

Full Length Research Article
Incidence of Colorectal Carcinoma in the Remote Area of Sindh, Pakistan
Muhammad Nawaz Abro1, Muhammad Ejaz Khan1, Muhammad Ibrahim2, Greesh Kumar Maheshwari3, Ghulam Asghar1, Sarfraz Ahmed4, Muhammad Qasim1, Muhammad Allim1, Quratulain Soomro1, Jahanzaib Khan1, Gotam Kumar5, Muhammad Zeeshan Ahmed2, Suvash Chandra Ojha6*
Adv. life sci., vol. 9, no. 4, pp. 539-546, December 2022
*– Corresponding Author: Suvash Chandra Ojha (Email: suvashojha@swmu.edu.cn)
Authors' Affiliations
2. Department of Biochemistry, Bahauddin Zakariya University, Multan – Pakistan
3. APPNA Institute of Public Health, Jinnah Sindh Medical University, Karachi – Pakistan
4. Department of Basic Sciences, University of Veterinary and Animal Sciences Lahore, Narowal, 51600, Narowal, Pakistan
5. Peoples University of Medical and Health Sciences, 67450, Nawabshah – Pakistan
6. Southwest Medical University, Jiangyang District, Luzhou, 646000, Sichuan – China
[Date Received: 20/08/2022; Date Revised: 19/11/2022; Date Published: 31/12/2022]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Colorectal carcinoma (CRC) is the third most common cancer in the world that show malignant growth in the colon, rectum, and or appendix. CRC is the second most common malignancy in females and third in males. This study aimed to ascertain the incidence of colorectal carcinoma (CRC) in a population in a remote area of Sindh, Pakistan, and also compared and correlated the sociodemographic characteristics and different parameters such as diagnosis, grade, and histopathology of the CRC cases.
Methods: The study was conducted from February 2012 to 2019 at Pakistan Atomic Energy Cancer Hospital (NORIN) Nawabshah Sindh, Pakistan. All cases were evaluated through a detailed history, clinical examination, radiological examination, and histopathology-proven cases. The sociodemographic parameters, diagnosis grades, and histopathology of the CRC were statistically compared and correlated by SPSS version 21.
Results: Out of a total of 10,848 reported patients, 424 (3.9%) were of CRC. The CRC was further comprised of 63.9% males and 36.1% females. We classified our patients into two age groups, ≤ 40 years (Group-A), and > 40 years (Group B). Group-A comprised 41% of patients, and their mean age was 28±6.98 years, while Group B comprised 59% of patients with a mean age of 43±8.3 years. Histological specimens divulged that most of the common specimens were of adenocarcinoma. Early diagnosis was very strenuous due to no signs and symptoms. Thus, the majority of the patients, approximately 39%, were found to be of grade 2 carcinoma.
Conclusion: Our study unveils an increased number of patients with CDC at an age of <40 belonging to rural areas. Further studies are needed to elucidate the cause of this high incidence with a particular focus on genetic and molecular risk factors.
Keywords: Active lifestyle, Colorectal Carcinoma; Age group; Colorectal Adenocarcinoma
Introduction![]()
malignant growth in the colon, rectum, and or appendix. According to World Health Organization (WHO), CRC is one of the most common prevailed cancers with 1.93 million present cases worldwide [1,2]. It is the third most common cancer in the world, fifth in Pakistan, and the fourth leading cause of mortality and morbidity [3,4]. Literature shows that CRC is the second most common malignancy among females and the third in males [1]. Approximately 1400000 new cases are reported every year. Recent data shows a higher incidence of CRC in developed countries. In recent years, it is noted that colorectal carcinoma has no longer been restrained from disease in developed countries. It is also upturned in developing countries as well. Approximately, 36% of new CRC cases were diagnosed in developing countries in the year 2000 with a continuous uptrend [5]. This rise has been attributed to a mass change in physical activity and the worse dietary habit patterns which ultimately superimpose on genetic predisposition.
Age is assumed as one of the major risk factors in CRC. Its occurrence is rare in patients ≤ 40 years. Hence, the incidence increases abruptly with every decade of life. The risk of CRC has been reported as 1 in 10 males after the eighth decade of life [6]. The risk of CRC over a lifetime has accounted for 5% and it totals 90% of the cases diagnosed in patients’ ˃50 years [6]. A recent report shows that the incidence of colorectal cancer increases over one year of age increment. It was analyzed that the most distinct increase in incidence was 46.1% in 49–50-year age transformation with an incidence rate ratio of 1.46. The outcomes also suggested that many CRC cases remain undisclosed and explode with exposure only when potential and standard screening was functionalized at the age of 50 [7]. The incidence of this disease in youngsters has been reduced due to potential exposure to risk factors, for instance, physical inactivity, western diet style, obesity, and antibiotic use, particularly in prenatal to adolescence. These risk factors affect the gut microbiota, host immunity, genetics, and epigenetics of colon epithelial cells. Early-onset colorectal cancer holds potential differential pathological, molecular, and clinical characteristics when compared to later onset. Several resources can be used to explicate the etiology of CRC at an early age for the development of premature detection, sound effective prevention, and potential various therapeutic strategies. Furthermore, additional cohort studies in youngsters and childhood integrated with specimen collection, absolute omics analysis of biomarkers, and molecular pathological approaches may provide a better understanding of this disease [8]. Data from prospective interventional studies stipulate that dietary fibers, calcium intake, fat intake, and CRC are not transparent with no exclusive conclusions [9,10]. Additional risk factors may incorporate the consumption of tobacco and alcohol, hormone replacement therapy in women, total calorie consumption, and physical activity related to obesity [11–13]. Interestingly, there has been a swift recognition that regular use of nonsteroidal anti-inflammatory agents such as aspirin and cyclooxygenase-2 inhibitors such as celecoxib, may have a preventive effect against colorectal adenomas and or carcinomas [14,15]. Advancements in molecular modeling of CRC further facilitate the direct therapeutics of biological characteristics of tumors. Although treatment options remain atypical, many sufferers may help to anticipate the extended survival rate. Furthermore, genetic profiling may allow treatment options so that many patients can get benefits and some are presumed to get exposed to toxicity from scant therapies [16].
A meta-analysis of cancer prevalence in Pakistan (2018) found a statistically significant range of CRC cases from 5 to 19% regarding age and 5% overall prevalence [17]. Another study used the database of the Pakistan Atomic Energy Commission Cancer Registry (PAECCR) program to analyze the trend of incidence of cancer in the Punjab Province of Pakistan for 30 years (1984-2014) and confirmed the 3460 positive cases of CRC out of 64204 [18]. A cross-sectional study reported a 2:1 ratio for the male to female and 33.3±7.9 years of mean age for incidence of young CRC cases from a tertiary care oncology center in Karachi, Pakistan. In CRC cases, 45% and 55% of patients accounted for rectal and colon cancer [6]. Similarly, a study confirmed a total of 5.9% CRC cases including 4.1% females and 7.9% males in the Section of Histopathology, Department of Pathology and Laboratory Medicine, Aga Khan University Hospital, Karachi, Pakistan [19]. Further a cross-sectional study recruited CRC cases from January 2018 to December 2019 and confirmed 60% of CRC cases below 40 years and 40% ≥40 years of age with an average age of 46.64±8.74 [20]. Another cross-sectional study on 113 CRC patients from Karachi, Pakistan, promulgates that colorectal cancerous patients in Pakistan are facing the problem of delay in diagnosis and presentation. This is the potential reason behind the detection of the disease at an advanced level with an outright poor prognosis. This report advocates that a CRC control program should be executed to diagnose this mortal disease at an early stage [21]. Occupational exposure from a broader perspective may profess colorectal carcinoma. Presumedly insignificant cases of these malignancies could be explicated considering occupational exposure as a cofactor in cancer proceedings [22]. Pakistan Atomic Energy Cancer Hospital (NORIN) Nawabshah, Pakistan grasps one of the leading oncological treatment centers in Sindh, Pakistan. The hospital commenced function in 2012 and provides a cancer treatment facility to more than 8.7 million population from various surrounding districts of Sindh, Pakistan [23,24]. The majority of the patients are treated free of cost with provincial and federal government donations. Although very few studies have reported CRC in youths of Pakistan in the past, data about the Sindh area of Pakistan is lacking on the greater population at high risk. The present study aimed to establish the contemporaneous pragmatic incidence of CRC in patients in a remote area of Sindh, Pakistan, based on age, gender, and socioeconomic status with a special focus on diagnosed histopathology. Further, it compared and correlated the sociodemographic characteristics and different parameters such as diagnosis, grade, and histopathology of the CRC cases.
Methods![]()
This study is a retrospective descriptive observational study at Pakistan Atomic Energy Cancer Hospital (NORIN), Nawabshah, Sindh, Pakistan, data retrospectively was collected from February 2012 to May 2019, through the oncology and radiotherapy Patient Department (OPD). The ethical research committee's approval was taken vide letter no. NORIN/2021/20R. Informed consent was taken from all patients. Patients: Patients were divided into two different age groups for data collection; group A ≤ 40 years and group B > 40 years. Data collection was performed through chart review utilizing predesigned and coded questionnaires. Detail of the demographic information, symptomatology, supposed risk factors, family history, histopathological features, and outcomes were collected for all selected patients. Surgical histopathology records were reviewed for tumor grading. Patients who were supposed to have suspected familial syndrome based on the clinical history and or colonoscopy findings, incomplete documented biopsy reports, and histopathological reports from other hospitals were also excluded from the data analysis. All cases were evaluated through a detailed history, clinical examination, radiological examination, and histopathology-proven cases [25]. All obtained data were arranged in an Excel spreadsheet. SPSS version 21 was used for the statistical analysis [26]. In descriptive statistics, frequency, percentage, mean, and standard deviation were obtained for the CRC cases. For the inferential statistics, the chi-square test was applied for the comparison between the sociodemographic parameters and diagnosis grades, and histopathology of the CRC cases. The Pearson correlation test was applied to correlate the sociodemographic characteristics and different parameters of CRC cases [27,28]. The significance level for all statistical tests was considered at 95% (p ≤ 0.05).
Results
![]()
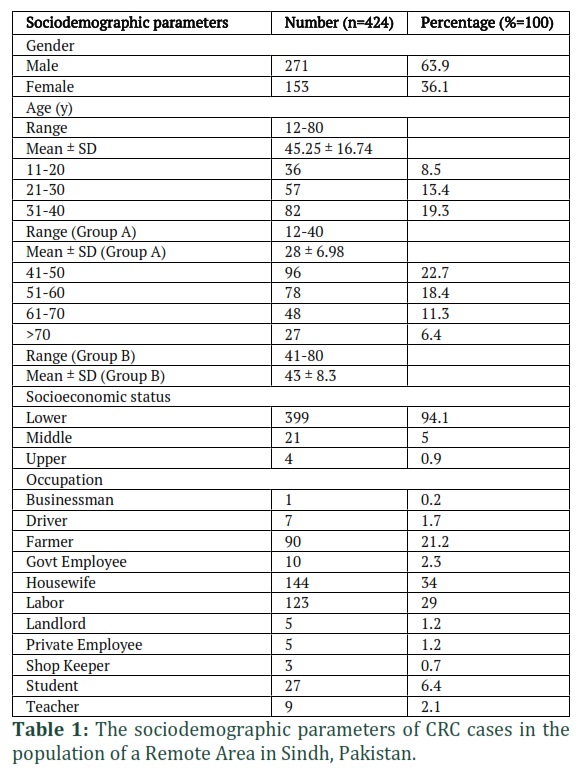
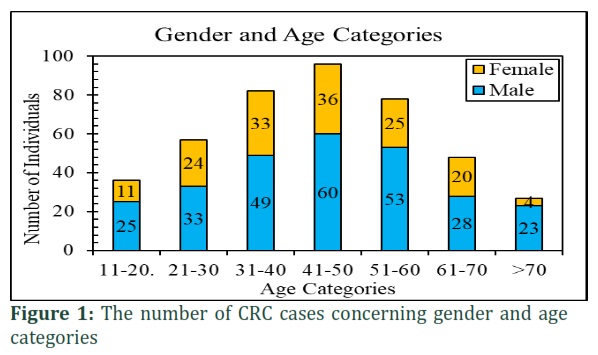
The frequency, percentages, mean, and standard deviation of the sociodemographic parameters of the colorectal carcinoma cases were analyzed by descriptive statistics. Table 1 represents the sociodemographic parameters of CRC cases in the population of a Remote Area in Sindh, Pakistan. A total of 10,848 patients of which 424 (3.9%) were suffering from CRC. The male and female cases of CRC were identified in a 1.77:1 ratio. The average age range of CRC cases was 12-80 years (M = 45.25, SD = 16.74). Furthermore, the age groups were categorized into two groups. Group A has patients with ages less than 40 years (M = 28, SD = 6.98) and Group B has patients with ages more than 40 years (M = 43, SD = 8.3). Figure 1 shows the incidence of CRC cases regarding gender and age categories. A maximum number of CRC cases were identified in the age group 41 to 50 years. In which, male CRC cases were higher than females. Similarly, CRC patients were divided into three socioeconomic statuses: lower, middle, and upper. The incidence of CRC was higher (94.1%) in the lower socio-economic class. According to the occupation, 34% of CRC cases were housewives and 29% of cases were laborers.
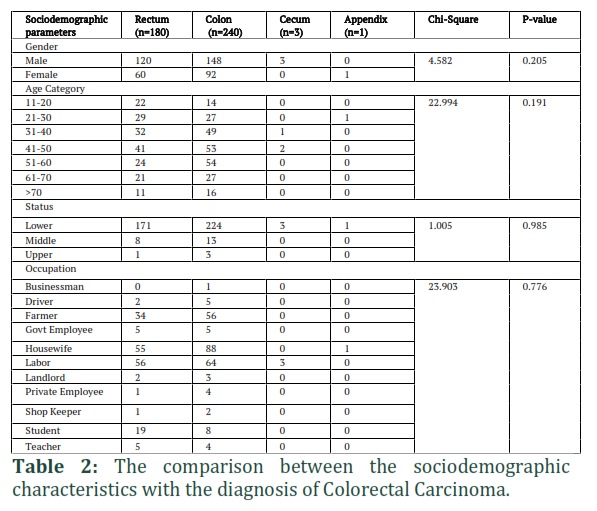
Table 2 shows the comparison between the sociodemographic characteristics with the incidence of diagnosis of CRC cases. A chi-square test of independence confirmed a nonsignificant association between gender (p = 0.205), age categories (p = 0.191), socioeconomic status (p = 0.985), and occupation (p = 0.776) with the diagnosis of CRC cases.
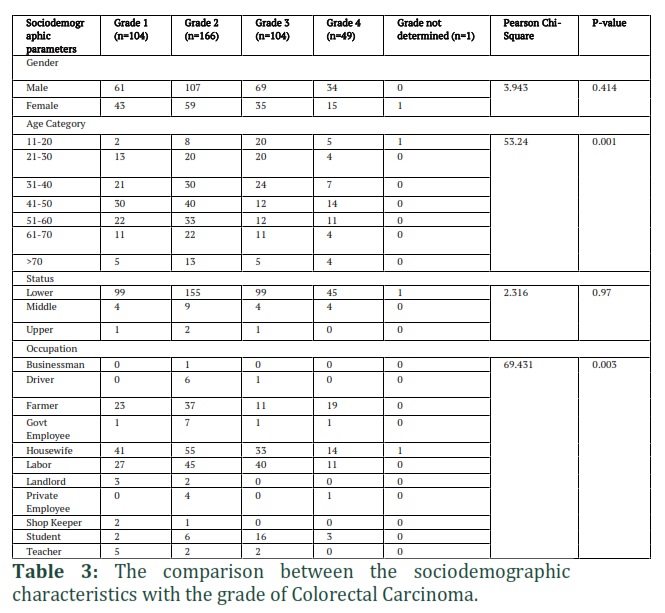
Table 3 shows the comparison between the sociodemographic characteristics with the incidence of the grades of CRC cases. A chi-square test of independence confirmed the significant association between the age categories (p = 0.001), and occupation (p = 0.003) with the grades of CRC cases.
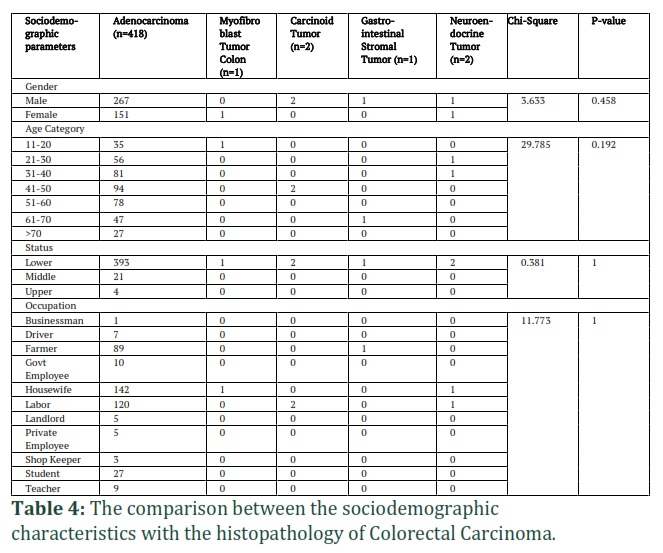
Table 4 shows the comparison between the sociodemographic characteristics with the incidence of the histopathology of CRC cases. A chi-square test of independence showed a nonsignificant association between gender (p = 0.458), age categories (p = 0.192), socioeconomic status (p = 1), and occupation (p = 1) with the histopathology of CRC cases.
Figure 2 depicts the correlation between the sociodemographic characteristics and different parameters of CRC cases. The age category was negatively and significantly correlated with the occupation (p≤0.001), and grade level (p≤0.01) of the CRC cases. Similarly, CRC diagnoses were negatively and significantly correlated with occupation (p≤0.01), and positive with histopathology (p≤0.001) of the CRC cases.
Table 3 shows the comparison between the sociodemographic characteristics with the incidence of the grades of CRC cases. A chi-square test of independence confirmed the significant association between the age categories (p = 0.001), and occupation (p = 0.003) with the grades of CRC cases. Table 4 shows the comparison between the sociodemographic characteristics with the incidence of the histopathology of CRC cases. A chi-square test of independence showed a nonsignificant association between gender (p = 0.458), age categories (p = 0.192), socioeconomic status (p = 1), and occupation (p = 1) with the histopathology of CRC cases. Figure 2 depicts the correlation between the sociodemographic characteristics and different parameters of CRC cases. The age category was negatively and significantly correlated with the occupation (p≤0.001), and grade level (p≤0.01) of the CRC cases. Similarly, CRC diagnoses were negatively and significantly correlated with occupation (p≤0.01), and positive with histopathology (p≤0.001) of the CRC cases.
Figures & Tables

Colorectal carcinoma is primarily presumed to be a disease in elder people. However, recently its rapid increase in the age group is pretty alarming. Epidemiological data shows that the incidence of CRC is much lower in the developing world. However, a recent report denotes a higher incidence of this disease or early onset in the developing world [29]. Interestingly, it is hypothesized that sporadic early-onset CRC is a biologically and clinically distinguished entity, which accounts for its aggressive pattern and quite poorer survival [30]. Our results demonstrate that the mean age is 45.25 ± 16.74 years (Table 1) for the onset or diagnosis of this carcinoma. CRC has been reported as the third most common in the world and the fifth most common cancer in Pakistan [3,4], and the tenth most common cancer out of 20 malignancies in our center. In the lifetime of an individual, there is a 5% risk that he/she might acquire CRC [31].
It has been observed that CRC screening is not routinely done in our region due to financial issues, lack of awareness, and advanced facilities. Even in major cities where people have more advanced medical facilities, it is not investigated routinely and leads to advanced-stage malignancies. Our research indicated that the majority of the patients, i.e., 39.6%, were diagnosed with carcinoma of grade II (Table 3). Unfortunately, there is no proper or adequate cancer data registry in Pakistan, and our study is one of the pilot studies on the early age onset of CRC. In Pakistan, however, limited studies have reported the incidence of age colorectal carcinoma to be 20.8% below 30 years of age group in a study at Shaukat Khanum Cancer Hospital (SKMCH), Pakistan [32], while Whilst, another study conducted at Dow University Hospital Karachi reported the incidence of colorectal carcinoma as 52% below age<40 [33]. Data from Globocan, Pakistan, reported colorectal carcinomas incidence to be 23.4% in males, and 26% in females under age 40 [34]. As per an Indian study, the incidence of colorectal carcinoma was found to be 33% in those <40 age [35]. A study in China reported its incidence as 6.1% in <30 age [34]. Egyptian research manifests CRC incidence as 36% at age [34,36]. In comparison to advanced countries, an American study demonstrates colorectal carcinomas incidence as 3.9% below the age of 40 years [37].
Our report analyzed a rural population from Nawabshah, Sindh. The mean age of the patients was 45.25 ± 16.74 years in our study, significantly lower than the mean age at colorectal diagnosis in other previously published series in other countries [6,17–21]. Our study findings showed that 63.9% of males and 36.1% of females were found to be victims of colorectal carcinoma (Table 1). Thus, the literature [6,17–21] supports sufficient evidence of CRC at a younger age in developing countries like Pakistan. The incidence of CRC has been reported to be dropped in the United States, and the quiet reason behind this success is proper or appropriate early screening [31], which seems scant in Pakistan.
Our study also depicts that colon cancer was more frequent in both males and females followed by rectum type. Similarly, the count of cecum and appendix-type cancers was found to be minimum in both males and females. The patterns of the colon and rectum were observed even higher in males compared to females. By gender, higher-grade carcinomas were observed in males compared to females. Similarly, in the general pyramid of the population, it was concluded that CRC incidence is higher in males compared to females. A similar study in Pakistan in a different area reported results akin to our study about colon and rectal carcinomas, and cancer grading based on gender and age [6]. The equal prevalence of colon and rectal cancers that we observed coincided with the ratios reported in countries that had been historically labeled as low-risk [38,39]. The even worse stage at presentation and poorer grade of tumors in our study population were similar to such studies globally showing the aggressiveness of the disease in the population of CRC patients.
Genetics plays a critical role in the incidence of CRC. It has been hypothesized that there are mutations in FBXW7 and POLE genes in young adults [31], which seem a protruding cause of CRC. It has also been reported that nutrition and an active lifestyle play an important role in preventing CRC, including sources of calcium, fiber, folate, vitamin D, vitamin B6, and magnesium in daily diet. Blood-thinning medications (like Aspirin), and NSAIDs (nonsteroidal anti-inflammatory drugs) have also shown protective effects against CRC [40]. On the other hand, consumption of alcohol, highly processed red meat, junk foods, smoking, inactive lifestyle, and poor socioeconomic status have also been deduced as cofactors in prompting CRC [41]. In developed countries, colorectal carcinoma is due to the consumption of highly red processed meat and less use of vegetables, and a fiber diet. However, in our study, the majority of the patients belong to low socioeconomic by professional farmers and laborers whose major part of the diet includes vegetables and fiber foods, and rare use of red meat and junk foods [42]. Evidence entailed that farming, quarrying, and mining are not torpid occupations, consequently, these physical activities could account for the lower risk. Despite this, some sparse evidence of increased risk in workers belongs to the pesticide or herbicide business.
Workers belonging to industrial branches with an increased threat of this disease could be efficaciously addressed to diagnosing and counseling programs to prevent the onset of carcinoma or to anticipate screening, with a beneficial effect on the potential of survival [43]. Smoking early in life has also been established as another risk factor for colon cancer. In a recent study, it has been declared that metabolic dysfunction leads to the onset of CRC at an early age, especially in the proximal and distal colon [44]. This study confirmed a nonsignificant association between sociodemographic characteristics of patients with the incidence of diagnosis and histopathology of CRC cases (Tables 2 and 4). However, age categories and occupation showed a significant association with the grades of CRC cases (Table 3). In the correlation analysis, a significantly negative correlation of age category with the occupation and grade level; and diagnoses with the occupation of the CRC cases was observed. Lastly, CRC diagnoses were significantly positive in correlation with histopathology of the CRC cases (Figure 2). In Pakistan, CRC is also sporting like other developed countries at a younger age. A physician should know the differential diagnosis possibility of CRC if symptoms are not improving, to catch the disease early and treat it with curative intention rather than let the disease spread and the treatment becomes palliative.
This study concludes that CRC can occur at an age of <40 despite gender distribution with late diagnosis betraying the aggressiveness of the disease. In Pakistan, proper screening methods are not being practiced for early diagnosis, which may lead to worse outcomes or poor prognosis. The only way we can overcome this lag is when doctors and or practitioners have sound knowledge about the disease with a firm grip over differential diagnosis. The population at risk such as a remote area of Sindh, Pakistan, needs to be identified and screened and should be educated about the relevant information and preventive measures of CRC. Another challenging task for medical professionals is to understand the role of the genetics behind CRC and make specified treatments.
![]()
Author Contributions
MNA, MEK, MI, GA, SA, MQ, SCO: Conception and design, data acquisition and analysis, interpretation, literature search, critical revision, and final approval. MA, QS, JK, GK, GKM: Data acquisition and analysis, interpretation, drafting, literature search, and final approval. MZA, SA, SCO: Wrote the paper, data acquisition and analysis, interpretation, critical revision, drafting, and final approval.
Acknowledgment
We are thankful to Pakistan Atomic Energy Cancer Hospital (NORIN) Nawabshah, Sindh, Pakistan, and its staff for supporting data collection.
References
- Gandomani HS, Yousefi SM, Aghajani M, Mohammadian-Hafshejani A, Tarazoj AA, Pouyesh V, Salehiniya H. Colorectal cancer in the world: incidence, mortality and risk factors. BioMed Research International, (2017); 4: 1656.
- WHO Cancer. World Health Organization: WHO. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on Nov 18, 2022).
- Rashid MU, Naeemi H, Muhammad N, Loya A, Lubiński J, Jakubowska A, Yusuf MA. Prevalence and spectrum of MLH1, MSH2, and MSH6 pathogenic germline variants in Pakistani colorectal cancer patients. Hereditary Cancer in Clinical Practice, (2019); 17: 1–16.
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer Journal for Clinicians, (2021); 71: 209–249.
- Anwar N, Badar F, Yusuf MA. Profile of patients with colorectal cancer at a tertiary care cancer hospital in Pakistan. In Proceedings of the Annals of the New York Academy of Sciences; Blackwell Publishing Inc., (2008); 1138: 199–203.
- Zahir MN, Azhar EM, Rafiq S, Ghias K, Shabbir-Moosajee M. Clinical Features and Outcome of Sporadic Colorectal Carcinoma in Young Patients: A Cross-Sectional Analysis from a Developing Country. ISRN Oncology, (2014); 2014: 1–8.
- Abualkhair WH, Zhou M, Ahnen D, Yu Q, Wu XC, Karlitz JJ. Trends in Incidence of Early-Onset Colorectal Cancer in the United States among Those Approaching Screening Age. JAMA Network Open, (2020); 3: e1920407–e1920407.
- Akimoto N, Ugai T, Zhong R, Hamada T, Fujiyoshi K, Giannakis M, Wu K, Cao Y, Ng K, Ogino S. Rising incidence of early-onset colorectal cancer — a call to action. Nature Reviews Clinical Oncology, (2021); 18: 230–243.
- Yu EYW, Wesselius A, Mehrkanoon S, Brinkman M, Van Den Brandt P, White E, Weiderpass E, Le Calvez-Kelm F, Gunter M, Huybrechts I, et al. Grain and dietary fiber intake and bladder cancer risk: A pooled analysis of prospective cohort studies. The American Journal of Clinical Nutrition, (2020); 112: 1252–1266.
- Wactawski-Wende J, Kotchen JM, Anderson GL, Assaf AR, Brunner RL, O’Sullivan MJ, Margolis KL, Ockene JK, Phillips L, Pottern L, et al. Calcium plus Vitamin D Supplementation and the Risk of Colorectal Cancer. The New England Journal of Medicine, (2006); 354: 684–696.
- Meyerhardt JA, Heseltine D, Niedzwiecki D, Hollis D, Saltz LB, Mayer RJ, Thomas J, Nelson H, Whittom R, Hantel A, et al. Impact of physical activity on cancer recurrence and survival in patients with stage III colon cancer: Findings from CALGB 89803. Journal of Clinical Oncology, (2006); 24: 3535–3541.
- Meyerhardt JA, Niedzwiecki D, Hollis D, Saltz LB, Hu FB, Mayer RJ, Nelson H, Whittom R, Hantel A, Thomas J, et al. Association of dietary patterns with cancer recurrence and survival in patients with stage III colon cancer. Obstetrical & Gynecological Survey, (2008); 63: 94–96.
- Meyerhardt JA, Niedzwiecki D, Hollis D, Saltz LB, Mayer RJ, Nelson H, Whittom R, Hantel A, Thomas J, Fuchs CS. Impact of body mass index and weight change after treatment on cancer recurrence and survival in patients with stage III colon cancer: Findings from cancer and leukemia group B 89803. Journal of Clinical Oncology, (2008); 26: 4109–4115.
- Flossmann E, Rothwell PM. Effect of aspirin on long-term risk of colorectal cancer: consistent evidence from randomised and observational studies. Lancet, 2007; 369: 1603–1613.
- Koehne CH, Dubois RN. COX-2 inhibition and colorectal cancer. Seminars in Oncology, (2004); 31: 12–21.
- Strickler JH, Yoshino T, Graham RP, Siena S, Bekaii-Saab T. Diagnosis and Treatment of ERBB2-Positive Metastatic Colorectal Cancer: A Review. JAMA Oncology, (2022); 325: 669–685.
- Idrees R, Fatima S, Abdul-Ghafar J, Raheem A, Ahmad Z. Cancer prevalence in Pakistan: Meta-analysis of various published studies to determine variation in cancer figures resulting from marked population heterogeneity in different parts of the country. World Journal of Surgical Oncology, (2018); 16: 1–11.
- Masood K, Masood A, Zafar J, Shahid A, Kamran M, Murad S, Masood M, Alluddin Z, Riaz M, Akhter N, et al. Trends and Analysis of Cancer Incidence for Common Male and Female Cancers in the Population of Punjab Province of Pakistan during 1984 to 2014. Asian Pacific Journal of Cancer Prevention, (2015); 16: 5297–5304.
- Ahmad Z, Idrees R, Fatima S, Uddin N, Ahmed A, Minhas K, Memon A, Fatima SS, Arif M, Hasan S, et al. Commonest cancers in Pakistan – findings and histopathological perspective from a premier surgical pathology center in Pakistan. Asian Pacific Journal of Cancer Prevention, (2016); 17: 1061–1075.
- Bhurgri AA, Khatti SN, Danish AA, Shaikh M, Seerani NL, Memon AS, Shaikh MK, Raza S, Shah SZA. Frequency of Rectal Cancer among Young and Older patients. Pakistan Journal of Medical & Health Sciences, (2022); 16: 28–29.
- Ahmed RN, Rai L, Samo KA, Saeed S, Salam A, Khan H, Memon AS. Factors affecting delay in diagnosis of colorectal cancer: A cross-sectional study from a tertiary care hospital of Karachi, Pakistan. International Journal of Clinical Practice, (2021); 75: e14529.
- Alexander DD, Weed DL, Mink PJ, Mitchell ME. A weight-of-evidence review of colorectal cancer in pesticide applicators: The agricultural health study and other epidemiologic studies. International Archives of Occupational and Environmental Health, (2012); 85: 715–745.
- Sohaib M, Shafiq A. PAEC’s Annual Cancer Registry Report 2015-2017.
- Sohaib, M.; Shafiq, A. PAEC Cancer Registry Report 2018 and 2019.
- Badar F, Mahmood S. Hospital-based cancer profile at the Shaukat Khanum memorial cancer hospital and research centre, Lahore, Pakistan. Journal of College of Physicians and Surgeons Pakistan, (2015); 25: 259–263.
- Ahmed MZ, Shahzad H, Rao T, Ali A, Samad N. Seroprevalence of Hepatitis C Virus (HCV) and Hepatitis B Virus (HBV) In District Vehari, Pakistan. Journal of College of Physicians and Surgeons Pakistan, (2020); 30: 550–551.
- Elalouf A, Edelman A, Sever D, Cohen S, Ovadia R, Agami O, Shayhet Y. Students’ Perception and Performance Regarding Structured Query Language Through Online and Face-to-Face Learning. Frontiers in Education, (2022); 7: 935997.
- Elalouf A, Moran R, Yaron B, Oman M. Pediatric Dental Emergency Visits and Treatment during Lockdown in the COVID-19 Pandemic: A Retrospective Study. International Journal of Environmental Research and Public Health, (2022); 19: 3774.
- Quach DT, Nguyen OT. Clinical, endoscopic and pathogical characteristics of early- onset colorectal cancer in Vietnamese. Asian Pacific Journal of Cancer Prevention, (2012); 13: 1767–1770.
- Chan KK, Dassanayake B, Deen R, Wickramarachchi RE, Kumarage SK, Samita S, Deen KI. Young patients with colorectal cancer have poor survival in the first twenty months after operation and predictable survival in the medium and long-term: Analysis of survival and prognostic markers. World Journal of Surgical Oncology, (2010); 8: 1–11.
- Campos FG. Colorectal cancer in young adults: A Difficult challenge. World Journal of Gastroenterology, (2017); 23: 5041–5044.
- Akbar A, Bhatti ABH, Khattak S, Syed AA, Kazmi AS, Jamshed A. Outcome of rectal cancer in patients aged 30 years or less in the Pakistani population. Asian Pacific Journal of Cancer Prevention, (2014); 15: 6339–6342.
- Amini AQ, Samo KA, Memon AS. Colorectal cancer in younger population: Our experience. Journal Of Pakistan Medical Association, (2013); 63: 1275–1277.
- Sarwar MR, Saqib A. Cancer prevalence, incidence and mortality rates in Pakistan in 2012. Cogent Medicine, (2017); 4: 1288773.
- Patil PS, Saklani A, Gambhire P, Mehta S, Engineer R, De’Souza A, Chopra S, Bal M. Colorectal Cancer in India: An Audit from a Tertiary Center in a Low Prevalence Area. Indian Journal of Surgical Oncology, (2017); 8: 484–490.
- Soliman AS, Bondy ML, El-Badawy SA, Mokhtar N, Eissa S, Bayoumy S, Seifeldin IA, Houlihan PS, Lukish JR, Watanabe T, et al. Contrasting molecular pathology of colorectal carcinoma in Egyptian and Western patients. British Journal of Cancer, (2001); 85: 1037–1046.
- Pirzada MT, Ahmed MJ, Muzzafar A, Nasir I. ul I, Shah MF, Khattak S, Syed AA. Rectal Carcinoma: Demographics and Clinicopathological Features from Pakistani Population Perspective. Cureus, (2017); 9.
- Bhurgri Y, Khan T, Kayani N, Ahmad R, Usman A, Bhurgri A, Bashir I, Hasan SH, Zaidi SMH. Incidence and current trends of colorectal malignancies in an unscreened, low risk population. Asian Pacific Journal of Cancer Prevention, (2011); 12: 703–708.
- Parkin DM, Bray F, Ferlay J, Pisani P. Global Cancer Statistics, 2002. CA: A Cancer Journal for Clinicians, (2005); 55: 74–108.
- Thanikachalam K, Khan G. Colorectal cancer and nutrition. Nutrients, (2019); 11: 164..
- Song M, Chan AT. Environmental factors, gut microbiota, and colorectal cancer prevention. Clinical Gastroenterology and Hepatology, (2019);17(2): 275-289.
- Oddone E, Modonesi C, Gatta G. Occupational exposures and colorectal cancers: A quantitative overview of epidemiological evidence. World Journal of Gastroenterology, (2014); 20: 12431–12444.
- Rawla P. Epidemiology of prostate cancer. World journal of oncology, (2019); 10(2): 63.
- Chen H, Zheng X, Zong X, Li Z, Li N, Hur J, Fritz CDL, Chapman W, Nickel KB, Tipping A, et al. Metabolic syndrome, metabolic comorbid conditions and risk of early-onset colorectal cancer. Gut, (2021); 70: 1147–1154.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0