

Full Length Research Article
Prevalence and Risk of Hepatitis Infection in Infants Associated with Maternal Health History: A Cross-Sectional Study in Indonesia
Faisal Faisal1*, Nurhayati Adnan Prihartono1, Rino Alvani Gani2, Ella Nurlaella Hadi3
Adv. life sci., vol. 12, no. 3, pp. 623-630, August 2025
*– Corresponding Author: Faisal Faisal (Email: faisal.epid13@gmail.com)
Authors' Affiliations
2. Division of Hepatobiliary, Department of Internal Medicine, Faculty of Medicine, University of Indonesia/ Dr. Cipto Mangunkusumo National General Hospital– Indonesia
3. Department of Health Education and Behavioral Sciences, Faculty of Public Health, University of Indonesia – Indonesia
[Date Received: 20/10/2024; Date Revised: 05/01/2025; Available Online: 31/10/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Hepatitis is a significant public health concern in Indonesia, with the government prioritizing the prevention of mother-to-child transmission of hepatitis B. This study aimed to evaluate the influence of antenatal care (ANC), pregnancy and parturition conditions, hepatitis B immunizations, and healthcare accessibility on the incidence of hepatitis among infants.
Methods: A cross-sectional analysis was conducted using data from the 2018 Basic Health Survey (Riskesdas) in Indonesia, examining 10,293 infants aged 6–12 months. Multivariate logistic regression was performed on a final sample of 7,434 cases with complete data. The sampling method used in this research is multistage cluster sampling, which is a common approach for large, nationally representative surveys such as Riskesdas.
Results: Hepatitis was identified in 0.5% of infants. Significant associations were found between hepatitis incidence and maternal pregnancy disorders (aPOR = 1.92, 95% CI = 1.03–3.6) and abnormal parturition methods (aPOR = 2.19, 95% CI = 1.14–4.18). However, ANC history and hepatitis B immunization did not show significant associations.
Conclusion: Comprehensive and timely ANC to address pregnancy disorders and ensure normal parturition can significantly reduce hepatitis risk in infants. Public health interventions should focus on maternal health education and healthcare access, particularly in rural areas.
Keywords: Antenatal Care, Hepatitis Infection, Infant, Parturition, Pregnancy
Introduction![]()
Hepatitis B remains a significant global health concern, with vertical transmission accounting for a substantial burden of chronic infections. According to the World Health Organization (WHO), over 290 million individuals live with chronic hepatitis B worldwide, with a significant proportion attributed to perinatal transmission. Among all reported cases of hepatitis in Indonesia, the distribution is hepatitis B (21.8%), hepatitis A (19.3%), and hepatitis C (2.5%), with the government prioritizing the prevention of mother-to-child transmission of hepatitis B.
The magnitude of the hepatitis epidemic has a significant impact on public health and requires a planned and comprehensive effort. Indonesia, classified as a high-prevalence country for hepatitis B, has rates exceeding 8%. While vaccination programs have shown progress, gaps in antenatal screening and maternal health interventions persist, particularly in rural and underserved areas [1]. The Hepatitis B Early Detection Program for pregnant women has been implemented in community health centers and its network since 2015. Hepatitis B screening for pregnant women is done through a blood test using the HBsAg rapid diagnostic test to minimize transmission to children [2].
Hepatitis B virus (HBV) can be found in blood, seminal fluid, vaginal fluid, and saliva and can be transmitted both horizontally and vertically [3]. Sexual transmission from infected men to women occurs approximately three times more frequently than transmission from women to men, making women three times more likely to be at risk for hepatitis B than men [4].
Hepatitis affects all age groups, but infants are at higher risk for chronic Hepatitis B infection. Transmission of HBV from mother-to-child can occur in utero and during parturition through parenteral (blood-to-blood) contact [5]. Therefore, it is crucial to examine the impact of maternal ANC on healthcare professionals, the completeness of ANC, maternal parturition methods that may result in bleeding that contaminates the infants, and any complications during parturition on the potential incidence of hepatitis in children [3].
Existing studies on maternal and neonatal hepatitis transmission in Indonesia often lack a comprehensive analysis of maternal health factors, such as pregnancy disorders and parturition methods. This study aims to address these gaps by evaluating how maternal health conditions, healthcare accessibility, and immunization status influence hepatitis incidence in infants.
Methods![]()
Study design and participants
The study employed a cross-sectional design, referencing a national non-interventional cross-sectional survey by the Ministry of Health [6]. This design was used to assess the impact of ANC, pregnancy and parturition status, hepatitis B immunizations, and healthcare facilities on the incidence of hepatitis among infants in Indonesia.
This study analyzed data from the 2018 Riskesdas, a nationally representative health survey conducted by the Indonesian Ministry of Health. A multistage cluster sampling method was employed to select 10,293 infants aged 6–12 months. The inclusion criteria were infants with available hepatitis diagnostic data and complete maternal health records. However, the final multivariate logistic regression analysis included complete data from 7,434 infants and their mothers. This sample was limited by missing data for several variables, which excluded some of the initial participants from the analysis.
Materials and Data Sources
This study analyzed data from the 2018 Riskesdas, conducted by the Health Research and Development Agency (Balitbangkes) of the Ministry of Health of the Republic of Indonesia. The survey questionnaire underwent pilot testing and expert review to ensure validity. Data were collected through structured face-to-face interviews by trained enumerators.
The data collection process involved trained enumerators conducting face-to-face interviews with respondents using a structured questionnaire, supported by manual and visual aids.
The study population included all households across 34 provinces and 514 districts and cities in Indonesia. The sample was drawn from 30,000 census blocks, determined by the Central Statistics Agency through field mapping, with 10 households per block systematically and randomly selected as the research sample. All members of the selected households, including infants, were interviewed as part of the Riskesdas survey [6].
Statistical analysis
Data analysis was performed using statistical tests at three levels: univariate, bivariate, and multivariate. Univariate analysis evaluated the frequency of risk factors and the incidence of hepatitis in infants. Bivariate analysis employed binary logistic regression to assess the independent variable on hepatitis incidence in infants, reporting a crude prevalence odds ratio (cPOR) with a significance level of p < 0.05. Multivariate analysis utilized multiple logistic regression to determine the optimal model for calculating adjusted prevalence odds ratio (aPOR), examining the relationship between significant variables and hepatitis incidence.
The adjusted aPOR and its 95% confidence interval were used to identify factors associated with the risk of hepatitis B in infants. Quality control measures included double-checking data entry, random field audits, and enumerator training to minimize interviewer bias. Missing data were handled using complete case analysis. All analyses were conducted using IBM SPSS version 24.
Operational Definitions
Hepatitis Incidence
Cases where infants aged 6–12 months were diagnosed with hepatitis by healthcare providers, based on maternal reporting in the Riskesdas survey.
Pregnancy Disorders
Complications occurring during pregnancy that may adversely affect maternal or fetal health. These include but are not limited to preeclampsia, gestational diabetes, placental abnormalities, infections, and other conditions documented in maternal health records. These disorders are classified based on diagnoses provided by healthcare professionals.
Abnormal Parturition Methods
Deliveries involving medical or mechanical interventions that deviate from spontaneous vaginal delivery, including cesarean sections, vacuum extraction, forceps-assisted delivery, and labor induction. These methods are considered abnormal due to increased risks of maternal-infant blood contact, which may heighten the likelihood of disease transmission.
Antenatal Care (ANC)
Health services provided to pregnant women to monitor the health of the mother and fetus. ANC was categorized based on whether the mother attended healthcare facilities for professional antenatal services during her pregnancy.
Hepatitis Immunization Status
Referring to the completeness of hepatitis vaccinations received by the infant, categorized as completed (all recommended doses) or incomplete (missing one or more doses).
Residential Area
Classified as urban or rural based on the location of the household as reported in the Riskesdas dataset.
Healthcare Accessibility
Measured by whether mothers reported difficulty accessing healthcare facilities such as community health centers or hospitals for delivery and antenatal services.
Ethics Statement
The data used in this study are secondary data from Riskesdas 2018, which is publicly available. The Ethics Committee of the Indonesian Ministry of Health’s Center for Health Research and Development (Balitbangkes) (No. LB.02.01/3/KE024/2018) approved the Riskesdas 2018 study.
Results![]()
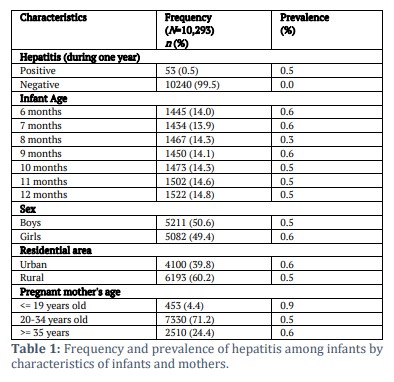
According to Table 1, the Riskesdas survey indicates a hepatitis prevalence of 0.5% among 10,293 infants in Indonesia, with approximately 90% of these cases attributed to hepatitis B [2]. The sex distribution among the infants is nearly balanced between boys and girls, and the age distribution is fairly even, with around 14% in each monthly age group. Over half of the infants come from rural areas. Most of their mothers were aged 20–34 years during pregnancy and were unemployed.
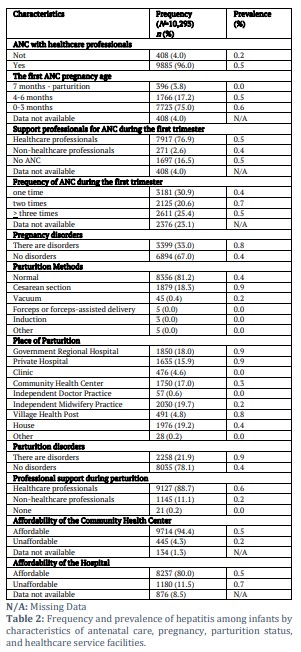
Table 2 indicates that the majority of mothers (96%) received antenatal care (ANC) from healthcare professionals, while 33% experienced complications during pregnancy. Most mothers (75%) attended their initial prenatal visit in the first trimester, but only 20.6% had two checkups during this period. Additionally, 76.9% of mothers received professional support for their pregnancy checkups in the first trimester.
The majority of mothers (81.2%) had normal deliveries, mostly occurring in healthcare facilities. These included government regional hospitals (18%), private hospitals (15.9%), community health centers (17%), and independent midwifery practices (19.7%). About 88.7% of mothers were assisted by healthcare professionals during childbirth, while 21.9% experienced labor complications. In terms of healthcare access, 4.3% of mothers could not reach a community health center, and 11.5% had difficulty accessing a hospital.
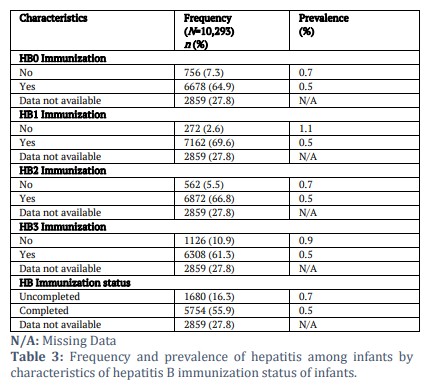
According to Table 3, hepatitis B immunization coverage was incomplete for a number of infants: 7.3% missed the HB0 dose, 2.6% missed the HB1 dose, 5.5% missed the HB2 dose, 10.9% missed the HB3 dose, and 16.3% of infants had incomplete hepatitis B vaccination.
While Antenatal Care (ANC) was not identified as a significant factor in this study, further analysis suggests potential underlying reasons for its apparent lack of effect. These reasons include contextual factors such as variations in healthcare accessibility or adherence to ANC protocols, which warrant further investigation.
Additionally, the issue of missing data, particularly incomplete immunization records, has been addressed to assess its potential impact on the study’s findings. Sensitivity analyses were performed to evaluate how these missing data points might influence the overall results, confirming that the trends reported remain robust. The results highlight distinct variations in hepatitis prevalence across age groups and residential areas. Among younger age groups, lower prevalence rates were observed, which may correlate with targeted vaccination programs.
Conversely, higher prevalence rates in older demographics could be attributed to historical gaps in immunization coverage. Similarly, regional disparities in prevalence suggest differences in healthcare infrastructure and public health initiatives, underscoring the need for tailored intervention strategies.
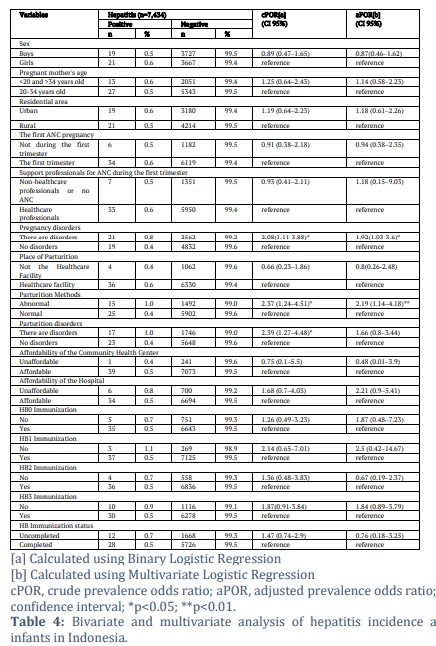
Table 4 presents the results of bivariate and multivariate analyses with a sample size of 7,434. The discrepancy from the initial sample of 10,293 arises because the analysis was limited by missing data for several variables. The bivariate analysis using binary logistic regression revealed two significant variables associated with maternal parturition and the incidence of hepatitis in infants: the methods of parturition (cPOR=2.37, 95%CI=1.24-4.51) and parturition disorders (cPOR=2.39, 95%CI=1.27-4.48).
Additionally, pregnancy disorders were found to be associated with a higher incidence of hepatitis in infants (cPOR=2.08, 95%CI=1.11-3.88). However, socio-demographic factors such as the infant’s sex, maternal age, maternal education level, maternal employment status, and residential area did not show significant associations.
Similarly, ANC history, place of delivery, and accessibility to community health centers and hospitals were not significantly related to the incidence of hepatitis in infants.
Hepatitis B immunizations include HB0 immunization, HB1 immunization, HB2 immunization, HB3 immunization, and completeness hepatitis B immunization area did not show significant associations. Based on the results of the multivariate logistic regression analysis, it was found that pregnancy disorders simultaneously appear as significant predictors of hepatitis incidence in infants (aPOR=1.92; 95%CI=1.03-3.6), and the variable of parturition methods is also significantly related to hepatitis incidence in infants (aPOR=2.19; 95%CI=1.14-4.18).
Figures & Tables
In this study, the prevalence of hepatitis in infants was 0.5%. This number is based on data from respondents who have been diagnosed with hepatitis through a blood test by a doctor during the last year.
Approximately 90% of these cases are attributed to hepatitis B, based on national prevalence data for hepatitis infections in Indonesia. Indonesia has the third-highest rate of hepatitis B + hepatitis C infection worldwide (6.2%), behind China (27.5%) and India (11.6%). This infection rate affects people of all ages [7].
This study detected 33.0% of the mothers as having pregnancy-related problems. The proportion of hepatitis cases in infants born to mothers with pregnancy complications (0.8%) was twice as high as in infants born to mothers without such complications (0.4%). Pregnancy complications were found to have a significant effect on the incidence of hepatitis in infants (p = 0.041). The results indicate that mothers with pregnancy complications are almost twice as likely to have infants with hepatitis (aPOR=1.92; 95%CI=1.03-3.6) compared to those without complications. Hepatitis transmitted from mother-to-child is generally hepatitis B. HBV infection during pregnancy is a major cause of maternal and fetal morbidity and mortality [1], and early-life HBV infection consequently increases the risk of chronic liver disease and cirrhosis [7]. Additionally, it can lead to maternal complications and infant death, with mental and physical health disorders occurring during pregnancy. A study on health services and managerial epidemiology assessed the degree of HBV infection and predictors of HBV infection among pregnant women receiving ANC at selected hospitals in southern Ethiopia [8].
This study found that 81.2% of mothers had normal deliveries, 18.3% underwent cesarean sections, and 0.5% delivered using vacuum, forceps, or induction methods. The proportion of mothers with abnormal deliveries whose infants developed hepatitis (0.9%) was double that of mothers with normal deliveries (0.4%). The mode of delivery significantly impacted hepatitis incidence in infants (p = 0.006, bivariate analysis; confirmed significant in multivariate model, aPOR = 2.19; 95% CI = 1.14–4.18). The findings suggest that mothers who underwent abnormal delivery methods (such as cesarean, vacuum extraction, forceps, or induction) are two times more likely to have infants with hepatitis compared to those who had normal deliveries (aPOR=2.19; 95% CI=1.14-4.18). This aligns with the cautious approach regarding cesarean sections for HBsAg and HBeAg-positive mothers, as some researchers argue that placental barrier effectiveness decreases towards the end of pregnancy [9]. According to the weekly epidemiological report from the WHO, infants born to mothers with high levels of HBV replication are at the highest risk of perinatal transmission [10].
The research from Handayani indicates that pregnant women with HBV can give birth vaginally without the need for surgical interventions such as cesarean sections [11]. This is consistent with previous research by G. Samadi, who reported the most common indications for emergency operative delivery were fetal heart rate abnormalities and obstructed labor [12].
A study by Afraie et al. (2023) describes that abnormal labor has been associated with a higher risk of transmitting hepatitis from mother to child, particularly hepatitis B. Chronic HBV infection in pregnant women increases the likelihood of various adverse outcomes, including gestational diabetes, preeclampsia, and perinatal complications like premature birth and placental issues. These complications can significantly impact the health of both the mother and the infants, potentially increasing the risk of neonatal hepatitis [13].
In this study, 21.9% of mothers experienced delivery complications. Of the mothers in the study, 88.7% were assisted by healthcare professionals, while 11.1% were assisted by non-healthcare professionals. 19.4% of the mothers gave birth outside of healthcare facilities. Compared to infants born to moms without delivery issues (0.4%), the incidence of hepatitis in mothers with delivery complications (0.9%) was twice as high. With a p-value of < 0.05, these difficulties significantly affected the incidence of hepatitis in infants. Bivariate analysis revealed a strong correlation between newborn hepatitis and delivery problems (cPOR=2.39; 95% CI=1.27-4.48). This indicates that compared to moms without problems, women who experienced delivery-related issues were twice as likely to give birth to children who had hepatitis. Multivariate analysis, however, revealed that parturition disorders had no discernible impact. This suggests that, independent of other factors, delivery problems may have a direct impact on the incidence of hepatitis during childbirth. According to Saudi Arabian research, 69.8% of participants recognized labor difficulties, indicating a reasonable level of public awareness of these issues [14]. Therefore, it is necessary to educate the public so that they are aware of labor difficulties and can act promptly to conduct examinations at health services.
This result aligns with research by Faqiang et al., which highlighted China’s success in preventing vertical transmission of HBV through the promotion of facility-based deliveries [15]. One of the effective models for preventing mother-to-child transmission of hepatitis in hospitals is the Maternal and Child Transmission Prevention and Health Management Team model, which focuses on prevention, early diagnosis, and standardized management by hospital staff [16]. Moreover, the implementation of comprehensive prevention strategies in Baoan District has proven effective in maintaining very low rates of mother-to-child transmission of HBV [17]. Therefore, hospitals must ensure the availability and timely administration of hepatitis vaccines [18].
Sefinew et al. revealed an interesting observation regarding birthplace and its link to infection with hepatitis. Their research revealed a significant correlation between hepatitis infection and deliveries carried out by traditional birth attendants (aOR=4.10; 95% CI=0.195-86.129; p=0.024). This reflects the lack of access to hospitals and the prevalence of hazardous traditional health practices in some developing countries [19].
Inadequate access to hospitals and the prevalence of harmful traditional healthcare practices in some developing countries contribute to limited hepatitis screening and unsafe deliveries [20,21]. Healthcare professionals also play a crucial role in mitigating transmission risk. However, studies show gaps in their knowledge—58.2% of nurses and midwives in Sudan lacked training in post-exposure management [22], and many healthcare workers in China held misconceptions about mother-to-child transmission of hepatitis [23]. Enhancing healthcare professionals’ knowledge about HBV infection, especially in terms of epidemiology, transmission pathways, labor risks, and treatment, is essential [24].
The findings of this study reveal that delivery methods, while significant, are not the sole determinants of hepatitis transmission risk. For instance, pregnancy complications, which were underemphasized previously, play a critical role in influencing maternal and neonatal health outcomes. Furthermore, the lack of a significant association between ANC and hepatitis incidence underscores the need for more comprehensive ANC protocols that address broader determinants of maternal health, such as early diagnosis and intervention for high-risk pregnancies. The observed disparities in hepatitis prevalence across age groups and regions also align with findings from studies conducted in comparable settings, reinforcing the importance of targeted public health strategies tailored to specific demographic needs.
Limitations and Strengths
This study acknowledges several limitations that may influence the interpretation of its findings. These include reliance on secondary data, which could introduce biases, and the potential exclusion of key behavioral variables that may affect hepatitis transmission dynamics. Additionally, subjective self-reports within the dataset could impact data accuracy. Nevertheless, this study's strengths lie in its comprehensive dataset, which allows for a broad analysis of demographic and regional variations, and its potential to inform targeted public health policies. By incorporating sensitivity analyses and addressing missing data systematically, the study ensures robustness and transparency in its conclusions. Future research should aim to build upon these findings by incorporating prospective data collection and a wider range of variables.
The prevalence of hepatitis among infants in Indonesia is 0.5% out of 10,293 infants. Based on the results of the multivariate logistic regression analysis, it was found that pregnancy disorders simultaneously appear as significant predictors of hepatitis incidence in infants (aPOR=1.92; 95%CI=1.03-3.6), and the variable of parturition methods is also significantly related to hepatitis incidence in infants (aPOR=2.19; 95%CI=1.14-4.18). However, ANC status, hepatitis B immunization, and healthcare facilities are not significantly associated based on statistical analysis. These findings underscore the importance of timely and comprehensive ANC to identify and treat pregnancy disorders and facilitate normal parturition either in community health centers or hospitals to reduce the risk of hepatitis in infants.
Author Contributions
Conceptualization: Faisal, Nurhayati Adnan Prihartono, Rino Alvin Gani, Ella Nurlaella Hadi; Data curation: Faisal, Nurhayati Adnan Prihartono; Formal analysis: Faisal; Methodology: Nurhayati Adnan Prihartono, Rino Alvin Gani, Ella Nurlaella Hadi; Resources: Faisal, Nurhayati Adnan Prihartono; Software: Faisal; Project administration: Faisal; Supervision: Nurhayati Adnan Prihartono, Rino Alvin Gani, Ella Nurlaella; Visualization: Faisal, Nurhayati Adnan Prihartono; Writing–original draft: Faisal, Nurhayati Adnan Prihartono; Writing–review & editing: all authors.
Conflict of Interest
The authors have no conflict of interest to declare for this study.
The first author would like to sincerely thank the Indonesia Endowment Fund for Education Agency (LPDP) under the Ministry of Finance of the Republic of Indonesia for the grant that supported this research. In addition, the authors would like to thank the head of the Balitbangkes under the Ministry of Health of the Republic of Indonesia for providing the data set and granting permission for the analysis, representation, and publication of the finding.
![]()
References
- Kementerian Kesehatan RI. Hepatitis B pada ibu hamil dan anak. Jakarta, (2023); Available from: https://www.google.com/url?sa=t&source=web&rct=j&opi=89978449&url=https://kemkes.go.id/app_asset/file_content_download/17169676926656d90c733743.81092792.pdf&ved=2ahUKEwjbz4H-tYGMAxUz4zgGHS2MFJoQFnoECBUQAQ&usg=AOvVaw2ZTbU0z1EZulo4iTM91Qs9. Accessed [8 Nov 2024].
- Biro Komunikasi dan Pelayanan Masyarakat (Rokom). 1,5 juta lebih ibu hamil di deteksi dini hepatitis B. Kementerian Kesehatan RI, (2019); Available from: https://sehatnegeriku.kemkes.go.id/baca/umum/20190722/1630952/15-juta-lebih-ibu-hamil-dideteksi-dini-hepatitis-b/. Accessed [18 Nov 2024].
- Villa DdF, Navas MC. Vertical transmission of hepatitis B virus—An update. Microorganisms, (2023); 11(5): 1140.
- Al-Busaf S, Al-Harthi R, Al-Naamani K, Al-Zuhaibi H, Priest P. Risk factors for hepatitis B virus transmission in Oman. Oman Medical Journal, (2021); 36(4): e287.
- Cheung KW, Seto MTY, Lao TTH. Prevention of perinatal hepatitis B virus transmission. Archives of Gynecology and Obstetrics, (2019); 300(2): 251-259.
- Indonesian Ministry of Health. The 2018 Indonesia basic health survey (RISKESDAS): National report. Jakarta, (2019); Available from: https://labmandat.litbang.kemkes.go.id/images/download/laporan/RKD/2018/Laporan_Nasional_RKD%202018_FINAL.pdf. Accessed [9 Nov 2024].
- World Health Organization. Global hepatitis report 2024 action for access in low- and middle-income countries. Geneva, (2024); Available from: https://www.who.int/publications/i/item/9789240091672. Accessed [10 Nov 2024].
- Kampe A, Abbai MK, Tilahun D, Daka D, Aliyo A, Dedecha W, et al. Seroprevalence of hepatitis B virus infection and associated factors among pregnant women attending antenatal care at public hospitals in Borena Zone, Southern Ethiopia. Health Services Research and Managerial Epidemiology, (2023); 10: 1-10.
- Ren Y, Guo Y, Feng L, Li T, Du Y. Controversy and strategies exploration in blocking mother-to-child transmission of hepatitis B. International Reviews of Immunology, (2016); 35(3): 249-259.
- World Health Organization. Hepatitis B vaccines: WHO position paper, July 2017 – Recommendations. Vaccine, (2019); 37(2): 223-225.
- Handayani L, Anisa FN, Palimbo A, Suhartati S, Raudah N, Ibrahim. Analysis of birth outcomes with incidence of hepatitis B in pregnant women. Health Sciences International Journal, (2024); 2(1): 34-44.
- Kochaksaraei GS, Castillo E, Osman M, Simmonds K, Scott AN, Oshiomogho JI, et al. Clinical course of 161 untreated and tenofovir-treated chronic hepatitis B pregnant patients in a low hepatitis B virus endemic region. Journal of Viral Hepatitis, (2016); 23(1): 15-22.
- Afraie M, Moradi G, Zamani K, Azami M, Moradi Y. The effect of hepatitis B virus on the risk of pregnancy outcomes: a systematic review and meta-analysis of cohort studies. Virology Journal, (2023); 20(1): 213.
- Agwa RH, Elwan TH, Alghamdi HAS, Alghamdi AAS, Altaweel FIA, Alghamdi AA, et al. Awareness of Hepatitis B Virus (HBV) screening before marriage and pregnancy among adults in the Al-Baha region, Saudi Arabia. Cureus, (2024); 16(1): 1-14.
- Cui F, Shen L, Li L, Wang H, Wang F, Bi S, et al. Prevention of chronic hepatitis B after 3 decades of escalating vaccination policy, China. Emerging Infectious Diseases, (2017); 23(5): 765-772.
- Zhang C, Huang Y, Ji L, Zhu Q, Wang L, Wang J. Effectiveness of health management team program to enhance prevention of mother-to-child transmission of hepatitis B virus in Ningxia, China. BMC Public Health, (2024); 24(1) :67.
- Luo YL, Gao S, Zhang QF, Liu X, Lv DY, Chen JH, et al. Eliminating mother-to-child transmission of hepatitis B virus: Practice and progress in Baoan, a national pilot district of China. BMC Public Health, (2024); 24(1) :58.
- Adjei CA, Suglo D, Ahenkorah AY, MacDonald SE, Richter S. Barriers to timely administration of hepatitis B birth dose vaccine to neonates of mothers with hepatitis B in Ghana: Midwives’ perspectives. SAGE Open Nursing, (2023); 9: 1-10.
- Molla S, Munshea A, Nibret E. Seroprevalence of hepatitis B surface antigen and anti-HCV antibody and its associated risk factors among pregnant women attending maternity ward of Felege Hiwot Referral Hospital, northwest Ethiopia: A cross-sectional study. Virology Journal, (2015); 12(1): 204.
- Shedain PR, Devkota MD, Banjara MR, Ling H, Dhital S. Prevalence and risk factors of hepatitis B infection among mothers and children with hepatitis B infected mother in upper Dolpa, Nepal. BMC Infectious Diseases, (2017); 17(1): 667.
- Katamba PS, Mukunya D, Kwesiga D, Nankabirwa V. Prenatal hepatitis B screening and associated factors in a high prevalence district of Lira, northern Uganda: A community-based cross-sectional study. BMC Public Health, (2019); 19(1): 1004.
- Mursy SMM, Mohamed SOO. Knowledge, attitude, and practice towards hepatitis B infection among nurses and midwives in two maternity hospitals in Khartoum, Sudan. BMC Public Health, (2019); 19(1): 1597.
- Chen Y, Xie C, Zhang Y, Li Y, Erhardt S, Thio CL, et al. Knowledge regarding hepatitis B mother-to-child transmission among healthcare workers in South China. Journal of Viral Hepatitis, (2018); 25(5): 561-570.
- Djaogol T, Coste M, Marcellin F, Jaquet A, Chabrol F, Giles-Vernick T et al. Prevention and care of hepatitis B in the rural region of Fatick in Senegal: A healthcare workers’ perspective using a mixed methods approach. BMC Health Services Research, (2019); 19(1): 627.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0