

Full Length Research Article
Alpha -1- Antitrypsin, Elastase Activity as Markers for Chronic Obstructive Pulmonary Disease Exacerbation
Dhuha Abd-Alkareem Mezaal1*, Raid J. M. Al-Timimi1, Haider Abdulhameed Alqaraghali2
Adv. life sci., vol. 12, no. 3, pp. 605-609, August 2025
*– Corresponding Author: Dhuha Abd-Alkareem Mezaal (Email: Duha_k1988@yahoo.com)
Authors' Affiliations
2. Department of Medicine, College of Medicine- Al-Nahrain University – Iraq
[Date Received: 20/10/2024; Date Revised: 05/01/2025; Available Online: 31/10/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Chronic obstructive pulmonary disease (COPD) is an illness distinguished by obstruction of airflow into the airways during the breathing process. It includes emphysema and chronic bronchitis. The study's objectives are to measure the levels of neutrophil elastase and alpha-1 anti-trypsin in patients with stable and exacerbating COPD and to ascertain whether there is a relationship between the two parameters and exacerbations of the disease.
Methods: A cross-sectional study was done between 40 stable and 40 exacerbation patients aged 30–85 years old, the levels of AAT and NE were measured in both groups by using the ELISA technique.
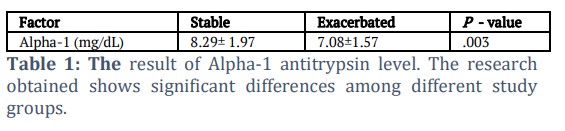
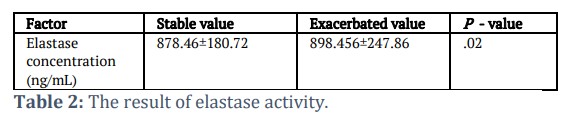
Results: In general, variables affecting the results—such as gender, age, and body mass index—were taken into consideration. The concentration of AAT in the patients was recorded at 8.29 ± 1.97 ng/ml and 7.08 ± 1.57 ng/ml for the stable and exacerbation groups, respectively (p = 0.003). Similarly, the concentration of elastase enzyme activity was recorded at 878.46 ± 180.72 ng/mL and 898.46 ± 247.86 ng/mL for the stable and exacerbation groups, respectively (p = 0.52).
Conclusion: AAT levels are higher in patients in the stable group than in those in the exacerbation groups, and the stable group's elastase concentration is lower than that of the exacerbation group. This discrepancy explains how the disease develops because the enzymes in the stable group control and limit the activity of elastase. In contrast, a breakdown in the exacerbation group led to an increase in elastase levels and lung tissue damage.
Keywords: Alpha-1 antitrypsin, Elastase Activity, Obstructive Pulmonary Disease, ELISA technique
Introduction![]()
Chronic Obstructive Pulmonary Disease (COPD) is a prevalent and curable disease is characterized by increasing tissue damage and airflow limitation. It includes emphysema and chronic bronchitis. It is associated with structural abnormalities in the lungs because of chronic inflammation brought on by long-term exposure to hazardous particles or gases, most commonly cigarette smoke. The symptoms of COPD can progress from being asymptomatic to respiratory failure [1]. COPD is the third most common reason for death [2]. Four levels of severity for COPD exist: I mild, II moderate, severe III, and IV extremely severe. Chronic obstructive pulmonary disease that responds to treatment is usually described as (stable), and in cases of recurrent infections with reduced lung function, it is called (Exacerbation) [3]. Comorbidities like cardiovascular disease, undernutrition, osteoporosis, gastric reflux, clinical depression, and anxiety led to an increase in a patient’s overall severity [4]. Chronic obstructive pulmonary disease is diagnosed using a number of tests and techniques through which the severity and development of the disease are assessed, the main examinations that are used for investigation and follow-up its Bronchodilator reversibility, Blood test, X-Ray or CT scan, Sputum test and Electrocardiogram (ECG or EKG) [5]. Smoking is considered a major risk factor in the development of the disease, but non-smokers can also develop this disease [6]. Other non-tobacco risk factors that lead to developing COPD include genetics and environmental factors, exposure to chemical products, passive smoking, environmental pollution, tuberculosis and chronic asthma [7]. It’s one of the most important proteins in the body. Belonging to the serpin superfamily [8]. AAT is made by hepatocytes and transported through the blood circulation to the lung, where it works to protect the lung tissues from lytic proteins that work to destroy the lung tissues by breaking the elastin fibers that work to preserve the effective shape of the parts of the lung [9]. A reduced amount of AAT in the blood occurs because of a genetic defect that causes little or no protein synthesis.[10]. This disorder suffers from it approximated 3.4 million individuals worldwide [11]. In 1963, Laurell and Eriksson reported the first description of alpha1-antitrypsin deficiency (AATD (, Laurell noted that in five of the 1500 serum protein electrophoresis (SPEP) that were sent for testing through his laboratory in Sweden, the alpha1-protein band was absent [12]. When a bacterial or viral infection affects the respiratory system, the immune system becomes activated, this triggers an immune response and one of the immune cells that is neutrophil will be activated, the neutrophil produces the elastase enzyme, one of the most important immune factors that act to destroy the bacterial or viral and it is the first factor that activates during infection [13]. Alpha-1 antitrypsin plays an important role in controlling elastase action and keeping healthy lung tissue. If the liver does not manufacture and releases enough alpha-1 antitrypsin, the lungs' alveoli will not be sufficiently protected, and emphysema or COPD will develop [14]. Disorders in AAT representation are often of genetic cause and result in an altered representation of the protein industry or function [15]. A significant inflammatory protease is found in the main granules of neutrophils and is involved in immune processes when discharged into the airway of chronically inflamed airway disorders [16, 17]. It is a glycoprotein with 218 amino acids in its polypeptide chain [18]. In general (NE) causes the carboxyl groups on tiny hydrophobic amino acids, such as valine, glycine, and alanine, to cleave; it mainly activates inflammatory processes and attracts leukocytes to the site of infection in the airways to get rid of Gram-negative bacteria [19]. Furthermore, it strongly increases mucus secretion and causes epithelial cells to secrete CXCL8, which could prolong the inflammatory state [20]. Its essential role is the breakdown of fibers of elastin which is a protein that responsible of elasticity to connective tissue. The involvement of NE in the etiology of COPD has been progressively identified in previous studies. This study aims to measure Neutrophil elastase activity and Alpha-1 antitrypsin in patients with COPD and compare stable and exacerbation values. It also seeks to establish the relationship between these markers for COPD exacerbation and to demonstrate whether this relationship can be used to differentiate between these markers.
Methods![]()
A cross-sectional study was conducted on 80 patients with COPD, subdivided into two groups. The first group was 40 patients in stable COPD, and the second group was 40 patients in COPD exacerbation with ages ranging from 15 to 85 years (41.16 ± 14.13) recruited from Al-Imameen Al-Kadhimin medical city, And Medical City Hospital Baghdad, Iraq.
Inclusion criteria
All adults’ patients diagnosed with COPD.
Exclusion criteria
Patients with autoimmune diseases, pregnant women, asthma, confirmed patients with TB, any types of malignancy and history of severe COVID 19 infections.
Blood sampling
5–10 mL of blood was drawn from each patient included in this study. Then left at room temperature (18–25 °C) to clot. Then serum was separated by centrifugation for 5 minutes at 3000 revolutions per minute (rpm), The serum collected will be stored at − 20°C until the time of testing done
Analysis of the parameters
The Sandwich Enzyme-linked immunosorbent assay (ELISA) kit for measurement of Alpha-1 antitrypsin and Elastase activity in serum.
The study was approved by the local ethical committee of the College of Medicine, Al-Nahrain University. In addition, an informed written consent for participation in the study was signed by the participant or the legal guardians of the investigated subjects according to the Helsinki principles.
Measurement of Human serum Alpha-1 antitrypsin by ELISA
According to the ELISA technique the Micro Elisa strip plate coated by an antibody specific to Alpha-1 antitrypsin. Subsequently, an α1-specific antibodies conjugated with Horseradish Peroxidase (HRP) were introduced into every Micro Elisa strip plate thoroughly and incubated. Each well receives an addition of the TMB substrate solution. The wells that contained both HRP conjugated α1-AT and α1-AT antibody appeared blue before the stop solution was added. At 450 nm wavelength, the optical density (OD) was determined spectrophotometrically. The OD value corresponded to the α1-AT concentration [21].
Measurement of Human serum elastase activity by ELISA
Sandwich-ELISA is the technique used with this ELISA kit [21].
Statistical analysis
The program (SPSS version 20) was used to process the data gathered for the investigation. The means and standard deviations of each result were displayed as (M ± SD). T-test comparisons were made, and p ≤0.05 was regarded as statistically significant. Numbers were used to represent categorical variables, and cross-tabulation was used to determine the frequency and percentage of each variable among the groups under study. The correlation was done between AAT and elastase using the Pearson correlation test [22]. Logistic regression was used to calculate odds ratio (ORs) and 95% confidence interval (CI) for stable and exacerbation patients.
Results![]()
Levels of Alpha-1 antitrypsin:
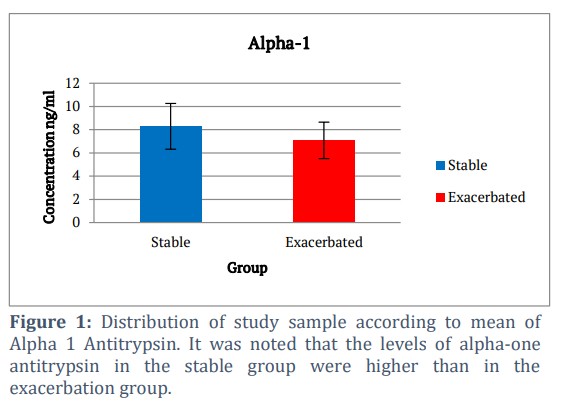
In our study, it was that we included 80 patients (40 stable and 40 exacerbated with mean of AAT level (8.29 ± 1.97 & 7.08 ± 1.57) respectively with a Spiro metrical diagnosis of COPD. During the study a decrease in alpha-1 anti-trypsin concentration was observed in the AECOPD group compared to the stable group as in table 1 and figure 1.
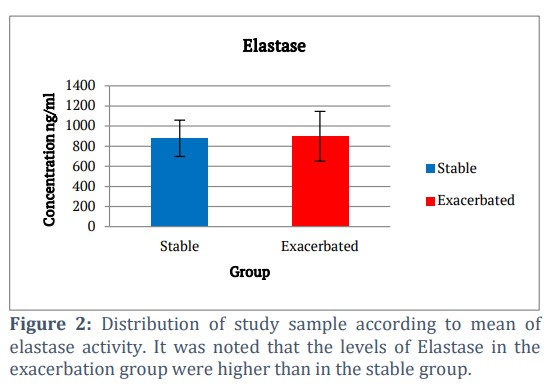
In our study, we observed that the elastase concentration was slightly higher in the exacerbation group compared to the stable group. The mean values were 878.46 ± 180.72 ng/mL and 898.46 ± 247.86 ng/mL for the stable and exacerbation groups, respectively (p = 0.52) as in table 2 and figure 2.
Correlated factors
In this study, we found an inverse relationship between the stable and AECOPD groups. So, we observed an increase in the concentration of elastase when decreased the level of AAT (r = – 0.151) when the p – value (0.003).
Figures & Tables

COPD Patients and Alpha-1 antitrypsin:
The prevalence of AAT deficiency in our study groups was at a high rate so the drop in level of AAT in exacerbation groups is more than the stable group is clearly linked with disease progression. These results took into consideration the similarity of risk factors between the two groups. The findings of our study are consistent with those of several previous studies. For example, Daniel J. Smith and colleagues reported that exacerbated COPD in hospitalized patients with AAT deficiency occurs at a higher rate compared to typical COPD cases. They further suggested that differences in severity and the slower resolution of exacerbations may be related to inflammatory variations. This is supported by the observation that sputum purulence and chronic bronchitis is associated with a higher frequency of exacerbations in AATD [23]. According to another study, people with severe AATD see a greater reduction in FEV1 than people with moderate FEV1. According to earlier research, patients with moderate COPD who are AAT-deficient and have FEV1 between 50 and 80 percent of the expected value have the highest FEV1.
According to the National Heart, Lung and Blood Institute (NHLBI):
That FEV1 value is 50–80% of the expected value Register of Patients with Severe AAT-deficient patients with moderate COPD have been found to have an annual drop of up to 76 mL [24].
COPD Patients and Elastase activity
That explains the role of it in development of disease and in relation to the other variables that were studied in this research, where this increase coincided with the decrease in the value of alpha -1 anti-trypsin and PFT in both groups. This is like data presented before in a COPD exacerbation study in the study of [25], they measured the neutrophil elastase in 90 samples from 30 COPD patients. Where pointed the mean level was 2454 ng/mL (1460 to 4125 ng/mL) also pointed there was a significant increase in neutrophil elastase levels at an exacerbation (P = .003) and previous studies did investigate links to the level of neutrophil elastase with COPD, Where found a previous study that participants with history of COPD had significantly greater protein levels from interleukin (IL)-8, and neutrophil elastase (NE), and the degree of airflow limitation (FEV1/FVC) [26].
COPD Patients and correlated factors
In our statistical study in table 3, we showed a relationship between the Pearson correlation coefficient indicated with (r) and the statistical significance indicated with (p – value) and some parameters. The relationship that was reached through our study between elastase and AAT is a clear inverse relationship that explains the pathological development and is consistent with many other studies, as one of the studies found a mutual relationship between these two variables by studying the genetic change in the production of AAT, where it was concluded that AAT deficiency is due to a genetic factor offset by an increase in elastase concentration and the persistence of inflammatory conditions [27].
Author Contributions
All authors contributed equally in executing the project and drafting this manuscript.
Funding
This research was funded by Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran.
- Singh D, Agusti A, Anzueto A, Barnes PJ, Bourbeau J, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease. The GOLD science committee report, (2019); 53(5):1900164.
- Wain LV, Shrine N, Artigas MS, Erzurumluoglu AM, Noyvert B, et al. Genome-wide association analyses for lung function and chronic obstructive pulmonary disease identify new loci and potential drug gable targets. Nature Genetics, (2017); 49(3): 416-425.
- Michael B, Daniel S, Tino S, Marc M, Heinz B, et al. Treatment of COPD Exacerbation in Switzerland Results and Recommendations of the European COPD Audit, European Respiratory Society, (2017); 94(4): 355-365.
- Vestbo J, Hurd S, Agusti A, Jones P, Vogel M, et al. Global strategy for the diagnosis management and prevention of chronic obstructive pulmonary disease. GOLD executive summary, (2013); 187: 347–365.
- Alana Biggers, COPD Tests and Diagnosis, https://www.healthline.com/health/copd/tests-diagnosis, November 7, 2018.
- Criner G, Jean B, Rebecca L, Daniel R, Donna G. Prevention of acute exacerbations of COPD. American College of Chest Physicians and Canadian Thoracic Society guideline Chest Journal, (2015); 147(4): 894-942.
- Postma D, Bush A, van M. Risk factors and early origins of chronic obstructive pulmonary disease. Lancet Journal, (2015); 385(9971): 899-909.
- Cornillet M, Zemack H, Jansson H, Sparrelid E, Ellis E, et al. Cells Increased Prevalence of Alpha-1-Antitrypsin Deficiency in Patients with Biliary Tract Cancer and Its Associated Clinic pathological Features. PubMed, (2023); 19 (1): 4-9.
- Kalsheker N, Robert S. Alpha-1-antitrypsin Deficiency. Biology, (2017); 1st Edition: 25-35.
- Kalfopoulos M, Wetmore K, ElMallah M. Pathophysiology of alpha-1 antitrypsin lung disease. Methods in Molecular Biology, (2017); 1639: 9–19.
- Kelly E, Catherine M, Tomas P, Noel G, Shane J. Alpha-1 antitrypsin deficiency. Respiratory Medicine Journal, (2010); 104 (6): 763-772.
- Dora E, John J. Alpha1-Antitrypsin (AAT) Deficiency Treatment and Management. Medscape Journal, (2020); 11.
- Demkow U, van FJ. Role of elastases in the pathogenesis of chronic obstructive pulmonary disease. European Journal of Medical Research, (2010); 15(2): 27.
- Karina A, Robert A. Alpha-1 Lung Disease. National Jewish Health. https://www.nationaljewish.org/conditions/alpha-1#:~:text=Alpha%2D1%20is%20one%20of,disease%20from%20this%20genetic%20condition. Accessed on 05 January 2025.
- Patel D, McAllister SL, Teckman JH, Alpha-1 antitrypsin deficiency liver disease. Translational Gastroenterology and Hepatology, (2021); 6(23).
- Belaaouaj A, Kim KS, Shapiro SD. Degradation of outer membrane protein A in Escherichia coli killing by neutrophil elastase. National library of medicine, (2000); 289(5482): 1185-1188.
- Reeves P, Lu H, and Jacobs L, Messina CGM, Bolsover S, et al. Killing activity of neutrophils is mediated through activation of proteases by K+ flux. Nature Journal, (2002); 416(6878): 291-297.
- Brilan S. Role of Elastases in Human Body. Enzyme Engineering Journal, (2022); 11(3): 5-9.
- Voynow JA, Shinbashi M. Neutrophil Elastase and Chronic Lung Disease. Biomolecules, (2021); 11(8): 1065.
- Peter J. Barnes, Jeffrey M. Drazen, Stephen I. Rennard, Neil C. Thomson: Asthma and COPD. (2008); (Second Edition): 737-749.
- Ye G, Oshins RA, Rouhani FN, Brantly ML, Chulay JD. Development validation and use of ELISA for antibodies to human alpha-1 antitrypsin. National Laboratory of Medicine, (2013); 388(1-2): 18-24.
- Norman G. Likert scales levels of measurement and the “laws” of statistics. Advances in Health Sciences Education, (2010); 15(5): 625–632.
- Smith DJ, Ellis PR, Turner AM. Exacerbations of Lung Disease in Alpha-1 Antitrypsin Deficiency. Chronic Obstructive Pulmonary Diseases, (2021); 8(1):162-176.
- Hiller M, Piitulainen E, Jehpsson L, Tanash H. Decline in FEV1 and hospitalized exacerbations in individuals with severe alpha-1 antitrypsin deficiency. International Journal of Chronic Obstructive Pulmonary Disease, (2019); 14: 1075–1083.
- Thulborn J, Mistry V, Brightling CE, Moffitt KL, Ribeiro D, et al. Neutrophil elastase as a biomarker for bacterial infection in COPD. Respiratory Research Journal, (2019); 20(1):170.
- Baines KJ, Simpson JL, Gibson PG. Innate Immune Responses Are Increased in Chronic Obstructive Pulmonary Disease. PLoS One , (2011); 6(3): e18426.
- Al Ashry HS, Strange C. COPD in individuals with the PiMZ alpha-1 antitrypsin genotype. European Respiratory Review, (2017); 26(146): 170068.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0