

Full Length Research Article
Study of bone disorders after thyroidectomy in women
Isam Nghaimesh Taeb1, Raid M. H. AL-Salih2*
Adv. life sci., vol. 12, no. 3, pp. 577-582, August 2025
*- Corresponding Author: Raid M. H. AL-Salih (Email: raidstry@gmail.com)
Authors' Affiliations
2. Department of Chemistry, College of Science, University of Thi-Qar, Thi-Qar, 64001 – Iraq
[Date Received: 31/12/2024; Date Revised: 18/02/2025; Available Online: 31/10/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: A reduction in IGF-1, thyroid hormones, as well as calcium, PTH, vitamin D, human bone-specific alkaline phosphatase (PAP), and Alkaline Phosphatase (ALP) are prominent complications that can arise after total thyroidectomy. These complications can exhibit a wide range of severity, from asymptomatic cases to acute life-threatening conditions.
Methods: The study included three patient groups (n = 30 each) at different time intervals post-thyroidectomy and one healthy control group (n = 30). Omitted from the study were patients with cancer, diabetes, hypertension, and pregnant women. The scope of the study was confined to patients who had undergone surgical removal of the thyroid gland due to benign tumors or other medical reasons.
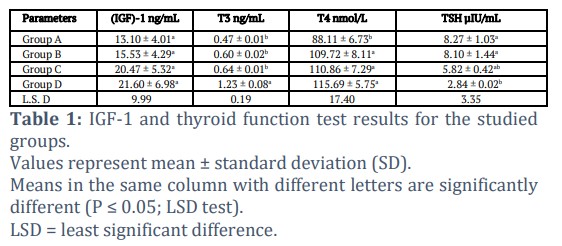
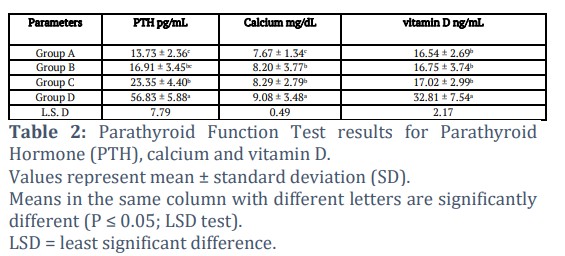
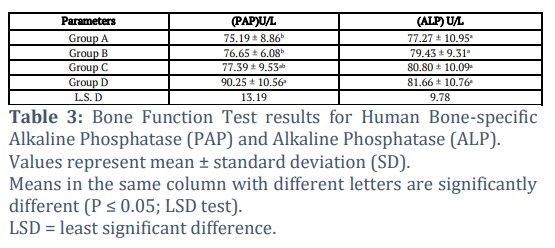
Results: The results demonstrated significant differences among the four groups in IGF-1, thyroid hormones, calcium, PTH, vitamin D, and bone-specific alkaline phosphatase (PAP and ALP). In comparison with the control group, the patient groups exhibited progressively higher levels of these parameters, with the highest values observed in Group D, indicating gradual recovery and metabolic adaptation following thyroidectomy.
Conclusion: The findings garnered from the conducted research indicate a progressive increase in thyroid hormones and parathyroid activity following total thyroidectomy. This trend, accompanied by elevated calcium, vitamin D, and bone-specific markers (PAP and ALP), suggests metabolic recovery and compensatory adaptation of endocrine and skeletal systems rather than functional decline. These results collectively highlight the body’s capacity for hormonal equilibrium and bone remodelling during the postoperative period.
Keywords: Bone disease, IGF-1, Hypoparathyroidism, Thyroidectomy
Introduction![]()
A bone condition referred to as osteoporosis includes loss of bone density, reduced bone quality, and weakening of bone tissue architecture. This progressive skeletal condition is prevalent and contributes to brittle bones as well as increased vulnerability to fractures. The incidence of osteoporosis is higher in females who are above 50 years of age than in males in their respective age groups, mainly due to estrogen deficiency and subsequent disruption of bone remodeling. In Taiwan, evidence shows more than 30% of women over age 50 are impacted by osteoporosis. Also in the USA, health care costs as well as morbidity of fractures associated with osteoporosis are higher than those associated with breast cancer, stroke, or heart attack [1-3].
Total thyroidectomy, which is the entire removal of the thyroid gland, is used in treating thyroid enlargement or thyroid cancers. Various studies sought to understand how thyroidectomy affects bone mineral density (BMD) and how calcium is processed by the body. The studies come forth with various hypotheses for how bone mass can be lost and how osteoporosis may arise after thyroid removal. These hypotheses include hormonal imbalances in thyroid hormones, including calcitonin deficiency, and loss of thyrotropin's defensive action through thyroxine treatment [4-6].
Additionally, various studies also demonstrated that there is an association between osteoporosis with thyrotropin-suppressive medication use post-surgery, particularly in women over menopause. Thyroid hormones have the potential to stimulate bone cells either through an indirect mechanism whereby the secretion of growth hormone (GH) and insulin-like growth factor-1 (IGF-1) is increased or through a direct mode of action that involves the influence of specific nuclear receptors on target genes. The existence of thyroid hormone receptors (TRs) is established in osteoblast-like cells and cell lines derived from humans and rodents, and recently in vitro osteoclasts derived from an osteoclastoma. However, there is no report on their presence in situ in human bone [7-9].
Insulin-like growth factor-1 (IGF-1) plays a crucial role in the development of the skeletal system during the early stages of life. From the moment of birth, both the serum IGF-1 levels and the bone mass of an individual increase simultaneously and reach their peak during puberty. The research demonstrates that abnormal skeletal development, such as dwarfism, gigantism, and acromegaly, can be caused by either low or high levels of IGF-1. Additionally, the insulin-like growth factor 1 signaling pathway is also indispensable in skeletal development. Interestingly, selective inactivation of Igf1 in liver cells only caused mild impairments in the widthwise growth of bones, with their lengthwise growth and amount of trabecular bone being unaffected [10,11]. The present investigation seeks to assess the reduced levels of IGF-1, thyroid hormones, calcium, PTH, vitamin D, human bone-specific alkaline phosphatase (PAP), and Alkaline Phosphatase (ALP) in patients who have undergone total thyroidectomy.
Methods![]()
This study was conducted at Nasiriyah Teaching Hospital in Thi-Qar, the Endocrine Glands Center in Thi-Qar governorate, during the period between 7/8/2022 to 1/4/2023. The study included 120 female subjects who were divided into four groups (n = 30 each). This comprised one healthy control group (Group A) and three patient groups (Groups B, C, and D) assessed at different postoperative intervals following total thyroidectomy.
There were 120 female subjects, control and patients with euthyroid goiter aged 25-45 years, who were included in this study. They were divided into four groups as follows:
Group A (control)
It Included 30 healthy subjects aged 25-45.
Group B (patients, after thyroidectomy)
Included patients from one day to one month after thyroidectomy.
Group C (patients, after thyroidectomy)
Included patients from one month and one day to one year after thyroidectomy.
Group D (patients, after thyroidectomy)
Included patients from one year, one day and more after thyroidectomy. Medical tests were performed on the blood of patients, including IGF-1, thyroid hormones, as well as calcium, PTH, vitamin D, human bone-specific alkaline phosphatase (PAP), and Alkaline Phosphatase (ALP), using the ELISA device.
Hormone Replacement Therapy
All post-thyroidectomy patients (Groups B, C, and D) were maintained on standard levothyroxine (T4) hormone replacement therapy according to hospital protocol. The initial dosage was prescribed by the attending endocrinologist and titrated over time based on serial thyroid function tests (T3, T4, TSH) to achieve euthyroid levels. The progressive increase in thyroid hormones and the corresponding decrease in TSH observed across postoperative groups reflect successful dose stabilization and endocrine adaptation following thyroidectomy.
Ethical approval
The samples were taken from Al-Nasiriyah Teaching Hospital after obtaining official approvals from the Dhi Qar Health Department and after studying the research project no.2022/204. An approval was obtained to complete the research in the institutions of the Dhi Qar Health Department, according to decision No. Dhi Qar/2022204 procured on 7/8/2022.
Results![]()
The findings of the inquiry, as demonstrated in Tables 1–3, revealed significant alterations in insulin-like growth factor, thyroid and parathyroid functions, and bone characteristics among the patient groups. Specifically, compared with the control group, post-thyroidectomy patients (Groups B–D) exhibited progressively higher levels of IGF-1, T3, T4, PTH, calcium, vitamin D, and bone formation markers (PAP and ALP), while TSH values decreased over time. The outcomes of the three patient groups also differed significantly from one another, and these trends are comprehensively depicted in the tables.
Figures & Tables
Thyroid hormones act by means of nuclear receptors in osteoblasts to induce osteoclastic bone resorption. Thus, thyroid disorders are among the most frequent causes of secondary osteoporosis. Previous studies demonstrated that hypothyroid patients exhibit increases in both osteoclastic and osteoblastic activities, with a prevailing emphasis on bone resorption. This results in a decline in bone mineral density (BMD), which can be rectified by the normalization of thyroid function [12-14]. The latter is associated with an increase in lumbar spine BMD, preceded by a significant attenuation in augmented bone turnover. However, there is a discrepancy in the results of studies that aim to determine whether antithyroid drugs (ATD) can completely normalize bone. There exist numerous patients who manifest bone pain and deformity due to issues with thyroid hormones. In recent years, an awareness has arisen about the central function of thyroid hormone in bone development and bone mass maintenance. Changes in thyroid hormone are involved in growth abnormalities, bone loss, and increased fracture risk. Thyroid hormones are essential for skeletal development and play an essential physiological role in adult bone structure and strength [15-17]. Although thyroid disease is a recognized risk factor for bone disease, thyroid hormones’ role in osteoporosis pathogenesis and their relationship with factors in fracture risk have been underappreciated, with the pathogenetic mechanism unclear. Hyperthyroidism features TSH suppression with increased T3 and T4 levels, predominantly due to Graves’ disease. This condition occurs following surgery, as outlined by The British Association of Endocrine and Thyroid Surgeons (BAETS) [18-20].
Notably, hypothyroidism is the most common long-term consequence after total thyroidectomy. The findings by Tsai et al. (2019) align with the current study, as total thyroidectomy plays a crucial and growing part in thyroid disease management [21-23]. In many hospitals, it is responsible for nearly half of all thyroid operations. Total thyroidectomy suitability in managing non-cancerous tumors and growths is, however, still controversial. It is being increasingly realized that total thyroidectomy is suitable for multinodular goiter (MNG) patients, especially with extensive nodular disease involving both lobes. If one of the lobes is in relatively good condition, then total excision of the gland is not necessary. It is being realized that in those with unilateral disease, about 10 percent of such cases would have recurrence in the long term. However, it is noteworthy that only half of these individuals will require surgical intervention [5,22,24-27]. The administration of a preliminary Hemithyroidectomy is potentially satisfactory for such patients. The primary objection to total thyroidectomy is its heightened susceptibility to associated complications. The occurrence of permanent recurrent laryngeal nerve palsy in recent studies about total thyroidectomy is 0.3% to 1.7% and for permanent hypoparathyroidism, it is 0.7% to 3%. The practice of capsular dissection, offering minimal harm to parathyroid glands but with careful preservation of recurrent nerves, has helped to reduce intraoperative morbidity in comparison with figures reported in earlier studies. Nevertheless, maintaining parathyroid glands on an intact vascular pedicle can remain technically demanding in the case of large goiters [27-29]. Among the numerous endocrinological reasons for secondary osteoporosis, such as hypogonadism, thyroid diseases, Cushing’s syndrome and hyperparathyroidism, excess or lack of thyrotropin (thyroid-stimulating hormone) and other thyroid hormones are potentially harmful to bone status. While endogenous hyperthyroidism is associated with an increased risk of osteoporosis due to augmented osteoclastic resorption and reduced bone formation, the effect of suppressive thyroxine therapy on osteoporosis is still uncertain. There exists a correlation between thyroid hormones and bone properties [30-32]. Both thyroxine (T4) and triiodothyronine (T3) thyroid hormones affect metabolic processes in all parts of the body and are necessary for normal bone turnover. Over the last few decades, thyroid hormones’ role in bone formation and maintaining bone mass has come to be appreciated. Changes in thyroid hormones can cause bone loss, growth disorders, as well as an increased risk of fracture [33,34].
Thyroid hormones are important in skeletal development and are essential for maintaining adult bone structure and strength. Thyroid dysfunction is recognized as an independent risk factor for bone disease, but thyroid hormones' role in osteoporosis pathogenesis and factors affecting fracture risk are underappreciated, with undefined pathways. There are reports of higher bone mineral density (BMD) in postsurgical permanent hypoparathyroidism patients. Our previous report showed that patients who experienced transient hypoparathyroidism postoperatively were in a subclinical hypoparathyroid (HP) state even after 5 years of surgery [35-38]. More research is now supporting a possible relationship between thyroid gland function, bone turnover, and fracture likelihood. The relationship, however, involving measures of thyroid responsiveness with osteoporosis and bone fractures, is still ambiguous. The goal of this research, then, was to identify relationships between thyroid sensitivity and bone mineral density (BMD), as well as fractures, in patients with normal thyroid function. [13].
Specific ablation of Igf1 from osteoblasts (OBs) or chondrocytes produced severe skeletal abnormalities, suggesting an even more important role for IGF-1 produced locally from bone and cartilage in skeletal development. Remarkably, an enhancement in bone mineral density (BMD) and serum IGF-1 levels was observed in therapies that reduced serum IGF-1 levels. This is probably due to the fact that signaling of IGF-1 activates osteoclast and osteoblast maturation, enhances the synthesis of type I collagen, and lowers the production of collagenase, which is essential for ongoing remodeling and sustaining of bone tissue [39,40]. Consequently, a decrease in IGF-1 levels may precipitate diminished mass of bone, bone disorders, and an elevated bone fracture risk. In addition, the activation of satellite cells and the formation of muscle protein is credited to the involvement of IGF-1; thus, reduced IGF-1 levels are related to sarcopenia (muscle mass and muscle power loss) and impaired physical function in patients, potentially increasing the risk of fractures and falls [41]. Overall, IGF-1 is essentially pivotal to the musculoskeletal system, and a decrease in its levels may lead to musculoskeletal disorders as well as an increased risk of fractures. Consequently, careful attention to fracture risk is warranted, especially in those presenting with low serum IGF-1 levels. An association was identified between osteoporosis, total thyroidectomy, and insulin-like growth factor, as it revealed a reduction in insulin-like growth factor, mineral density, vitamin D, and bone mass. Thyroid hormones are known to exert an influence on the modulation of insulin-like growth factor type 1 (IGF-1) and insulin-like growth factor-binding protein-3 (IGFBP-3) expression. It is well established that both IGF-1 and IGFBPs are closely associated with the physiological processes and developmental aspects of the thyroid gland [42,43].
Recent clinical and pre-clinical investigations suggested that PTH can augment the bony density of the jaw, while also enhancing soft tissue healing and bone filling subsequent to tooth extraction. Moreover, in vivo studies showed that PTH directly triggers survival signaling in osteoblasts, with the postponement of osteoblast apoptosis being a significant contributor to the increased osteoblast number. Despite having high bone mineral density (BMD), individuals diagnosed with hypoparathyroidism are susceptible to vertebral fractures (VFs) [26,31,44]. Hypoparathyroidism, a postoperative complication of total thyroidectomy, is observed with a frequency ranging from 7% to 51%. This wide range in incidence is attributed to variations in the technical proficiency of the surgical operator and the procedural complexity and is further exacerbated by the absence of a universal nomenclature for the identification and definition of this complication. A multicenter analysis conducted in our nation determined the prevalence of hypoparathyroidism to be 22.9% at 3 to 6 months post-surgery, 16.7% at 12 months post-surgery, and 14.5% at the final outpatient assessment [45-48].
Vitamin D plays an important role in the growth and development of a healthy, strong skeletal system. Additionally, Vitamin D is needed for processing calcium and phosphorus, providing an adequate supply of these minerals for mineralization of bones. The mean serum 25(OH) D levels in both thyroid patients and controls, however, were below the recommended levels [49,50]. Furthermore, patients with preoperative Vitamin D levels below 20 ng/mL had a lower incidence of transient hypoparathyroidism. It is worth noting that the active Vitamin D metabolite, 1, 25(OH) 2D, plays a key role in opening calcium channels in the gut and stimulating the formation of calcium binding proteins in intestinal cells, ultimately leading to increased absorption of calcium and phosphate from the gut. In this manner, optimal conditions for bone mineralization are established [51-53].
Circulating levels of alkaline phosphatase (ALP) and their variants offer insight into processes of bone metabolism. Through systemically increasing the ratio of inorganic phosphate to pyrophosphate, ALP encourages mineralization while also decreasing extracellular levels of pyrophosphate, a compound that restricts mineral development. ALP activity reduction is linked to reduced bone remodeling. The bone-specific isoenzyme (B-ALP) is implicated in the calcification of bone and is used as a marker of bone remodeling based on osteoblast activity. Higher levels of ALP are utilized in the diagnosis of rickets in children, although they are also linked with bone formation. Alkaline phosphatase (ALP) proves to be a valuable tool in distinguishing rickets from other conditions that share similar clinical and laboratory characteristics [54-56]. Hypothyroid patients, for instance, typically display higher than normal bone density, frequently accompanied by normal or low ALP values [55]. The wide postoperative range defined for Group B (1 day – 1 month) may have introduced variability in hormonal and biochemical recovery patterns, as it combines both acute and stabilized postoperative stages. Future research should consider narrower postoperative intervals for improved group homogeneity.
Acknowledgement
Pathological Analyses Department, College of Science at University of Sumer and Department of Chemistry, College of Science at University of Thi-Qar is acknowledged by the authors for providing the facilities needed to conduct the study.
Author Contributions
The authors shared the progress, material preparation, and collection of the samples. Every author has read and approved the finished manuscript.
No conflicts of interest are disclosed by the authors.![]()
References
- Foessl I, Dimai HP, Obermayer-Pietsch B. Long-term and sequential treatment for osteoporosis. Nature Reviews Endocrinology, (2023); 19(9): 520-533.
- Gielen E, Dupont J, Dejaeger M, Laurent MR. Sarcopenia, osteoporosis and frailty. Metabolism, (2023); 145(2023): 155638.
- Bartl R (2023) Definition and Pathogenesis of Osteoporosis. Osteoporosis in Clinical Practice: Springer. pp. 19-28.
- Zhou S, Wang D, Liu X, Li Z, Wang Y. Transoral thyroidectomy vestibular approach vs. conventional open thyroidectomy: a systematic review and meta-analysis. Endocrine, (2023); 81(1): 36-46.
- Kim KH, Ji YB, Song CM, Kim E, Kim KN, et al. Learning curve of transoral robotic thyroidectomy. Surgical Endoscopy, (2023); 37(1): 535-543.
- Delitala AP, Scuteri A, Doria C. Thyroid hormone diseases and osteoporosis. Journal of clinical medicine, (2020); 9(4): 1034.
- Wang S, Wang Y, Zhu L, He L, Lv M, et al. Effects of TSH suppressive therapy on bone mineral density (BMD) and bone turnover markers (BTMs) in patients with differentiated thyroid cancer in Northeast China: a prospective controlled cohort study. Endocrine, (2023); 79(1): 113-124.
- Jia H, Qu W, Cai X, Li M, Qian Y, et al. Assessment for bone health in patients with differentiated thyroid carcinoma after postoperative TSH suppression therapy: A new Fracture Risk Assessment Algorithm. Frontiers in Endocrinology, (2023); 14(2023): 1286947.
- Yavuz DG, Dincer YC, Hekimsoy Z, Aydin K, Gokkaya N, et al. Bone mineral density and fracture status of differentiated thyroid cancer patients under TSH suppression treatment; 2023. Bioscientifica.
- Bian A, Ma Y, Zhou X, Guo Y, Wang W, et al. Association between sarcopenia and levels of growth hormone and insulin-like growth factor-1 in the elderly. BMC musculoskeletal disorders, (2020); 21(2020): 1-9.
- Park J, Yan G, Kwon KC, Liu M, Gonnella PA, et al. Oral delivery of novel human IGF-1 bioencapsulated in lettuce cells promotes musculoskeletal cell proliferation, differentiation and diabetic fracture healing. Biomaterials, 2020; 233(2020): 119591.
- Bassett JD, Williams GR. Role of thyroid hormones in skeletal development and bone maintenance. Endocrine reviews, (2016); 37(2): 135-187.
- Liu C, Hua L, Liu K, Xin Z. Impaired sensitivity to thyroid hormone correlates to osteoporosis and fractures in euthyroid individuals. Journal of Endocrinological Investigation, (2023); 46(10): 2017-2029.
- Iwobi N, Sparks NR. Endocrine Disruptor-Induced Bone Damage Due to Hormone Dysregulation: A Review. International Journal of Molecular Sciences, (2023); 24(9): 8263.
- Mudri D, Kizivat T, Mihaljević I, Bilić Ćurčić I. Wnt Inhibitors and Bone Mineral Density in Patients with Graves’ Disease Treated with Antithyroid Drugs: A Preliminary Prospective Study. Metabolites, (2022); 12(8): 711.
- Mudri D, Bilić Ćurčić I, Meštrović L, Mihaljević I, Kizivat T. Hyperthyroidism and Wnt Signaling Pathway: Influence on Bone Remodeling. Metabolites, (2023); 13(2): 241.
- Marino L, Kim A, Ni B, Celi FS. Thyroid hormone action and liver disease, a complex interplay. Hepatology, (2025); 81(2): 651-669.
- Ahmed M, Mital D, Abubaker NE, Panourgia M, Owles H, et al. Bone health in people living with HIV/AIDS: an update of where we are and potential future strategies. Microorganisms, (2023); 11(3): 789.
- Wang LT, Chen LR, Chen KH. Hormone-Related and Drug-Induced Osteoporosis: A Cellular and Molecular Overview. International Journal of Molecular Sciences, (2023); 24(6): 5814.
- Son O. Comparison of the effect of Dapagliflozin and Pioglitazone on the risk of osteoporosis in postmenopausal women with Type-2 diabetes. Pakistan Journal of Medical Sciences, (2023); 39(5): 1238.
- Tsai SH, Chien SC, Nguyen PA, Chien PH, Ma HP, et al. Incidences of hypothyroidism associated with surgical procedures for thyroid disorders: a nationwide population-based study. Frontiers in Pharmacology, (2019); 10(2019): 1378.
- Díez JJ, Iglesias P. Prevalence of thyroid dysfunction and its relationship to income level and employment status: a nationwide population-based study in Spain. Hormones, (2023); 22(2): 243-252.
- Digkas E, Smith DR, Wennstig AK, Matikas A, Tegnelius E, et al. Incidence and risk factors of hypothyroidism after treatment for early breast cancer: a population-based cohort study. Breast Cancer Research and Treatment, (2024); 204(1): 79-87.
- Hsiao V, Light TJ, Adil AA, Tao M, Chiu AS, et al. Complication rates of total thyroidectomy vs hemithyroidectomy for treatment of papillary thyroid micro carcinoma: a systematic review and meta-analysis. JAMA Otolaryngology–Head & Neck Surgery, (2022); 148(6): 531-539.
- Leboulleux S, Bournaud C, Chougnet CN, Zerdoud S, Al Ghuzlan A, et al. Thyroidectomy without radioiodine in patients with low-risk thyroid cancer. New England Journal of Medicine, (2022); 386(10): 923-932.
- Frey S, Van Den Heede K, Triponez F, Bizard JP, Godiris-Petit G, et al. Prevention of hypocalcemia and hypoparathyroidism after total thyroidectomy. Recommendations of the Francophone Association of Endocrine Surgery (AFCE) with the French Society of Endocrinology (SFE) and the French Society of Nuclear Medicine (SFMN). Journal of Visceral Surgery, (2023); 160(3): S95-S109.
- Sakthivel P, Thakar A, Prashanth A, Bhalla A, Kakkar A, et al. FHNO 2019 Abstract Edition. Journal of Head & Neck Physicians and Surgeons, (2019); 7(Suppl 1): S1-S130.
- Barile A, Quarchioni S, Bruno F, Ierardi AM, Arrigoni F, et al. Interventional radiology of the thyroid gland: critical review and state of the art. Gland surgery, (2018); 7(2): 132.
- Liddy W, Bonilla-Velez J, Triponez F, Kamani D, Randolph G (2021) Principles in thyroid surgery. Surgery of the Thyroid and Parathyroid Glands: Elsevier. pp. 272-293. e275.
- Lee D, Ahn MB. A Causality between Thyroid Function and Bone Mineral Density in Childhood: Abnormal Thyrotropin May Be Another Pediatric Predictor of Bone Fragility. Metabolites, (2023); 13(3): 372.
- Jeon S, Lee YS, Oh SR, Jeong J, Lee DH, et al. Recent advances in endocrine organoids for therapeutic application. Advanced Drug Delivery Reviews, (2023); 199(2023): 114959.
- Ebeling PR, Nguyen HH, Aleksova J, Vincent AJ, Wong P, et al. Secondary osteoporosis. Endocrine Reviews, (2022); 43(2): 240-313.
- Mullur R, Liu YY, Brent GA. Thyroid hormone regulation of metabolism. Physiological reviews, (2014); 94(2): 355-382.
- Mondal S, Raja K, Schweizer U, Mugesh G. Chemistry and biology in the biosynthesis and action of thyroid hormones. Angewandte Chemie International Edition, (2016); 55(27): 7606-7630.
- Wu J, Huang H, Yu X. How does Hashimoto’s thyroiditis affect bone metabolism?. Reviews in Endocrine and Metabolic Disorders, (2023); 24(2): 191-205.
- Wang H, Luo Y, Wang H, Li F, Yu F, et al. Mechanistic advances in osteoporosis and anti‐osteoporosis therapies. MedComm, (2023); 4(3): e244.
- Deng Y, Han Y, Gao S, Dong W, Yu Y. The Physiological Functions and Polymorphisms of Type II Deiodinase. Endocrinology and Metabolism, (2023); 38(2): 190-202.
- Zhao Y, Peng X, Wang Q, Zhang Z, Wang L, et al. Crosstalk between the neuroendocrine system and bone homeostasis. Endocrine Reviews, (2024); 45(1): 95-124.
- Hussein NMSE (2023) The role of Insulin Growth Factor axis in stem cell based periodontal regeneration under diabetic conditions. University of Leeds.
- Desai S. The role of mechanical loading, sex and TRAP/ACP5 on bone properties. 2023. Karolinska Institutet (Sweden)
- Kevin M Defining molecular pathways regulating musculoskeletal disorders in COPD and acute exacerbation. RMIT University.
- Zöllner SK, Amatruda JF, Bauer S, Collaud S, de Álava E, et al. Ewing sarcoma—diagnosis, treatment, clinical challenges and future perspectives. Journal of clinical medicine, (2021); 10(8): 1685.
- Clough GP (2021) Does the integration of healthcare and social care help improve the health of senior citizens in the UK? The University of Manchester (United Kingdom).
- Ferraz MP. Bone Grafts in Dental Medicine: An Overview of Autografts, Allografts and Synthetic Materials. Materials, (2023); 16(11): 4117.
- Milyani AA, Al-Agha AE. BLUEPRINT OF PAEDIATRIC ENDOCRINOLOGY. 2023; 1-357. King Abdulaziz University
- Vardhan A, Hutchison A (2022) Calcium, Phosphate, and Renal Osteodystrophy: CKD: Mineral and Bone Disorder. Nolph and Gokal's Textbook of Peritoneal Dialysis: Springer. pp. 537-573.
- Dobrovolska O, Marchenko K, Dobrovolskii O, Dvornyk V, Kuz G, et al. Dental implantology: surgical and prosthetic aspects. 2022. Полтавський державний медичний університет
- Corpas E, Larrad-Jiménez Á, Vinales K, Correa R, Ruiz-Torres A (2021) Physiology and Diseases of the Parathyroid Glands in the Elderly. Endocrinology of Aging: Elsevier. pp. 59-102.
- Fischer V, Haffner-Luntzer M, Amling M, Ignatius A. Calcium and vitamin D in bone fracture healing and post-traumatic bone turnover. European Cells and Materials, (2018); 35(2018): 365-385.
- Pinotti L, Manoni M, Ferrari L, Tretola M, Cazzola R, et al. The contribution of dietary magnesium in farm animals and human nutrition. Nutrients, (2021); 13(2): 509.
- Vilar Tabanera JA, Gómez Ramirez J, Brabyn P, Barranquero AG, Puerta Vicente A, et al. Dynamics of PTH levels in the development of post-operative hypoparathyroidism. Acta Chirurgica Belgica, (2024); 124(2): 99-106.
- Lykke E, Christensen A, Juhl K, Feldt-Rasmussen U, Friberg Hitz M, et al. Effect of near infrared autofluorescence guided total thyroidectomy on postoperative hypoparathyroidism: a randomized clinical trial. European Archives of Oto-Rhino-Laryngology, (2023); 280(5): 2593-2603.
- Naushad A, Sattar S, Salik M, Wajid M, Khalid F, et al. Frequency and Risk Factors of Permanent Hypoparathyroidism After Total Thyroidectomy: An Experience at a Tertiary Care Hospital in Pakistan. Ear, Nose & Throat Journal, (2023); 0(0): 1-6.
- Melot C, Deniziaut G, Menegaux F, Chereau N, et al. Incidental parathyroidectomy during total thyroidectomy and functional parathyroid preservation: a Retrospective Cohort Study. BMC surgery, (2023); 23(1): 269.
- Cannalire G, Pilloni S, Esposito S, Biasucci G, Di Franco A, et al. Alkaline phosphatase in clinical practice in childhood: Focus on rickets. Frontiers in Endocrinology, (2023); 14(2023): 1111445.
- Hanga-Farcaș A, Miere F, Filip GA, Clichici S, Fritea L, et al. Phytochemical Compounds Involved in the Bone Regeneration Process and Their Innovative Administration: A Systematic Review. Plants, (2023); 12(10): 2055.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0

