

Full Length Research Article
Natalizumab Antibodies and C-X-C Motif Chemokine Ligand 13 Serum Levels in Multiple Sclerosis Patients
Hadeel Abood Mohammed1, Ahmed Abdul-Hassan Abbas2*, Nawfal Mahdi Shaheed3
Adv. life sci., vol. 12, no. 3, pp. 553-557, August 2025
*- Corresponding Author: Ahmed Abdul-Hassan Abbas (Email: ahmed26770@yahoo.com)
Authors' Affiliations
2. Department of Microbiology, College of Medicine, Al-Nahrain University, Kadhimiya, Baghdad – Iraq
3. Neurology Department, Baghdad Teaching Hospital, Baghdad – Iraq
[Date Received: 22/12/2023; Date Revised: 08/03/2025; Available Online: 31/10/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Natalizumab is a humanized monoclonal antibody that is an established therapy for relapsing–remitting multiple sclerosis (RRMS). A fraction of patients, however, form anti-drug antibodies that have the potential to lessen the efficacy of therapy. To counteract this, the current study aimed to determine the incidence of anti-natalizumab immunoglobulins and examine their relationship with serum levels of C-X-C motif chemokine ligand 13 (CXCL13). Since CXCL13 is a marker of immune activation, determination of levels may provide informative insights on therapeutic effect and interpatient variation.
Methods: The study was conducted between February and September 2021 and included sixty patients with multiple sclerosis who attended the Multiple Sclerosis Center in Baghdad Teaching Hospital and 30 healthy individuals as control group. The patients were on natalizumab for about one year and divided into two groups (30 responders and 30 non-responders); all of them were diagnosed by consultant physicians. Studied markers like CXCL13 and Natalizumab Abs were measured by ELISA.
Results: The presence of anti-natalizumab antibodies in non-responder patients, responder patients, and healthy controls was (5, 0, 0), respectively. There was a statistically significant relationship between the presence of anti-natalizumab and the CXCL13 protein serum level in patients with multiple sclerosis (MS) (p < 0.001).
Conclusion: The presence of anti-natalizumab antibodies and its significant correlation with serum levels of CXCL13 in MS patients could be an informative indicator towards natalizumab treatment.
Keywords: Multiple Sclerosis, C-X-C motif chemokine ligand 13, Natalizumab
Introduction![]()
Natalizumab is a monoclonal antibody (IgG4κ class) and is used as a medication against the α4-integrin. It is also the first drug that implemented a molecularly targeted approach for treating RRMS. Through selective blockade of very late antigen-4 (VLA-4), natalizumab inhibits activated leukocytes from attaching to the vascular endothelium, thus preventing them from crossing the blood-brain barrier and entering the central nervous system (CNS). Through interrupting this key step in immune cell trafficking, inflammatory infiltration is reduced effectively, limiting demyelination and neurodegeneration in MS [1].
Even though therapeutic, a minority of patients develop anti-drug antibodies to natalizumab, most frequently within the first three months after initiation of therapy. These antibodies, particularly those of a neutralizing nature, are highly effective at decreasing circulating concentrations of natalizumab, diminishing drug access and therapeutic effect. Recurrent antibody production is characteristically accompanied by increased relapse activity and elevated therapy discontinuation rates [2]. Although overall rates of neutralizing antibody formation are relatively low (approximately 6%), impacts on long-term control of disease warrant periodic monitoring of immunogenicity in therapy with natalizumab [3,4].
Amongst candidate biomarkers for therapeutic response, CXCL13 has attracted significant interest. CXCL13 is a strong chemotactic cue for B lymphocytes in MS that promotes directed migration into inflamed CNS tissues. Elevated CSF levels of CXCL13 have, in numerous studies, correlated with disease activity and immune dysfunction. Its detectable presence not merely echoes chronic inflammatory activity but could, in addition, be a predictive indicator of therapeutic effect [5]. Monitoring serum or CSF levels of CXCL13 could, therefore, yield useful information about therapeutic responsiveness and underlying immunodynamics during natalizumab therapy.
Methods![]()
The present research work included sixty patients with MS who attended the Multiple Sclerosis Center in Baghdad Teaching Hospital during the period February 2021–September 2021.
All 60 patients had relapsing–remitting multiple sclerosis (RRMS) that was diagnosed by consultant physicians according to MacDonald’s criteria. The patients included in the study received natalizumab for about one year and were divided into two groups (30 responders and 30 non-responders). Patients were classified based on clinical and radiological responses. Responders had no relapses and no new or enhanced MRI lesions during natalizumab therapy, whereas non-responders experienced one or more relapses or new lesion activity despite treatment. The MS patients having various chronic illnesses were excluded from the study. The samples for the control group were collected from apparently healthy volunteers (30 individuals) at the blood donor center in Al-Yarmouk Teaching Hospital and from healthy relatives’ volunteers who matched the patient group in age and sex, as well as had no chronic or systemic diseases.
2 mL of whole blood was collected from all multiple sclerosis patients and controls. ELISA was used for the detection of studied markers (C-X-C motif chemokine ligand 13, Natalizumab Abs).
Ethical standards
The institutional review board IRB (2020-1099) in the College of Medicine at Al-Nahrain University approved the current research work. Written informed consent was attained from individuals who contributed to this study. The authors approve that pertinent principles and guided procedures were kept in mind during the completion of the current research work.
Statistical Analysis
Data were coded and entered into the computer using Microsoft Excel Software and analyzed using the Statistical Package for Social Sciences (SPSS) version 26 for statistical analysis. Categorical data were described as counts and percentages, and the Chi-square test was used to outline the relationship between these data. The significance level was set at p ≤ 0.05.
Results![]()
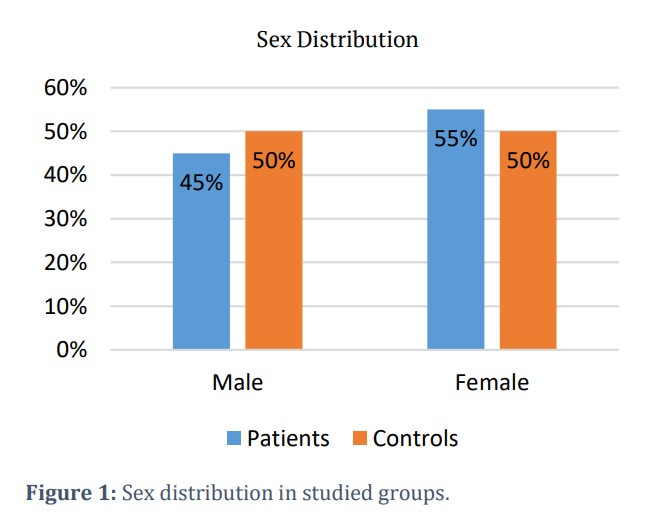
In the present study, the occurrence of multiple sclerosis was higher among females compared to males. The count of female cases was 33 (55.0%) while the count of male cases was 27 (45.0%) (Figure 1).
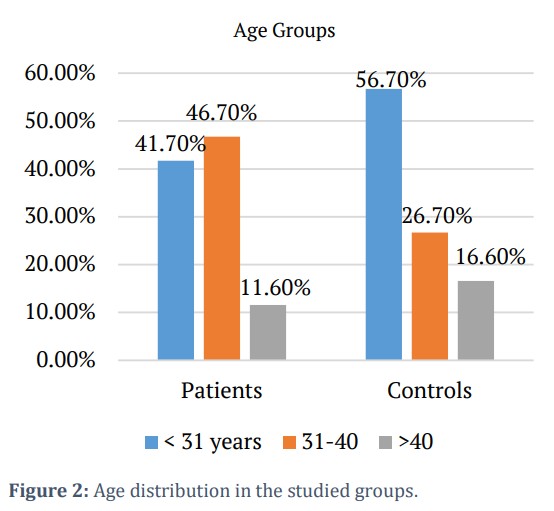
There were three age groups, with the largest age group being: 31-41 years with 28 patients (46.7%), followed by: < 31 years, which comprises 25 patients (41.7%), and 7 (11.6%) patients within the age group > 40 years (Figure 2). There were no statistically significant differences between the mean age of MS patients and the control group (P = 0.602).
On the other hand, the current study showed a statistically significant difference between patients and the control group, as well as between responders and non-responders regarding the seropositivity of anti-natalizumab Ab.
The frequency of natalizumab Ab in MS patients (Nonresponder, Responder) and healthy controls was 5 (16.7 %), 0 (0.0 %), and 0 (0.0 %), respectively. Whereas the total of negative cases among the non-responder group, responder, and healthy control was 25 (83.3%), 30 (100%), and 30 (100 %), respectively (Table 1).
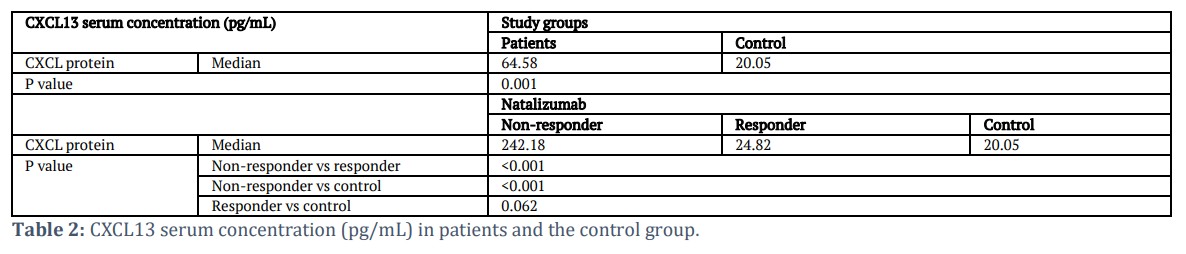
In addition, CXCL13 levels were higher among MS patients in comparison with the healthy group (P value < 0.001), also there was a significant difference between the non-responding and responding group (P value < 0.001), as shown in Table 2.
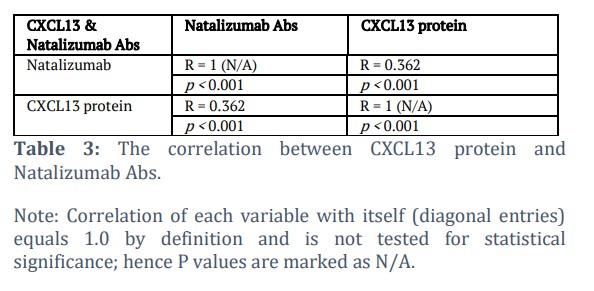
The study also demonstrated a statistically significant correlation between the presence of anti-natalizumab antibodies and serum CXCL13 levels (p < 0.001) (Table 3).
Figures & Tables

Clinical studies have indicated that almost 9% of patients with MS administered natalizumab form anti-drug antibodies, a reaction that is associated with reduced circulating natalizumab concentrations, reduced drug efficacy, and resultant diminished therapeutic effect [6]. In the present study, 16.7% of non-responder MS patients were seropositive for anti-natalizumab antibodies, while neither responder patients nor healthy controls demonstrated seropositivity.
Polman CH et al. (2006) noted that in a two-year follow-up, 57 patients on natalizumab therapy generated antibodies at least once. Among them, 37 patients (6%) had persistent antibodies, comprised of those detectable at two or more time points with ≥ 42 days interval between them. Persistent antibodies were correlated with higher incidence of infusion-related adverse effects as well as significant loss in therapeutic efficacy [7]. Likewise, Vennegoor A et al. (2013) noted that antibodies were generated by 58% of the patients on natalizumab, all within the initial 24 weeks of therapy. These antibodies inversely correlated with natalizumab serum levels (p < 0.001) [8]. Results from a phase III study by Deisenhammer F et al. (2019) also noted that elevated baseline anti-drug antibody (ADA) titers predicted long-term persistence, and those patients with sustained ADA often had undetectable drug levels on continued therapy, implicating significant therapeutic failure [9].
CXCL13, a potent B-cell chemoattractant, has been proposed as a biomarker across multiple immune-mediated disorders, including MS, where its levels can rise considerably (Sellebjerg et al., 2009) [10]. In the current analysis, a strong and statistically significant association was demonstrated between anti-natalizumab antibody presence and serum CXCL13 concentrations in non-responder MS patients (p < 0.001). DiSano KD et al. (2020) identified that for the future activity of MS in patients, CXCL13 is a robust predictor (p = 0.0002), with activity-positive patients displaying markedly higher CXCL13 levels compared to activity-negative counterparts (p < 0.0001) [11]. Consistently, Festa ED et al. (2009) reported a positive correlation between serum CXCL13 concentrations and MRI activity both in the first year (R = 0.33, p < 0.05) and over a two-year follow-up (R = 0.35, p < 0.01) [12]. Khademi et al. (2011) further demonstrated that CXCL13 expression, when evaluated in 465 MS patients relative to healthy and neurological disease controls, was associated with higher relapse rates, greater disability scores (EDSS), and increased lesion burden [5].
Subsequent studies have confirmed these results. Sellebjerg et al. (2009) found raised CSF concentrations of CXCL13 in patients with RRMS, Clinically Isolated Syndrome (CIS), primary progressive multiple sclerosis (PPMS), and secondary progressive multiple sclerosis (SPMS) but not raised levels of CXCL12, compared to controls. High levels of CSF CXCL13 significantly correlated with B-cell numbers, markers of immune activation, and clinical disease activity in CIS and RRMS patients. Notably, therapy with a course of high-dose methylprednisolone or with natalizumab reduced CSF CXCL13 concentrations significantly [13]. Likewise, Ferraro D et al. (2015) demonstrated that CSF levels of CXCL13 correlated significantly with CSF leucocyte number, protein content, and IgG index, and that levels ≥15.4 pg/mL had strong predictive value for MS diagnosis and for subsequent clinical relapse within the first year of onset of disease [14].
CXCL13 is a member of the lymphoid chemokine family (CXCL12, CXCL13, CCL19, and CCL21) that governs the migration and organization of B-cells in secondary lymphoid organs both in steady-state and inflammatory settings [15,16]. Primarily produced by stromal cells in the follicles, CXCL13 chemoattracts activated B lymphocytes and CXCR5-positive follicular helper T cells, thereby promoting the development of germinal centers [17-19]. B and T cells release lymphotoxin-α (LTα) that, in turn, upregulates the expression of CXCL13 by stimulation of the follicular dendritic cells (Sellebjerg et al., 2009) [20]. CXCL13 exerts its biological activities by acting on its receptor, CXCR5, that is broadly expressed on the majority of B lymphocytes, some subpopulations of T cells, and transiently upregulated upon T cell activation [21,22]. By promoting lymphocyte recruitment, CXCL13 directly contributes to the infiltration of the CNS and lesion formation in MS, and evidence exists that supports local synthesis within active demyelinating lesions. Together, the measured positivity for anti-natalizumab antibodies and their strong correlation with serum CXCL13 concentrations in MS subjects could be a useful indicator of response to therapy with natalizumab.
Acknowledgement
We genuinely appreciate the worthwhile assistance from all the patients, their families, as well as staff from the involved units for making the study a success. Special thanks are also directed at hospital staff for helping us procure the required samples, especially in the difficult situations brought about by the COVID-19 pandemic.
Author Contributions
Hadeel Abood Mohammed: Conducted the lab tests of the research and prepared the initial version of this manuscript.
Dr. Ahmed Abdul-Hassan Abbas: Designed and supervised the project for the preparation of the final manuscript.
Nawfal Mahdi Shaheed: Facilitated the collection of samples and clinical assessment.
Authors confirm that there is no financial or non-financial conflict of interest that could have had any influence on the work published in this paper. Personal, professional, or institutional relationships were not involved that could be understood as having any effect on the study's objectivity, data analysis, or results.![]()
References
- McCormack PL. Natalizumab: a review of its use in the management of relapsing-remitting multiple sclerosis. Drugs, (2013); 73(13): 1463-1481.
- Hegen H, Auer M, Deisenhammer F. Predictors of Response to Multiple Sclerosis Therapeutics in Individual Patients. Drugs, (2016); 76(15): 1421-1445.
- Sehr T, Proschmann U, Thomas K, Marggraf M, Straube E, et al. New insights into the pharmacokinetics and pharmacodynamics of natalizumab treatment for patients with multiple sclerosis, obtained from clinical and in vitro studies. Journal of neuroinflammation, (2016); 13(1): 164.
- Kaufmann M, Haase R, Proschmann U, Ziemssen T, Akgün K. Real-World Lab Data in Natalizumab Treated Multiple Sclerosis Patients Up to 6 Years LongTerm Follow Up. Frontiers in neurology, (2018); 9(2018): 1071.
- Khademi M, Kockum I, Andersson ML, Iacobaeus E, Brundin L, et al. Cerebrospinal fluid CXCL13 in multiple sclerosis: a suggestive prognostic marker for the disease course. Multiple Sclerosis Journal, (2010); 17(3): 335-343
- Sorensen PS, Jensen PH, Haghikia A, Lundkvist M, Vedeler C et al. Occurrence of antibodies against natalizumab in relapsing multiple sclerosis patients treated with natalizumab. Multiple Sclerosis Journal, (2011); 17(9): 1074-1078.
- Polman CH, O’Connor PW, Havrdova E, Hutchinson M, Kappos L, et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. New England Journal of Medicine, (2006); 354(9): 899-910.
- Vennegoor A, Rispens T, Strijbis EM, Seewann A, Uitdehaag BM, et al. Clinical relevance of serum natalizumab concentration and anti-natalizumab antibodies in multiple sclerosis. Multiple Sclerosis Journal, (2013); 19(5): 593-600.
- Deisenhammer F, Jank M, Lauren A, Sjödin A, Ryner M, et al. Prediction of natalizumab anti-drug antibodies persistency. Multiple Sclerosis Journal, (2019); 25(3): 392-398.
- Alvarez E, Piccio L, Mikesell RJ, Klawiter EC, Parks BJ, et al. CXCL13 is a biomarker of inflammation in multiple sclerosis, neuromyelitis optica, and other neurological conditions. Multiple Sclerosis Journal, (2013); 19(9): 1204-1208.
- DiSano KD, Gilli F, Pachner AR. Intrathecally produced CXCL13: A predictive biomarker in multiple sclerosis. Multiple Sclerosis Journal–Experimental, (2020); 6(4): 2055217320981396.
- Festa ED, Hankiewicz K, Kim S, Skurnick J, Wolansky LJ, et al. Serum levels of CXCL13 are elevated in active multiple sclerosis. Multiple Sclerosis Journal, (2009); 15(11): 1271-1279.
- Sellebjerg F, Bornsen L, Khademi M, Krakauer M, Olsson T, et al. Increased cerebrospinal fluid concentrations of the chemokine CXCL13 in active MS. Neurology, (2009); 73(23): 2003-2010.
- Krumbholz M, Theil D, Cepok S, Hemmer B, Kivisäkk P, et al. Chemokines in multiple sclerosis: CXCL12 and CXCL13 up-regulation is differentially linked to CNS immune cell recruitment. Brain, (2005); 129(1): 200-211.
- Cyster JG. Chemokines, sphingosine-1-phosphate, and cell migration in secondary lymphoid organs. Annual Review of Immunology, (2005); 23(1): 127-159.
- Okada T, Cyster JG. B-cell migration and interactions in the early phase of antibody responses. Current opinion in immunology, (2006); 18(3): 278-285.
- Zotos D, Coquet JM, Zhang Y, Light A, D’Costa K, et al. IL-21 regulates germinal center B-cell differentiation and proliferation through a B-cell-intrinsic mechanism. Journal of Experimental Medicine, (2010); 207(2): 365-378.
- Crotty S. The 1-1-1 fallacy. Immunological reviews, (2012); 247(1): 133-142.
- Victora GD, Nussenzweig MC. Germinal centers. Annual review of immunology, (2012); 30(1): 429-457.
- Yu P, Wang Y, Chin RK, Martinez-Pomares L, Gordon S, et al. B-cells control the migration of a subset of dendritic cells into B-cell follicles via CXC chemokine ligand 13 in a lymphotoxin-dependent fashion. The Journal of Immunology, (2002); 168(10): 5117-5123.
- Langenkamp A, Nagata K, Murphy K, Wu L, Lanzavecchia A, et al. Kinetics and expression patterns of chemokine receptors in human CD4+ T lymphocytes primed by myeloid or plasmacytoid dendritic cells. European journal of immunology, (2003); 33(2): 474-482.
- Kim CH, Rott LS, Clark-Lewis I, Campbell DJ, Wu L, et al. Subspecialization of CXCR5+ T cells: B helper activity is focused in a germinal center–localized subset of CXCR5+ T cells. The Journal of experimental medicine, (2001); 193(12): 1373-1382.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0

