smoking Effects on IL-31 Levels and Leukocyte differential counts in Humans. Annals of Tropical Medicine and Public Health. (2020); 23(11).
- Mills KH. IL-17 and IL-17-producing cells in protection versus pathology. Nature Reviews Immunology, (2022); 1-17.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0