

Review Article
The Contagious Nature of SARS-CoV-2 Omicron Variant and Vaccine Efficacy
Shahab Ahmad Khan1, Ijaz Ahmad2*, Wajid Khan1, Hayat Khan3, Abdullah1, Sadiq Akbar1
Adv. life sci., vol. 9, no. 4, pp. 429-436, December 2022
*– Corresponding Author: Ijaz Ahmad (Email: Ijazahmad383@gmail.com)
Authors' Affiliations
2. Department of Microbiology, Abasyn University Peshawar, Peshawar- Pakistan
3. Department of Microbiology, University of Swabi, Swabi- Pakistan
[Date Received: 05/06/2022: Date Revised: 28/10/2022; Date Published: 31/12/2022]
Abstract![]()
Introduction
Methods
Discussion
Conclusion
References
Abstract
Since the first coronavirus disease-19 (COVID-19) outbreak, variants of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have continued to dominate the global population. The repeated waves of emerging variants, each replacing the previous one with a greater rate of transmissibility and mutations, are the primary cause of the global pandemic. Public health concerns dramatically rose when a highly mutated variant, omicron (B.1.1.529) emerged in late 2021. Omicron has more than 50 mutations, and over 30 mutations are in their spike protein that contributes to the virologic characteristics of the variant. Omicron is more contagious than previously reported SARS-CoV-2 strains and can re-infect people who have already contracted other SARS-CoV-2 infections. The variant has acquired a unique immune escape mechanism against monoclonal antibodies and vaccines. Currently, there are no specific therapeutic drugs or vaccines available to prevent omicron infection and sub lineages emergence. The review was designed to search the recent research or literature papers and compile the most pertinent data on the virologic characteristics of the variant of concern. The study reviewed and discussed the present prevalence, infectivity, dominance, immune evasion, therapeutic options, vaccine efficacy, and the future prospect of the omicron variant. Omicron variant has become a global public health concern due to the emergence of highly mutated sub lineages. Developing variant-specific therapeutic drugs or vaccines is desirable to prevent the spread of these contagious variants globally.
Keywords: COVID-19; SARS-CoV-2; Omicron variant; Vaccine efficacy; Immune evasion
Introduction![]()
The coronavirus disease-19 (COVID-19) was initially reported in December 2019 from China’s Wuhan City and then spread across the world. Later on March 11, 2020, the Covid-19 pandemic was declared upon reporting from many countries [1]. Since the Covid-19 pandemic, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) worldwide, has caused millions of deaths and severe hospitalizations [2]. After the influenza pandemic in 1918, Covid-19 has appeared to be the leading world health crisis. Globally the SARS-CoV-2 infections have created a significant challenge for healthcare workers and researchers due to the contagious nature and incessant mutation in the viral genome since its emergence [3]. The repeated waves of newly emerging SARS-CoV-2 variants, each of which replaced the previous one with a greater rate of transmissibility and mutations, were the major cause of the global pandemic [4]. SARS-CoV-2 is mostly transmitted through close contact with the infected persons, either symptomatic, asymptomatic, or pre-symptomatic, having the virus in their respiratory droplets [5]. The incubation period for SARS-CoV-2 ranges from 5 to 14 days. However, most patients develop symptoms on the 11th days after infection [5]. The symptoms for the symptomatic patients include fever, cough, sore throat, shortness of breath, loss of taste, smell, nausea, myalgia, and malaise [6]. Similar symptoms were also reported for the infection caused by emerging variants [5].
In late 2020, the World Health Organization (WHO) identified the various variant of SARS-CoV-2 including Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), and Delta (B.1.617.2) [4]. In November 2021, a highly transmissible and mutated variant of omicron (B1.1.529) emerged in Botswana, and South Africa and abruptly spread across the world [7]. In contrast to the other variants, omicron has more than 50 mutations, including over 30 in their spike protein, many of which are present in the receptor-binding domain (RBD), that help in substantial immune escape [8]. Among the RBD mutations, the N501Y and Q498R have a higher receptor binding affinity for the angiotensin-converting enzyme (ACE-2), which makes the variant more transmissible and contagious [9]. A preliminary shred of evidence in clinical studies has documented that the higher transmissibility and immune evasion mechanism in the omicron variant could lead to severe consequences [10, 11]. Studies showed that the omicron variant escapes from humoral immunity elicited by either infection or vaccination [4]. According to Chinese scientists, the omicron variant in vitro studies have an immune evasion mechanism from mutations at N440K, T478K, and N501Y amino acid residues [12]. Omicron was classified as a variant of concern (VOC) due to its higher rate of infectivity, which is more than ten times higher than the original SARS-CoV-2 and two times than the Delta variant [13, 14]. Extensive research has been done to observe the transmission mechanisms of these variants, reinfection, presenting symptoms, immune evasion, and disease severity [15, 16, 17]. It is terrifying that cases of omicron infection are on the rise globally and possibly the disease may cause a tremendous burden on the fragile healthcare system that has already been harmed by the SARS-CoV-2 pandemic [18, 19]. The higher number of mutations in the omicron variant has raised overwhelming concerns within medical and scientific communities [20]. Therefore, the purpose of this review was to summarize the pathogenicity, transmissibility, and therapeutic options along with vaccine efficacy against the contagious SARS-CoV-2 omicron variant. We also discussed the disease’s prevalence, preventive measures, and prospects.
Methods![]()
Literature Search and Selection Criteria
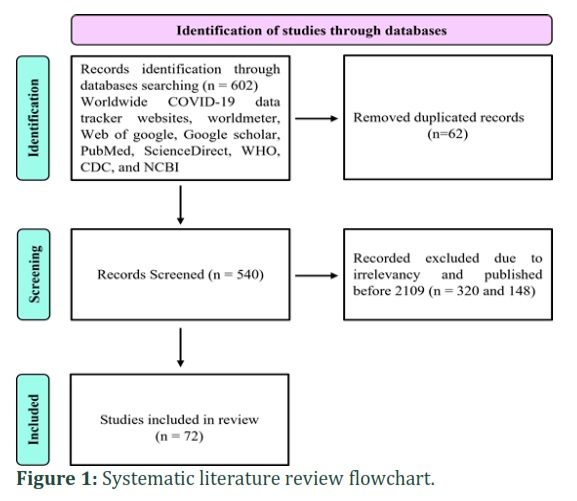
The most current publications and data reports on variants of concern (VOC) were included in the study. The related research articles were collected from the worldwide COVID-19 data tracker websites, Webs of Google, Google Scholar, PubMed, Preprint, World Health Organization (WHO), Center for Disease Control and Prevention (CDC), and National Center for Biotechnology Information (NCBI) Databases. We used the keywords of omicron variant, vaccine efficacy against VOC, therapeutic option, COVID-19, and SARS-CoV-2. In all, 602 papers were accessed; however, 62 were disregarded because of duplication. The remaining papers' titles and abstracts were analysed by the authors, among them, 320 and 148 papers were excluded respectively because of irrelevance and published before 2019. The remaining 72 most recent and relevant papers were included in the study. We also accessed multiple data tracker websites such as worldometer, statistica, update of COVID, etc., and the most cited data sites globally were included in the study shown in Figure 1.
Causes of Viral Mutations
Among the RNA viruses that undergo rapid mutations, SARS-CoV-2 and influenza have been reported as the most mutated viruses [9]. During a pandemic-like situation, viruses continuously replicates and spreads to the environment, which causes an excessive rate of viral transmissions [21]. Thus, any error during the replication process can lead to mutations affecting the characteristics of the virus in virulence, transmission, and immune escape [22]. SARS-CoV-2 has the highest number of replications, with over one billion copies in an infected individual. Hence, it has more chances of genomic mutations [23]. Viral mutation can occur either by antigenic drift or shift. In the antigenic drift mechanism, genes undergo arbitrary copying errors that lead to alteration in virus surface proteins and antigens. In contrast, in the antigenic shift, two different but related virus strains simultaneously affect one cell. During the re-assortment of the viral genome, segments combine and produce a new variant [24]. The entry mechanism of omicron into the host cell is through the endocytic pathway, whereas the Delta variant uses the transmembrane serine protease 2 (TMPRS22) [25]. TMPRS22 is strongly expressed in alveolar lung cells, and omicron may not depend on this route for reproduction, which might result in minor or nonexistent lung involvement after exposure [26]. The differences in host cell infectivity mechanisms may have contributed to the SARS-CoV-2 variant's disease presentation. The formation of syncytia (cell fusion) was more in Delta infection than omicron variant; therefore, Delta variant had a severity in the clinical manifestation and tissue tropism [27].
SARS-COV-2 Variants Classification
Since 2020, the World Health Organization (WHO) has classified distinct variants of SARS-CoV-2 into the variants of interest (VOI) and the VOC. Currently, the VOI includes the Lambda C.37 and Mu B.1.621 variants, while the VOC includes the Alpha B.1.1.17, Beta B.1.351, Gamma P.1, Delta B.1.617.2, and omicron B.1.1.529 variants [28]. Among them, the VOC pathogenicity is more severe with a higher rate of infectivity, antibody escape, and failure or insufficient response to treatment [29].
The Omicron (B.1.1.529) Variant
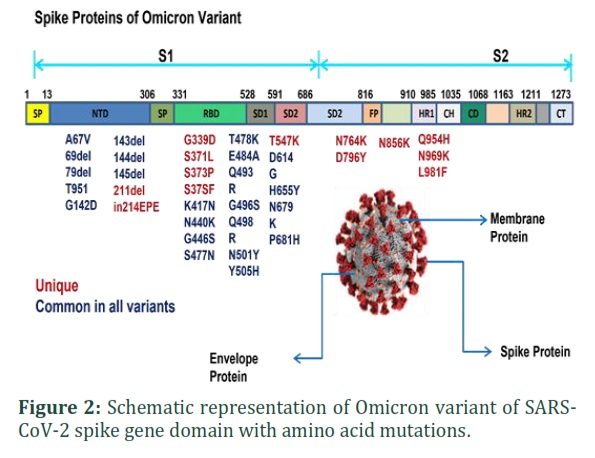
Omicron as VOC has been classified into two major clades and lineages, the Nextstrain clades and Pango lineages. These lineages of omicron have rapidly split up further into sub-variant lineages. In the Nextstrain clade, the subclades of omicron are 21K, 21L, 21M, 22A, 22B, 22C, and 22D. The Pango lineage includes sub-lineages of BA.1.1, BA.2, BA.2.12.1, BA.4, BA.5, BA.2.75, BJ.1, BA.4.6, XBB, and BA.2.3.20 [30, 31]. The omicron variant is of broad concern to the world today because of the multiple mutations in the viral genome [32]. Many of these mutations are within the RBD. These mutations have a significant impact on escaping from host cell receptors and antibody evasion against SARS-CoV-2 [33]. Omicron spike protein secures a maximum of 36-point mutations, three deletions, and one insertion mutation compared to the initial SARS-CoV-2 spike proteins shown in Figure 2 [34]. Among these mutations, 15 mutations are in the RBD, including 10 of them in the receptor-binding motif [34]. The mutations in the receptor-binding motif directly interact with most monoclonal antibodies (mAbs) and human ACE-2 [35, 36]. In contrast, dominant Delta variant has seven mutations in the spike protein and only two mutations in the RBD. Therefore, the omicron variant might significantly affect the binding affinity to ACE-2 and the efficacy of mAbs [37]. Because the interaction of the SARS-CoV-2 spike protein with ACE-2 receptor is directly related to the host infectivity [38].
In comparison to the native SARS-CoV-2, the omicron spike protein contains tens of mutations, including all those observed in other major variants [39]. The N-terminal domain of the spike protein is a target site for the therapeutic monoclonal neutralizing antibodies. Any deletions in the N-terminal domain can make the variant more resistant to antibody interaction [39]. The omicron variant currently experiences six deletions in the N-terminal domain, such as 69, 70, 143, 144, 145, and 211 [40]. Deletion 211 is unique to omicron, while the rest are found in other major variants. The mutations in the N-terminal domain are A67V, T95I, and G142D. Insertion is present at the position of 214, which includes three amino acids in the viral genome [40]. The RBD of spike proteins has direct contact with the host ACE-2 receptor and represents a key role in virus transmissibility [41]. There are four mutations in the RBD: E484A, N501Y, S477N, and K417N [42]. In addition, omicron shares several mutations with other variants, specifically on the furin cleavage region, including H655Y, T547K, P681H, and N679K. The mutations D796Y, L981F, N764K, N856K, N969K, and Q954H are within the S2 subunit [40]. The omicron variant has a significant evolution advantage with a sophisticated level of secondary attack and an increased reproduction rate compared to the Delta variant [43]. Wang and Cheng reported that the sequence analysis of the Omicron variant has two sub-clades and suggested that it is from the 20B clade of SARS-CoV-2 instead of the delta variant [27]. Phylogenetic analysis revealed that omicron is interrelated to the gamma variant via the multiple sequence alignment program on signature mutations [44]. The mutated omicron variants have upraised public health concerns worldwide [45].
Infectivity Value (R˚) and Effective Reproduction number (Re) of Omicron Variant
R˚ (R naught) represents an epidemiological term that shows the contagiousness of an infectious disease by measuring the number of replications. The value is derived from the infectivity period of infection with the mode of transmission, the type of contact, and the state of herd immunity [46]. The R˚ of the original COVID-19 was between 2.4 to 2.6, and for the Alpha strain, it was 4 to 5 [47]. It was 5 to 8 for the Delta variant, in contrast, the R˚ of omicron was reported up to 10 by the experts in the London School of Hygiene and Tropical Medicine [30, 31]. This was further supported by Burki as well [48]. These data shows that the omicron variant (B.1.1.529) is more contagious than all SARS-CoV-2 variants, as well as smallpox, which had an R˚ of 4 to 6. However, the R˚ of omicron is lower than that of measles, frequently cited as 12 to 18 [49, 50]. Omicron’s effective reproduction number (Re) is higher than other SARS-CoV-2 variants [51]. The reports in the early days of the outbreak suggested that the omicron Re was ranged from 1.5 to 3. The omicron Re is recently reported to be lower than 1; however, the latest estimates should not be taken for granted because several factors might have contribution to it, and shreds of evidence suggest that omicron has greater potential to re-emerge and cause infections [52].
Prevalence of COVID-19 Omicron Variant
On March 6, 2022, a worldwide report revealed over 433 million confirmed cases of the omicron variant, including over 5.9 million deaths. The Western Pacific Region had a progressive increase of 46% in morbidity at the regional level, while the other areas experienced a minor decline [53]. The weekly fatalities rate increased in the Western Pacific and Eastern Mediterranean areas, while a drop was reported from the continents, such as Africa at 39%, Europe at 15%, the United States of America at 9%, and South-East Asia at 3%, respectively [53]. As of October 5, 2022, the worldwide COVID-19 prevalence has surpassed 624 million cases, with a higher rate in the United States, India, France, Brazil, and Germany, with over 30 million cases, respectively [54]. The data further showed that until now, Pakistan had reported over 1.5 million confirmed cases, including 32 thousand deaths. On January 27, 2022, 68,624 people tested with 8,183 positive and 30 death cases for COVID-19, which was the most significant prevalence in Pakistan [55].
Diagnostic Test for Omicron Variant
The Reverse Transcription Polymerase Chain Reaction (RT-PCR) is one of the standard tests for detecting COVID-19 variants [56]. The effectiveness of the rapid antigen detection tests (RADTs) has been reported even at a lower dilution to detect the omicron variant [56]. Omicron may be screened using RT-PCR-based S-gene target failure (SGTF) tests that cannot detect the S-gene with deletions of 69 and 70 amino acid residues. RT-PCR single nucleotide polymorphism assay can also be utilized to detect VOC, including omicron [57]. The United States Food and Drug Authority (FDA) has listed the identified molecular tests which might be impacted by the omicron variant [58]. Real-time RT-PCR is currently the widely used test that can easily detect the omicron variant, while in this regard, the RADTs may require additional studies [57].
Comparison of Omicron with Other Variants
Recent studies showed that omicron's severity was lesser than other variants in post-hospitalization and disease symptoms. The current risk for omicron hospitalization ranges from 40% to 80%, which is lesser than that for Delta variant [58]. In fully vaccinated people, omicron is possibly not causing severe infections, specifically in those who have received booster doses [59]. Most reported cases were of mild illness or even clinically asymptomatic. The Hong Kong University researchers revealed from their ex-vivo culture studies that the omicron replication rate is 70 times faster in a human bronchus. In contrast, the Delta variant is ten times slower in human lung tissue. In infected patients, it might represent the reason for omicron’s lower disease severity [60, 61]. Omicron exhibits mild clinical characteristics in cases of reinfection; the risk of hospitalization was 29% lower in the omicron-infected individuals’ than those of the early strain’s infections, as stated by a South African private health insurer department in Johannesburg on the 4th of December [62].
Therapeutic Options
Currently, there are no effective antiviral drugs are available, although many compounds have shown effectiveness against SARS-CoV-2 [63]. The FDA has issued some of them as emergency use authorization for the treatment of COVID-19. The antiviral drug Paxlovid with the combination of nirmatrelvir and ritonavir, are approved for oral therapy to inhibit viral protein [64]. Paxlovid is recommended by the National Institutes of Health (NIH) as the first-line therapy for mild-to-moderate COVID-19 patients of 12 years age and older at high risk of the disease [65]. Molnupiravir is a nucleoside analogue that has been given emergency use authorization for high-risk people older than 65 years of age [64].
Similarly, Remdesivir is a second-choice drug for non-hospitalized high-risk COVID-19 patients at least 12 years of age [66]. The effectiveness of drugs against the omicron variant is currently being investigated, and the efficacy of bioequivalent monoclonal antibodies against omicron has not been thoroughly investigated. Some reports show the effectiveness of Sotrovimab, neutralizing antibodies against omicron [67]. The effect of currently available monoclonal neutralizing antibodies, such as Sotrovimab, Etesevimab, and Bamlanivimab needs to be assessed thoroughly. There are currently no clinical or laboratory data on the efficacy of remdesivir and other more recent oral antivirals against omicron [68]. The non-structural proteins of the virus may serve as a therapeutic target for future drug discoveries [69].
Vaccine Efficacy to Omicron Variant
Omicron has more spike mutations than the original SARS-CoV-2 strain. Therefore, the vaccines designed against the other variants might be compromised because omicron has a vast ability to evade neutralizing antibodies, and the vaccine's effectiveness [69]. The mRNA vaccines such as Moderna and mRNA-1273 encode the entire spike protein of the SARS-CoV-2 strain. Hence, the neutralization titer of antibodies against the omicron variant was reported 35 times lower than those against the original SARS-CoV-2 strain following two doses of the vaccine mRNA-1273. However, neutralization titers against omicron were 20 times greater after the third dose of the mRNA-1273 vaccination [70]. The mRNA-1273, mRNA-1273.211, and mRNA-1273.213 booster doses all at 100µg, produced nearly identical neutralizing titers against the omicron variant with 2.5 to 2.6 times higher than of 50µg booster dose [71]. The sub lineages BA.2.12.1, BA.4, and BA.5 have shown stronger antibody neutralization than BA.2 against both the plasma from three-dose vaccinations and infections following vaccination. Because of this, it was suggested that an omicron BA.1-based vaccination would not be the best antigen to produce broad-spectrum protection against new omicron sub lineages[71, 72].
People who received two doses of an inactivated vaccine cannot counter omicron transmission by producing immune molecules [73]. Laboratory evidence suggests that the most widely used COVID-19 vaccines globally have limited or no response to the rapidly spreading omicron variant infection. Individuals receiving inactivated vaccines with a third dose produce a moderate level of neutralizing antibodies that provide potent protection against viral infection [73]. Although, the booster dose of mRNA and purified protein-based vaccines seem to retain better protection against omicron infection [72]. A nationwide cohort study from Denmark on vaccine effectiveness estimated for Pfizer BioNTech-Comirnaty and Moderna, mRNA-1273 with 55% and 37% respectively against the omicron variant infection [73].
At all post-vaccination intervals and for all combinations of primary courses and booster doses examined, the omicron variant vaccine efficacy was lower than that of the Delta variant [72, 73]. Similarly, the study on vaccines effectiveness in England-based 204036 symptomatic omicron cases resulted from those individuals who received two doses of Pfizer BioNTech-Comirnaty vaccine, the effectiveness of the first dose was 63% which retained two to four weeks, whereas effectiveness dropped to 10% after 25 weeks of the second dose. For individuals who had received two doses of mRNA-1273, the vaccine effectiveness was 68% retaining for two to four weeks and dropped to 7% after 25 weeks of the second dose [74]. The efficacy of the AstraZeneca-Vaxzervria vaccine among those who received two doses exhibited no preventive effect after 20 weeks in the symptomatic infection of omicron. However, individuals who received AstraZeneca-Vaxzervria as the primary course and Pfizer BioNTech-Comirnaty vaccine as a booster dose recorded 64% efficacy and 69% in those who had Pfizer BioNTech-Comirnaty as the primary course [74]. Uncertainty exists over the effectiveness of the available vaccinations in protection against the omicron sub lineages. The currently available data indicated that the BA.2.12.1, BA.4, and BA.5 subvariants evade neutralizing antibodies to a large amount, produced by both infection and immunization [69].
Medicinal Compounds used as Inhibitors Against Omicron Variant
The omicron variant poses a substantial health threat globally because of the less therapeutic efficacy of universal vaccines [75]. The omicron variant’s RBD has the maximum number of mutations, which increases the likelihood of reinfections [76]. The disease condition has become more difficult due to the emergence of omicron variant sub lineages, necessitating the urgent discovery of some effective therapies [77]. Hakami et al., have discovered four novel and effective pharmacological compounds from sources of medicinal plants [78]. By concentrating on the RBD of the spike protein from SARS-CoV-2 and docking them against the omicron variant, they discovered the antiviral properties of plant compounds [79]. Similarly, the efficacy of L-theanine derivatives from the tea plant against the SARS-CoV-2 variants, including omicron, was reported. According to the study, the compound suppresses the major protease of SARS-CoV-2 and ACE2 activities [80]. Naturally occurring compounds from various plant extracts showed an inhibitory effect against the non-structural proteins (nsp7, nsp8) of the omicron variant [81]. Studies are being conducted to fully investigate the exact mechanisms and inhibitory effect of different natural compounds against the emerging SARS-Cov-2 Variants [82].
Prevention of New Variants from Emergence
SARS-CoV-2 transmission prevention is compulsory to prevent the new variants. Preventive measures should be followed to prevent the emergence of new variants, including social distancing, hand washing with sanitizers, face masks or shields, and avoiding crowded places. The emergence of new variants is incredibly low, reducing viral transmissibility [79]. To avail herd immunity, the availability of SARS-CoV-2 vaccines is crucial worldwide [40]. To assess the increase of prevalence in communities, methods such as molecular surveillance, whole-genome sequencing, and spike dropout evaluation are extremely useful in concocting healthcare systems to manipulate recent cases well ahead of time [83].
Figures & Tables
The omicron variant is distinguished due to many mutations in its spike protein which contribute to its high transmission rate, pathogenicity, and reinfection. Currently, no therapeutic drugs or vaccines are available against the SARS-CoV-2 omicron variant. The quick replication and higher transmission rate with emerging omicron sublineages worldwide have raised public health concerns. The decline in viral transmissibility is crucial to contain and prevent the emergence of new variants. In particular, the development of novel therapeutics and variant-specific vaccines may be helpful in preventing the spread of omicron variants.
Author Contributions
Shahab Ahmad Khan, Ijaz Ahmad, and Wajid Khan apprehended the idea, searched the literature, reviewed papers, wrote, and prepared the original manuscript. Ijaz Ahmad designed the methodology, reported the results, reviewed the manuscript, and made corrections to the original draft. Wajid Khan and Hayat Khan reviewed the manuscript, made corrections, and wrote the conclusion. Abdullah and Sadiq Akbar conducted the search strategy and collected data from databases. Ijaz Ahmad supervised the manuscript. Shahab Ahmad Khan, Ijaz Ahmad, and Wajid Khan equally contributed to this work. All authors read and approved the final manuscript. ![]()
No conflict of interest to declare.
![]()
References
- Cucinotta D, Vanelli M, WHO Declares COVID-19 a Pandemic. Acta Biomed: Atenei Parmensis, (2020); 91(1): 157–60.
- Ansori AN, Kharisma VD, Fadholly A, Tacharina MR, Antonius Y, Parikesit AA. Severe Acute Respiratory Syndrome Coronavirus-2 Emergence And Its Treatment With Alternative Medicines: A review. Research Journal of Pharmacy and Technology, (2021); 14(10): 5551-57
- Aleem A, Samad AB, Slenker AK. Emerging variants of SARS-CoV-2 and novel therapeutics against coronavirus (COVID-19). In StatPearls Publishing, (2022); 12.
- Barouch DH. Covid-19 Vaccines-Immunity, Variants, Boosters. New England Journal of Medicine, (2022); 387(11): 1011-20.
- Cascella M, Rajnik M, Aleem A, Dulebohn SC, Di Napoli R. Features, evaluation, and treatment of coronavirus (COVID-19). Statpearls, (2022); 5.
- Stokes EK, Zambrano LD, Anderson KN, Marder EP, Raz KM, Felix SE, Tie Y, Fullerton KE. Coronavirus disease 2019 case surveillance—United States, January 22–May 30, 2020. Morbidity and Mortality Weekly Report, (2020); 6;69(24):759.
- Callaway E. Delta Coronavirus Variant: Scientists Brace For Impact. Nature, (2021); 595(7865): 17-8.
- Sahoo JP, Samal KC. World on alert: WHO designated South African new COVID strain (Omicron/B. 1.1. 529) as a variant of concern. Biotica Research Today, (2021); 293(11): 1086-88.
- Arora S, Grover V, Saluja P, Algarni YA, Saquib SA, Asif SM, Batra K, Alshahrani MY, Das G, Jain R, Ohri A. Literature review of omicron: a grim reality amidst COVID-19. Microorganisms, (2022); 10(2): 451.
- Wang L, Cheng G. Sequence analysis of the emerging SARS‐CoV‐2 variant Omicron in South Africa. Journal of Medical Virology, (2022); 94(4): 1728-33.
- Cele S, Jackson L, Khoury DS, Khan K, Moyo-Gwete T, Tegally H, San JE, et al.,. SARS-CoV-2 Omicron has extensive but incomplete escape of Pfizer BNT162b2 elicited neutralization and requires ACE2 for infection. MedRxiv, (2021); 12.
- Lauring AS, Frydman J, Andino R. The role of mutational robustness in RNA virus evolution. Nature Reviews Microbiology, (2013); 11(5): 327-36.
- Lippi G, Mattiuzzi C, Henry BM. Updated picture of SARS-CoV-2 variants and mutations. Diagnosis, (2022); 9(1): 11-17.
- Cui Z, Liu P, Wang N, Wang L, Fan K, Zhu Q, Wang K, Chen R, Feng R, Jia Z, Yang M. Structural and functional characterizations of infectivity and immune evasion of SARS-CoV-2 Omicron. Cell, (2022); 185(5): 860-71.
- Vaughan A. Omicron emerges, (2021; 7.
- Liu L, Iketani S, Guo Y, Chan JF, Wang M, Liu L, Luo Y, Chu H, Huang Y, Nair MS, Yu J. Striking antibody evasion manifested by the Omicron variant of SARS-CoV-2. Nature, (2022); 602(7898): 676-81.
- Pulliam JR, van Schalkwyk C, Govender N, von Gottberg A, Cohen C, Groome MJ, Dushoff J, Mlisana K, Moultrie H. Increased risk of SARS-CoV-2 reinfection associated with emergence of Omicron in South Africa. Science, (2022); 376(6593): 4947.
- Tracking SARS-CoV-2 Variant: Available from https://www.who.int/en/activities/tracking-SARS-CoV-2-variants, Accessed October 18, 2022.
- Co-Variants: Available from https://covariants.org, Accessed October 18, 2022.
- Mohiuddin M, Kasahara K. Investigating the aggressiveness of the COVID-19 Omicron variant and suggestions for possible treatment options. Respiratory Medicine, (2021); 4: 106716.
- French G, Hulse M, Nguyen D, Sobotka K, Webster K, Corman J, Aboagye‐Nyame B, Dion M, Johnson M, Zalinger B, Ewing M. Impact of hospital strain on excess deaths during the COVID‐19 pandemic—United States, July 2020–July 2021. American Journal of Transplantation, (2022); 22(2): 654-57.
- Chen DY, Kenney D, Chin CV, Tavares AH, Khan N, Conway HL, Liu G, Choudhary MC, Gertje HP, OConnell AK, Kotton DN. Role of spike in the pathogenic and antigenic behavior of SARS-CoV-2 BA. 1 Omicron. BioRxiv, (2022); 1.
- Spinello A, Saltalamacchia A, Borisek J, Magistrato A. Allosteric cross-talk among spike’s receptor-binding domain mutations of the SARS-CoV-2 South African variant triggers an effective hijacking of human cell receptor. The Journal of Physical Chemistry Letters, (2021); 12(25): 5987-93.
- Zhao H, Lu L, Peng Z, Chen LL, Meng X, Zhang C, Ip JD, Chan WM, Chu AW, Chan KH, Jin DY. SARS-CoV-2 Omicron variant shows less efficient replication and fusion activity when compared with Delta variant in TMPRSS2-expressed cells. Emerging microbes & infections, (2022); 31;11(1): 277-83.
- Saito A, Irie T, Suzuki R, Maemura T, Nasser H, Uriu K, Kosugi Y, Shirakawa K, Sadamasu K, Kimura I, Ito J. Enhanced fusogenicity and pathogenicity of SARS-CoV-2 Delta P681R mutation. Nature, (2022); 602(7896): 300-306.
- Youk J, Kim T, Evans KV, Jeong YI, Hur Y, Hong SP, Kim JH, Yi K, Kim SY, Na KJ, Bleazard T. Three-dimensional human alveolar stem cell culture models reveal infection response to SARS-CoV-2. Cell Stem Cell, (2020); 27(6): 905-919.
- Suryadevara N, Shrihari S, Gilchuk P, VanBlargan LA, Binshtein E, Zost SJ, Nargi RS, Sutton RE, Winkler ES, Chen EC, Fouch ME. Neutralizing and protective human monoclonal antibodies recognizing the N-terminal domain of the SARS-CoV-2 spike protein. Cell, (2021); 184(9): 2316-2331.
- Chen J, Wang R, Gilby NB, Wei GW. Omicron variant (B. 1.1. 529): Infectivity, vaccine breakthrough, and antibody resistance. Journal of Chemical Information And Modeling, (2022); 6.
- World Health Organization. The effects of virus variants on COVID-19 vaccines. Available from:https://www.who.int/news-room/feature-stories/detail/the-effects-of-virus-variants-on-covid-19-vaccines, (2021), Accessed March 29, 2022.
- Sender R, Bar-On YM, Gleizer S, Bernshtein B, Flamholz A, Phillips R, Milo R. The total number and mass of SARS-CoV-2 virions. Proceedings of the National Academy of Sciences, (2021); 118(25): e2024815118.
- Paulonis JJ. The Antigenic Shift or Drift of the Influenza Virus. Washington Academy of Sciences. Journal of the Washington Academy of Sciences, (2019); 105(1): 7-12.
- Choi JY, Smith DM. SARS-CoV-2 variants of concern. Yonsei Medical Journal, (2021); 62(11): 961.
- Update on omicron. World Health Organization. Available from: https://www.who.int/news/item/update-on-omicron, (2021), Accessed May 3, 2022.
- He X, Hong W, Pan X, Lu G, Wei X. SARS‐CoV‐2 Omicron variant: characteristics and prevention. Medical Communication, (2020).
- Ettaboina, Santhosh, Nakkala, Komalatha, Chathalingath, Nayana. An investigation on Omicron Variant Corona Virus and its Impact, (2022); 10.46632/psr/1/1/3. (2021).
- Lupala CS, Ye Y, Chen H, Su XD, Liu H. Mutations on RBD of SARS-CoV-2 Omicron variant result in stronger binding to human ACE2 receptor. Biochemical and Biophysical Research Communications, (2022); 590: 34-41.
- Wu L, Zhou L, Mo M, Liu T, Wu C, Gong C, Lu K, Gong L, Zhu W, Xu Z. SARS-CoV-2 Omicron RBD shows weaker binding affinity than the currently dominant Delta variant to human ACE2. Signal Transduction And Targeted Therapy, (2022); 7(1): 1-3.
- European Centre for Disease Prevention and Control. Epidemiological Update: Omicron Variant of Concern (VOC)-Data As of 11 December 2021. Available from: https://www.ecdc.europa.eu/en/news-events/epidemiological-update-omicron-variantconcern-voc-data-11-december-(2021), Accessed October 18, 2022.
- Abbott S, Hellewell J, Thompson RN, Sherratt K, Gibbs HP, Bosse NI, Munday JD, Meakin S, Doughty EL, Chun JY, Chan YW. Estimating the time-varying reproduction number of SARS-CoV-2 using national and subnational case counts. Wellcome Open Research, (2020); 5(112): 112.
- Koleya T, Kumara M, Goswami A, Ethayathulla AS, Hariprasada G. Structural modeling of Omicron spike protein and its complex with human ACE-2 receptor: Molecular basis for high transmissibility of the virus. Biochemical and Biophysical Research Communications, (2022); 7.
- Venkatakrishnan AJ, Anand P, Lenehan PJ, Suratekar R, Raghunathan B, Niesen MJ, Soundararajan V. Omicron variant of SARS-CoV-2 harbors a unique insertion mutation of putative viral or human genomic origin. Preprints, (2021).
- Kannan SR, Spratt AN, Sharma K, Chand HS, Byrareddy SN, Singh K. Omicron SARS-CoV-2 variant: Unique features and their impact on pre-existing antibodies. Journal of Autoimmunity, (2022); 126:102779.
- Sun Y, Lin W, Dong W, Xu J. Origin and evolutionary analysis of the SARS-CoV-2 Omicron variant. Journal of Biosafety and Biosecurity, (2022); 4(1): 33-37.
- Grassly NC, Fraser C. Mathematical models of infectious disease transmission. Nature Reviews Microbiology, (2008); (6): 477-87.
- Hendaus MA, Jomha FA. Delta variant of COVID-19: A simple explanation. Qatar Medical Journal, (2021); (3): 49.
- Burki TK. Omicron variant and booster COVID-19 vaccines. The Lancet Respiratory Medicine, (2022); 10(2): e17.
- Guerra FM, Bolotin S, Lim G, Heffernan J, Deeks SL, Li Y, Crowcroft NS. The basic reproduction number (R0) of measles: a systematic review. The Lancet Infectious Diseases, (2017); 17(12): e420-28.
- Omicron variant global prevalence. Available from https://www.statista.com/statistics/1279100/number-omicron-variant worldwid11742399try, (2022). Accessed on March 8 and October 18, 2022.
- Wolter N, Jassat W, Walaza S, Welch R, Moultrie H, Groome M, Amoako DG, Everatt J, Bhiman JN, Scheepers C, Tebeila N. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: a data linkage study. The Lancet, (2022); 399(10323): 437-46.
- COVID-19 Situation in Pakistan. Update on Omicron. Available from: https://covid.gov.pk, (2022). Accessed October 17, 2022.
- Deerain J, Druce J, Tran T, Batty M, Yoga Y, Fennell M, Dwyer DE, Kok J, Williamson DA. Assessment of the analytical sensitivity of 10 lateral flow devices against the SARS-CoV-2 Omicron variant. Journal of Clinical Microbiology (2022); 60(2) :e02479-21.
- Vogels CB, Breban MI, Alpert T, Petrone ME, Watkins AE, Ott IM, de Jesus JG, Claro IM, Ferreira GM, Crispim MA, Network BU. PCR assay to enhance global surveillance for SARS-CoV-2 variants of concern. MedRxiv, (2021); 12.
- US Food and Drug Administration (FDA). SARS-CoV-2 Viral Mutations: Impact on COVID-19 Tests, (2021). Available from:https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/sars-cov2-viral-mutations-impact-covid-19-tests. Accessed October 16, 2022.
- Omicron SARS-CoV-2 Can Infect Faster and Better than Delta in Human Bronchus but with Less Severe Infection in Lung. Available from https://www. med.hku.hk/en/news/press/20211215-omicron-SARS-CoV-2-infection, (2022). Accessed March 23, 2022.
- Burki T. Booster shots for COVID-19—the debate continues. The Lancet Infectious Diseases, (2021); 21(10): 1359-1360.
- Dyer O. Covid-19: Omicron is causing more infections but fewer hospital admissions than delta, South African data show, (2021).
- Ledford H. How severe are Omicron infections. Nature, (2021); 600(7890): 577-78.
- Khan S, Siddique R, Shereen MA, Ali A, Liu J, Bai Q, Bashir N, Xue M. Emergence of a novel coronavirus, severe acute respiratory syndrome coronavirus 2: biology and therapeutic options. Journal of Clinical Microbiology, (2020); 58(5): e00187-200.
- Therapeutic Drugs against COVID-19. Available from https://www.goodrx.com/conditions/covid-19/coronavirus-treatments-on-the-way. Accessed October 18, 2022.
- Saravolatz LD, Depcinski S, Sharma M. Molnupiravir and nirmatrelvir-ritonavir: oral COVID antiviral drugs. Clinical Infectious Diseases, (2022); 4.
- Ansems K, Grundeis F, Dahms K, Mikolajewska A, Thieme V, Piechotta V, Metzendorf MI, Stegemann M, Benstoem C, Fichtner F. Remdesivir for the treatment of COVID‐19. Cochrane Database of Systematic Reviews, (2021); (8).
- Cameroni E, Bowen JE, Rosen LE, Saliba C, Zepeda SK, Culap K, Pinto D, VanBlargan LA, De Marco A, di Iulio J, Zatta F. Broadly neutralizing antibodies overcome SARS-CoV-2 Omicron antigenic shift. Nature, (2022); 602(7898): 664-670.
- Aggarwal A, Stella AO, Walker G, Akerman A, Milogiannakis V, Hoppe AC, Mathivanan V, Fichter C, McAllery S, Amatayakul-Chantler S, Roth N. SARS-CoV-2 Omicron: reduction of potent humoral responses and resistance to clinical immunotherapeutics relative to viral variants of concern. MedRxiv, (2021); 1.
- Zang J, Yin Y, Xu S, Qiao W, Liu Q, Lavillette D, Zhang C, Wang H, Huang Z. Neutralizing Potency of Prototype and Omicron RBD mRNA Vaccines Against Omicron Variant. Frontiers in Immunology, (2022); 13: 908478-82.
- Pajon R, Doria-Rose NA, Shen X, Schmidt SD, O’Dell S, McDanal C, Feng W, Tong J, Eaton A, Maglinao M, Tang H. SARS-CoV-2 Omicron variant neutralization after mRNA-1273 booster vaccination. New England Journal of Medicine, (2022); 386(11): 1088-1091.
- Zou L, Ruan F, Huang M, Liang L, Huang H, Hong Z, Yu J, Kang M, Song Y, Xia J, Guo Q. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. New England Journal of Medicine, (2020); 382(12): 1177-79.
- da Silva MK, Fulco UL, da Silva Júnior ED, Oliveira JI. Moving targets: COVID-19 vaccine efficacy against Omicron subvariants. Molecular Therapy, (2022); 30(8): 2644-45.
- Cao Y, Yisimayi A, Jian F, Song W, Xiao T, Wang L, Du S, Wang J, Li Q, Chen X, Yu Y. BA. 2.12. 1, BA. 4 and BA. 5 escape antibodies elicited by Omicron infection. Nature, (2022); 608(7923): 593-602.
- Ahmad I, Khan H, Salman M, Rehman L, Khan SA, Saddam IK, Naeem I, Qazi NU. Modeling interaction between non-structural protein 2 of Chikungunya Virus and various protein factors of innate pathway. Biomedical Letters, (2022); 8(2): 162-9.
- Mohapatra RK, Sarangi AK, Kandi V, Azam M, Tiwari R, Dhama K. Omicron (B. 1.1. 529 variant of SARS‐CoV‐2); an emerging threat: current global scenario. Journal of medical virology, (2022); 94(5): 1780-83.
- Dolgin E. Omicron thwarts some of the world’s most-used COVID vaccines. Nature, (2022); 601(7893): 311.
- Gram MA, Emborg HD, Schelde AB, Friis NU, Nielsen KF, Moustsen-Helms IR, Legarth R, Lam JU, Chaine M, Malik AZ, Rasmussen M. Vaccine effectiveness against SARS-CoV-2 infection or COVID-19 hospitalization with the Alpha, Delta, or Omicron SARS-CoV-2 variant: A nationwide Danish cohort study. PLoS Medicine, (2022); 19(9): e1003992.
- Hansen CH, Schelde AB, Moustsen-Helms IR, Emborg HD, Krause TG, Mølbak K, Valentiner-Branth P. Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish Cohort Study. MedRxiv, (2021).
- Andrews N, Stowe J, Kirsebom F, Toffa S, Rickeard T, Gallagher E, Gower C, Kall M, Groves N, O’Connell AM, Simons D. Covid-19 vaccine effectiveness against the Omicron (B. 1.1. 529) variant. New England Journal of Medicine, (2022); 386(16): 1532-46.
- Muik, Alexander, Bonny Gaby Lui, Ann-Kathrin Wallisch, Maren Bacher, Julia Mühl, Jonas Reinholz, Orkun Ozhelvaci et al.,. "Neutralization of SARS-CoV-2 Omicron by BNT162b2 mRNA vaccine–elicited human sera. Science, (2022); eabn7591.
- Roessler A, Riepler L, Bante D, von Laer D, Kimpel J. SARS-CoV-2 B. 1.1. 529 variant (Omicron) evades neutralization by sera from vaccinated and convalescent individuals. MedRxiv, (2021).
- Alamri MA, ul Qamar MT, Mirza MU, Alqahtani SM, Froeyen M, Chen LL. Discovery of human coronaviruses pan-papain-like protease inhibitors using computational approaches. Journal of pharmaceutical analysis, (2020); 10(6): 546-59.
- Hakami AR. Targeting the RBD of omicron variant (B. 1.1. 529) with medicinal phytocompounds to abrogate the binding of spike glycoprotein with the hACE2 using computational molecular search and simulation approach. Biology, (2022); 11(2): 258.
- Lu J, Zhang Y, Qi D, Yan C, Wu B, Huang JH, Yao J, Wu E, Zhang G. An L-theanine derivative targets against SARS-CoV-2 and its Delta and Omicron variants. Heliyon, (2022); 9:e09660.
- Oreshkova N, Molenaar RJ, Vreman S, Harders F, Munnink BB, Hakze-van Der Honing RW, Gerhards N, Tolsma P, Bouwstra R, Sikkema RS, Tacken MG. SARS-CoV-2 infection in farmed minks, the Netherlands, April and May 2020. Eurosurveillance, (2020); 25(23): 2001005.
- Goc A, Rath M, Niedzwiecki A. Composition of naturally occurring compounds decreases activity of Omicron and SARS-CoV-2 RdRp complex. European Journal of Microbiology and Immunology, (2022); 12(2): 39-45.
- Naidu SA, Mustafa G, Clemens RA, Naidu AS. Plant-derived natural non-nucleoside analog inhibitors (NNAIs) against RNA-dependent RNA polymerase complex (nsp7/nsp8/nsp12) of SARS-CoV-2. Journal of Dietary Supplements, (2021); 17: 1-30.
- Van Egeren D, Novokhodko A, Stoddard M, Tran U, Zetter B, Rogers MS, Joseph-McCarthy D, Chakravarty A. Controlling long-term SARS-CoV-2 infections can slow viral evolution and reduce the risk of treatment failure. Scientific reports, (2021); 11(1): 1-9.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0
![]()