

Full Length Research Article
Radiographic Evaluation of Knee Joint in Patients with Knee pain and its correlation with Osteoarthritis and Gender
Maryam Shahzad1, Taiba Zulfiqar*1, Abid Ali2
Adv. life sci., vol. 9, no. 3, pp. 309-312, October 2022
*– Corresponding Author: Taiba Zulfiqar (Email: taibazulfiqar1@gmail.com)
Authors' Affiliations
2. Department of Allied Health Sciences, The University of Lahore, Lahore – Pakistan
[Date Received: 21/02/2021; Date Revised: 25/07/2022; Date Published: 31/10/2022]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Osteoarthritis (OA) is the most rampant reason of knee discomfort and pain. Knee osteoarthritis accounts for 83 percent of the overall Osteoarthritis burden. Knee osteoarthritis (KOA) is projected to grow more frequent as age progresses, and it is more common in women and overweight individuals. The Kellgren and Lawrence scoring criteria is usually employed to estimate the severity of disease. To evaluate the Radiographic findings associated with knee joint pain and to assess the prevalence of osteoarthritis in individuals with knee joint discomfort, as well as its correlation with gender.
Methods: From August to December 2021, cross-sectional research was undertaken at the Department of Radiology, Amin Medical Complex, Sialkot. This research comprised participants of both gender having knee discomfort, ranging in age from forty to eighty yrs. SPSS version 24 was employed to record the data and analyze the information.
Results: Total 100 Patients (M=45, F=55) were enrolled in this study. Out of 100 participants with knee pain 45(45%) patients had abnormal knee radiographic findings. Osteoarthritis of the knee accounted for 35% of all abnormal radiographic findings in this study, with synovial effusion accounting for 8% of the total, and erosion only contributing for 2%. Knee osteoarthritis was found to be more prevalent in females than in males (24% vs. 11%), demonstrating that gender is a significant predictor for knee osteoarthritic disease. Findings corroborate the implementation of the Kellgren-Lawrence marking scheme to characterize Knee osteoarthritis in population research.
Conclusion: The findings suggest that radiographic aspects of knee Osteoarthritis are substantially linked to knee discomfort, and that it is more frequent in people over the age of 55. Knee osteoarthritis is substantially linked with gender, with females suffering from it at a higher rate. The findings authenticate the implementation of the Kellgren-Lawrence grading scheme to characterize Knee osteoarthritis in population research.
Keywords: Osteoarthritis; Radiographic aspects of knee osteoarthritis; Aging, Kellgren-Lawrence scoring system
Introduction![]()
Osteoarthritis (OA) seems to be the most frequent sort of arthritis, afflicting almost 250 million individuals across the globe [1]. Osteoarthritis is a degenerative joint ailment characterized by the degradation of basal bone structure and joint cartilage [2]. OA is a widespread joint ailment and the significant contributor of morbidity in the elderly [3]. The knees, feet, hips, facets and hands are the most often afflicted joints by OA, although knee OA contributes for 83% of the entire OA stress.[4]. According to research in Pakistan, knee osteoarthritis affects twenty-eight percent of the urban population and twenty-five percent of the rural population [5]. Around 12% of adults above the age of sixty have symptomatic knee OA [6]. Knee osteoarthritis (OA) is a complex, deteriorative joint disease marked by persistent discomfort and functional impairment [7]. Knee OA, the most prominent category of OA, is the eleventh leading element of worldwide disability and the thirty-eight leading cause of malady-adjusted life yrs[8]. For the assessment of knee OA, the EULAR proposed 3 symptoms i.e persistent knee discomfort, limited joint stiffness, and diminished mobility. Crepitus, joint mobility limitation, and bony hypertrophy are also helpful in the diagnosis of knee OA [9]. Knee OA constitutes about 4th or 5th of all OA cases globally, and its prevalence rises with obesity and age [10]. Obesity is one of the significant warning indicators, producing inflammatory response, discomfort, decreased joint mobility, and a lower quality of life [11]. Knee discomfort and pain is frequently the initial presenting indication of knee OA, and it is typically attributed to OA in people over 55 years of age. In many nations, the condition is projected to grow more widespread as a result of aging and obesity [12]. Walking up and down stairs causes discomfort in the patellofemoral joint, which can be addressed with conservative treatment such as quadriceps strengthening exercises, and rarely, with surgical procedure such as arthroplasty of the patellofemoral joint [13]. According to a comprehensive assessment of the literature, fifteen to seventy-six percent of individuals with knee joint pain had radiographic OA, while fifteen to eighty-one percent of those with radiographic knee Osteoarthritis had pain and discomfort [14]. Currently, joint ache is diagnosed using traditional radiography, which is insensitive and has a number of drawbacks. In individuals suspected of having knee OA, the appearance of osteophytes on all radiographic projections of the knee correctly anticipates the knee pain [15]. The Kellgren and Lawrence classification scale is utilized to determine disease intensity regarding clinical evaluations of joint stiffness, pain and impairments in functional capacity, as well as radiographic examination of osteophytes, osseous sclerosis, and knee joint-space constriction [16].
Methods![]()
This research was undertaken at the Department of Radiology, Amin Medical Complex, Sialkot. The ethical authorization was acquired from the ethical review committee and each participant granted their informed consent. An aggregate of 100 patients were enrolled in this study. Antero-posterior and Lateral radiographs were acquired for the radiographic evaluation of knee pain. Simple random sampling technique was used and on the basis of firsthand observation, data was obtained with the assistance of Radiologist. This research comprised participants of both gender with knee discomfort, ranging in age from forty to eighty yrs. The individuals with specific prior knee joint medical issue (such as, tumors, knee trauma, knee surgery or rheumatoid arthritis) were ruled out from this study. To examine radiographic abnormalities related with knee pain and to estimate the prevalence of OA among participants with knee joint discomfort and its correlation with gender, all patients encountered radiographic examination and x-rays of the knee joint were collected from each patient. The Kellgren-Lawrence and individual characteristics scales were used to evaluate radiographs. Age and gender were also collected as demographic data. In order to calculate the sample size, the convenient approach was employed. All of the information was gathered and entered into a pre-made proforma. SPSS version 24 was utilized to code and analyze the results. The correlation method was utilized to explore relation b/w Gender and knee osteoarthritis (KOA). P-value less than or equal to 0.05 is generally regarded as significant.
Results![]()
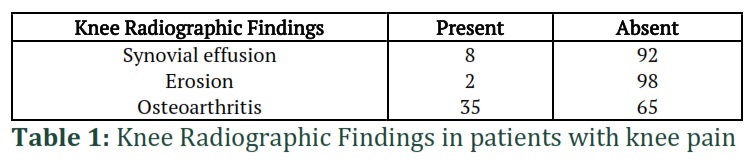
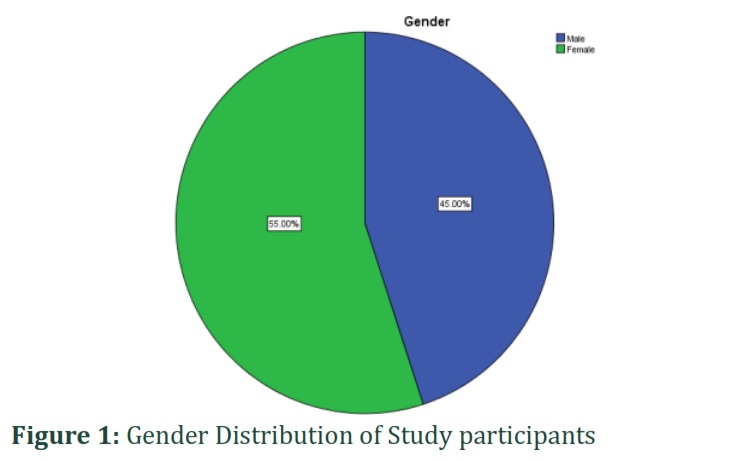
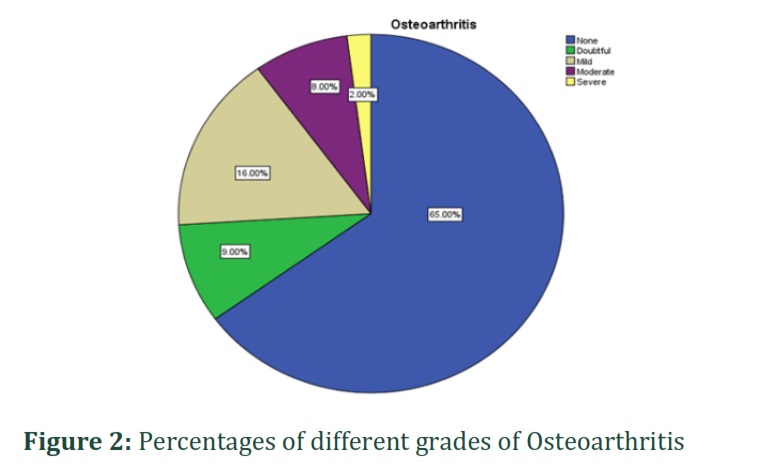
This research comprised a total of hundred participants who had knee pain. Out of 100 patients, 45 (45%) were men and 55 (55%) were women (Figure I). The patients' average age was 58.89 ± 9.675 years. Among 100 participants with knee discomfort, 45 percent of the subjects had aberrant knee radiographic findings, with osteoarthritis accounting for 35%. Synovial effusion accounts for 8% of the total, whereas erosion only contributes for 2% (Table-I). Among the anomalous radiographic findings, the most prevalent was osteoarthritis (OA), which accounted for 35% of all abnormal findings (Figure II).
The findings showed that radiographic characteristics of knee Osteoarthritis are strongly correlated to knee discomfort and pain. The findings also reconfigure the application of Kellgren-Lawrence scoring method to classify knee OA in population studies.
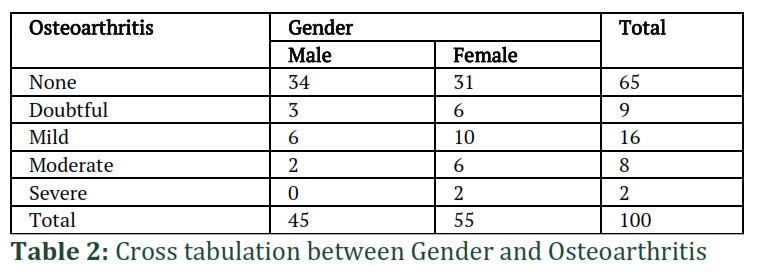
According to the Kellgren-Lawrence grading scale, 65% of the participants have (Grade 0) OA (i.e., no radiographic findings associated with KOA), (Grade 1) accounts for 9% (9 participants have Doubtful OA), (Grade 2) accounts for 16% (16 participants have Mild OA), (Grade 3) accounts for 8% (8 participants have moderate OA), and (Grade 4) accounts for 2% (2 participants have Severe OA), as shown in (Table IV). The severity of knee osteoarthritis increases with advancing age i.e., patients with age greater than 55 have more severe type of osteoarthritis (Table-V).
Figures & Tables
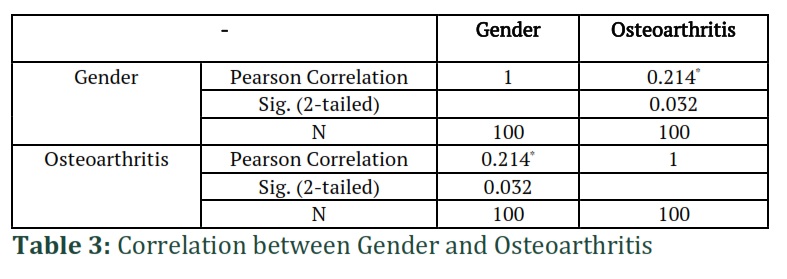


The objective of this study was to determine the radiographic findings linked with knee pain and to examine the occurrence of osteoarthritis in individuals with knee joint pain, as well as its association with gender. The most typical joint malady in the world is osteoarthritis of the knee. The findings show that radiographic aspects of knee OA are strongly linked to knee pain and discomfort. Depending on age, gender distribution, and disease criteria, the approximate population prevalence ranges from four to fifty percent [5, 17-21]. These disparities might be attributed to variances in ethnicity, way of living, or sociodemographic status, and knee osteoarthritis (KOA) affects between 27 to 90 % of those aged 60 years or older in developed nations [22]. The average age of the participants in this study was 58.89 ± 9.675 years which is comparable to the mean age of 56.28 ± 8.786 years reported by Iqbal MN et al in their study [5]. KOA was found to be more frequent in females than in males (24% vs. 11%), designating that gender is a substantial provoking element for knee osteoarthritis (KOA).
This discrepancy might well be explained by scarcity of regular exercise, motility, societal concerns, especially in our location, and a greater obesity rate among women in general. Additional factor for the gender disproportion might be cartilage tissue's vulnerability to sex hormones, as men have larger knee articular volume than women [23]. The increased rate of OA in females shortly after menopause indicates that estrogen insufficiency is a factor in the disease’s development [5, 24]. A Kellgren-Lawrence score of 0 (normal), I (doubtful possible osteophytic lipping and narrowed Knee JS), II (definite osteophytes and possible JS narrowing), III (moderate numerous osteophytes, definite JS narrowing, and some sclerosis and possible malformation of bone ends), or IV (large osteophytes, marked JS narrowing, severe sclerosis, and definite deformity of bone ends) was assigned to each knee. For the purposes of this investigation, the highest grade given to a subject’s radiograph was given to the knee that was more badly afflicted. A KL score of 2 or above indicated the presence of OA in the knee [25]. In this study, 65 % of the subjects exhibited (Grade 0) Osteoarthritis, 9 % had (Grade 1), 16 % experienced (Grade 2), 8 % showed (Grade 3), and 2 % had (Grade 4) OA as per the KL scoring system. Furthermore, Age groups and grades of osteoarthritis are significantly correlated with each other as shown in the Table-V (Chi-Square Tests). The results indicate that radiographic aspects of knee osteoarthritis (OA) are substantially linked to knee discomfort and pain, and that knee pain and discomfort is more frequent in people over 55 years old. Knee osteoarthritis has a strong association to gender, with females having the highest prevalence. The findings also corroborate the implementation of the Kellgren-Lawrence marking scheme to characterize KOA in population research.
![]()
Author Contributions
Maryam made conception and design of data.Taiba accomplished data analysis and interpretation of data,Revising it critically for important intellectual content.
![]()
The authors declare that there is no conflict of interest regarding the publication of this paper.
![]()
References
- Vos T, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet, (2012); 380(9859): 2163-96.
- Sharma L. Osteoarthritis year in review 2015: clinical. Elsevier, (2016); 24(1): 36-48.
- Arden N, et al. Epidemiology of Osteoarthritis: Atlas of Osteroarthritis. 2014; 2:90. Springer Healthcare Tarporley.
- Vos T, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. The lancet, (2012); 380(9859): 2163-2196.
- Iqbal MN, et al. Frequency of factors associated with knee osteoarthritis. JPMA-Journal of the Pakistan Medical Association, (2011); 61(8): 786.
- LawrenceRC, F, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. American College of Rheumatology, (2008); 58(1): 26-35.
- Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. The Lancet, (2019); 393(10182): 1745-1759.
- Cross M et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. British Medical Journal, (2014); 73(7): 1323-1330.
- Zhang W et al. EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis. British Medical Journal, (2010); 69(3): 483-489.
- Reddy KS. Global Burden of Disease Study 2015 provides GPS for global health 2030. The Lancet, (2016); 388(10053): 1448-1449.
- Schell J et al. Strawberries improve pain and inflammation in obese adults with radiographic evidence of knee osteoarthritis. Multidisciplinary Digital Publishing Institute, (2017); 9(9): 949.
- Turkiewicz A et al. Prevalence of knee pain and knee OA in southern Sweden and the proportion that seeks medical care. Oxford Academic Journal, (2015); 54(5): 827-835.
- Wenham, C, A. Grainger, and P. Conaghan. The role of imaging modalities in the diagnosis, differential diagnosis and clinical assessment of peripheral joint osteoarthritis. Elsevier, (2014); 22(10): 1692-1702.
- Bedson J, Croft PR. The discordance between clinical and radiographic knee osteoarthritis: a systematic search and summary of the literature. BioMed Central, (2008); 9(1): 1-11.
- Cicuttini FM, et al., Association of pain with radiological changes in different compartments and views of the knee joint. Elsevier, (1996); 4(2): 143-147.
- Kellgren JH, Lawrence J. Radiological assessment of Rheumatoid Arthritis. National Library of Medicine, (1957); 16(4): 494.
- Zeng Qy, et al. Associated risk factors of knee osteoarthritis: a population survey in Taiyuan, China. Chinese medical journal, (2006); 119(18): 1522-1527.
- Haq SA, et al. Prevalence of rheumatic diseases and associated outcomes in rural and urban communities in Bangladesh: a COPCORD study. The Journal of rheumatology, (2005); 32(2): 348-353.
- Khalid MU, Akhtar M. Frequency of osteoarthritis among patients of knee joint pain. JSZMC, (2015); 6(4): 885-887.
- Messier SP, et al. Weight loss reduces knee‐joint loads in overweight and obese older adults with knee osteoarthritis. American College of Rheumatology, (2005); 52(7): 2026-2032.
- Miranda H, et al. A prospective study on knee pain and its risk factors. Elsevier, (2002); 10(8): 623-630.
- Felson, D.T. An update on the pathogenesis and epidemiology of osteoarthritis. Radiologic Clinics of North America, (2004); 42(1): 1-9.
- Jones G et al. Sex and site differences in cartilage development: a possible explanation for variations in knee osteoarthritis in later life. Official Journal of the American College of Rheumatology, (2000); 43(11): 2543-2549.
- Al-Arfaj AS. Radiographic osteoarthritis and obesity. Saudi Medical Journal, (2002); 23(8): 938-942.
- Lethbridge‐Çejku M, et al. Association of radiographic features of osteoarthritis of the knee with knee pain: data from the Baltimore Longitudinal Study of Aging. Official Journal of the American College of Rheumatology, (1995); 8(3): 182-188.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0