

Review Article
Deciphering the Potential Therapeutic Intervention Points of 2019-nCoV: A Pharmacological Perspective
Asma Khurshid1*, Rashid Amin2*, Athar Aziz3, Omema Ahmed4, Mahmoud E. F. Abdel-Haliem2,5
Adv. life sci., vol. 9, no. 4, pp. 412-428, December 2022
*– Corresponding Author: Asma Khurshid (Email: asma.khurshid@duhs.edu.pk)
Authors' Affiliations
2. Department of Biology, College of Sciences, University of Hafr Al Batin, Hafar Al-batin – Saudi Arabia
3. School of Environment and Life Sciences, Biomedical Research Centre University of Salford – United Kingdom
4. Department of Computer Science, Habib University, Karachi – Pakistan
5. Botany and Microbiology Department, Faculty of Science, Zagazig University, Zagazig – Egypt
[Date Received: 09/04/2022: Date Revised: 26/10/2022; Date Published: 31/12/2022]
Editorial Note: This article has post-publication modifications in authors’ sequence.
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
The emerging and re-emergence of viral outbreaks in the history of mankind has always pose severe global intimidation to public health and economy. The debilitating effects of 2019-nCoV (2019 novel coronavirus) outbreak has swiftly spread worldwide due to its highly contagious nature with severe risk of respiratory tract infections and higher mortality rate, necessitating the urgent need for the production of effective vaccine and potential therapeutic agents. The active evolution of SARS-CoV-2 strain in different population and environment strive immense challenge against anti-viral therapeutic development based on viral pathogenicity. The potential FDA drugs are evaluated based on their known safety and efficacy with exceptional pharmacokinetic profiles for the treatment of nCoV-2019. Existing knowledge related to MERS-CoV and SARS-CoV epidemic has provided a better understanding to explore purposeful therapeutics strategies against novel coronavirus disease (COVID-19). To limited extend, the ongoing promising and hopeful treatments includes convalescent plasma therapy, remdesivir, lopinavir/ritonavir, ACE inhibitors, TMPRSS2 inhibitors, hydroxychloroquine, interferon, ribavirin, tocilizumab, and corticosteroids however clinical efficacy of some of them need to be validated in randomized clinical trials (RCTs). The global struggle to make a protected and successful Coronavirus immunization is finally proving to be fruitful. Although challenges such as strain variation resistant, possible side effects, adequate supply of vaccines to all countries and limited availability of second dose still diverting the option of possible efficacious therapeutics strategies to work alongside with vaccine development with improved efficacy and safety profile. This review is focused on the potential advancement in therapeutic approaches with possible repurposing of the available drugs and explores the current status of available vaccines with hope that these strategies found to be cogent in controlling SARS-CoV-2 outbreak.
Keywords: Coronavirus disease 2019 (COVID-19); Remdesivir; Therapeutics; Plasma therapy; Hydroxychloroquine; Anti-viral; Angiotensin-converting enzyme 2; Type II transmembrane serine protease
Introduction![]()
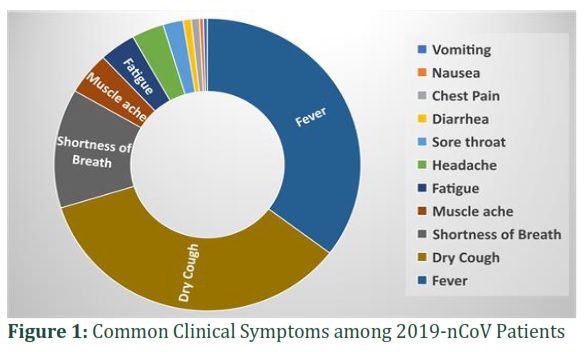
The SARS-CoV-2 virus affects with greater infectivity than the SARS-CoV pandemic of 2003. SARS-CoV-2 outbreak with all efforts still sprouting with so far globally confirmed cases exceed more than 264 million people with global deaths of 5.2 million so far [1]. In December 2019, cases of viral pneumonia emerged in Wuhan, (the capital city of Hubei province) China caused by some unknown etiology linked to be found with a seafood and animal market in Wuhan [2]. From airway epithelial cells of infected patients, the virus was isolated and upon genome sequencing, it was identified as a novel coronavirus belongs to family of Coronaviridae [3]. The novel new member of a viral family on 12th of January 2020 was named as 2019 novel coronavirus (2019-nCoV), which later on, officially renamed on 12th February 2020 as coronavirus disease 2019 (COVID-19) [2]. Later, this novel virus was termed as “the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)” by the International Committee on Taxonomy of Viruses (ICTV) [4,5]. Since its first reported case on 1st of December 2019, the infection rate has increased exponentially among the susceptible population, and it suddenly spread all over the world as a major global threat [6]. In February 2020, WHO represent a Public Health Emergency of International Concern because of COVID-19 pandemic upon confirmation of human-to-human transmission of COVID-19 [7]. The high rate of mortality and morbidity of SARS-CoV2 infection has been observed among immunocompromised individuals due to old age and weaken immune system with underlying complications, including diabetes, cardiovascular disease, hypertension and HIV infection [2,8,9]. The 80% of confirmed patients from this group were among 30 to 80 years of aged [10]. In general population the major clinical manifestations of the SARS-CoV-2 infection as illustrated in figure 1, includes dry cough, loss of smell and taste, myalgia, fatigue, septic shock, headache, diarrhea, fever, shortness of breath, nausea, vomiting, abdominal discomfort specially in immunosuppressed patients followed by the general reported complications multi-organ failure, pneumonia, RNAaemia, neurological complications, acute respiratory distress syndrome (ARDS) even death [2,11-14].
Methods![]()
Literature Search Strategy and Selection Criteria
A systematic search was carried out from PubMed, Google Scholar, Google Web Browser, online COVID databases for relevant papers by providing key terms SARS-CoV-2, therapeutics of COVID-19, COVID-19 vaccine, molecular biology of SARS-CoV-2, current data on COVID-19, COVID vaccination data, epidemiological and clinical characteristics of coronavirus, specific therapies in COVID-19, SARS-CoV-2 receptor, Dexamethasone for COVID-19, Bacteriophages and coronavirus, COVID-19 VACCINE TRACKER etc. The literature was screened in detailed and dept analysis was performed for the specific information for the inclusion of relevant contents according to the required information. In this study, 113 peer reviewed research articles and 18 websites were selected.
According to the Chen et al study the most commonly observed clinical symptoms based on 99 hospitalized COVID-19 patients is being depicted in the graph. The three most commonly found symptoms include fever, dry cough and shortness of breath followed by muscle ache and fatigue [15].
Pathophysiology of SARS-CoV-2
SARS-CoV-2 contains a positive-sense single-stranded RNA genome of approximately 120 nm in diameter. The seventh coronavirus which infect humans is SARS-CoV-2 classified as beta-coronavirus (βCoV) genera that can results severe acute respiratory syndrome [6,16]. Till 2019, six coronaviruses can cause infections in human and leads to respiratory diseases were identified: HCoV-229E, HKU1, HCoV-NL63, HCoV-OC43, MERS-CoV, SARS-CoV [17]. Genome analysis of SARS-CoV-2 at initial phase of pandemic reveals 79.6% sequence similarity with SARS-CoV and 50% with MERS- CoV although it is found to be (96.2%) identical to Bat-CoV RaTG13, all human coronaviruses are human origin [2]. Therefore, it has been speculated that bats might be the possible hosts for SARS-CoV-2 infection in humans, however the possibility of transmission to any intermediated host still needs to be explored [7].
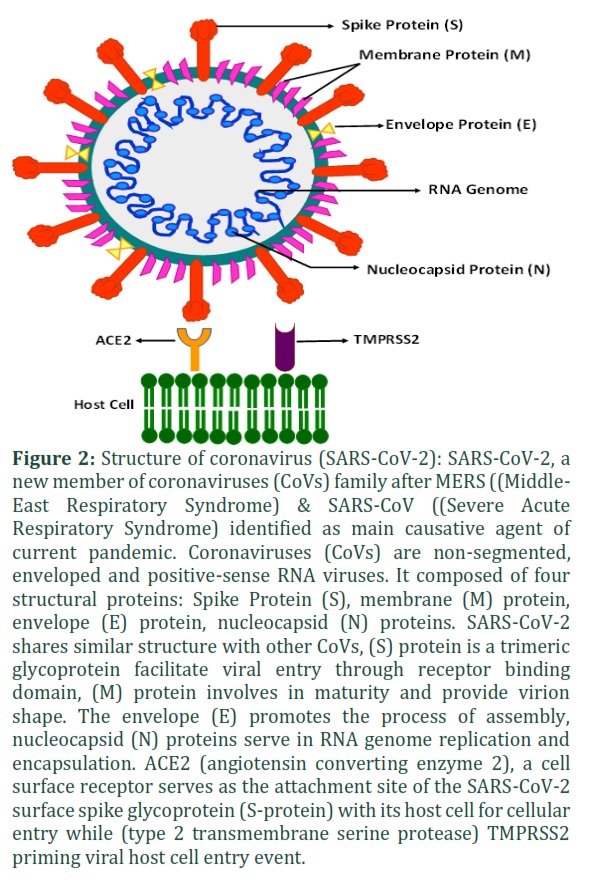
Like other RNA viruses, the envelope of novel corona virus also comprised several glycoproteins with RNA genome in the core, as figure 2 summarizes the basic structure of novel coronavirus highlighting its major structural proteins. Among the four structural proteins of SARS-CoV-2, spike glycoproteins (S) upon binding to angiotensin-converting enzyme 2 (ACE2) receptor on human alveolar epithelial cells facilitate viral entry [3,18]. SARS-CoV-2 targets its host cells through the viral spike protein type I membrane glycoprotein that binds to the ACE2 receptor. The virus also requires the host cell co-receptor (type 2 transmembrane serine protease (TMPRSS2)) to facilitate its entry into the alveolar wall of the respiratory system through the type II pneumocyte, followed by the endocytosis into the pneumocyte cytoplasm [19]. The viral lipid bilayer will break down by host cell lysosomal enzymes in a process called uncoating. By using the RNA-dependent RNA-polymerase of the host cell, the viral structural proteins and genome has been replicated inside the type II pneumocyte, this is followed by budding off of the SAR-CoV-2 and destroying the type II pneumocytes. This results in the release of cytokines such as interleukin-6 (IL-6), interleukin-1 (IL-1), tissue necrosis factor alpha (TNF-α) by monocytes and macrophages thus causing clinical manifestations such as systemic manifestations that includes acute inflammation, fever and smooth muscle dilation [20]. It is now considered that the main mortality cause among susceptible patients is due to pro-inflammatory cytokine storm or may because of secondary bacterial infections. Thus, ongoing research is exploring different therapies for the treatment of cytokine storm, which could be fatal due to multi-organ dysfunction syndrome in patients specifically undergo to major surgery, trauma, sepsis and cardiopulmonary bypass leads to a systemic inflammatory response Syndrome (SIRS). Therefore, drugs inhibiting the IL-1 receptor is considered as a potential treatment for COVID-19 patients [21].
Deciphering the Virus behind the Pandemic
In SARS-CoV-2 S1 subunit C-terminal domains (CTD) possess strong binding affinity for human ACE2 (hACE2). The receptor-binding domain (RBD) within SARS-CoV-2 CTD is responsible for binding with hACE2 receptor with greater affinity compared to SARS-CoV RBD [3,22]. Despite the zoonotic origin of the virus through natural evolution, there is still some controversy related to the viral origin due to the direct interaction of the spike protein (S) with the human receptor (ACE2) implying human-to-human transmission in a limited time followed by evolution [14]. According to a study carried, out of 99 infected patients (32 women and 67 men all found to be infected) while 49 patients had an exposure history of Huanan seafood market. The remaining 50 (51%) patients suffers with chronic diseases [15]. The sequence of SARS-CoV-2 virus obtained from Wuhan, China; in December 2019 has been compared with the viral genome sequence collected in April 2020 from North America demonstrating to be different. As viruses can rapidly evolve and adapt among the different human population and environment, it could also be susceptible to previous or other human coronaviruses and recombinational events of SARS-CoV-2. So far three genetic varieties of the virus have been revolving globally [23]. SARS-CoV-2 possess the largest genome (∼30 kb) in size among RNA viruses. As an RNA virus the high mutation rate of SARS-CoV-2 is due to its natural genetic variability. To fully elucidate the evolving mechanism of SARS-CoV-2 for its potential binding to human receptors it is crucial to disentangle the zoonotic transfer of coronavirus among species and infer the prevalence of viral infection among susceptible populations [24]. Based on immunological and genetic limitations among various populations it is possible that SARS-CoV-2 evolution could be altered due to replication environments. However due to evolutionary strain, the SARS-CoV-2 will continue to keep mutating [4].
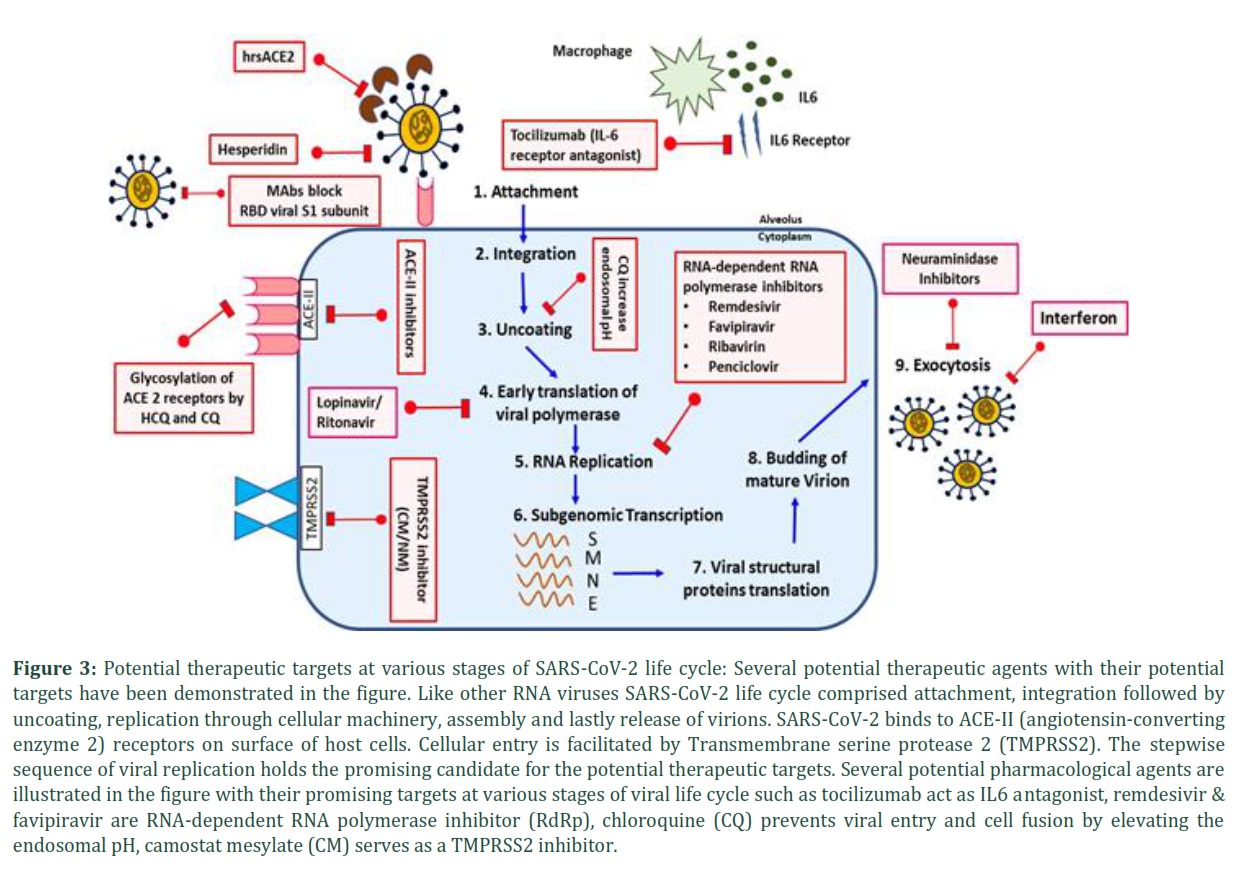
Possible Pharmacological Targets
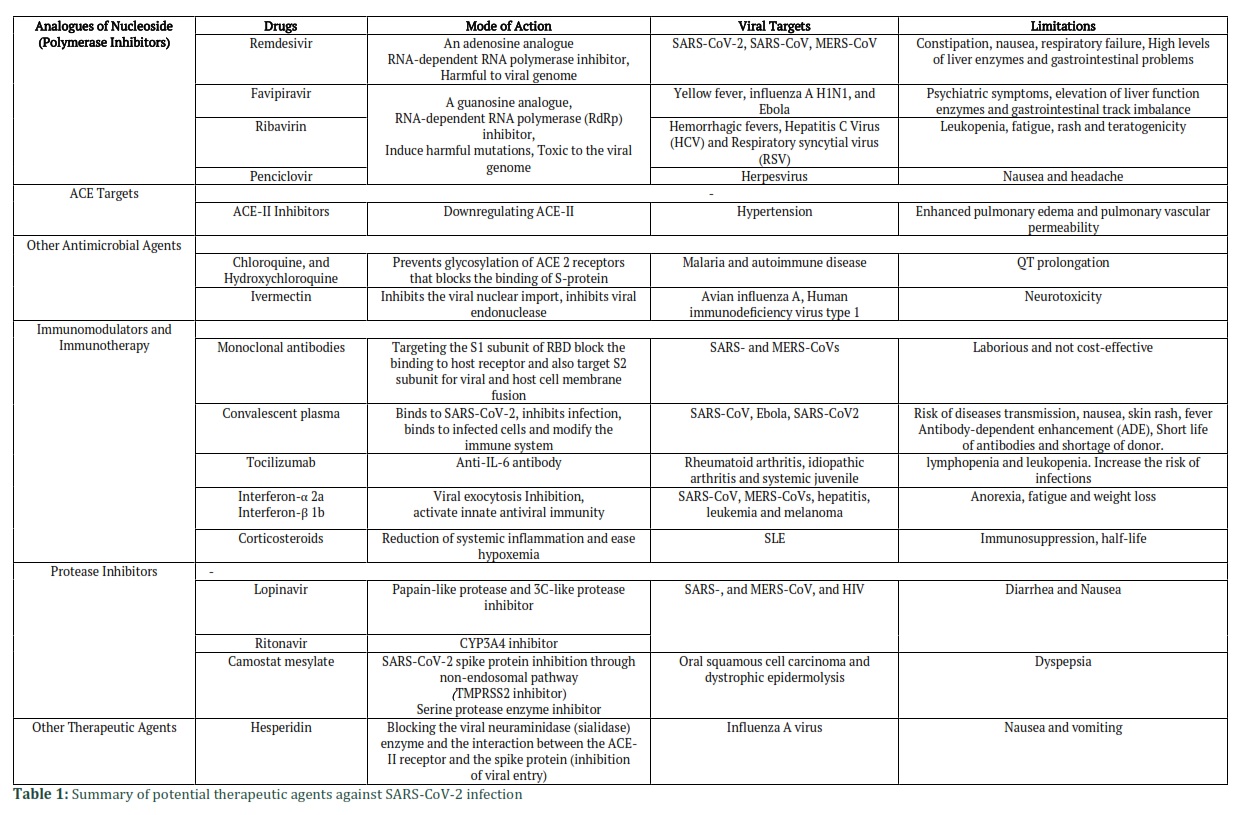
As a new member of viral family, it is a long journey to uncover and explore the facts about SARS-CoV-2. However, limited broad-spectrum antiviral drugs have been tested against COVID-19 infection in clinical trials, resulting in clinical recovery, but due to their side effects some drugs were withdrawn. Several aspects need to be considered such as the host response, the active viral components and the key pathway players for cell entry. Some of the potential therapeutic targets during viral life cycle are depicted in figure 3. Despite being closely related to SARS-CoV and MERS in terms of clinical features and genetic identity, several previously used drugs on SARS-CoV and MERS have been tested against SARS-CoV-2 targeting the variable stages in the lifecycle of SARS-CoV-2 [25], The possible targets to be considered for anti-viral drug or vaccine designing would be the host and viral attachment site or blocking the viral entry into the host cells. The cellular entry of SARS-CoV-2 is linked to the viral spike proteins to receptors, priming event of S protein by host proteases (TMPRSS2), ACE2 (angiotensin-converting enzyme 2). The S spike glycoprotein of SARS-CoV-2 is a potential target because neutralizing antibodies are usually guided towards it. Targeting the crucial process of viral replication, exocytosis and budding could be promising targets for anti-viral treatments. The binding of ligands or mABs prevent the interaction of viral receptor to the host cell that potentially inhibits the viral entry [21]. Many anti-influenza drugs have been taken into account because of the resemblance among respiratory viruses in terms of viral entry into host cell, uncoating, and replication [26]. Herein, potential therapeutics (such as antiviral agents and anti-inflammatory agents) are discussed with associated challenges and their efficacy in combating the SARS-CoV-2 based on available literature as summarized in table 1.
Expected risk Associated with Potential Therapeutic Approaches
RNA-dependent RNA polymerase inhibitors (Nucleoside Analogues): Remdesivir (RDV)
Remdesivir so far considered to be the most clinically successful drug against SARS-CoV-2. The broad-spectrum activity of Remdesivir was evaluated against filoviruses, paramyxoviruses, pneumoviruses, Nipah viruses, Ebola viruses, SARS-CoVs and MERS [27-29]. Remdesivir is an adenosine analogue works by inhibiting the viral replication through targeting the RNA-dependent RNA polymerase (RdRp) cause premature termination of viral RNA transcription [30,31]. The nsp12 residue is the potential binding site of remdesivir on RNA-dependent RNA polymerase (RdRp). In case of any mutation on nsp12 due to continuous evolving of virus, it is speculated that remdesivir may become resistance [32]. Remdesivir is a phosphoramidate prodrug and found to reduce the recovery time for individuals with SARS-CoV-2. However, the evidence which proven its role in reducing the mortality is still lacking [24]. Remdesivir recently found to be potent against COVID-19 in vivo [33]. According to an in vitro study remdesivir in combination with emetine was found to shrink the viral load by 65% [34]. Many RCT are being conducted to access the safety and efficacy of RDV among COVID-19 patients. Remdesivir has been proven to be more beneficial for patients not taking invasive ventilation with a mortality rate of 5% in contrast with patients taking invasive ventilation with a mortality rate of 18% [35]. As reported, a remdesivir study was conducted from January 25, 2020, until March 7, 2020, in challenging hospitalized patients for 10 days in which 200 mg was intravenously administered on first day followed by 100 mg daily for the next 9 days [36,37]. Reported side effects include constipation, nausea, respiratory failure and gastrointestinal problems [4,31,38].
Favipiravir
Favipiravir is a guanine analogue and RNA dependent RNA polymerase (RdRP) inhibitor, it works by introducing hazardous mutations in the viral genome [39]. In the active phosphoribosylated form, Favipiravir has been identified as a viral RNA polymerase substrate in several viruses [40]. Favipiravir has proven to be an effective antiviral agent against Ebola, A H1N1, influenza yellow fever and Ebola [41,42]. In China, Favipiravir was approved in March 2020 for the treatment of SARS-CoV-2 [4]. In patients taking Favipiravir some notable side effects were observed such as psychiatric symptoms, elevation of liver function enzymes and gastrointestinal track disturbance [43,44].
Ribavirin
Since 1980 Ribavirin was used for the treatment of respiratory syncytial virus among children [45]. The FDA approved the guanosine analogue ribavirin as a prodrug found to be effective against viral hemorrhagic fevers, Hepatitis C Virus (HCV) and Respiratory syncytial virus (RSV) infection usually along with interferon (IFN-α2b) [24,46]. Ribavirin in combinational therapy showed promising results against COVID-19 patients through inhibition of viral RdRp finally blocking the function of viral protein [47]. However, studies related to its safety need to be investigated further. The major side effect which limits its use against SARS-CoV-2 is due to the reduction in hemoglobin concentration in patients with respiratory disorders [24].
Penciclovir
Penciclovir is a guanosine analogue, previously reported to block the activity of herpes DNA polymerase enzyme against herpes viruses to prevent viral replication. It was among the first agent tested for SARS-CoV-2 infection. In in vitro studies, penciclovir showed relatively low level of efficacy against SARS-CoV-2 infection. In another study on penciclovir promising outcome was observed by preventing the activity SARS-CoV-2 RNA-polymerase indicating its role to be explored further in clinical trials [48,49]. Although due to its safety concerns in breastfeeding and pregnancy associated with nausea and headache, limitation in oral absorbance and uptake are some of the major side effects limiting its use [50].
Protease Inhibitors
TMPRSS2 inhibitor
Another fascinating strategy is targeting the spike protein of SARS-CoV virus that play a critical part in facilitating the viral entry into the target cells seems to be promising approach in many in vitro studies. In order to proceed for the infectious viral entry, cleavage and activation are the key steps of the SARS-CoV spike protein through the host cell’s proteases, which could be TMPRSS2 (Type II transmembrane serine protease). TMPRSS2 investigated as a potential antiviral agent due to its potential to cleave and activate the spike protein of SARS-CoV. It is well documented here that TMPRSS2 is used by SARS-CoV-2 for S protein priming [51]. Previously cysteine PI K11777 showed favorable efficacy against MERS-CoV and SARS-CoV in 293T, (expressing ACE2) or CD13, or Vero cells [52,53]. Study conducted on Caco-2 and Vero-TMPRSS2 cells, the use of camostat mesylate an approved potent serine protease inhibitor partially prevents the spike-driven entry of SARS-CoV-2. According to the recent study clinically tested serine protease inhibitor camostat mesylate has found to partially prevent the SARS-CoV-2 spike mediated cellular entry by showing its activity against TMPRSS2 into Vero-TMPRSS2 and Caco-2 cells [20,51,54]. Although further in vivo and in vitro studies are required to explore the mechanism of camostat mesylate as a potential antiviral agent against SARS-CoV-2 [54]. Some other related drugs such as nafamostat could potentially be considered as an antiviral agent against SARS-CoV-2 patients for off label treatment [51,55].
Lopinavir/Ritonavir
Lopinavir/ritonavir demonstrates as a promising candidate against MERS-CoV in tissue culture model although further investigations required to explore regarding its efficacy and safety despite its ability in reducing the progression of the disease in marmosets [56,57]. Lopinavir/ritonavir as an protease inhibitor works as combination therapy found to be effective against HIV [58]. Based on previous clinical studies on SARS patients lopinavir-ritonavir therapy considered as a potential therapeutic agent against SARS-CoV-2. However no significant result has been achieved so far on clinical data obtained from COVID-19 patients therefore there is an vital need of a well-controlled and more customized clinical studies against COVID-19 [45,59].
ACE (Angiotensin-converting enzyme) inhibitors
According to the recent study conducted on non-survivors of COVID-19, particular comorbidities include diabetes and cerebrovascular disease [5]. As reported, these types of patients were generally treated with angiotensin II type I receptor blockers (ARB) or ACE inhibitors [60]. The binding of the surface spike glycoprotein (S- protein) of SARS-CoV-2 and SARS-CoV is facilitated by epithelial cells (intestine, lung, and kidney) expressed ACE2 receptors. Without the presence of acute respiratory distress syndrome (ARDS), under strict monitoring of ARB or ACE, inhibitors are considered as a potential treatment against SARS- CoV infection [4]. SARS-CoV-2 utilizes ACE-II receptor as a primary receptor and the lung tissue decreased in expression of ACE-II could possibly indicate the major source of lung injury deal by SARS-CoV-2 [61]. For COVID-19 patients, the use of ACE-II inhibitors was suggested as it is presenting a potential agent among hypertension patients in decreasing the morality and pulmonary inflammatory response [62]. The binding affinity of human SARS-CoV-2 spike protein with ACE II receptor is more compared to SARS-CoV. Recently, a novel therapeutic strategy of human recombinant soluble ACE2 (hrsACE2) found to prevent the entry of SARS-CoV-2 into the host cell thus reduces the viral load but possibly only in early stage patients [63,64].
Antimicrobial Agents
Hydroxychloroquine, Chloroquine and Azithromycin
For more than 50 years, hydroxychloroquine (HCQ) and chloroquine (CQ) have been used widely for the treatment of malaria and autoimmune diseases. Chloroquine is a derivative of 4-aminoquinoline and reported as anti-infective (including anti-bacterial, anti-parasite, anti-viral, and anti-fungal), immunomodulating, anti-thrombotic, anti-tumor, and metabolic effects anti-infection (including anti-parasite, anti-bacterial, anti-fungal and anti-viral), anti-thrombotic and metabolic effects. Chloroquine is found to be useful against viral infections in in vitro studies however results are not very hopeful in clinical trials and animal studies of chloroquine [65,66]. It has been found to be effective against influenza A and B virus in vitro [67,68], COVID-19 [69], HIV-1 [70,71] and SARS COV-1 [72,73]. Multiple mechanisms have been suggested related to antiviral activity of Chloroquine. It blocks virus and cell fusion by increasing the acidic endosomal pH (ranges from 4-7). In addition to this, it also prevents the glycosylation of the angiotensin-converting enzyme 2 (ACE 2) receptors that ultimately block the binding of S-protein. Entry of the virus into the cells is facilitated by ACE 2 receptor [4,74]. Chloroquine serves as a zinc ionophore and reported to increase the intracellular levels of zinc that ultimately permit the entry of zinc into the cells. This results in inhibiting the activity of RNA-dependent RNA polymerase [75]. In vitro chloroquine is found to be effective against SARS-CoV-2. It has been proposed that low dose of hydroxychloroquine in combination with anti-inflammatory drug could be effective in severely ill patients at late stages of SARS-CoV-2 infection by controlling the cytokine storm due to its immunomodulatory effect. However, the efficacy of hydroxychloroquine found to be more effective compared to chloroquine in autoimmune conditions [5,76]. Although patient allergic with hydroxychloroquine or with retinopathy, pregnant or breastfeed is strictly prohibited. Its adverse effects have found on hepatic and renal systems. Adverse reactions of chloroquine phosphate tablets have been reported in a clinical trial conducted on SARS-CoV-2 patients [77].
Azithromycin is considered to be a potent agent against severe respiratory tract infections in patients dealing from viral infections. The clinical trial of azithromycin in combination with hydroxychloroquine recently shows better efficiency in viral elimination against SARS-CoV-2 in Chinese patients [78]. The administration of hydroxychloroquine, chloroquine and azithromycin required special care and designed for effective monitoring on selected patients against SARS-CoV-2 infection [79].
Ivermectin
Ivermectin has been recognized as an antiparasitic agent and known to be efficient against broad range of viral infections in vitro. The anti-viral studies of ivermectin have been reported against many RNA viruses including Avian influenza A, Human immunodeficiency virus type 1, Yellow fever, Dengue fever, Zika etc. The proposed mechanism of action is through blocking the importin (IMP) α/β receptor, which plays crucial role in carrying viral proteins into the nucleus of host cell [80]. It is a broad-spectrum drug that found to be effective against dengue virus infection upon oral administration. In-vitro studies of Ivermectin has been found to be effective against SARS-CoV-2 in reducing the viral RNA up to ~5000-fold for 48 hours. Due to its efficacy ivermectin could be a potential candidate against SARS-CoV-2 infection however its definite mechanism of action is currently under investigation. Due to its potential as an antiviral agent against SARS-CoV-2 there is an immense need for further investigation in humans [20,81].
Immunotherapy and Immunomodulators
Corticosteroids
Corticosteroids possess immunosuppressive and anti-inflammatory properties serving as a good candidate in diminishing the effects of pneumonia. It has been also found to be potent against ARDS with profound impact in reduction of systemic inflammation and ease hypoxemia that eventually control the respiratory deficiency [82,83]. Efficacy of corticosteroid in low dose against SARS-CoV-2 pneumonia patients has been evaluated which shows promising rate of recovery of clinical symptoms [84]. In SARS-CoV-2 patients with extrapulmonary systemic hyperinflammation syndromes associated markers found to be increased, corticosteroids therapy improves the mortality rate in such cases. Due to infection drop in levels of suppressor, helper and regulatory T cell counts were observed. Other factors that contribute involve granulocyte colony-stimulating factor, macrophage inflammatory protein 1-α, inflammatory cytokines biomarkers and cytokines (IL-2, IL-6, IL-7), C-reactive protein, tumor necrosis factor-α in patients severely ill patients that possibly leads to activation of NF-kB signaling and JAK/STAT pathway. Due to p38 phosphorylation and NF-KB nuclear translocation results in induction of chemokines and inflammatory cytokines that leads to the “cytokine storm”. In most cases Therefore, the immunomodulation of p38 MAPK and NF-kB activation potentially considered as a therapeutic target. Corticosteroid act as an anti- immunosuppressive and inflammatory agent such as dexamethasone, hydrocortisone and methylprednisone. Corticosteroids interact with glucocorticoid receptors (GRs) by crossing through host cell membrane that moves into the nucleus and upon binding with glucocorticoid response elements (GRE) that regulate the expression of many genes. The Corticosteroid exhibit anti-inflammatory properties via release of proinflammatory cascade such as phospholipase A2 in immune cells like dendritic cells, lymphocytes, macrophages, mast cells and eosinophils. However due to the side effects of corticosteroids against viral immune response on COVID-19 patients its potential as an anti-SARS-CoV-2 agent is dubious [83]. The considerable major factors that can have a main impact on the clinical outcome are half-life, dosage, formulation, and selection of patient [11].
Dexamethasone: A Life Saving Steroid
Dexamethasone, approved by the FDA in 1958, is a broad-spectrum synthetic corticosteroid immunosuppressor 30 times stronger as compared to cortisone with extended duration of action recently shows promising results on COVID-19 patients. Till now, and without any published set of data as a result of a trial it has been recently announced that low dose treatment of low-cost cheap corticosteroid dexamethasone, is reducing the mortality rate of severely ill patients who need help in breathing. Since 1960s, dexamethasone has been widely used in cure of asthma and rheumatoid arthritis. Dexamethasone is known to be more effective for patients on ventilators by reducing the death risk from 40% to 28% compared to those who in need of oxygen by 25% to 20% at a low dose of 6 mg per day for 10 days by treating the overreaction of immune response. However, it does not much helpful on patients with milder symptoms of infection [85-87].
The acute respiratory distress syndrome (ARDS) develops in many patients, and it is linked with enormous inflammatory response and subsequent cytokine storms could lead to lung damage. The defensive action against COVID-19 is linked with specific antibodies and activated T cells [88]. The action of dexamethasone is not limited to the harmful effect and production of cytokine but also reduces the role of T cells and inhibit the release of antibodies from B-cells that result in viral load increase. Thus, dexamethasone can only be effective as a short-term treatment option in severely ill patients as it could be risky during recovery due to existence of virus while the production of antibodies will be interrupted by the body [89].
Passive Immunotherapy
Convalescent serum
Another alternative and promising approach is utilization of convalescent plasma from the recovered patients or seroconverted patients from viral infections has a long history [90]. Based on the previous experienced on SARS, H5N1 avian influenza, 1918 influenza, 2009 influenza H1N1, severe Ebola virus and MERS viral infections passive immunotherapy is considered as a possible curative option against SARS-CoV-2 infections. Injecting the antibodies to susceptible and infected patients, is a rapid mean of providing immunity for effective cure and prevention [69,91-93]. According to the study among COVID-19 and ARDS patient clinical condition were significantly improved following the convalescent plasma transfusion [93]. This treatment, can be effective against SARS-CoV-2 infection, is a potential and successful candidate according to the several studies [69]. The development of the IgG antibodies among infected patients has significantly increases the chances of its future use [94]. Although, according to a reported RCT the use of convalescent plasma in addition with standard treatment no improvement in clinical symptoms was observed. This is because antibody therapy is more effective at early stages of disease progression and shows more profound effects in severely ill patients related to patients who are seriously sick [2,95]. The main objective behind isolating the neutralizing antibodies from recently recovered patients is to inactivate the virus through transfusion into the infected patients [96]. The neutralizing antibodies exerts its therapeutic action by delaying the binding of S proteins to their receptors leads to interfere with conformational changes, necessary to target for membrane binding for immune response modulation. Induction of phagocytosis and cellular cytotoxicity could possibly be as a result of administration of convalescent serum. However, the major limitation associated with passive immunotherapy is the risk of antibody-dependent enhancement (ADE), short life of antibodies and shortage of donor [49,97]. The potency and safety of passive immunotherapy has been examined and improvement in radiological and clinical symptoms with reduced viral load was observed upon infusion of convalescent plasma into SARS-CoV2 patients [91,93,98,99]. The major possible setbacks are soon after the transfusion are fever, nausea, disease transmission risk and skin rash [100].
Monoclonal or polyclonal antibodies
Antibodies isolated from B-cells are known as monoclonal antibodies (MAbs) and so far, around 70 recombinant mABs have been authorized by FDA for the treatment of cardiovascular diseases, auto-immune, inflammatory, arthritis, malignant and infectious diseases [101]. Based on the previous in vivo and in vitro studies favorable outcome on SARS-CoV and MERS monoclonal antibodies (MAbs) has been proposed as a potential therapeutic against COVID-19 [102,103]. The possible action of MAbs is to target an RBD (receptor- binding domain) of the viral S1 subunit of protein in order to block the host receptor binding thus inhibiting viral entry [7,104]. Another potential target is the S1 subunit involves in viral and host cell membrane fusion. Injecting the highly active and specific monoclonal antibodies (MAbs) offer more advanced alternative to plasma with minimized risk of transmission of blood borne diseases. So far, many MABs targeting the SARS-CoV RBD (S1 and S2 subunits) were tested. Thus, based on similarity among the spike protein of SARS-CoV and SARS, MABs are considered as a favorable candidate for further investigation against COVID-19 [49].
Tocilizumab
Tocilizumab blocks the pro-inflammatory cytokine IL-6 (interleukin-6) receptor released as a result of viral infection hence serve as an IL-6 receptor antagonist. A humanized monoclonal antibody, Tocilizumab – known to be used in rheumatoid arthritis treatment for many years and in cytokine release syndrome associated with COVID-19 under randomized controlled trials [105-107]. In a clinical trial conducted in China improvement in clinical symptoms was observed on 20 severely ill SARS-CoV-2 patients after tocilizumab treatment according to the non-peer reviewed study [48]. In another study conducted at the Spedali Civili University Hospital in Brescia (Italy), COVID-19 pneumonia patients showed positive outcome with tocilizumab treatment indicating the future need of randomized clinical trial [3,108]. In ongoing clinical trials by FDA phase III as a result of tocilizumab treatment, clinical symptoms and rate of recovery improved in severe COVID-19 patients [3]. Another IL-6 receptor antagonist Sarilumab is currently in phase II/III clinical trial in severe COVID-19 infected patients for efficacy evaluation. It is worth mentioning here that among COVID-19 patients, the repeated dose of Tocilizumab is suggested in case of failure of response after the first dose in order to get a larger response [109]. Although septic shock and gastrointestinal perforation has been observed in some COVID-19 patients after tocilizumab treatment it further linked with higher risk of leukopenia. The potential efficacy and safety profiles of monoclonal and polyclonal antibodies against SARS-CoV-2 therapeutics needs to be investigated further but due to it high cost like any other tocilizumab is also limit its use [108].
Interferons
Interferon, an immunomodulatory antiviral compound works by inhibiting the viral exocytosis. Interferon beta (IFN-β) showed potent activity against MERS-CoV infections in Vero cells [110]. As an anti-SARS-CoV-1 agent interferon alfa and beta presented invitro activity [56,57]. Trials against SARS-CoV-2 related to efficacy of interferon-alpha-2a have been conducted in China in combination with ribavirin [96,111]. However due to adverse side effects record, such as anemia, GI and depressive symptoms in MERS pandemic this combination is not advisable without a SARS-CoV-2 clinical trial [48].
Other Therapeutic Agents
Hesperidin
Studies suggested the protective effects of hesperidin at early stages of infection against influenza A virus, by blocking the viral neuraminidase (sialidase) enzyme that play a key role in release of virions from infected cells [112]. Hesperidin is found in high amount in the rinds of a few citrus species, this compound is a flavanone group member of the flavonoid family with a broad range of pharmacological activities [113]. According to recent studies hesperidin has been found to block the association between spike protein and ACE-II receptor upon binding to RBD of spike protein of SARS-CoV-2 thus this led to the inhibition of viral entry into the host cell. These findings provide the supportive basis of conducting the clinical trials as so far, no side effects have been reported regardless of low prevalence of vomiting and nausea [49].
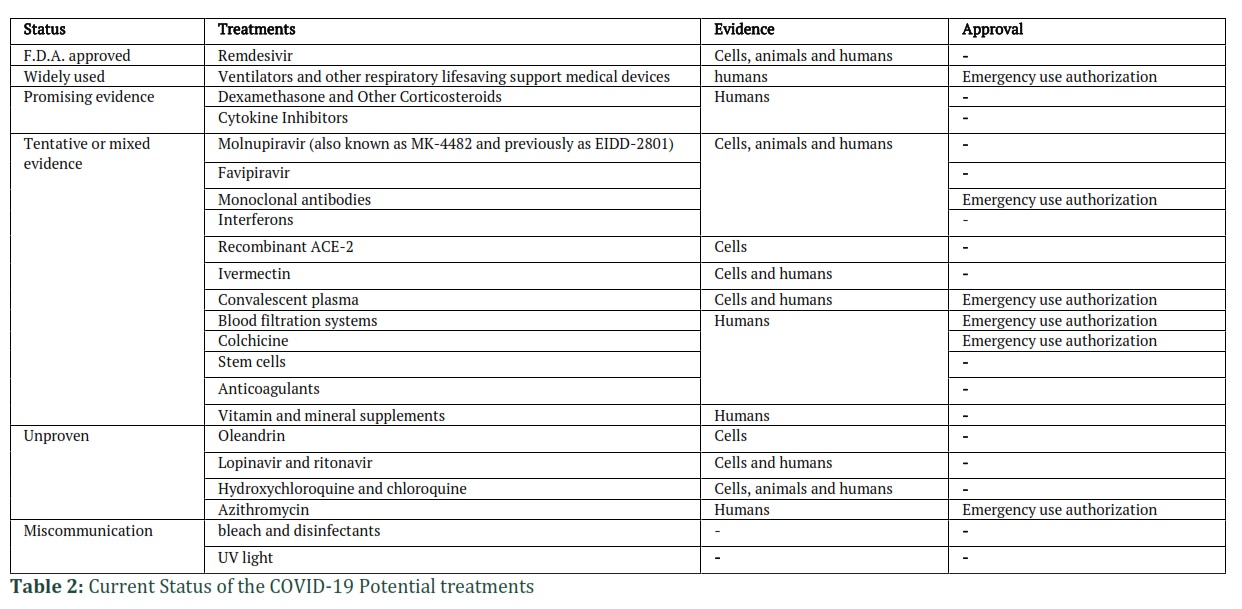
On-going investigations uncovers various FDA approved drugs and in silico virtual screening methods using modeling and molecular docking approaches could be promising approach in search of potential anti-viral drug against COVID-19 treatment. The current status of the potential COVID-19 treatments [114] has been summarized in table 1.
Bacteriophage: A Novel Approach
The high rate of mortality among COVID-19 patients could possibly be due to a delayed communication between adaptive and innate immune systems, leading to a slower production of antibodies. If the contributing factor behind the mortality rate among elderly patients is bacterial infections, then the extra time required by the body’s adaptive immune system for antibody generation that could be achieved by decreasing the growth rate of bacteria in respiratory system of infected patients [115]. Bacteriophages are viruses that selectively target a specific bacterium without causing any harm to humans. Broad range antibiotics might also target the beneficial bacteria alongside the harmful ones, thus possibly allowing for the development of antibiotic resistant bacteria due to their overuse [116]. By the discovery of phage display technique, bacteriophages have a potential to produce recombinant antibodies that was previously effectively used for MERS-CoV. This technique inhibits ACE2 association that could possibly be engineered by serum of immune patients [117]. Therefore, bacteriophages can be used for the development of synthetic antibodies for the treatment of SARS-CoV patients, thus reduce the mortality rate . However careful design of clinical trials is needed for bacteriophage selection against the bacteria specifically causing the respiratory problems among infected patients or the synthetic antibody production. The time taken by the body in order to develop the antibodies and the link associated with the role of bacteria in mortality rate is also not well established [118].
Vaccine Development: Mechanism of action of Vaccines
The vaccine protective effects are mainly based on viral neutralizing antibodies that target Antibody/B Cell Protection induced by approved viral vaccines. These antibodies inhibit viral interaction with its cellular receptor or block conformational changes needed for viral fusion within cell membrane. The anti-CoV-2 vaccines development process were accelerated and become available within eight to ten months compared to previous vaccines preparation that took around eight to ten years before being commercially ready. The general approach for vaccine preparation was rely on the only viral surface spike protein as an antigen that available for the immunological cells and antibodies in the body.
The common types of COVID-19 vaccines are protein subunit, nanoparticles or virus-like particles, whole virus, nucleic acid (RNA AND DNA) and viral vector. They work by production of antigen either through smuggling it into the body or utilizing own body’s cells for viral antigen production. The whole virus vaccine method utilizes whole viruses (live-attenuated or inactivated) to modulate an immune response. The two main techniques involve: live attenuated vaccines that used fragile form of the virus capable of replicating that does not lead to any disease and other one is the inactivated vaccines in which viral genetic material turns to be non- functional so incapable of replicating but able to trigger an immune response. In subunit vaccines viral protein fragments used to evoke immune response that could be weak with minimal side effects. On the other side nucleic acid based vaccines utilizes genetic material that instruct cells for antigen production, such as viral spike protein. Upon entering of genetic material into the human cells, body cells act as protein factories for antigen production. They are easy and simple to make, and economical however RNA vaccines require ultra-cold temperatures form storage (-70℃ or lower) that could be challenging for developing countries. Viral vector vaccines based on utilizing non-pathogenic virus through proving instructions to genetic material for antigen production. But the virus is dissimilar to the one vaccine is targeted in order to give command to our body own cellular genetic material and take over that antigen producing factories. The other approach is nanoparticles and virus-like particles (VLPs) based on engineered foreign virus epitopes shows on their surface, making them highly immunogenic. Molecules initiate innate immunity is encapsulated within VLPs to increase immune responses and activate T helper type 1 (Th1) polarized immune cascades (type 1 immunity) instead of pathogenic elevating Th2 polarization. So far approved vaccines manufactured by Moderna, and Pfizer based on lipid nanoparticle (LNP) delivery systems and mRNA technology, while the formulations approved for Johnson, AstraZeneca and Johnson although Gam-COVID-vac (Sputnik V) possess DNA dispatch within recombinant non-replicating adenovirus (AdV) vector. The AdV and mRNA vaccines code the making of the SARS-CoV-2 spike (S) protein, that serve as primary target for neutralizing antibodies comes from therapeutic monoclonal antibodies and natural infection.
A current status of COVID-19 Vaccine
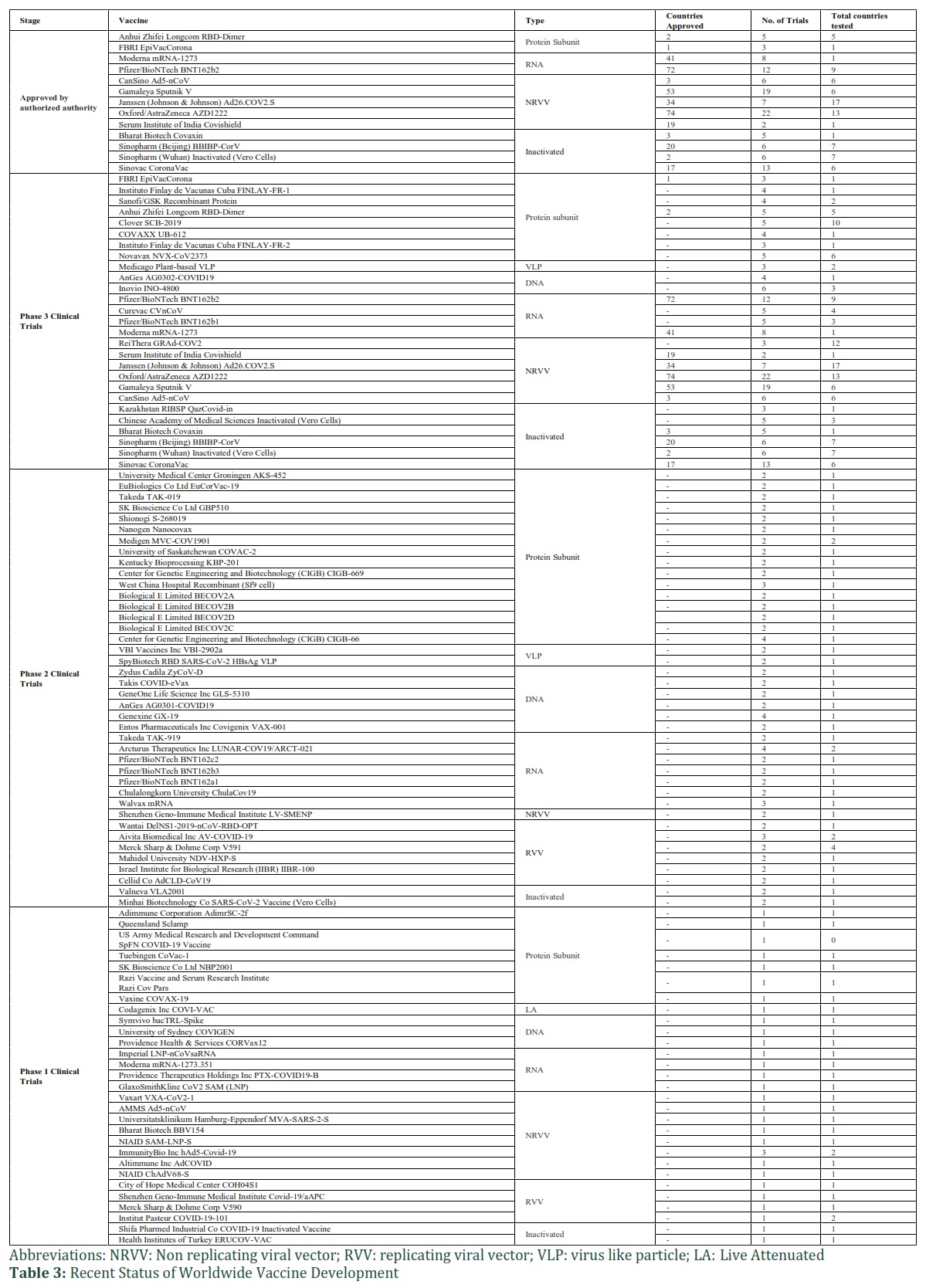
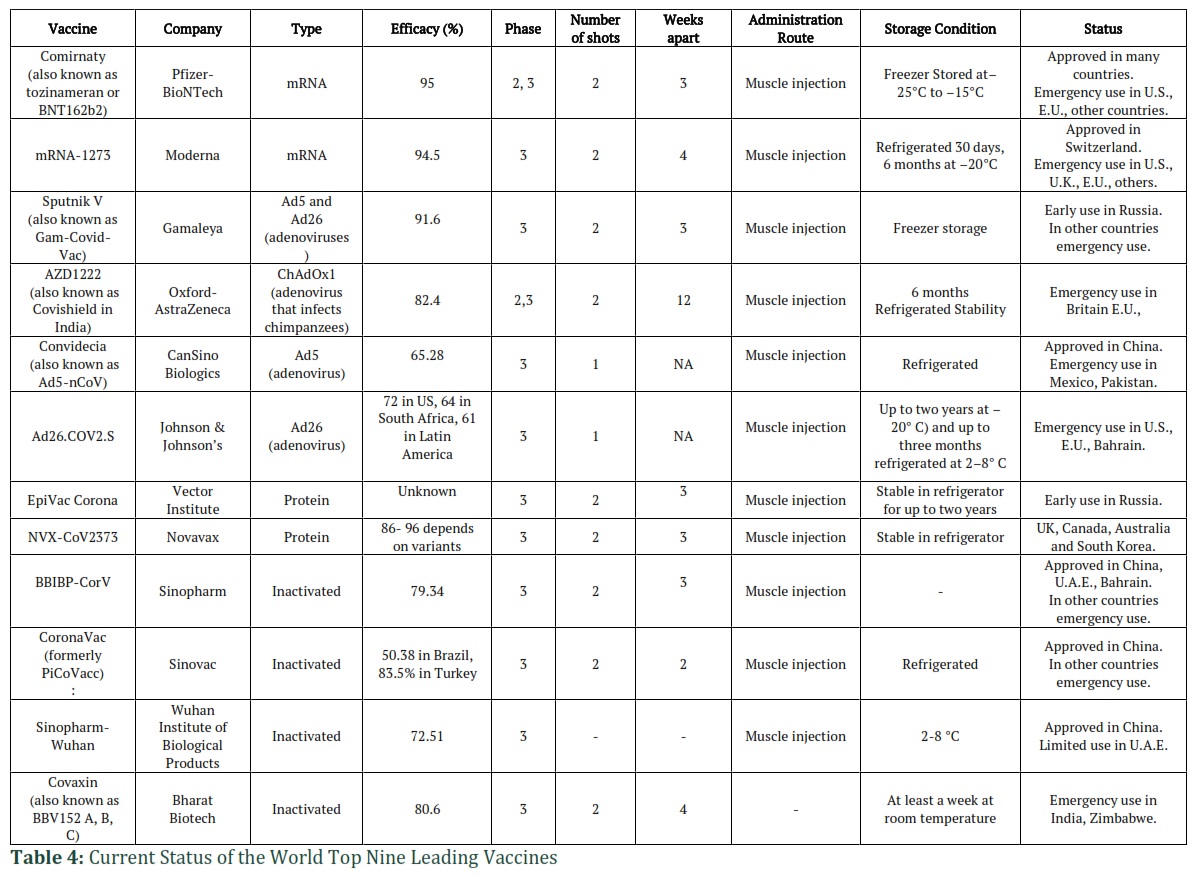
In order to end this pandemic, an enormous portion of the world population should be resistant to the infection. Herd immunity develops when reasonable segment of a community (the herd) gets immune for a particular disease. In that case risk of infections spread from one person to another is very low that leads to better protection of population against contagious diseases. The most practical approach to accomplish this is via immunization. Through history, humankind has frequently depended on vaccine technology to cut down the loss of life against infectious diseases [119]. So far there are more than 200 vaccines contestant being developed and analyzed at a rapid speed. The production of vaccines consists of the following stages: exploratory, preclinical and clinical phases. The recent status of the worldwide vaccine development has been summarized in table 2 with number of trials in total number of countries [120]. In a race of vaccine development, AZ-Oxford University has sold more than 2.5 billion doses so far followed by AstraZeneca that deals around 500 million doses each to US and the India along with 400 million vaccines to the European Union. The highest seller of COVID-19 vaccines has been chased by Novavax by selling 1.3 billion vaccine doses. Till now 10% and 6% have been sold by Moderna and Pfizer-BioNTech of the total manufactured vaccine doses respectively [121]. It has been reported that so far around 359 million doses have been given across the globe in 122 countries, accounting for almost 9.25 million doses per day. In the US only, 107 million doses have been administered that counts for 2.9 million vaccine doses per day, this would eventually take 5 months to cover 75% of its whole population to get immunized with 2 doses [122]. The demand for COVID-19 vaccines is global, but across communities, the need is differentially spread. In the first phase, health-care staff in hospitals has been prioritized followed by staff working in health centers and eventually among the elderly and the eligible people with specific medical conditions. It is estimated that around 8.09 million people globally doses so far received the two doses of vaccination [123]. Although several countries are still waiting to receive their first vaccine shots. With emergence of new viral strains, Moderna has developed a booster shot against two SARS-CoV-2 variant strains including B.1.351 (501Y.V2) and B.1.1.7, that initially originated from UK and having lower level of antibody as compared to previously identified strains, although both strains are found to have several mutations on the spike protein. At present, Moderna vaccine has been given in two shots in monthly timespan while investigation of its third shot against B.1.351 strain has been underway. Among all variants B.1.351 is found to be most fast growing strain of SARS-CoV-2 that originated in October 2020 from South Africa [124]. Currently, mRNA based vaccine from Pfizer-BioNTech in phase 2, 3 recently been approved in Bahrain, Saudi Arabia, Switzerland in necessity in U.S., E.U., other countries while Moderna is in phase 3 has been using in Switzerland and urgency in U.S., U.K., E.U., others [125]. In the race of safe and effective vaccine production against coronavirus so far 76 vaccines are currently in clinical trials while 22 have cross the last steps of analysis among them around 77 candidates are under preclinical investigation in animals. Until present, 42 vaccines are in phase 1 while 30 and 21 vaccines are in phase 2 and phase 3 respectively. There are 6 vaccines that are authorized for limited used. The details of world top 9 vaccines against COVID-19 have been listed in table 3 [126].
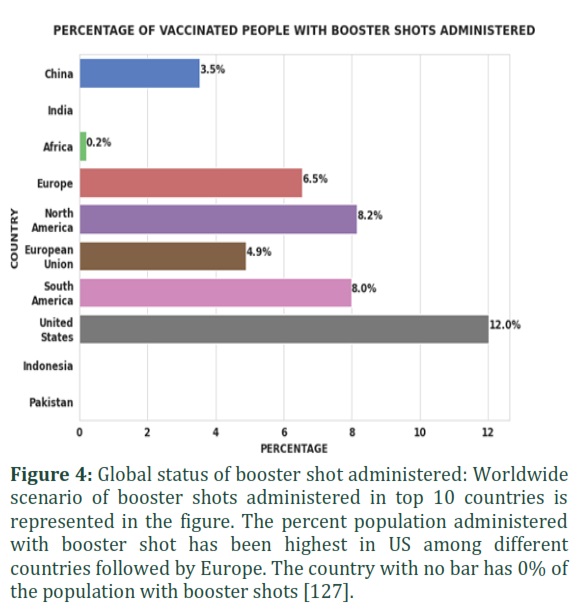
Booster shot an additional dose of COVID-19 that usually administered once given after the protective effects of original shot(s) initiates to decline gradually during course of time. The booster dose provides better prevention by either restoring or enhancing protection from severe coronavirus infection as mentioned in the figure 4. A booster dose usually given to an individual whose vaccination schedule has been completed. However as compared to booster dose an additional dose usually given to individuals with moderately to severely compromised immune systems (having weakened immune system due to any medical symptom or as a receipt of immunosuppressive medications or treatments). This additional dose results in betterment of responses in immunocompromised individuals against their previous vaccination program. In immunocompromised individuals, the third dose is considered as the final dose of the primary vaccine series.
From Delta to Omicron variant: How this new variant possibly reshapes the pandemic
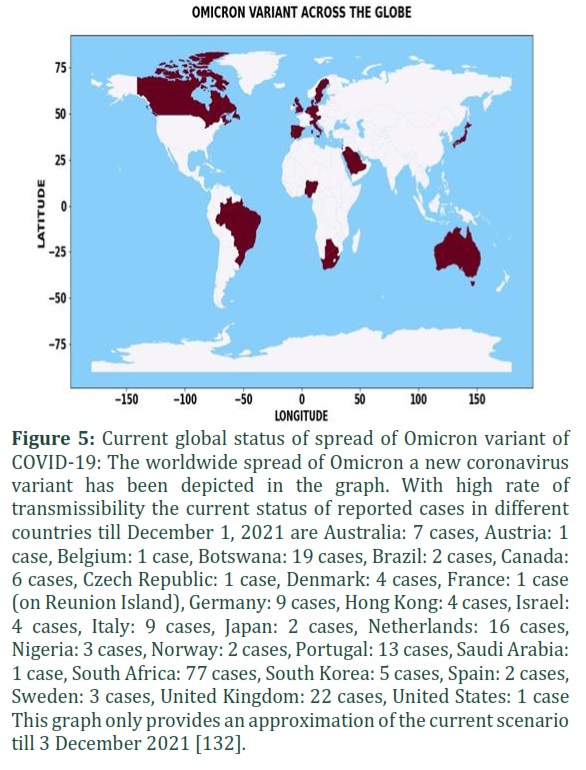
The designation of coronavirus variants by WHO as a variant of concern due to their contagious nature stays under high surveillance as regular updates needs to be monitor regularly. So far, up till now, five variants of concern have been named as: Alpha, Beta, Gamma, Delta and Omicron [128]. From the journey that begins from the B.1.1.7 (Alpha variant of coronavirus) in last December that swept rapidly across England, and then completely into the world [129]. Followed by another variant initially detected in South Africa, the B.1.351 or Beta variant contains both an E484K mutation that connects with immune escape while making N501Y mutation leads to help many other variants of coronavirus more contagious. The three identified SARS-CoV-2 variants contains mutations into ACE2 interacting surface of the RBD such as N501Y, K417N and E484K in B.1.351, N501Y in B.1.1.7 and iN501Y, K417T and E484K in P.1. These variants (B.1.351 and B.1.1.7) possess high potential of transmissibility and become global strain of concern. As these variants contain various variations in the immunodominant (S) spike protein that helps viral entry through ACE2. These mutations in the recognition site of receptor on spike protein are mainly responsible for immune escape. The mutations in receptor-binding domain leads to strong association of ACE2 and its global escape through neutralization of monoclonal antibody directed by E484K, although N501Y and K417N as these works as together against other crucial antibody types. The third variant of concern, Gamma variant, that spread across Brazil did not reach many other places. The B.1.617.2 Delta variant of coronavirus has predominately spared through the US and across the world. It rapidly took over from the B.1.1.7, or Alpha variant in many countries. Delta contains many mutations on the spike protein capable of stimulating the immune system, as people who have been already infected once with any other variant will likely become infected again [130]. Currently the Omicron variant of coronavirus has been detected in several countries worldwide as mentioned in the figure 5. The nations all over the world are looking to identify about cases of the Omicron variant with the increasing fear of enforcement of governmental policies in respect to closing border and revised restrictions with SOPs (wearing mask, use of disinfectants, maintaining social distancing). The new variant designated as B.1.1.529 was first detected on the 11th of November 2021 in Botswana, with 30 more mutations on its Spike protein, double what was originally carried by the Delta variant, making it potentially more transmissible with a Ro value of 1.93, as compared to Delta’s 1.47. On the 1st of December, South Africa detected 8,561 cases, more from the 3,402 initially reported on the 26th of November 21; leading to various hundreds of cases per day in mid-November, with the dominant spared in Gauteng Province. So far, genome sequencing is required to confirm the Omicron cases as PCR tests is not as effective due to mutations that distinguishes it from Delta. The spread of variant across the globe might depend on reasons such as prior infection rates and vaccination capacity of that nation [130]. . Based on initial evidence in South Africa, the new variant might spread at a higher rate than the Delta one as it has been found to be 50% more contagious than earlier lineages. It’s also containing 23 mutations, together with N501Y with high risk of spreading that therapeutically works with monoclonal antibody and vaccines. Same as Delta, Omicron also contains a mutation called D614G, which links the virus efficiently to the cells it is going to infect. It might be expected that fully vaccinated people who are now becoming infected with this Omicron variant are able to spread this virus. The number of existing mutations that affects the spike protein as many leading vaccines target the Spike protein such as Moderna, Johnson & Johnson Pfizer/BioNTech and AstraZeneca as they have been designed using portion of genetic sequences, instead of whole virus therefore mostly, they use a part of the Spike protein to evoke immune response. Thus, any change in the spike protein will make it less identifiable to immune system proteins and to cells triggered by a vaccine [128]. As per WHO, current treatment includes oxygen therapy and dexamethasone, while the other two antiviral drugs Molnupiravir and Favipiravir also look promising, but we have to wait for more data from clinical trials [130]. Omicron contains almost 32 changes to the Spike protein, it also bears a mutation called E484A, that is almost similar to E484K but not completely. The ‘poly-mutant Spike’ is completely resistant to neutralizing antibodies for many people who tested who had already vaccinated with two doses of an RNA vaccine or get recovered from COVID-19 [131]. Despite the global burden of the pandemic, finally a breakthrough has been witnessed in combating the spread of COVID-19 infections. Currently, there are seven most promising vaccines that are currently available to the public within the needed quantity in around 73 countries so far. Novel Vaccine technology has put the nations under huge economic constraints in terms of testing, batching, mass production and final commercialization of the to make it accessible for the public. Although it has been a big challenge to cover an entire global population including low-income countries that find harder to cover essential aspects of food, healthcare and education. Currently, immunization pace will take years to achieve heard immunity at global community level while reported side effects, strain resistant factor and variations in diverse accessibility with variable efficiency among population are still some of the considerable factors. Despite the availability of vaccines, there are still several logistical challenges to overcome in the foreseeable future. Therefore, along with vaccine technology different traditional discussed on-going therapeutic strategies against SARS-CoV-2, through combinational drug approaches could be the way forward against the treatment of SARS-CoV-2 or for any future pandemics. Plasma therapy along with anti-viral agent Remdesivir, although RCT analysis results will confirm the further detailed regarding proposed therapies. The information currently available on existing treatments are based on a limited number of trials and preliminary studies, thus there is an alarming need for more studies on infected individuals to test the effectiveness and protection of current drugs and explore the potential new candidates. Detailed structural studies of SARS-CoV-2 possibly explore the potential therapeutic targets from natural or synthetic sources. However, dissecting the major mysteries behind virus pathogenicity, immunological response and replication pathways will provide the possibility to further explore the potential targeted therapies. Due to the lengthening of the pandemic and pathogenicity of the virus, efficacious therapies may be in based in combinations with proper clinical monitoring and assessment profile.
Figures & Tables
Despite the global burden of the pandemic, finally a breakthrough has been witnessed in combating the spread of COVID-19 infections. Currently, there are seven most promising vaccines that are currently available to the public within the needed quantity in around 73 countries so far. Novel Vaccine technology has put the nations under huge economic constraints in terms of testing, batching, mass production and final commercialization of the to make it accessible for the public. Although it has been a bigchallenge to cover an entire global population including low-income countries that find harder to cover essential aspects of food, healthcare and education. Currently, immunization pace will take years to achieve heard immunity at global community level while reported side effects, strain resistant factor and variations in diverse accessibility with variable efficiency among population are still some of the considerable factors. Despite the availability of vaccines, there are still several logistical challenges to overcome in the foreseeable future. Therefore, along with vaccine technology different traditional discussed on-going therapeutic strategies against SARS-CoV-2, through combinational drug approaches could be the way forward against the treatment of SARS-CoV-2 or for any future pandemics. Plasma therapy along with anti-viral agent Remdesivir, although RCT analysis results will confirm the further detailed regarding proposed therapies. The information currently available on existing treatments are based on a limited number of trials and preliminary studies, thus there is an alarming need for more studies on infected individuals to test the effectiveness and protection of current drugs and explore the potential new candidates. Detailed structural studies of SARS-CoV-2 possibly explore the potential therapeutic targets from natural or synthetic sources. However, dissecting the major mysteries behind virus pathogenicity, immunological response and replication pathways will provide the possibility to further explore the potential targeted therapies. Due to the lengthening of the pandemic and pathogenicity of the virus,efficacious therapies may be in based in combinations with proper clinical monitoring and assessment profile.
Author Contributions
AK contributed to main manuscript writing, data mining and analysis, RA contributed in designing, data analysis and review, AZ has contributed in Data Analysis and interpretation, manuscript review and revision. OA has contributed to data collection, Data analysis, image sketching, MAH has contributed in figures and tables correction, Wrote and analysed new variant. ![]()
The authors declare that there is no conflict of interest.
![]()
References
- University JH (2021) Coronavirus Resource Center.
- Wang H, Li X, Li T, Zhang S, Wang L, et al. The genetic sequence, origin, and diagnosis of SARS-CoV-2. Eur J Clin Microbiol Infect Dis, (2020).
- Huang C, Wang Y, Li X, Ren L, Zhao J, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet, (2020); 395(10223): 497-506.
- Jean SS, Lee PI, Hsueh PR. Treatment options for COVID-19: The reality and challenges. J Microbiol Immunol Infect, (2020); 53(3): 436-443.
- Zhou F, Yu T, Du R, Fan G, Liu Y, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet, (2020); 395(10229): 1054-1062.
- Cheng ZJ, Shan J. 2019 Novel coronavirus: where we are and what we know. Infection, (2020); 48(2): 155-163.
- Zhao N, Zhou ZL, Wu L, Zhang XD, Han SB, et al. An update on the status of COVID-19: a comprehensive review. Eur Rev Med Pharmacol Sci, (2020); 24(8): 4597-4606.
- Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int J Antimicrob Agents, (2020); 55(3): 105924.
- Park SJ, Yu KM, Kim YI, Kim SM, Kim EH, et al. Antiviral Efficacies of FDA-Approved Drugs against SARS-CoV-2 Infection in Ferrets. mBio, (2020); 11(3).
- Epidemiology Working Group for Ncip Epidemic Response CCfDC, Prevention. [The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China]. Zhonghua Liu Xing Bing Xue Za Zhi, (2020); 41(2): 145-151.
- Hossein-Khannazer N, Shokoohian B, Shpichka A, Aghdaei HA, Timashev P, et al. Novel therapeutic approaches for treatment of COVID-19. J Mol Med (Berl), (2020); 98(6): 789-803.
- Shanmugaraj B, Malla A, Phoolcharoen W. Emergence of Novel Coronavirus 2019-nCoV: Need for Rapid Vaccine and Biologics Development. Pathogens, (2020); 9(2).
- Elgamasy S, Kamel MG, Ghozy S, Khalil A, Morra ME, et al. First Case of Focal Epilepsy Associated with SARS-Coronavirus-2. J Med Virol, (2020).
- Zeouk I, Bekhti K, Lorenzo-Morales J. From Wuhan to COVID-19 Pandemic: An Up-to-Date Review of Its Pathogenesis, Potential Therapeutics, and Recent Advances. Microorganisms, (2020); 8(6).
- Chen N, Zhou M, Dong X, Qu J, Gong F, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet, (2020); 395(10223): 507-513.
- Gao Y, Yan L, Huang Y, Liu F, Zhao Y, et al. Structure of the RNA-dependent RNA polymerase from COVID-19 virus. Science, (2020); 368(6492): 779-782.
- Seah I, Su X, Lingam G. Revisiting the dangers of the coronavirus in the ophthalmology practice. Eye (Lond), (2020); 34(7): 1155-1157.
- Chan JF, Kok KH, Zhu Z, Chu H, To KK, et al. Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerg Microbes Infect, (2020); 9(1): 221-236.
- Sawicki SG, Sawicki DL. Coronavirus transcription: a perspective. Curr Top Microbiol Immunol, (2005); 28731-55.
- Hussain A, Kaler J, Dubey AK. Emerging Pharmaceutical Treatments of Novel COVID-19: A Review. Cureus, (2020); 12(5): e8260.
- Salvi R, Patankar P. Emerging pharmacotherapies for COVID-19. Biomed Pharmacother, (2020); 128110267.
- Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, et al. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell, (2020); 181(2): 281-292 e286.
- Forster P, Forster L, Renfrew C, Forster M. Phylogenetic network analysis of SARS-CoV-2 genomes. Proc Natl Acad Sci U S A, (2020); 117(17): 9241-9243.
- Martinez MA. Compounds with Therapeutic Potential against Novel Respiratory 2019 Coronavirus. Antimicrob Agents Chemother, (2020); 64(5).
- Pandey SC, Pande V, Sati D, Upreti S, Samant M. Vaccination strategies to combat novel corona virus SARS-CoV-2. Life Sci, (2020); 256117956.
- Graham RL, Donaldson EF, Baric RS. A decade after SARS: strategies for controlling emerging coronaviruses. Nat Rev Microbiol, (2013); 11(12): 836-848.
- Elhusseiny KM, Abd-Elshahed Abd-Elhay F, Kamel MG. Possible therapeutic agents for COVID-19: a comprehensive review. Expert Rev Anti Infect Ther, (2020).
- Warren TK, Jordan R, Lo MK, Ray AS, Mackman RL, et al. Therapeutic efficacy of the small molecule GS-5734 against Ebola virus in rhesus monkeys. Nature, (2016); 531(7594): 381-385.
- Lo MK, Jordan R, Arvey A, Sudhamsu J, Shrivastava-Ranjan P, et al. GS-5734 and its parent nucleoside analog inhibit Filo-, Pneumo-, and Paramyxoviruses. Sci Rep, (2017); 743395.
- Agostini ML, Andres EL, Sims AC, Graham RL, Sheahan TP, et al. Coronavirus Susceptibility to the Antiviral Remdesivir (GS-5734) Is Mediated by the Viral Polymerase and the Proofreading Exoribonuclease. mBio, (2018); 9(2).
- Gordon CJ, Tchesnokov EP, Feng JY, Porter DP, Gotte M. The antiviral compound remdesivir potently inhibits RNA-dependent RNA polymerase from Middle East respiratory syndrome coronavirus. J Biol Chem, (2020); 295(15): 4773-4779.
- Aditya K. P RS, Timir Tripathi. Rational Design of the Remdesivir Binding Site in the RNA-dependent RNA Polymerase of SARS-CoV-2: Implications for Potential Resistance. bioRxiv, (2020).
- Wang M, Cao R, Zhang L, Yang X, Liu J, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res, (2020); 30(3): 269-271.
- Choy KT, Wong AY, Kaewpreedee P, Sia SF, Chen D, et al. Remdesivir, lopinavir, emetine, and homoharringtonine inhibit SARS-CoV-2 replication in vitro. Antiviral Res, (2020); 178104786.
- Jonathan Grein MD, Norio Ohmagari MD, Daniel Shin MD, George Diaz MD, Erika Asperges MD, et al. Compassionate Use of Remdesivir for Patients with Severe Covid-19. N Engl J Med, (2020); 3822327-2336.
- Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, et al. First Case of 2019 Novel Coronavirus in the United States. N Engl J Med, (2020); 382(10): 929-936.
- Sheahan TP, Sims AC, Graham RL, Menachery VD, Gralinski LE, et al. Broad-spectrum antiviral GS-5734 inhibits both epidemic and zoonotic coronaviruses. Sci Transl Med, (2017); 9(396).
- Mehta N, Mazer-Amirshahi M, Alkindi N, Pourmand A. Pharmacotherapy in COVID-19; A narrative review for emergency providers. Am J Emerg Med, (2020).
- Baranovich T, Wong SS, Armstrong J, Marjuki H, Webby RJ, et al. T-705 (favipiravir) induces lethal mutagenesis in influenza A H1N1 viruses in vitro. J Virol, (2013); 87(7): 3741-3751.
- Furuta Y, Komeno T, Nakamura T. Favipiravir (T-705), a broad spectrum inhibitor of viral RNA polymerase. Proc Jpn Acad Ser B Phys Biol Sci, (2017); 93(7): 449-463.
- De Clercq E. New Nucleoside Analogues for the Treatment of Hemorrhagic Fever Virus Infections. Chem Asian J, (2019); 14(22): 3962-3968.
- Sissoko D, Laouenan C, Folkesson E, M'Lebing AB, Beavogui AH, et al. Experimental Treatment with Favipiravir for Ebola Virus Disease (the JIKI Trial): A Historically Controlled, Single-Arm Proof-of-Concept Trial in Guinea. PLoS Med, (2016); 13(3): e1001967.
- Chang Chen YZ, Jianying Huang, Ping Yin, Zhenshun Cheng, Jianyuan Wu, Song Chen, Yongxi Zhang, Bo Chen, Mengxin Lu, Yongwen Luo, Lingao Ju, Jingyi Zhang, Xinghuan Wang. Favipiravir versus Arbidol for COVID-19: A Randomized Clinical Trial medRxiv (2020).
- Shiraki K, Daikoku T. Favipiravir, an anti-influenza drug against life-threatening RNA virus infections. Pharmacol Ther, (2020); 209107512.
- Bimonte S, Crispo A, Amore A, Celentano E, Cuomo A, et al. Potential Antiviral Drugs for SARS-Cov-2 Treatment: Preclinical Findings and Ongoing Clinical Research. In Vivo, (2020); 34(3 Suppl): 1597-1602.
- Falzarano D, de Wit E, Rasmussen AL, Feldmann F, Okumura A, et al. Treatment with interferon-α2b and ribavirin improves outcome in MERS-CoV-infected rhesus macaques. Nat Med, (2013); 19(10): 1313-1317.
- Elfiky AA. Anti-HCV, nucleotide inhibitors, repurposing against COVID-19. Life Sci, (2020); 248117477.
- Gul MH, Htun ZM, Shaukat N, Imran M, Khan A. Potential specific therapies in COVID-19. Ther Adv Respir Dis, (2020); 141753466620926853.
- Elhusseiny KM, Abd-Elhay FA, Kamel MG. Possible therapeutic agents for COVID-19: a comprehensive review. Expert Rev Anti Infect Ther, (2020); 1-15.
- Mubareka S, Leung V, Aoki FY, Vinh DC. Famciclovir: a focus on efficacy and safety. Expert Opin Drug Saf, (2010); 9(4): 643-658.
- Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell, (2020); 181(2): 271-280.e278.
- Zhou Y, Vedantham P, Lu K, Agudelo J, Carrion R, Jr., et al. Protease inhibitors targeting coronavirus and filovirus entry. Antiviral Res, (2015); 11676-84.
- Glowacka I, Bertram S, Müller MA, Allen P, Soilleux E, et al. Evidence that TMPRSS2 activates the severe acute respiratory syndrome coronavirus spike protein for membrane fusion and reduces viral control by the humoral immune response. J Virol, (2011); 85(9): 4122-4134.
- Aljofan M GA. COVID-19 treatment: the race against time. Electron J Gen Med, (2020); 17.
- Yamamoto M, Matsuyama S, Li X, Takeda M, Kawaguchi Y, et al. Identification of Nafamostat as a Potent Inhibitor of Middle East Respiratory Syndrome Coronavirus S Protein-Mediated Membrane Fusion Using the Split-Protein-Based Cell-Cell Fusion Assay. Antimicrob Agents Chemother, (2016); 60(11): 6532-6539.
- Chan JF, Yao Y, Yeung ML, Deng W, Bao L, et al. Treatment With Lopinavir/Ritonavir or Interferon-beta1b Improves Outcome of MERS-CoV Infection in a Nonhuman Primate Model of Common Marmoset. J Infect Dis, (2015); 212(12): 1904-1913.
- Zumla A, Chan JF, Azhar EI, Hui DS, Yuen KY. Coronaviruses – drug discovery and therapeutic options. Nat Rev Drug Discov, (2016); 15(5): 327-347.
- Moyle GJ, Back D. Principles and practice of HIV-protease inhibitor pharmacoenhancement. HIV Med, (2001); 2(2): 105-113.
- Arabi YM, Alothman A, Balkhy HH, Al-Dawood A, AlJohani S, et al. Treatment of Middle East Respiratory Syndrome with a combination of lopinavir-ritonavir and interferon-beta1b (MIRACLE trial): study protocol for a randomized controlled trial. Trials, (2018); 19(1): 81.
- Yang X, Yu Y, Xu J, Shu H, Xia J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med, (2020); 8(5): 475-481.
- Kuba K, Imai Y, Rao S, Gao H, Guo F, et al. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus-induced lung injury. Nat Med, (2005); 11(8): 875-879.
- Sun ML, Yang JM, Sun YP, Su GH. [Inhibitors of RAS Might Be a Good Choice for the Therapy of COVID-19 Pneumonia]. Zhonghua Jie He He Hu Xi Za Zhi, (2020); 43(0): E014.
- Monteil V, Kwon H, Prado P, Hagelkrüys A, Wimmer RA, et al. Inhibition of SARS-CoV-2 Infections in Engineered Human Tissues Using Clinical-Grade Soluble Human ACE2. Cell, (2020); 181(4): 905-913.e907.
- Lukassen S, Chua RL, Trefzer T, Kahn NC, Schneider MA, et al. SARS-CoV-2 receptor ACE2 and TMPRSS2 are primarily expressed in bronchial transient secretory cells. Embo j, (2020); 39(10): e105114.
- Z.-X. WEI T-TT, S.-P. JIANG. The antiviral mechanisms, effects, safety and adverse effects of chloroquine. European Review for Medical and Pharmacological Sciences (2020); 247164-7172.
- Plantone D, Koudriavtseva T. Current and Future Use of Chloroquine and Hydroxychloroquine in Infectious, Immune, Neoplastic, and Neurological Diseases: A Mini-Review. Clin Drug Investig, (2018); 38(8): 653-671.
- Andrea Savarino LDT, Isabella Donatelli, Roberto Cauda, Antonio Cassone. New insights into the antiviral effects of chloroquine. Lancet Infect Dis (2006); 6767–69.
- Shibata M, Aoki H, Tsurumi T, Sugiura Y, Nishiyama Y, et al. Mechanism of uncoating of influenza B virus in MDCK cells: action of chloroquine. J Gen Virol, (1983); 64(Pt 5): 1149-1156.
- Cheng Y, Wong R, Soo YO, Wong WS, Lee CK, et al. Use of convalescent plasma therapy in SARS patients in Hong Kong. Eur J Clin Microbiol Infect Dis, (2005); 24(1): 44-46.
- Joshi SR, Butala N, Patwardhan MR, Daver NG, Kelkar D. Low cost anti-retroviral options: chloroquine based ARV regimen combined with hydroxyurea and lamivudine: a new economical triple therapy. J Assoc Physicians India, (2004); 52597-598.
- Savarino A, Boelaert JR, Cassone A, Majori G, Cauda R. Effects of chloroquine on viral infections: an old drug against today's diseases? Lancet Infect Dis, (2003); 3(11): 722-727.
- Keyaerts E, Vijgen L, Maes P, Neyts J, Van Ranst M. In vitro inhibition of severe acute respiratory syndrome coronavirus by chloroquine. Biochem Biophys Res Commun, (2004); 323(1): 264-268.
- Vincent MJ, Bergeron E, Benjannet S, Erickson BR, Rollin PE, et al. Chloroquine is a potent inhibitor of SARS coronavirus infection and spread. Virol J, (2005); 269.
- Kearney JE. Chloroquine as a Potential Treatment and Prevention Measure for the 2019 Novel Coronavirus: A Review. J Chem Inf, (2020); 531689–1699.
- Xue J, Moyer A, Peng B, Wu J, Hannafon BN, et al. Chloroquine is a zinc ionophore. PLoS One, (2014); 9(10): e109180.
- Yao X, Ye F, Zhang M, Cui C, Huang B, et al. In Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin Infect Dis, (2020).
- Gautret P, Lagier JC, Parola P, Hoang VT, Meddeb L, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. Int J Antimicrob Agents, (2020); 105949.
- Toumi M, Aballea S. Commentary on "Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open label non-randomized clinical trial" by Gautret et al. J Mark Access Health Policy, (2020); 8(1): 1758390.
- Juurlink DN. Safety considerations with chloroquine, hydroxychloroquine and azithromycin in the management of SARS-CoV-2 infection. CMAJ, (2020); 192(17): E450-E453.
- Heidary F, Gharebaghi R. Ivermectin: a systematic review from antiviral effects to COVID-19 complementary regimen. J Antibiot (Tokyo), (2020); 1-10.
- Şimşek Yavuz S, Ünal S. Antiviral treatment of COVID-19. Turk J Med Sci, (2020); 50(Si-1): 611-619.
- Thompson BT. Glucocorticoids and acute lung injury. Crit Care Med, (2003); 31(4 Suppl): S253-257.
- Siddiqi HK, Mehra MR. COVID-19 illness in native and immunosuppressed states: A clinical-therapeutic staging proposal. J Heart Lung Transplant, (2020); 39(5): 405-407.
- Yin Wang WJ, , Qi He,, Cheng Wang, , Baoju Liu, , Pan Zhou, , Nianguo Dong, Qiaoxia Tong. Early, low-dose and short-term application of corticosteroid treatment in patients with severe COVID-19 pneumonia: single-center experience from Wuhan, China. medRxiv, (2020).
- Roberts M (2020) Coronavirus: Dexamethasone proves first life-saving drug. Health editor, BBC News online: BBC News. pp. June.
- Ledford H (2020) Coronavirus breakthrough: dexamethasone is first drug shown to save lives. Nature.
- Jarvis LM (2020) Dexamethasone appears to help severe cases of COVID-19. Chemical & Engineering News: Infectious disease
- Abdolahi N, Kaheh E, Golsha R, Khodabakhshi B, Norouzi A, et al. Letter to the editor: efficacy of different methods of combination regimen administrations including dexamethasone, intravenous immunoglobulin, and interferon-beta to treat critically ill COVID-19 patients: a structured summary of a study protocol for a randomized controlled trial. Trials, (2020); 21(1): 549.
- T C Theoharides 1 2 3 PC. Dexamethasone for COVID-19? Not So Fast J Biol Regul Homeost Agents, , (2020); 34(3).
- Casadevall A, Pirofski LA. The convalescent sera option for containing COVID-19. J Clin Invest, (2020); 130(4): 1545-1548.
- Duan K, Liu B, Li C, Zhang H, Yu T, et al. Effectiveness of convalescent plasma therapy in severe COVID-19 patients. Proc Natl Acad Sci U S A, (2020); 117(17): 9490-9496.
- Zhiqiang Zheng VMM, Sebastian Maurer-Stroh, Chow Wenn Yew, Carol Leong, Nur Khairiah Mohd-Ismail, Suganya Cheyyatraivendran Arularasu, Vincent Tak, Kwong Chow, Raymond Lin Tzer Pin, Ali Mirazimi,, Wanjin Hong, Yee-Joo Tan Monoclonal antibodies for the S2 subunit of spike of SARS-CoV cross-react with the newly-emerged SARS-CoV-2. bioRxiv, (2020).
- Shen C, Wang Z, Zhao F, Yang Y, Li J, et al. Treatment of 5 Critically Ill Patients With COVID-19 With Convalescent Plasma. JAMA, (2020).
- Long QX, Liu BZ, Deng HJ, Wu GC, Deng K, et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat Med, (2020); 26(6): 845-848.
- Casadevall A, Joyner MJ, Pirofski LA. A Randomized Trial of Convalescent Plasma for COVID-19-Potentially Hopeful Signals. Jama, (2020).
- Lu CC, Chen MY, Lee WS, Chang YL. Potential therapeutic agents against COVID-19: What we know so far. J Chin Med Assoc, (2020); 83(6): 534-536.
- Bakker AB, Marissen WE, Kramer RA, Rice AB, Weldon WC, et al. Novel human monoclonal antibody combination effectively neutralizing natural rabies virus variants and individual in vitro escape mutants. J Virol, (2005); 79(14): 9062-9068.
- Zhang B, Liu S, Tan T, Huang W, Dong Y, et al. Treatment With Convalescent Plasma for Critically Ill Patients With Severe Acute Respiratory Syndrome Coronavirus 2 Infection. Chest, (2020).
- Ahn JY, Sohn Y, Lee SH, Cho Y, Hyun JH, et al. Use of Convalescent Plasma Therapy in Two COVID-19 Patients with Acute Respiratory Distress Syndrome in Korea. J Korean Med Sci, (2020); 35(14): e149.
- van Griensven J, Edwards T, de Lamballerie X, Semple MG, Gallian P, et al. Evaluation of Convalescent Plasma for Ebola Virus Disease in Guinea. N Engl J Med, (2016); 374(1): 33-42.
- Shepard HM, Phillips GL, C DT, Feldmann M. Developments in therapy with monoclonal antibodies and related proteins. Clin Med (Lond), (2017); 17(3): 220-232.
- Jiang L, Wang N, Zuo T, Shi X, Poon KM, et al. Potent neutralization of MERS-CoV by human neutralizing monoclonal antibodies to the viral spike glycoprotein. Sci Transl Med, (2014); 6(234): 234ra259.
- Coughlin MM, Prabhakar BS. Neutralizing human monoclonal antibodies to severe acute respiratory syndrome coronavirus: target, mechanism of action, and therapeutic potential. Rev Med Virol, (2012); 22(1): 2-17.
- Jia HP, Look DC, Shi L, Hickey M, Pewe L, et al. ACE2 receptor expression and severe acute respiratory syndrome coronavirus infection depend on differentiation of human airway epithelia. J Virol, (2005); 79(23): 14614-14621.
- De Benedetti F, Brunner HI, Ruperto N, Kenwright A, Wright S, et al. Randomized trial of tocilizumab in systemic juvenile idiopathic arthritis. N Engl J Med, (2012); 367(25): 2385-2395.
- Le RQ, Li L, Yuan W, Shord SS, Nie L, et al. FDA Approval Summary: Tocilizumab for Treatment of Chimeric Antigen Receptor T Cell-Induced Severe or Life-Threatening Cytokine Release Syndrome. Oncologist, (2018); 23(8): 943-947.
- Abidi E, El Nekidy WS, Alefishat E, Rahman N, Petroianu GA, et al. Tocilizumab and COVID-19: Timing of Administration and Efficacy. Front Pharmacol, (2022); 13825749.
- Toniati P, Piva S, Cattalini M, Garrafa E, Regola F, et al. Tocilizumab for the treatment of severe COVID-19 pneumonia with hyperinflammatory syndrome and acute respiratory failure: A single center study of 100 patients in Brescia, Italy. Autoimmun Rev, (2020); 19(7): 102568.
- Luo P, Liu Y, Qiu L, Liu X, Liu D, et al. Tocilizumab treatment in COVID-19: A single center experience. J Med Virol, (2020); 92(7): 814-818.
- Chan JF, Chan KH, Kao RY, To KK, Zheng BJ, et al. Broad-spectrum antivirals for the emerging Middle East respiratory syndrome coronavirus. J Infect, (2013); 67(6): 606-616.
- Hart BJ, Dyall J, Postnikova E, Zhou H, Kindrachuk J, et al. Interferon-beta and mycophenolic acid are potent inhibitors of Middle East respiratory syndrome coronavirus in cell-based assays. J Gen Virol, (2014); 95(Pt 3): 571-577.
- Saha RK, Takahashi T, Suzuki T. Glucosyl hesperidin prevents influenza a virus replication in vitro by inhibition of viral sialidase. Biol Pharm Bull, (2009); 32(7): 1188-1192.
- Li C, Schluesener H. Health-promoting effects of the citrus flavanone hesperidin. Crit Rev Food Sci Nutr, (2017); 57(3): 613-631.
- Katherine J. Wu CZaJC (2021) Coronavirus Drug and Treatment Tracker. US: The NewYork Times.
- Tay MZ, Poh CM, Rénia L, MacAry PA, Ng LFP. The trinity of COVID-19: immunity, inflammation and intervention. Nat Rev Immunol, (2020); 20(6): 363-374.
- Czaplewski L, Bax R, Clokie M, Dawson M, Fairhead H, et al. Alternatives to antibiotics-a pipeline portfolio review. Lancet Infect Dis, (2016); 16(2): 239-251.
- Lim CC, Woo PCY, Lim TS. Development of a Phage Display Panning Strategy Utilizing Crude Antigens: Isolation of MERS-CoV Nucleoprotein human antibodies. Sci Rep, (2019); 9(1): 6088.
- Wojewodzic MW. Bacteriophages Could Be a Potential Game Changer in the Trajectory of Coronavirus Disease (COVID-19). PHAGE: Therapy, Applications, and Research (2020); 160-65.
- data Owi (2021) The Our World in Data COVID vaccination data. US: University of Oxford.
- TRACKER C-V (2021) COVID-19 VACCINE TRACKER. COVID-19 VACCINE TRACKER.
- Koop A (2020) Tracking COVID-19 Vaccines Around the World. Visual Capitalist.
- Bloomberg (2021) More Than 359 Million Shots Given: Covid-19 Tracker. Bloomberg.
- Bloomberg (2021) More Than 124 Million Shots Given: Covid-19 Tracker. Bloomberg.
- Jones A (2021) Moderna Developing Booster Shot for New Virus Variant B.1.351. US: The Scientist.
- Carl Zimmer JCaS-LW (2021) Coronavirus Vaccine Tracker. US: The NewYork Times.
- Carl Zimmer JCaS-LW (2021) Coronavirus Vaccine Tracker. NewYork.
- Cameron Appel DB, Daniel Gavrilov, Charlie Giattino, Joe Hasell, Bobbie Macdonald, Edouard Mathieu, Esteban Ortiz-Ospina, Hannah Ritchie, Lucas Rodés-Guirao, Max Roser (2021) Data on COVID-19 (coronavirus) by Our World in Data. England: Our World in Data.
- Maxouris REaC (2021) What we know and don't know about the Omicron variant. UK: CNN Health.
- trtworld (2021) Two cases of Omicron variant detected in Britain – latest updates. 27 Nov 21 ed.
- Fox M (2021) Coronavirus variants: Here's what we know. 1 Dec 2021 ed. Uk: CNN Health.
- Ledford ECH (2021) How bad is Omicron? What scientists know so far. US: Nature.
- Rob Picheta C (2021) The first cases of the Omicron variant identified around the world. London: CNN.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0
![]()