

Full Length Research Article
Evaluation and determining of the Pattern of the Human Albumin Utilization at Shahid Rahimi Hospital, Khorramabad, Iran
Vahid Rahimi1, Fanak Fahimi2,3, Javad Ghasemian Yadegari4, Hadi Hayati Abbarik5, Arian Karimi Rouzbahani1,6, Zahra Heydari1,6, Ali Kharazmkia7*
Adv. life sci., vol. 9, no. 4, pp. 595-602, December 2022
*– Corresponding Author: Ali Kharazmkia (Email: kharazmkia@gmail.com)
Authors' Affiliations
2. Department of Clinical Pharmacy, School of Pharmacy, Shahid Beheshti University of Medical Sciences, Tehran – Iran
3. School of Pharmatech American Career College, California, USA
4. Department of pharmacognosy, School of Pharmacy, Lorestan University of Medical Sciences, Khorramabad – Iran
5. Department of Pharmacoeconomics and Management, School of Pharmacy, Lorestan University of Medical Sciences, Khorramabad – Iran
6. USERN Office, Lorestan University of Medical Sciences, Khorramabad – Iran
7. Department of Clinical Pharmacy, School of Pharmacy, Lorestan University of Medical Sciences, Khorramabad – Iran
[Date Received: 01/10/2022; Date Revised: 14/11/2022; Date Published: 31/12/2022]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: The World Health Organization (WHO) has supported many intervention strategies, including executive, educational, and monitoring proceedings to improve the evaluation of drug use and the drug management system. Since the resources are limited, it is essential to utilize existing resources properly. Serum albumin is the most abundant blood protein produced in the liver. Different forms of albumin are available in the market and employed to treat hypovolemia, Cirrhotic ascites, severe burns, septic shock, hyperstimulation syndrome, etc. Due to the high price of albumin and its importance for saving patient’s lives.
Methods: precisely according to the determined protocols, and it’s unreasonable and irrational medication should be avoided. Statistical analysis was performed in Shahid Rahimi Hospital of Khorramabad, Iran, from March 2018 to March 2019. Albumin administration for randomly selected patients receiving albumin in different wards was evaluated. The main sources to retrieve information were pharmacy drug folders, patient folders (including laboratory information), and nursing folders. Age, sex, weight, ward, albumin level, symptoms, and final dose were recorded for each patient. Contraindications to the administration of albumin or any caution in its use were also considered. Data were analyzed by using SPSS16 and Excel software. Independent T-test and Chi-square test were employed to compare quantitative and qualitative variables. 271 patients were studied, including 160 men and 111 women.
Results: The two male and female surgical wards with 41 patients had the highest percentage of patients admitted with albumin administration. Also, the most common cause of albumin administration in patients was hypoalbuminemia. 55% of albumin prescriptions in Shahid Rahimi Hospital of Khorramabad were irrational, driving a substantial financial burden for the healthcare system and patients. Among all the prescribed cases, only 5.2% were approved by the pharmacist. Finally, 77.1% of patients recovered, and 22.9% died.
Conclusion: Considering that the highest percentage of patients receiving albumin administration, both among patients with irrational administration and in general, were in men's and women's surgical wards, it is recommended that the drugs prescribed in these wards be further investigated and get pre- Approved by a pharmacist to prevent higher medical costs for patients and healthcare system.
Keywords: Albumin; Hypovolemia; Cirrhotic Ascites; Septic Shock; Hyperstimulation Syndrome
Introduction![]()
Albumin is part of the globular protein family, all soluble in water and sensitive to heat. Albumin is generally a transport protein that binds to different ligands and carries them to various body parts through the blood. Human serum albumin is the major protein in human blood plasma and makes up about 50% of human plasma proteins. Albumin binds to and transports water, cations (such as Ca2+, Na+, and K+), fatty acids, hormones, bilirubin, thyroxine, and drugs (including barbiturates). Its primary function is to regulate blood oncotic pressure [1].
The reference range of albumin is 3.6-5 g / dL or 36-50 g / dL; more or less of this range causes problems in the body. Low albumin may be due to liver disease, nephrotic syndrome, burns, non-absorption of protein from the small intestine, malabsorption, malnutrition, late pregnancy, genetic changes, and malignancies. High albumin is almost always caused by dehydration [2].
The most important uses of intravenous albumin solutions include hypovolemia, adult respiratory distress syndrome (ARDS), burns, acute/severe nephrosis, and hepatorenal syndrome (HRS) (improved renal function). Intradialytic hypotension (treatment), Hemodynamic support of pediatric and neonatal shock, Hemolytic disease of infants, Cirrhotic ascites (prevention of central volume evacuation after paresthesia); Ovarian hyperstimulation syndrome (ovarian hyperstimulation) (treatment), plasma volume exchange (replacement fluid), in the correction of hypoproteinemia. In these cases, albumin leads to recovery and plays an auxiliary role [3-18].
Off-label uses include cirrhosis (in combination with diuretics to facilitate diuresis), spontaneous bacterial peritonitis (treatment), and volume increase in anemic patients with cirrhosis [19-22].
Medications can cause unwanted side effects. Contrary to popular belief, the side effects of a drug are considered specific to the arbitrary use of the drug, and it should be noted that unwanted side effects are caused by the use of all types of drugs; Both prescription and over-the-counter medications. Albumin should not be taken arbitrarily, and even doctors should not prescribe this drug except when necessary. Side effects of albumin-containing medications, the types of which have already been described, are as follows:
Heart failure, edema, hypertension, hypotension, tachycardia, chills, headache, itchy skin, skin rash, urticaria, hypervolemia, nausea, vomiting, anaphylaxis [23], Bronchial spasm, pulmonary edema [24], Fever in some cases.
Albumin is contraindicated, including sensitivity to albumin or any component of the formulation; severe anemia, heart failure; Patients at risk for increased heart overload (e.g., patients with renal failure, severe anemia, chronic anemia, or heart failure); Dilute with sterile water for injection (may cause hemolysis or acute renal failure) [25].
In severe liver diseases, renal impairment, and patients with sodium disorders, albumin should be used with extreme caution. Studies have shown that many cases of albumin use, which the consumer clinically requires, were unnecessary or inappropriate. Institutions must therefore define and implement guidelines for the responsible use of such agents in an increasingly costly healthcare setting [26].
Drug use in many hospitals around the world and, consequently, in Iranian hospitals, does not fully comply with the rules set by the Ministry of Health. Due to their high medical and pharmacological importance and their high price, some albumin-like drugs require more care in terms of how and how much to use. Therefore, in the forthcoming research project, we decided to study the amount and method of prescribing and consuming albumin and the amount of observing the prescribed protocols for prescribing this drug for one year in Shahid Rahimi Hospital in Khorramabad.
Methods![]()
In this study, we evaluated the appropriateness of using albumin in accordance with UpToDate and checked its compliance with this protocol. We tried to perform a drug utilization evaluation (DUE) on albumin, which is mostly performed in critical patients and thus has a significant effect on patient mortality. We filled in the required information for each patient based on her file in Shahid Rahimi Hospital and by comparing each one with UpToDate, we reported the rationality of albumin administration, the additional costs imposed on the person, the hospital and the government, etc.
A statistical survey was conducted in Shahid Rahimi Hospital, Khorramabad, Iran, from April 1 to March 2017. Albumin administration was evaluated for randomly selected patients who received albumin in different departments. If the use of albumin changes during hospitalization, the patient should be included in the study more than once. The main source for retrieved information was pharmacy drug files, patient files (including laboratory information) and nursing files. Age, sex, weight, section, albumin level, symptoms and final dose were recorded for each patient. Contraindications for administration of albumin or any precautions in its use were also investigated.
The data were analyzed using SPSS16 and Excel software, independent T-test and chi-square were used to compare quantitative and qualitative variables. Data were expressed as Mean ± SD or percentage. A P value of less than 0.05 is considered a statistically significant difference.
Results![]()
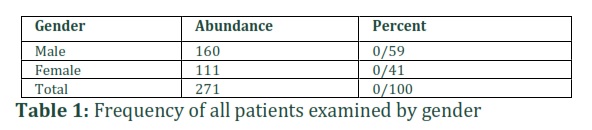
The present study was designed and conducted to evaluate the consumption and appropriateness of albumin administration in patients admitted to Shahid Rahimi Hospital in Khorramabad city in Lorestan province. This study examined 271 medical records, including 160 men (59.0%) and 111 women (41.0%) for whom albumin was prescribed (Table 1).
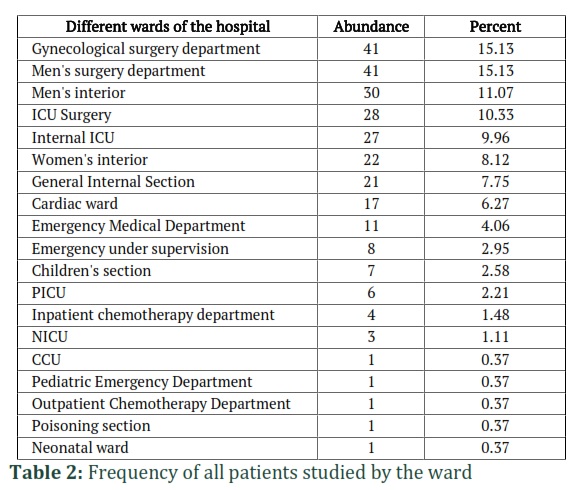
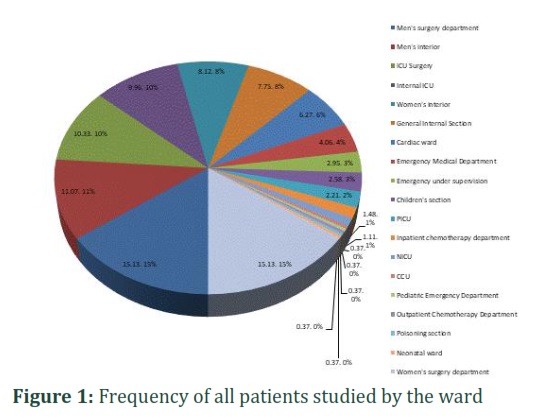
Dispersion of patients in different wards of the hospital and the amount of albumin prescribed in each ward
Other objectives of this study were the distribution of patients in different hospital wards and the amount of albumin prescribed in each ward. After that, men's internal ward with (11.07%) frequency, surgical ICU with (10.33%), internal ICU (9.96%), women's internal ward (8.12%), general ward (7.75%) ), Cardiac hospitalization (6.27%), emergency medical department (4.06%), emergency department (2.95%), pediatric ward (2.58%), Pediatric Intensive Care Unit (PICU) (2.21%), inpatient chemotherapy ward (1.48%), Neonatal Intensive Care Unit (NICU) (1.11%), The Coronary Care Unit (CCU) (0.37%), pediatric emergency department (0.37%), outpatient chemotherapy ward (0.37%), poisoning ward (0.37%) Percent) and neonatal ward (0.37 percent) were in the next positions (Table 2 and Figure 1 ).
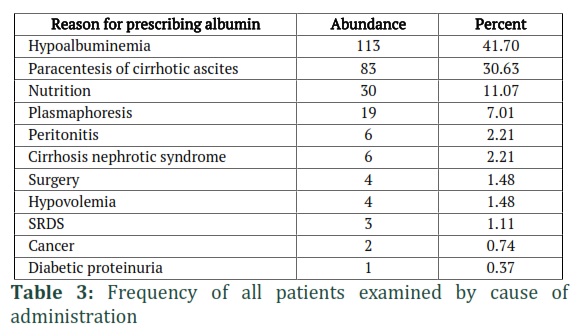
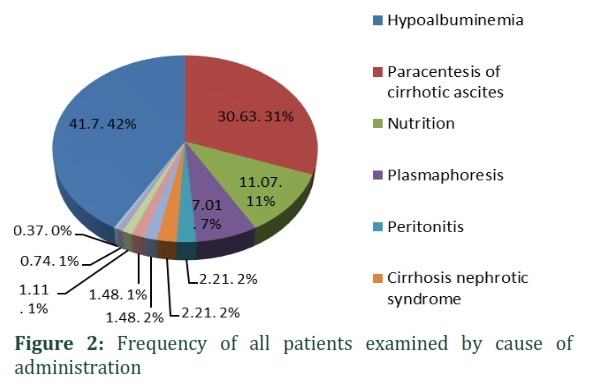
The frequency of all patients studied according to the cause of albumin administration
In this study, the examined cases were also examined in terms of the cause of albumin administration. The cause of hospitalization was 113 patients (41.7%) with hypoalbuminemia. Other causes of hospitalization in order of frequency are paracentesis of cirrhotic ascites (30.63%), nutritional (11.07%), plasmapheresis (7.01%), peritonitis (2.21%), cirrhosis and nephrotic syndrome (21 2.2%), surgery (1.48%), hypovolemia (1.48%), SRDS (1.11%), cancer (0.74%) and diabetic proteinuria (0.37%) (Table 3 and Figure 2),
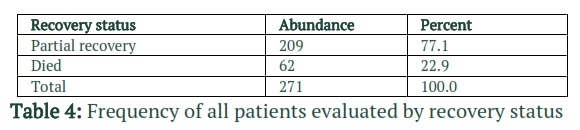
Frequency of all patients examined by recovery status
In this study, the final status of patients who received albumin was also evaluated, and the result was that out of 271 patients, 209 (77.1%) improved, and 69 (22.9%) died Were (Table 4).
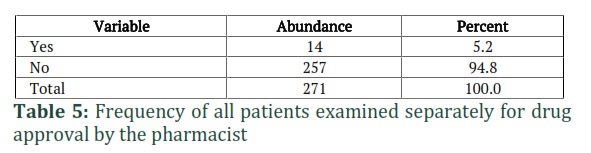
The frequency of all patients examined separately for albumin drug approval by the hospital pharmacist
Of all the cases studied, 14 cases (5.2%) were approved by the pharmacist before receiving the albumin by the patient, and 257 cases (94.8%) were not authorized by the pharmacist (Table 5). In addition, with the presence of a clinical pharmacist at Shahid Rahimi Hospital, he was not advised to prescribe albumin in any of the cases.
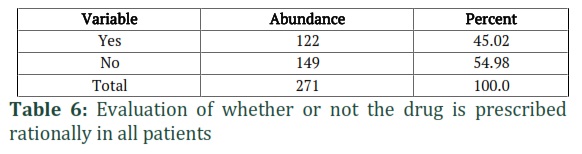
Evaluation of whether or not it is reasonable to prescribe the drug to all patients examined based on UpToDate
Prescribing the drug was reasonable in 122 of the total cases (45.02%), and in 149 cases (54.98%), these prescriptions were not appropriate (Table 6).
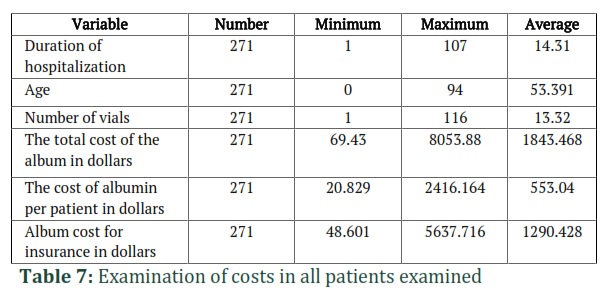
Evaluation of hospitalization period, age, number of vials, and the number of expenses in all patients
The mean length of hospital stay in this study was 14.31 days (with a minimum of 1 and a maximum of 107 days). The mean age of patients was 53.3 years with a minimum of 0 and a maximum of 94 years). The number of vials consumed per patient varied from one to 116, and the average vial consumption in patients was 13.32. The average cost of total drug in dollars in the studied patients was $ 1843. The average price of albumin per patient was estimated at $ 553.04. The average cost for insurance was estimated at $ 1290,428. (Table 7).
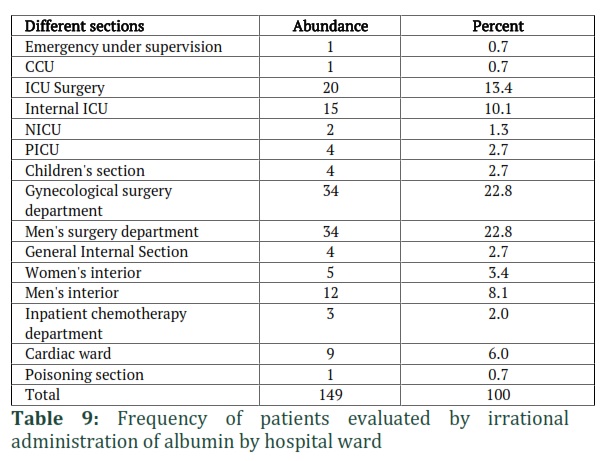
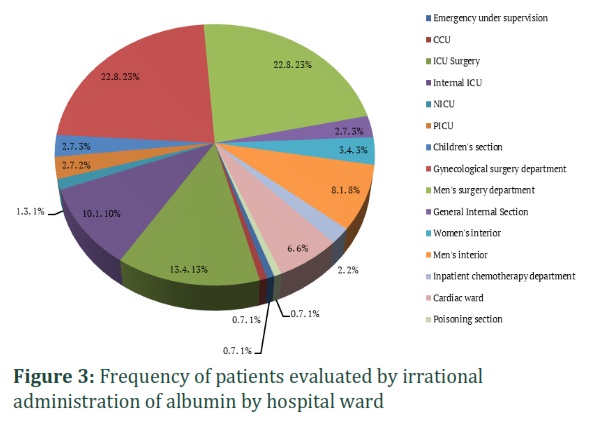
Frequency of patients studied by irrational administration of albumin by hospital ward
The distribution of patients for whom irrational albumin administration was performed in different wards of the hospital and the amount of albumin administration in each ward were evaluated. They were hospitalized with albumin. Then, surgical ICU with (13.4%), internal ICU (10.1%), men's internal medicine ward with (8.1%), cardiac hospitalization (0.6%), women's internal medicine (3.4%), General Internal Medicine, Pediatric Ward and PICU each with (2.7%), Inpatient Chemotherapy Ward (0.2%), NICU (1.3%) followed by Emergency Room, CCU and Poisoning Ward each Were 0.7% (Table 9 and Figure 3).
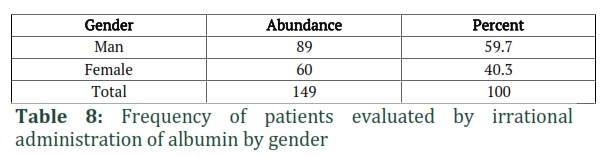
Frequency of patients studied by irrational administration of albumin by gender
In this study, studies performed on all patients described were performed on a group of 149 patients in whom albumin administration was unreasonable to compare the results. 149 patients, including 89 men (59.7%) and 60 women (40.3%) for whom albumin was irrationally prescribed, were studied (Table 8).
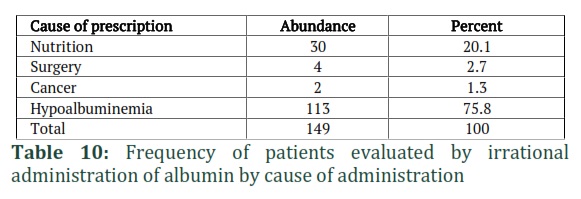
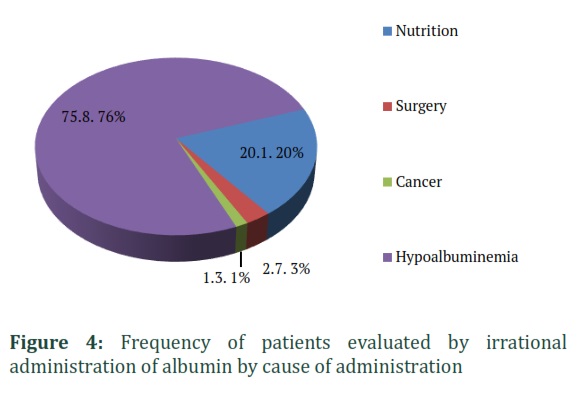
Frequency of drug administration in patients studied with irrational albumin administration
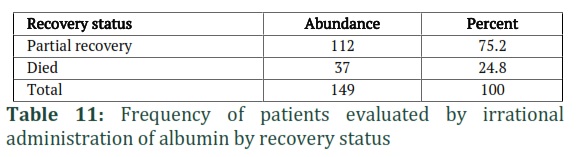
The cause of drug administration was hypoalbuminemia in 75.8% of cases, followed by nutritional causes with 20.1% of cases, surgery with 2.7% of cases, and finally cancers with 1.3% of patients (Table 10 and diagram 4).Frequency of patients evaluated by irrational administration of albumin by recovery status
Regarding the recovery status of patients with irrational albumin administration, 75.2% (112 cases) of these patients improved, and 24.8% (37 cases) died (Table 11).
Frequency of patients evaluated by irrational administration of albumin separately for drug approval by the hospital pharmacist
Out of 149 cases of irrational albumin administration, 141 (94.6%) were not approved by the pharmacist, and only 8 (5.4%) were approved by the pharmacist (Table 12).
Evaluation of hospitalization duration, age, number of vials, and the costs in patients with irrational albumin administration
In this study, the mean length of hospital stay of patients with irrational albumin administration was 17.19 days (with a minimum of 1 and a maximum of 107 days). The mean age of patients was 54.83 years, with a minimum of 0 and a maximum of 94 years. The number of vials consumed per patient varied from one to 115, and the average vial consumption in patients was 7.84. The average total cost of the drug in dollars in the studied patients was $ 1084.87, the average price of albumin per patient was $ 325,434, and the average cost for insurance was $ 759,346. (Table 13).
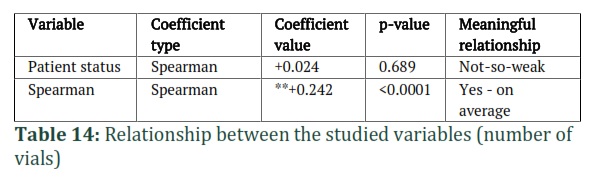
Relationship between the number of vials consumed and the patient's recovery status
This study investigated the relationship between the number of vials consumed and the patient's recovery status. During this study, the Spearman coefficient was evaluated for 0.024 and coherent, so the relationship between these two variables is coherent but weak. Examining the P-value of these two variables, no significant association was found between them (p-value = 0.689) (Table 14).
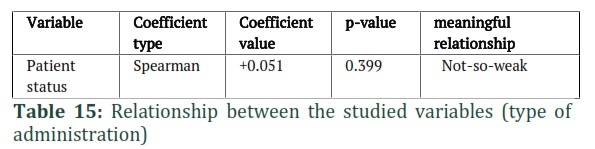
Relationship between the number of vials consumed and the type of prescription
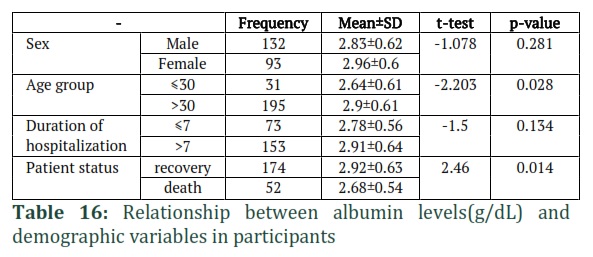
Also, the relationship between the number of vials and the type of administration was investigated. During the studies, the relationship between these two variables with a P-value of less than 0.0001 was significant, and the value of the spearman coefficient equal to + 0.242 indicates a relationship. It is consistent and moderate (Table 14). 16-1-3-R relationship between the type of administration and the patient's condition in the present study, the relationship between the kind of administration and the patient's condition was also examined. Still, the relationship between the two was not considered significant, with P-value = 0.399. Also, the Spearman coefficient, in this case, was equal to +0.051, which indicates a weak and consistent relationship (Table 15).The results showed that the mean albumin level before albumin administration in the study participants was 2.87±0.62 (g/dL). The results did not show a statistically significant difference in the mean albumin level before albumin administration based on gender and length of hospital stay in the study participants (P> 0.05) while the mean albumin level before albumin administration in the age group over 30 years and in patients who had partial recovery were significantly higher (p <0.05).
Figures & Tables

Discussion![]()
Albumin is not a drug that can be used as a calorie-suppressing protein in poor nutritional status or dietary supplements. Iatrogenic increase in blood albumin concentration to more than 4 g/dL increases catabolism in the body. In general, albumin should be prescribed to the patient to improve the balance of albumin synthesis rate and metabolism. Patients may experience severe diarrhea of more than 2 liters per day due to an enteral diet. In these patients, after ascertaining the cause of diarrhea, ruling out other possible causes, and switching diet from antral to parenteral, the blood albumin level should be below Keep 2 grams per deciliter [27-29]. A limited number of extensive controlled studies have been performed to evaluate the accuracy of albumin administration in medical centers and the unnecessary costs of prescribing this drug to patients and insurance companies. These studies differ in terms of design, objectives, and method of implementation [30-33].
In the present study, 271 patients, including 160 men (59.0%) and 111 women (41.0%) who were prescribed albumin, were studied, and out of 271 patients, 209 (77.1%) were Recovered, and 69 patients (22.9%) died. The primary purpose of this study was to evaluate the consumption and rationality of albumin administration in patients admitted to Shahid Rahimi Hospital in Khorramabad. In order to determine the distribution of patients in different wards of the hospital and the amount of albumin administration in each ward, it was found that the two wards of gynecological surgery and male surgery each with a frequency of 41 patients (15.13%) and CCU wards, ward. The pediatric emergency department, outpatient chemotherapy ward, poisoning ward, and neonatal ward had the frequency of one patient (0.37%) and had the highest and lowest percentages of patients admitted with albumin administration. The studies performed for all the patients described were also performed for a group of 149 patients in whom albumin administration was unreasonable to compare the results. In this study, 149 patients, including 89 men (59.7%) and 60 women (40.3%), for whom albumin drug was irrationally prescribed, were studied, and 75.2% (112 cases) were recovered. These patients improved, and 24.8% (37 cases) of them died. The two wards of gynecological surgery and male surgery each had a frequency of 34 patients (22.8%). Poisoning was 0.7% each. As described, both in the general examination of patients and in patients with irrational administration of albumin, it was found that the most use of albumin was in surgical wards (men and women). Therefore, in cases of albumin requests for patients admitted to these wards should be done with more supervision by the pharmacist.
Further monitoring will reduce the consumption of this vital drug and the costs incurred by patients and insurance companies. In addition, if each drug discussed in this study, albumin, is prescribed correctly and rationally, health services will be more effective for patients with fewer side effects. They will increase the quality of treatment and increase patient satisfaction. In the discussion of costs imposed on the patient and insurance companies in this study, the number of vials consumed per patient varied from one to 116, and the average vial consumption in patients was 13.32. The average cost of prescription drugs was estimated at $ 1843.46. The average price of albumin per patient was $ 553.04, and the average cost of insurance was estimated at $ 1290,428. In the group that prescribed albumin to irrational patients, the average cost of prescribed drugs was estimated at $ 1084.78. The average cost of albumin for a patient was $ 325.43, and the average insurance price was $ 759,346. As it is known, a very high fee is paid by patients due to irrational albumin administration, so that out of $ 250,711.73 total albumin administration for 3611 albumin vials, only $ 112870.42 (45.02%) of the total cost is spent on rational albumin administration and 54.98% The total consumption of albumin, i.e., 137841.31 dollars, is due to irrational prescriptions. These high costs will be reduced with more supervision, and the difference can be spent on creating better quality insurance benefits for patients. As previously described, in this study, no significant relationship was observed between the number of vials consumed and the state of improvement (P-value = 0.689), and the relationship between these two variables was evaluated as weak (Spearman coefficient equal to 0.024). From this, it can be fortunately concluded that the irrational administration of albumin to patients does not overshadow their recovery status and is not life-threatening for patients. However, it can expose patients to side effects without receiving therapeutic effects of albumin.
Also, the relationship between the number of vials and the type of administration was investigated. During the studies, the relationship between these two variables was significant (P-value less than 0.0001), and the spearman coefficient value equal to + 0.242 indicates a relationship. Alignment and intermediate communication. This suggests that in cases where patients have been given irrational prescriptions, albumin consumption is higher, and this shows the need for more control of pharmacists in prescribing this drug because although defining albumin for patients is not life-threatening. Still, consumption and its irrational administration have no therapeutic effects for the patient, but the patient is at risk of side effects of albumin and has a heavy financial burden for the health care system and the patient himself. In the present study, the relationship between the type of administration and the patient's condition was also examined, but the relationship between the two was not considered significant, with a P-value of P-0.399. Also, the spearman coefficient in this case was equal to +0.051, which indicates a weak and consistent relationship.
In conclusion, the process of administration of albumin in Shahid Rahimi Hospital in Khorramabad was not desirable and the adoption of policies such as adherence to the standard protocol Regarding the logical prescription of albumin, it can be helpful. Albumin is an expensive medication prescribed unnecessarily for many patients. Using the clinical pharmacist's prepared guideline could minimize the situations where its administration is not needed. The obtained results indicate the need to review and monitor the prescription of clinically important drugs, by preparing an in-hospital protocol, and the need to establish a pharmaceutical care department in the hospital in order to promote the rational prescription of drugs.
![]()
Author Contributions
Hadi Hayati Abbarik, Arian Karimi Rouzbahani: Data analysis
Vahid Rahimi, Fanak Fahimi, Javad Ghasemian Yadegari: Monitoring of research
Waleed K. Khawaja, Noora M. Hameed, Mohammad Karimi: Drafting
Hadi Hayati Abbarik, Arian Karimi Rouzbahani, Zahra Heydari, Ali Kharazmkia: Manuscript scanning
Vahid Rahimi, Fanak Fahimi, Javad Ghasemian Yadegari, Hadi Hayati Abbarik, Arian Karimi Rouzbahani, Zahra Heydari, Ali Kharazmkia: Data evaluation
References
- Talasaz AH, Jahangard-Rafsanjani Z, Ziaie S, et al. Evaluation of the Pattern of Human Albumin Utilization at a University Af-fliated Hospital. Archives of Iranian Medicine, (2012); 15(2): 85-87.
- http://fda.gov.ir/item/463 [Internet]. 2019. Available from: http://fda.gov.ir/item/463
- Abbas KM, Al-Rahmanny AHJ. Toxic effects of various oil concentrations obtained from Rosmarinus officinalis on Musca domestica adults (Diptera: Muscidae) in different time periods. Caspian Journal of Environmental Sciences, (2022); 20(2): 401-405.
- Kleinman ME, Chameides L, Schexnayder SM, et al. Part 14: Pediatric advanced life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation, (2010);122(3):876–908.
- Ebrahimi Y, AL-Baghdady HFA, Hameed NM, Iswanto AH, Shnain Ali M, Hammoodi HA, Hashim Kzar H, Aravindhan S, Khodaei SM, Alikord M, Pirhadi M. Common fatty acids and polyphenols in olive oil and its benefits to heart and human health. Caspian Journal of Environmental Sciences, 2022; 1-7.
- Caraceni P, Angeli P, Prati D, et al. AISF-SIMTI position paper: The appropriate use of albumin in patients with liver cirrhosis. Blood Transfusion, (2016);14(1):8–22.
- Benetti G, Rosi S, Romano A, et al. Terlipressin given by continuous intravenous infusion versus intravenous boluses in the treatment of hepatorenal syndrome: A randomized controlled study. Hepatology, (2015);63(3):983–92.
- Ortega R, Ginès P, Uriz J, et al. Terlipressin therapy with and without albumin for patients with hepatorenal syndrome: Results of a prospective, nonrandomized study. Hepatology, (2002);36(4 I):941–8.
- Rodés J, Soriano G, Guevara M, et al. Terlipressin and Albumin vs Albumin in Patients With Cirrhosis and Hepatorenal Syndrome: A Randomized Study. Gastroenterology, (2008);134(5):1352–9.
- Brierley J, Carcillo JA, Choong K, et al. Clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine. Critical Care Medicine, (2009);37(2):666–88.
- Romanelli RG, La Villa G, Barletta G, et al. Long-term albumin infusion improves survival in patients with cirrhosis and ascites: An unblinded randomized trial. World Journal of Gastroenterology, (2006);12(9):1403–7.
- Giefer MJ, Murray KF, Colletti RB. Pathophysiology, diagnosis, and management of pediatric ascites. Journal of Pediatric Gastroenterology and Nutrition, (2011); 52(5): 503–13.
- NIEUWKAMP GA. Ovarian hyperstimulation syndrome. Emergency Medicine [Internet], (1994); 6(1):8-11.
- Venetis CA, Kolibianakis EM, Toulis KA, et al. Intravenous albumin administration for the prevention of severe ovarian hyperstimulation syndrome: A systematic review and metaanalysis. Fertil Steril, (2011); 95(1): 188-196.3.
- Pfeifer S, Butts S, Dumesic D, et al. Prevention and treatment of moderate and severe ovarian hyperstimulation syndrome: a guideline. Fertil Steril, (2016); 106(7): 1634–47.
- Jee BC, Suh CS, Kim YB, et al. Administration of intravenous albumin around the time of oocyte retrieval reduces pregnancy rate without preventing ovarian hyperstimulation syndrome: A systematic review and meta-analysis. Gynecologic and Obstetric Investigation, (2010); 70(1): 47–54.
- Bellver J, Muñoz EA, Ballesteros A, et al. Intravenous albumin does not prevent moderate-severe ovarian hyperstimulation syndrome in high-risk IVF patients: A randomized controlled study. Human Reproduction, (2003); 18(11): 2283–8.
- Angeli P, Volpin R, Gerunda G, et al. The treatment of the type 1 hepatorenal syndrome (HRS) with the combined administration of midodrine and octreotide. Journal of Hepatology, (1998); 28:70.
- Romanelli RG, La Villa G, Barletta G, et al. Long-term albumin infusion improves survival in patients with cirrhosis and ascites: An unblinded randomized trial. World Journal of Gastroenterology, (2006) ;12(9): 1403–7.
- Moore KP, Wong F, Gines P, et al. The management of ascites in cirrhosis: Report on the consensus conference of The International Ascites Club. Hepatology, (2003); 38(1): 258–66.
- Vermeulen Jr LC, Ratko TA, Erstad BL, et al. A Paradigm for Consensus: The University Hospital Consortium Guidelines for the Use of Albumin, Nonprotein Colloid, and Crystalloid Solutions. Archives of Internal Medicine [Internet], (1995); 27;155(4):373–9.
- Abd Elaal MM, Zaghloul SG, Bakr HG, et al. evaluation of different therapeutic approaches for spontaneous bacterial peritonitis. Arab Journal of Gastroenterology [Internet], (2012);13(2):65–70.
- Ring J, Messmer K. INCIDENCE AND SEVERITY OF ANAPHYLACTOID REACTIONS TO COLLOID VOLUME SUBSTITUTES. Lancet [Internet], (1977); 26 [cited 2019 Mar 1];309(8009):466–9.
- Kappos L, Radue E-W, O’ Connor P, et al. New England Journal. The New England Journal of Medicine, (2010);362(5):387–401.
- Hemolysis Associated with 25% Human Albumin Diluted with Sterile Water -United States, 1994-1998, (1994).
- Mihara E, Hirai H, Yamamoto H, et al. "Active and water-soluble form of lipidated Wnt protein is maintained by a serum glycoprotein afamin/α-albumin".eLife.Feb, (2016); 5:44-63.
- Erstad BL, Gales BJ, Rappaport WD. The use of albumin in clinical practice. Archives of Internal Medicine, (1991); 151: 901 – 911.
- Vermeulen Jr LC, Ratko TA, Erstad BL, et al. A Paradigm for Consensus: The University Hospital Consortium Guidelines for the Use of Albumin, Nonprotein Colloid, and Crystalloid Solutions. Archives of Internal Medicine [Internet], (1995); 27;155(4):373–9.
- Guthrie RD, Hines C. Use of intravenous albumin in the critically ill patient. American Journal of Gastroenterology, (1991); 86: 255-263.
- Virgilio RW, Rice CL, Smith DE, et al. Crystalloid vs. colloid resuscitation: Is one better? A randomized clinical study. Surgery, (1979); 85: 129 – 139.
- Golub R, Sorrento JJ, Cantu RJ, et al. Efcacy of albumin supplementation in the surgical intensive care unit: a prospective, randomized study. Critical Care Medicine, (1994); 22: 613-619.
- Rubin H, Carlson S, DeMeo M, et al. Randomized, double-bind study of intravenous human albumin in hypoalbuminemic patients receiving total parenteral nutrition. Critical Care Medicine, (1997); 25: 249-252.
- Salerno F, Badalamenti S, Lorenzano E, et al. Randomized comparative study of hemaccel vs. albumin infusion after total paracentesis in cirrhotic patients with refractory ascites. Hepatology, (1991); 13: 707 – 713.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0