

Full Length Research Article
Anti-D Antibody Prevalence and Its Role in Hemolytic Disease Among Fetuses and Neonates in Erbil City
Abbas Bahram Younus1, Bestoon Shekhany1,2*, Mohammed Omar Abdullah3, Faruk Suzergoz1
Adv. life sci., vol. 12, no. 3, pp. 564-568, August 2025
*- Corresponding Author: Bestoon Shekhany (Email: bestoon.hamed@epu.edu.iq)
Authors' Affiliations
2. Department of Medical Laboratory Technology, Soran Technical College, Erbil Polytechnic University, Erbil – Iraq
3. Department of Community Health Nursing, College of Health Technology, Cihan University-Erbil, Erbil – Iraq
[Date Received: 17/09/2024; Date Revised: 02/03/2025; Available Online: 31/10/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Hematologists and obstetricians have focused their attention on the Rh antigen alloimmunization, especially the Rh-D antigen, which leads to severe health defects such as haemolytic disease of the fetus and newborn (HDFN). This study aimed to develop a profile for mothers with negative Rh-D who get pregnant with babies with positive Rh-D and to determine the rate of anti-D antibodies.
Methods: In this study, 1028 blood samples were collected from 514 parents, who are mothers with Rh-negative and fathers with Rh-positive, in Erbil city of Iraq, from April 2022 to April 2023. All participating mothers were Rh-negative women married to Rh-positive men, and inclusion was not limited to those with a prior Rh-positive child. However, most participants had experienced at least one pregnancy, and their obstetric histories were recorded through verbal interviews. This ensures that the reported 1.7% prevalence of anti-D antibodies represents all Rh-negative mothers with Rh-positive partners, rather than a pre-selected subgroup. Next, ABO and RhD typing tests were done for all samples (fathers and mothers), and then the Du test and antibody screening were applied to all mother samples.
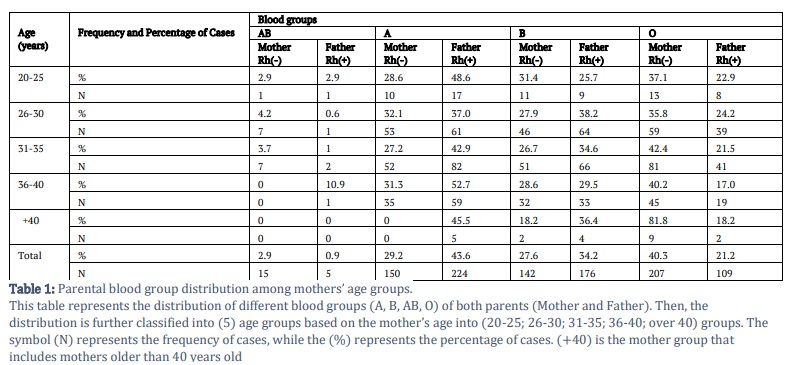
Results: Mothers’ blood samples were divided into age groups: 20-25: 35 (7%), 26-30: 165 (32%), 31-35: 191 (37%), 36-40: 112 (22%), and over 40: 11 (2%). Among Rh-negative mothers, blood group O was most common (40.3%), and AB least (2.9%). Of the nine anti-D–positive mothers, the highest distribution was observed in the 36–40 age group (44%), followed by 26–30 and 31–35 (22% each), and over 40 (11%), with no cases in the 20–25 age group.
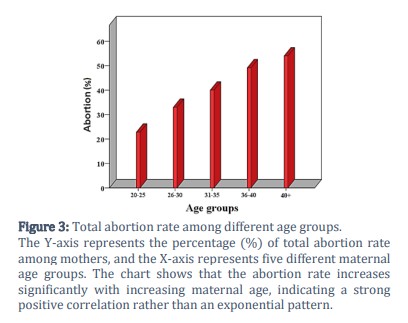
Conclusion: The abortion rate showed a positive correlation with increasing maternal age and pregnancy duration. Anti-D antibodies and other alloantibodies have become the major cause of HDFN. Therefore, primary screening for antibodies, monitoring, and blood transfusion are crucial in order to prevent the severity of the antibody effect on the infant.
Keywords: HDFN, Haemolytic disease, Rh-D, Anti-D, Abortion
Introduction![]()
Erythroblastosis fetalis, often known as haemolytic disease of the fetus and newborn (HDFN), is a haemolytic disorder that mostly affects fetuses with rhesus-positive blood and newborns with rhesus-negative mothers. Due to rhesus or ABO incompatibility between the maternal and fetal blood, alloimmunization occurs, which causes maternal antibodies to attack fetal red blood cells. According to estimates, 3–8 people out of every 100,000 suffer from HDFN each year. Prior to the development of immunoprophylactic medications, HDFN was previously known to result in fetal mortality in 1% of all pregnancies, but if detected early, the disease may now be reasonably successfully controlled with fewer difficulties [1-3]. Mother’s alloantibody results in HDFN, which causes many clinical signs and symptoms such as fetal anemia, hyperbilirubinemia, fetal hydrops, and cardiomegaly [4,5].
After ABO, the rhesus system is the most significant blood group system [6,7]. Only five of the 50 known blood group antigens that comprise the Rh system are significant. Normally, none of the Rh-positive or negative people have anti-D antibodies, but when a mother (Rh-negative) gets exposed to fetal D-antigen, she will begin to produce antibodies against the fetal D-antigen, which later will cause hemagglutination and haemolysis and is referred to as Rh incompatibility [8,9]. Kell antigen is the third most important antigen system that causes serious haemolytic transfusion reactions HTR and HDFN after the previous two systems (ABO and Rh), and a total of 25 Kell antigens have been identified [10].
The majority of alloimmunizations and subsequent haemolytic transfusion responses are prevented by red blood cell (RBC) compatibility in the ABO, Rh, and Kell systems; these reactions have a frequency of 1:4000-12000 blood transfusions [11].
The RhD blood group antigen in the Rh blood group system is routinely typed alongside ABO for patients and blood donors in many countries, highlighting the importance of preventing RhD immunization by providing RhD-compatible units or appropriate antenatal care [12].
RBC serology tests are mostly used as a common macroscopic screen for the detection of the presence of alloantibodies, either by direct antiglobulin testing [13] or indirect antiglobulin testing [14]. But if the phenotypic tests are not sufficient for anti-D antibody identification, blood group gene sequencing offers the advantage of identifying feto-maternal blood group incompatibilities from the DNA sequence [15,16].
This study aimed to design a geographic data profile for hemolytic disease cases in Erbil city of Iraq, which includes Rh-D negative mothers who have been pregnant with Rh-D positive babies, as well as to determine the frequency of anti-D antibodies phenotypically.
Methods![]()
In this study, 1028 blood samples were collected from 514 parents (mothers with Rh-negative and fathers with Rh-positive) from both private and government hospitals in Erbil, Iraq, from April 2022 to April 2023. On the other hand, some histories have been taken from parents (abortion, delivery, and blood transfusion times), through verbal interview. Next, the ABO group test has been done by the tube method using anti-A, anti-B, and anti-D blend (IgG + IgM) sera reagents (Biorex, UK). Then the Du test was performed for mothers by mixing 100 µl of anti-D sera with 50 µl of 5% suspension of RBC, incubating for 15–30 min at 37 °C, and then washing the RBC four times with normal saline. The RBC was then examined for agglutination by adding 100 µl of Anti-Human Globulin (AHG) (Biorex, UK) along with centrifugation at 2000 rpm.
Antibody screening was applied for all the mother samples by mixing 100 µl of patient serum, 50 µl of appropriate screening cells, and 100 µl of enhancement reagent (Bovine Albumin, Biorex, UK) into each tube, then incubation at 37 °C for 15 to 30 min and centrifugation in order to check agglutination in this phase, then washing 4 times and adding 100 µl of AHG in the last phase with centrifugation in order to check the agglutination (macroscopically and microscopically). In the end, all negative tests were confirmed by applying check cells to those samples.
Antibody identification was applied to all positive samples in the antibody screening step to detect anti-D antibodies by using the same procedure, but with a specific antibody detection panel cell (Ortho, UK). Then, titration was applied to all positive anti-D samples. Eventually, all statistical analyses were carried out using SPSS Software, version 20 (SPSS Inc., Chicago, IL, USA).
Results![]()
In this study, 1028 blood samples were taken from the parents, then further divided into 5 different age-based groups according to the mother's ages. The groups have been categorized as (20-25; 26-30; 31-35; 36-40; and over 40). Among all groups, the highest number was 191 (37%) in the (31-35) age category, followed by 165 (32%), 112 (22%), 35 (7%) and 11 (2%) for the (26-30, 36-40, 20-25, and over 40) age groups, respectively.
After taking blood samples from parents and categorizing them into various groups, an ABO typing test was done for all the samples (Father and Mother), as illustrated in Table 1. As a result, in the first age group, the most common blood group (BG) among Rh-negative mothers was O (37.1%), and the least common BG was 2.9% for AB. In the second age group, the most common BG was Group O, which was 35.8%, and the least common one was 4.2% for the AB group. In the third age group, the most common BG among mothers was Group O, which was 42.4%, and the least common one was the AB group, which was 3.7%. In the fourth age group, the most common BG was Group O, which was 40.2%; meanwhile, there were no mothers with BG AB type. Finally, in the last age group, the most common BG was Group O (81.8%), followed by Group B (18.2%), while no other blood groups were detected. Overall, 40.3% of all the mothers’ Blood groups were O.
On the other hand, in the first age group, the most common BG among Rh-positive fathers was Group A, which was 48.6%, and the least common was the AB group, with a percentage of 2.9. In the second age group, the most common BG was Group B, which was 38.2%, and the least common was the AB group, with a percentage of 0.6. In the third age group, the most common BG was Group A (42.9%), and the least common was the AB group (1%). In the fourth age group, the most common BG was Group A, which was 52.7%, and the least common was the AB group, with a percentage of 0.9. Finally, in the last age group, the most common BG was Group A, which was 45.5%, and the least common was the O group, with a percentage of 18.2, and there was no case of an AB blood group. Overall, 43.6% of all the fathers' blood groups were A.
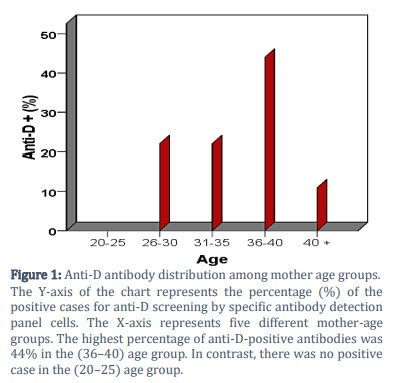
Out of 514 tested mothers, samples that had been screened for antibodies, especially anti-D antibodies, it was determined that only nine of the mothers (1.7%) were positive for anti-D antibodies. Figure 1 shows the percentage of all the positive cases and their distribution among different age groups. As a result, the highest percentage of anti-D-positive antibodies was 44% in the (36-40) age group. In contrast, there was no positive case in the (20–25) age group.
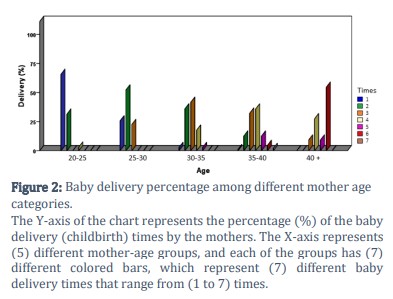
In regards to delivery times, the majority of mothers (65.7%) in the first age group gave birth to a baby one time, in the second group (52.1%) of them gave birth to a baby two times, in the third group (41.5%) of the mothers gave birth to a baby three times, in the fourth group (35.7%) of the mothers gave birth to a baby four times, and in the last group (54.5%) gave birth to a baby six times. The delivery times are illustrated in Figure 2.
On the other hand, in regard to abortion percentage, most of the mothers (54.6 %) in the fifth group (over 41) have experienced abortion in their age group, followed by 49.1% of the fourth group and 40 %, 33 %, and 22.8 % for the third, second, and first groups, respectively. The abortion percentage among age groups is illustrated in Figure 3.
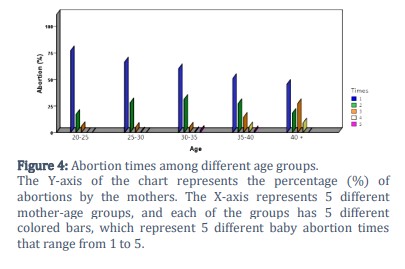
In regard to abortion times, as shown in Figure 4, most of the mothers experienced one-time abortion in their lives, followed by two-time abortions.
Figures & Tables
ABO and Rh typing was done by the traditional tube method using monoclonal antisera, which is similar to the Al Joudi (2000) [17] study in Iraq and the Shahverdi (2017) [18] study in Iran, while some other studies appear to use other techniques. One such study was the Karim (2015) [19] study in Southern Pakistan, in which the ID card Gel technique was used for ABO and Rh typing, then the Du testing was applied for the detection of weak D in all samples.
Antibody screening and identification were done in this study using the indirect Coombs test through the tube method, similar to Al Joudi (2000) [17], while the study of Karim (2015) [19] performed these tests using only Gel cards. On the other hand, the Iranian study of Shahverdi (2017) [18] recommended both methods as a confirmation.
Blood group O was the most predominant among all 514 mother samples in this study, which was 207 (40.3%) of all the cases, followed by 150 (29.2%), 142 (27.6%), and 15 (2.9%) for the A, B, and AB groups, respectively. Unlike other studies, such as Shahverdi (2018) [18] in Iran, in which Group A is most common among all alloimmunized women, and in the study of Karim (2015) [19], blood group B is predominant.
Anti-D antibodies were detected in only nine (1.7%) out of 514 Rh-negative mothers, nearly 44% of them in the age group of (36-40), in which approximately half of them got pregnant more than four times, and faced abortion at least once in their lives. This study is quite similar to the previous study in Iraq, in which the percentage of Anti-D antibody positive cases was (1.7 %). In addition, an Iranian study by Karim (2015) [19] had 2.9 % of positive cases, and the Dajak (2011) [20] study in Croatia with a percentage of (1.3). In contrast to previous mentioned studies, in a study by Shahverdi (2018) [18] the percentage was significantly higher, in which out of 1035 D-negative pregnant women, 125 (12%) cases were positive.
In regard to the effect of the anti-D antibody on the abortion rate and HDFN, the rate of abortion shows a positive correlation with the increasing age and number of pregnancies. The high rate of abortion and anti-D isolation was detected in the fourth and fifth age groups (36-40 and over 40 mothers), despite taking samples randomly (without the concern of trimesters), as illustrated in the Figures 1 and 3. This consequence effect is similar to Al Joudi (2000) [17], Hundrić-Haspl (1997) [21], Dajak (2011) [20] and Karim (2015) [19] studies.
Anti-D detection in pregnant women with Rh-negative blood group is the primary vital test that has to be done for these mothers in all three trimesters; however, some studies, such as Karim (2015) [19] recommend that Rh-positive women, alongside Rh-negative women, have to be checked for anti-D and non-anti-D alloantibodies. In addition, the study by Dajak (2011) [20] stated that there are severe cases of HDFN in women whose mothers were Rh-positive.
Limitations of the Study
This study has certain limitations. Information on obstetric and transfusion histories such as abortions, deliveries, and blood transfusions was collected through verbal interviews, which may introduce recall bias and affect the accuracy of associations between abortion history, parity, and anti-D positivity. Moreover, the cross-sectional design limits causal inference, and the lack of trimester-based stratification or longitudinal antibody data may influence result interpretation. Future research should use verified medical records and multicenter longitudinal sampling to minimize bias and improve generalizability.
Author Contributions
Study conception, design & data collection: Abbas Bahram YOUNUS.
Analysis & interpretation of results: all authors.
Draft manuscript preparation: Bestoon SHEKHANY and Mohammed O. Abdullah.
Research supervision: Faruk SUZERGOZ.
No conflicts of interest are disclosed by the authors.![]()
References
- Myle AK, Al-Khattabi GH. Hemolytic Disease of the Newborn: A Review of Current Trends and Prospects. Pediatric Health, Medicine and Therapeutics, (2021); 12(2021): 491-498.
- Routray SS, Behera R, Mallick B, Acharya D, Sahoo JP, et al. The Spectrum of Hemolytic Disease of the Newborn: Evaluating the Etiology of Unconjugated Hyperbilirubinemia Among Neonates Pertinent to Immunohematological Workup. Cureus, (2021); 13(8): e16940.
- Pegoraro V, Urbinati D, Visser GHA, Di Renzo GC, Zipursky A, et al. Hemolytic disease of the fetus and newborn due to Rh(D) incompatibility: A preventable disease that still produces significant morbidity and mortality in children. PLoS ONE, (2020); 15(7): e0235807.
- De Haas M, Thurik FF, Koelewijn JM, Van der Schoot CE. Haemolytic disease of the fetus and newborn. Vox Sang, (2015); 109(2): 99-113.
- Daniels G (2001) Blood group antibodies in haemolytic disease of the fetus and newborn. In: Hadley A, Soothill P, editors. Alloimmune Disorders of Pregnancy: Anaemia, Thrombocytopenia and Neutropenia in the Fetus and Newborn. Cambridge: Cambridge University Press. pp. 21-40.
- Cowan H. The discovery of human blood groups: Karl Otto Landsteiner. British Journal of Cardiac Nursing, (2017); 12(6): 290-292.
- Westhoff CM. The Rh blood group system in review: a new face for the next decade. Transfusion, (2004); 44(11): 1663-1673.
- Akkök Ç A, Seghatchian J. Immunohematologic issues in ABO-incompatible allogeneic hematopoietic stem cell transplantation. Transfus Apher Science, (2018); 57(6): 812-815.
- Shahata W, Khalil H, Abass A-E, Adam I, Hussien S. Blood group and Rhesus antigens among Blood donors attending the Central Blood Bank, Sudan. Sudan Journal of Medical Sciences, (2013); 7(4): 245-248.
- Mitra R, Mishra N, Rath GP. Blood groups systems. Indian Journal of Anaesthesia, (2014); 58(5): 524-528.
- Klein HG, Anstee DJ (2005) Blood donors and the withdrawal of blood. Mollison’s Blood Transfusion in Clinical Medicine. Oxford UK: Blackwell Publishing. pp. 1-18.
- Malomgré W, Neumeister B. Recent and future trends in blood group typing. Analytical and Bioanalytical Chemistry, (2009); 393(5): 1443-1451.
- Dinesh D. Review of positive direct antiglobulin tests found on cord blood sampling. Journal of Paediatrics and Child Health, (2005); 41(9-10): 504-507.
- Hadley A, Soothill P. Alloimmune Disorders of Pregnancy: Anaemia, Thrombocytopenia and Neutropenia in the Fetus and Newborn. 2002; Cambridge University Press.
- McBean R, Liew YW, Wilson B, Kupatawintu P, Emthip M, et al. Genotyping confirms inheritance of the rare At(a-) type in a case of haemolytic disease of the newborn. The Journal of Pathology: Clinical Research, (2016); 2(1): 53-55.
- McBean RS, Hyland CA, Hendry JL, Shabani-Rad MT, Flower RL. SARA: A "new" low-frequency MNS antigen (MNS47) provides further evidence of the extreme diversity of the MNS blood group system. Transfusion, (2015); 55(6 Pt 2): 1451-1456.
- Al-Joudi FS, Ahmed al-Salih SA. Incidence of Rhesus isoimmunization in Rhesus-negative mothers in Ramadi, Iraq, in the mid-1990s. East Mediterr Health J, (2000); 6(5-6): 1122-1125.
- Shahverdi E, Moghaddam M, Gorzin F. Maternal red blood cell alloantibodies identified in blood samples obtained from Iranian pregnant women: the first population study in Iran. Transfusion, (2017); 57(1): 97-101.
- Karim F, Moiz B, Kamran N. Risk of maternal alloimmunization in Southern Pakistan – a study in a cohort of 1000 pregnant women. Transfusion and Apheresis Science, (2015); 52(1): 99-102.
- Dajak S, Stefanović V, Capkun V. Severe hemolytic disease of fetus and newborn caused by red blood cell antibodies undetected at first-trimester screening (CME). Transfusion, (2011); 51(7): 1380-1388.
- Hundrić-Haspl Z, Juraković-Loncar N, Grgicević D. The effect of Rh-D immunoprophylaxis with hyperimmune anti-D-immunoglobulin on the occurrence of RhD immunization in pregnancy. Lijecnicki vjesnik, (1997); 119(7): 189-193.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0

