

Full Length Research Article
Does Dapagliflozin ameliorate kidney function in Saudi type II diabetic patients with chronic kidney diseases?
Wesam Abdel-Razaq1,5, Mahmoud Mansour*1,5, Tariq M. Aldebasi2,3, Sham Alonazi1, Ghada Al-Sanoni1, Sarah Alwaily1, Abeer Alzubaidi4, Yousef Al-Rajhi1,4, Abdullkarem M. Albekairy1,4,5
Adv. life sci., vol. 12, no. 3, pp. 631-641, August 2025
*– Corresponding Author: Mahmoud Mansour (Email: mansoura@ksau-hs.edu.sa)
Authors' Affiliations
2. College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, 11481 – Saudi Arabia
3. Ophthalmology Department, King Abdulaziz Medical City, Riyadh – Saudi Arabia
4. Pharmaceutical Care Department, King Abdulaziz Medical City, National Guard Health Affairs, Riyadh, 11426 – Saudi Arabia
5. King Abdullah International Medical Research Centre, Ministry of National Guard Health Affairs, Riyadh 11481– Saudi Arabia
[Date Received: 20/10/2024; Date Revised: 05/01/2025; Available Online: 31/10/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: In recent years, type 2 diabetes mellitus (T2DM) has become increasingly prevalent and is associated with numerous cardiovascular and renal complications. Various drug classes are utilized for treating and preventing complications in patients with T2DM. Dapagliflozin, a selective sodium-glucose cotransporter-2 inhibitor, has recently been approved for treating chronic kidney disease (CKD), whether DM is present. This study evaluates dapagliflozin effectiveness in managing T2DM patients with CKD.
Methods: Adult diabetic patients with CKD who received 10 mg dapagliflozin once daily for 12 months were compared with another group on a glucose-lowering regimen without dapagliflozin. Data of HbA1C and kidney function tests, including eGFR, serum creatinine, blood urea nitrogen (BUN), sodium, potassium, calcium, and albumin levels were retrieved before starting dapagliflozin treatment and then every three months for a total of 12 months.
Results: 159 diabetic patients with varying CKD stages received a glucose-lowering regimen. Group I (n=84) included 51 males and 33 females who were administered dapagliflozin, while group II (n =75) comprised 35 males and 40 females who received different glucose-lowering regimens without dapagliflozin. Furthermore, during the 12-month study period, a higher proportion of patients in the dapagliflozin group were identified as having retinopathy, cataracts, and glaucoma (29.8%, 11.9%, and 4.8%, respectively).
Conclusion: The present findings indicate that dapagliflozin did not demonstrate a significant renal protective effect during the first 12 months in this cohort. Further research is warranted to assess the long-term impact of dapagliflozin.
Keywords: Dapagliflozin, Diabetes Mellitus, Chronic Kidney Disease, Renal Failure
Introduction![]()
Chronic kidney disease (CKD) is a complex illness caused by the loss of nephrons, which progressively declines kidney function over time. This may ultimately result in end-stage renal disease (ESRD) and death. Globally, an estimated 700 million people suffer from CKD [1]. Furthermore, CKD is a contributing risk factor associated with a diminished quality of life and a lower life expectancy. Several systemic diseases, such as type 2 diabetes mellitus (T2DM), hypertension, cardiovascular diseases, or primary kidney diseases like glomerulonephritis, can induce CKD. Diabetes mellitus (DM) is one of the leading causes of ESRD in developed countries due to its prevalence and impact on kidney function [2]. Studying these risks in Saudi patients with CKD is crucial due to the increasing prevalence of T2DM and its effects on kidney disease progression [3,4]. Such an investigation into the Saudi population will enable healthcare providers to develop tailored health strategies that improve long-term therapeutic outcomes. However, the complex pathogenesis of DM-related CKD involves structural, physiological, hemodynamic, and inflammatory processes, necessitating a comprehensive, multidisciplinary approach to treatment [5].
Until recently, only angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin-receptor blockers (ARBs) have been proven to slow the decline in kidney function; however, most evidence was generated in patients with T2DM [6-9]. Recent studies suggest a move towards a holistic strategy involving a combination of antihypertensive, antihyperglycemic, and hypolipidemic therapies to slow CKD progression and reduce cardiovascular events. Current management of diabetic kidney disease (DKD) primarily includes ACEIs, ARBs, and sodium-dependent glucose transporter 2 (SGLT-2) inhibitors, which have demonstrated significant renal and cardiovascular benefits [10].
SGLT-2 inhibitors are a class of anti-hyperglycemic medications that target the SGLT-2 transporters in the kidneys, specifically in the proximal convoluted tubules. These drugs inhibit the reabsorption of glucose from the urine, thus reducing blood sugar levels in patients with T2DM. They have demonstrated promising, favorable effects on kidney and cardiovascular outcomes in large clinical trials with T2DM patients [10-12]. There are four SGLT-2 inhibitors approved by the FDA for adult use, including canagliflozin, dapagliflozin, empagliflozin, and ertugliflozin. Although their indications may vary slightly, all four are intended to be used in conjunction with diet and exercise to improve blood sugar control in adults with T2DM [13,14].
Recent evidence suggests that SGLT-2 inhibitors may have beneficial impacts on cardiovascular and renal outcomes in patients with T2DM. Studies have reported that prolonged administration of canagliflozin conferred protection for the cardiovascular and renal systems in T2DM patients with CKD [15]. However, the benefits of SGLT-2 inhibitors seem to be independent of their blood glucose-lowering effects but could be mediated by natriuresis and glucose-induced osmotic diuresis, resulting in a decrease in intra-glomerular pressure. So, the underlying mechanisms remain not fully understood [16-18]. Furthermore, dapagliflozin is utilized to minimize the risk of a decline in estimated glomerular filtration rate (eGFR), ESRD, cardiovascular mortality, and hospitalization due to heart failure in individuals with CKD at risk of progression [13].
Several reports have demonstrated that SGLT-2 inhibitors reduce death rates and cardiovascular adverse events among patients with T2DM [14,15,19]. The CREDENCE trial was the first study to demonstrate a significant reduction in the risk of kidney and cardiovascular events due to the SGLT-2 inhibitors in T2DM patients with high albuminuria and/or impaired kidney function [17]. Moreover, the DAPA-CKD trial revealed a 39% decrease in the risk of deteriorating kidney function due to dapagliflozin in CKD patients, both with and without T2DM, as well as a significant reduction in the progression to ESRD or kidney failure-related death [20].
Therefore, patients with reduced eGFR and higher albuminuria levels are poised to experience the greatest benefits of SGLT-2 inhibitors, which are consistent across patients with and without DM. This challenges the notion that these medications act solely to mitigate diabetes-related kidney damage. Thus, potential mechanisms for renal protection may include hemodynamic changes, blood pressure control, improved salt sensitivities, and improvements in glucose, uric acid, and triglyceride levels. Many outstanding reviews have already been published on dapagliflozin and CKD management, discussing both its effectiveness and safety [21,22].
The current study aimed to assess the potential impacts of long-term use (12 months) of a single daily dose of 10 mg of dapagliflozin on ameliorating kidney function parameters in patients with T2DM and CKD. Furthermore, it is crucial to evaluate the long-term efficacy and safety of the SGLT-2 inhibitor in T2DM patients with CKD to potentially avoid adverse outcomes such as retinopathy, cataracts, and glaucoma in these individuals.
Methods![]()
Study Design
Patients with T2DM who were subsequently diagnosed with CKD were included in this retrospective cohort study, which was carried out at King Abdulaziz Medical City (KAMC), National Guard, Riyadh, Saudi Arabia. Patients were either treated with dapagliflozin in conjunction with other glucose-lowering drugs (Group I, n = 84) or with glucose-lowering drugs only (Group II, n = 75). Dapagliflozin was administered at a dose of 10 mg once daily. For subgroup analysis, all 159 patients were reclassified into four categories to evaluate insulin effects: Group A (n = 21, 13.2%) received dapagliflozin alone; Group B (n = 63, 39.6%) received dapagliflozin with insulin; Group C (n = 30, 18.9%) received neither dapagliflozin nor insulin; and Group D (n = 45, 28.3%) received insulin without dapagliflozin. These subgroup totals correspond accurately to the overall study population (n = 159).
Data Collection
Data from 159 Saudi citizens aged 38–96 years, with T2DM and CKD at different stages, were gathered from the patients’ electronic medical records. Medical record review was conducted in compliance with clinical data confidentiality protection measures of the Institutional Review Board at King Abdullah International Medical Research Center. Each patient was assigned an anonymous number to ensure confidentiality. Hemoglobin A1C (HbA1C), blood electrolytes (sodium, potassium, and calcium), and kidney function test parameters, including serum creatinine, blood urea nitrogen (BUN), serum albumin, eGFR, and albuminuria were retrieved before starting treatment, and at 3, 6, 9, and 12 months of treatment. Demographic data, including age, gender, BMI, and other comorbidities were also collected. The study was conducted following the Declaration of Helsinki and approved by the Institutional Review Board at King Abdullah International Medical Research Center, Riyadh, Saudi Arabia.
Statistical Methods
The mean ± standard deviation (SD), along with the median and interquartile range (IQR), were used to summarize quantitative variables, and frequency and proportions were used to express categorical variables. Quantitative data were compared using unpaired t-tests, while categorical data were compared using chi-squared tests, as appropriate to assess differences between patient groups. A longitudinal analysis was conducted to assess changes in HbA1C levels, kidney function parameters, and other clinical outcomes over the 12-month study period, with measurements taken at baseline and every three months thereafter. The analysis aimed to identify trends and patterns in these variables across different time points for each treatment group. A two-way ANOVA was used to evaluate the effects of time and treatment on the outcomes to identify significant differences between specific time points and groups. Univariate regression analysis was used to describe the association between diabetes-related eye disorders (i.e., retinopathy, glaucoma, and cataracts) and patients’ variables. Odds ratios and confidence intervals (CIs) at the 95% level were calculated to determine the likelihood of outcomes in patients and the strength and direction of these associations. All tests were two-sided and a p-value <0.05 was considered significant. Data were entered in Microsoft Excel 2010 and descriptive and statistical analyses were performed using the GraphPad Prism® software package version 9.0 (San Diego, CA, USA).
Results![]()
Patient Baseline Characteristics
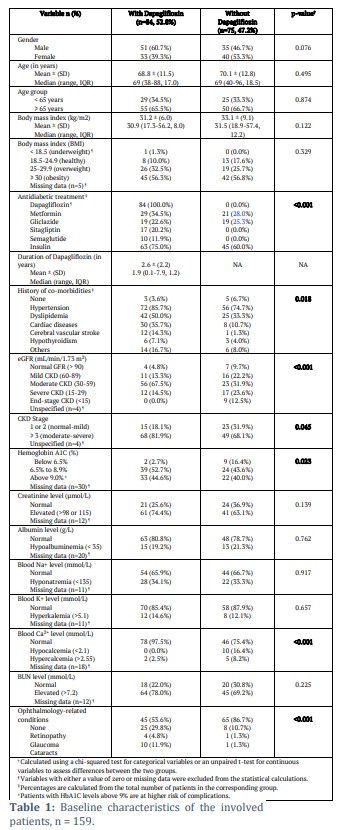
Of the 159 T2DM patients with CKD included in this study, 84 patients were treated with dapagliflozin in combination with other glucose-lowering drugs (group I), and 75 patients were treated with glucose-lowering drugs without dapagliflozin (group II). The baseline characteristics of the patients are shown in Table 1. The gender distribution in the dapagliflozin group (I) was predominantly male (60.7%), whereas the non-dapagliflozin group (II) had a slightly higher percentage of females (53.3%). However, this difference was not statistically significant (p-value of 0.076). Age-wise, both groups had a comparable mean age, around 70 years, and the distribution of patients below and above 65 years of age was also similar. Obesity was the most common BMI category in both groups. The mean BMI was slightly higher in the non-dapagliflozin group, but again, the difference was not statistically significant.
Notably, there was a significant difference in the use of other antidiabetic medications, especially insulin, with 75% of the dapagliflozin group on insulin compared to 60% in the non-dapagliflozin group (p-value < 0.001). Of the 84 patients (dapagliflozin group), 29 (34.5%) were on metformin, 19 (22.6%) were on sulfonylureas, 17 (20.2%) were on DPP-4 inhibitors, and 10 (11.9%) were on semaglutide. While the non-dapagliflozin group (75 patients) was included as a control group, who were treated with other glucose-lowering drugs. Of these, 21 (28.0%) were on metformin, and 19 (25.3%) were on sulfonylureas.
The prevalence of co-morbidities such as dyslipidemia and hypertension was significantly higher in the dapagliflozin group, with hypertension present in 85.7% of patients (p = 0.018). Kidney function, measured by eGFR, showed that a higher percentage of the dapagliflozin group had moderate CKD (67.5%) compared to the non-dapagliflozin group (31.9%), and more patients in the dapagliflozin group had a CKD stage of 3 or higher. These differences were significant (p < 0.001 and p = 0.045, respectively).
HbA1C levels, which indicate blood sugar control, were higher in the dapagliflozin group, with 44.6% of patients having levels above 9.0%, compared to 40.0% in the non-dapagliflozin group. This was also statistically significant, with a p-value of 0.023. Other laboratory parameters, including creatinine, albumin, sodium, potassium, and BUN levels, exhibited no significant differences between the two groups.
Remarkably, the study also found considerable variations in ophthalmology-related conditions, with the dapagliflozin group showing a higher proportion of patients with retinopathy, cataracts, and glaucoma (p-value < 0.001). This may imply that dapagliflozin could have an impact on the occurrence of eye conditions in T2DM patients with CKD.
Hemoglobin A1C and Kidney Function Changes
The HbA1C levels, blood electrolytes, and other kidney function parameters were monitored over a 12-month period to evaluate the efficacy of antidiabetic drugs with and without dapagliflozin regarding glycemic control and improvement of renal function in T2DM patients with CKD. Measurements were taken at baseline (0 months) and at 3, 6, 9, and 12 months.
Hemoglobin A1C
Initially, HbA1C levels were slightly higher in the dapagliflozin group (8.99 ± 1.88%) compared to the non-dapagliflozin group (8.62 ± 2.48%). However, this difference was not statistically significant (p-value of 0.336). Both groups with and without Dapagliflozin showed fluctuations in HbA1C levels, and the reduction in HbA1C levels over time was minimal and gradual, though the dapagliflozin group consistently maintained higher levels (data not shown). In the dapagliflozin group, the HbA1C level was reduced to 8.29 ± 1.52% by the third month, representing a decline of 0.70 %. At the six-month mark, there was a slight increase to 8.58 ± 1.80%, followed by stabilization around 8.61 ± 1.8% at nine months, and a final decrease to 8.40 ± 1.59% at twelve months. In the group without dapagliflozin, the HbA1C level was also slightly decreased by the third month to 7.83 ± 1.69%, marking a reduction of 0.79 % points. However, there was a slight increase to 8.01 ± 1.39% and 8.25 ± 2.10% at six and nine months, respectively, and a final level of 7.87 ± 1.61% at twelve months. A two-way ANOVA analysis revealed significant effects for both the time (p = 0.024) and treatment (p = 0.012).
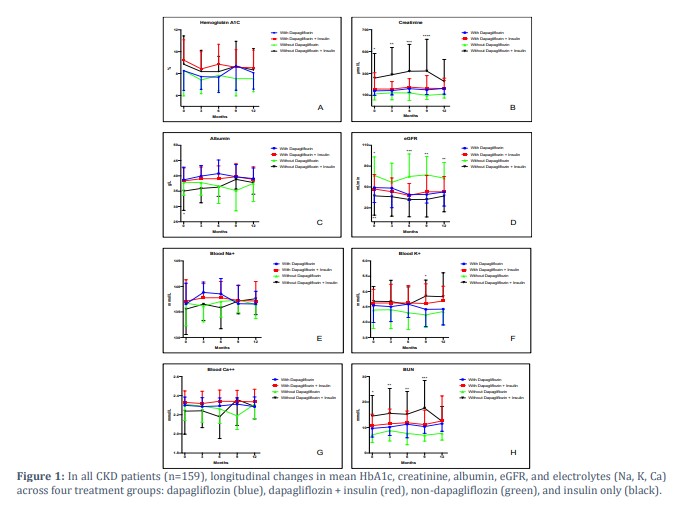
Thus, to realize the effects of various antidiabetic medications, patients were categorized into four groups as follows: Group A (n=21, 13.2%) which included patients who received dapagliflozin, Group B (n=63, 39.6%) who received dapagliflozin along with insulin, Group C (n=30, 18.9%) who did not receive dapagliflozin or insulin, and Group D (n=45, 28.3%) those received insulin without dapagliflozin. Figure 1 displays the longitudinal changes in the mean levels of parameters assessed in the present research, including HbA1c, creatinine, albumin, eGFR, blood electrolytes (Na, K, and Ca), and BUN. These parameters were measured at baseline and every three months for 12 months.
At baseline, all groups had similar mean HbA1C levels (Figure 1A), with the highest in the dapagliflozin and insulin group (9.23 ± 1.86%). By 3 months, all groups showed a decrease in mean HbA1C levels, with the dapagliflozin group showing a reduction from 8.26 ± 1.80% to 7.72 ± 1.61%. However, the group without dapagliflozin achieved the lowest mean (7.41 ± 1.26%). By 6 and 9 months, HbA1C levels fluctuated, with the dapagliflozin group experiencing an increase at 9 months (8.71 ± 2.24%). At 12 months, mean HbA1C levels stabilized, with slight improvements in the group without dapagliflozin. These trends suggest that although dapagliflozin, whether used alone or in combination with insulin, may initially reduce HbA1C levels, the long-term control varies among individuals. However, the two-way ANOVA analysis revealed no statistically significant time effects on HbA1C levels over 12 months among all groups (p=0.085).
Creatinine Blood Test
Regarding creatinine levels (Figure 1B), results show remarkable changes over 12 months across the four groups. The group treated with dapagliflozin showed a steady increase in creatinine levels from 140.3 ± 41.6 µmol/L at baseline to 162.9 ± 52.7 µmol/L at 12 months. All biochemical parameters were standardized to SI units for consistency: BUN (mmol/L), Sodium (Na⁺, mmol/L), Potassium (K⁺, mmol/L), Calcium (Ca²⁺, mmol/L), and Albumin (g/L). Patients on dapagliflozin and insulin exhibited a similar trend, with levels rising from 157.0 ± 149.3 µmol/L to 161.9 ± 94.8 µmol/L. The group without dapagliflozin initially had lower creatinine levels (112.0 ± 54.7 µmol/L) but showed a slight decrease to 110.9 ± 36.5 µmol/L by the end of the study. The group without dapagliflozin but with insulin exhibited the greatest variation in creatinine levels over time, which started with significantly higher creatinine levels (256.9 ± 225.8 µmol/L) at baseline, and significantly increased and peaked at 321.9 ± 290.6 µmol/L at 9 months before decreasing to 227.2 ± 200.7 µmol/L at 12 months. This group showed the highest values and the greatest changes in creatinine levels over the 12 months. This fluctuation indicates a larger range of changes compared to the other groups. A two-way ANOVA indicated a statistically significant difference between treatments (p < 0.001), with the most notable differences observed between groups rather than over time within the same group (p = 0.579).
Albumin Blood Test
In contrast to creatinine, albumin levels (Figure 1C) show a notable increase in all groups, except group C (without dapagliflozin or insulin). At baseline, albumin levels were fairly similar across groups, with the "without dapagliflozin + insulin" group having the lowest mean (35.03 ± 6.29 g/L). By 3 and 6 months, a considerable increase was observed in the group treated with dapagliflozin (mean rising from 38.7 ± 4.1 to 39.9± 3.4 and 40.8 ± 4.4 g/L, respectively). The most significant change occurred in the group without dapagliflozin, which showed a reduction from 37.9 ± 4.9 g/L at baseline to 35.2 ± 6.6 g/L at 9 months, before slightly rising again to 37.6 ± 6.0 g/L at 12 months. However, none of these changes were statistically significant (p=0.581). Throughout the 12 months, the group with dapagliflozin and insulin exhibited relatively stable albumin levels, indicating less variability compared to other groups. A two-way ANOVA analysis indicated a statistically significant difference between treatments (P < 0.001), yet no statistically significant time effect was observed over 12 months among all groups (p=0.581).
Estimated Glomerular Filtration Rate (eGFR)
The effects of dapagliflozin, both with and without insulin, on eGFR (Figure 1D) over a 12-month period exhibited different patterns across treatment groups. The mean eGFR values in the dapagliflozin group and the dapagliflozin plus insulin group showed a slight decline from 49.1 ± 21.4 mL/min at baseline to 42.9 ± 20.2 mL/min and from 47.1 ± 20.7 mL/min at baseline to 43.1 ± 22.1 mL/min at 12 months, respectively. In contrast, the group without dapagliflozin displayed a relatively stable eGFR, with a mean value of 66.7 ± 26.5 mL/min at baseline and 62.7 ± 22.5 mL/min at 12 months. The group without dapagliflozin but with insulin maintained the lowest eGFR, with minimal changes from 37.3 ± 27.7 mL/min at baseline to 37.0 ± 22.7 mL/min at 12 months. Overall, dapagliflozin treatment, with or without insulin, was associated with a modest decline in eGFR, whereas the groups without dapagliflozin exhibited more stable eGFR values over the study period. Like creatinine and albumin, two-way ANOVA analysis indicated a statistically significant difference between treatments (P < 0.001), but not statistically significant across time intervals among all groups (p=0.315).
Electrolyte Blood Test
In Figure 1E, sodium (Na) levels remain relatively stable across all treatment groups over the 12 months, showing minor fluctuations. The overall range of Na across all groups was within normal values, which ranged from a mean minimum of 135.6 ± 4.9 mmol/L (in the group without dapagliflozin + insulin, at baseline) to a mean maximum of 138.8 ± 2.0 mmol/L (in the dapagliflozin group, at 3 months). Potassium (K) levels (Figure 1F) exhibited a slight but not significant increase, particularly in the non-dapagliflozin groups, suggesting a potential worsening of kidney function. Like Na, the overall range of K fell within the physiological normal limit, which was from a mean minimum of 4.2 ± 0.4 mmol/L (in the group without dapagliflozin, at 9 months) to a mean maximum of 4.7 ± 0.5 mmol/L (in the group without dapagliflozin + insulin, at month 12). The calcium (Ca) levels (Figure 1G) also remained stable with only minor variations in all treatment groups. The overall Ca range remained consistent in the group without dapagliflozin + insulin, changing slightly from a mean minimum of 2.2 ± 0.3 mmol/L at 6 months to a mean maximum of 2.4 ± 0.3 mmol/L at 3 months, respectively.
Blood Urea Nitrogen (BUN)
The study results then observed varying trends in BUN levels among different treatment groups (Figure 1H). The mean BUN in the dapagliflozin group increased from 9.7 ± 3.4 mmol/L at baseline to 11.6 ± 3.0 mmol/L at 12 months. The dapagliflozin plus insulin group showed a similar increasing trend, from 10.8 ± 4.5 mmol/L at baseline to 12.6 ± 9.8 mmol/L at 12 months. However, the group without dapagliflozin exhibited a less pronounced change, with mean BUN values moving from 7.1 ± 2.9 mmol/L at baseline to 7.7 ± 2.7 mmol/L at 12 months. Conversely, the group without dapagliflozin but with insulin initially had the highest BUN levels, starting at 14.5 ± 8.1 mmol/L and peaking at 17.6 ± 10.9 mmol/L at 9 months before decreasing to 12.5 ± 5.8 mmol/L at 12 months. Overall, dapagliflozin treatment, with or without insulin, was associated with a rise in BUN levels, whereas the groups without dapagliflozin demonstrated relatively stable or slightly fluctuating BUN levels throughout the study period. Moreover, two-way ANOVA analysis indicated a statistically significant difference between treatments (P < 0.001), but not across time (p=0.700).
Hemoglobin A1C and kidney function changes in advanced CKD patients
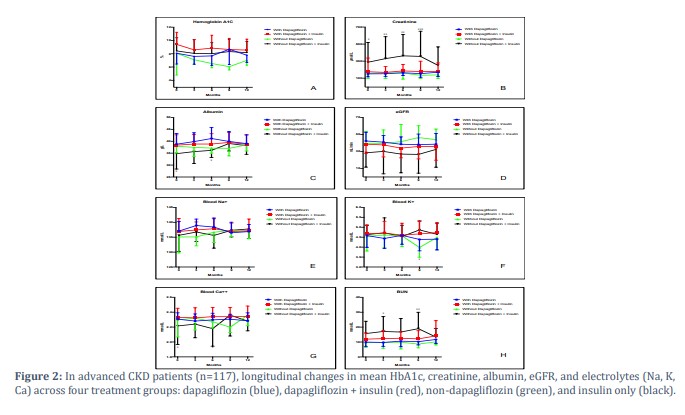
To specifically assess the impact of CKD, all measured parameters (HbA1C, Creatinine, Albumin, eGFR, Blood electrolytes, and BUN) were reevaluated among the same four patient groups with advanced stages of CKD (n=117). Figure 2 presents the longitudinal changes in the mean levels of various clinical data of patients with CKD stage III and higher over a 12-month period.
Hemoglobin A1C
The mean HbA1C levels (Figure 2A) in patients with advanced CKD stages exhibited a similar trend to patients with any CKD stage, but with a slightly higher baseline and a smaller decrease in HbA1C levels in the group treated with dapagliflozin plus insulin. This predicts a more pronounced effect in patients with lower stages of CKD. The most significant reduction was observed in the dapagliflozin and the dapagliflozin plus insulin groups.
Creatinine, Albumin, and eGFR
Just as an increase in the creatinine levels over time was shown for all groups in Figure 1, patients with advanced CKD stages (Figure 2B) exhibited a steeper increase in creatinine levels across all groups, indicating more pronounced kidney dysfunction. Although the albumin levels remain relatively stable in Figure 1C, Figure 2C displays an initial increase in albumin levels in patients with advanced CKD stages (except for those without the dapagliflozin group), followed by a statistically nonsignificant decrease in albumin levels over time, with the smallest decrease observed in the dapagliflozin plus insulin group. In contrast to other groups that maintained low but stable levels of eGFR, the dapagliflozin groups showed a slight, though not statistically significant, decline in eGFR over time in patients with advanced CKD stages (Figure 2D), implying poorer renal outcomes. However, these changes did not reach statistical significance. Groups receiving dapagliflozin experienced a slower rate of decline.
Electrolyte Blood Test
The blood electrolytes (Na, K, and Ca) remained relatively stable with minor variations across all groups in all CKD stages (Figure 1E, 1F & 1G) and advanced CKD stages (Figure 2E, 2F & 2G). However, potassium levels increased slightly over time, with more variability observed in the non-dapagliflozin groups.
Blood Urea Nitrogen (BUN)
When comparing BUN levels in patients with different CKD stages (Figure 1H), it is evident that the increase in BUN levels was more pronounced in patients with advanced CKD stages over 12 months in all groups (Figure 2H). The non-dapagliflozin groups showed a steeper increase in BUN levels. However, when combined with insulin, dapagliflozin appeared to help maintain almost stable BUN levels across different CKD stages, though the overall increase was still greater in advanced CKD stages.
Diabetes eye disorders and participant factors
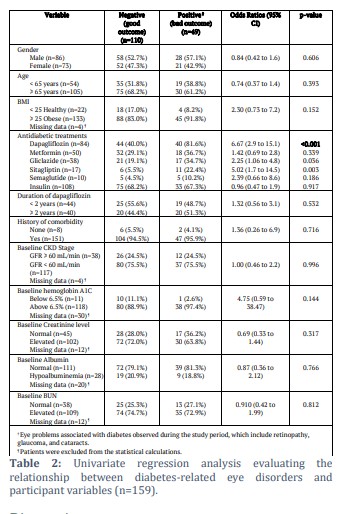
Finally, Table 2 presents a univariate regression analysis exploring the association between various participant variables and diabetes-related eye disorders among the study patients. 49 (30.8%) patients developed diabetes-related eye disorders, such as retinopathy, cataracts, and glaucoma. Gender and age do not show a significant association with the outcomes, as indicated by their p-values of 0.606 and 0.393, respectively. The analysis surprisingly revealed that dapagliflozin was significantly associated with a higher probability of eye disorders, with an odds ratio of 6.67 and a highly significant p-value of <0.001. Other treatments, such as gliclazide (OR 2.25, p = 0.036) and sitagliptin (OR 5.02, p = 0.003), were also significantly associated with bad outcomes.
Figures & Tables
There is currently a scarcity of research assessing the effectiveness of dapagliflozin when combined with insulin or other glucose-lowering treatments for managing blood glycemic levels and improving renal function in patients with T2DM and CKD. The present study assessed the efficacy of a 10 mg daily dose of dapagliflozin used in combination with conventional glucose-lowering drugs over 12 months in T2DM patients with CKD versus patients who received antidiabetic medications without dapagliflozin.
Initially, the effectiveness of dapagliflozin was evaluated by comparing its impact on HbA1C levels between two groups: one group of patients who received dapagliflozin in addition to the conventional antidiabetic medications, and the other group who received the glucose-lowering medications without dapagliflozin. Results showed that both groups experienced a relatively stable trend in HbA1C levels over the 12-month period, with more fluctuations observed in the dapagliflozin group.
It was then decided to categorize patients into four groups to recognize the effects of various antidiabetic medications, particularly patients using insulin. The groups were as follows: Group A received dapagliflozin, Group B received dapagliflozin with insulin, Group C did not receive dapagliflozin or insulin, and Group D received insulin without dapagliflozin. Although dapagliflozin showed the largest initial HbA1C reduction, sustained control was not maintained throughout the 12-month study period. The impact of dapagliflozin on HbA1C was most notable when administered with insulin, resulting in a greater reduction in HbA1C levels compared to patients solely on insulin treatment. Surprisingly, the group without dapagliflozin achieved the lowest mean HbA1C levels, indicating potential long-term benefits of this treatment approach. Overall, patients demonstrated comparable fluctuations in HbA1C levels across all treatment groups throughout the 12-month study period. Despite these fluctuations, the present results indicate a slight overall reduction in A1C levels in the dapagliflozin group, suggesting some level of efficacy in managing A1C over time. However, the long-term control varied among individuals, and no significant time effects were observed among all groups. Unfortunately, the current findings are inconsistent with several previous studies that demonstrated a significant reduction in HbA1C and improved glycemic control with dapagliflozin [21-23].
On the other hand, the present study also assessed the effects of dapagliflozin on kidney function parameters and blood electrolytes. Results revealed a similar trend of fluctuations in most of the data measured in the four patient groups over 12 months. Combination therapy (dapagliflozin with other antidiabetic drugs) resulted in a transient drop in eGFR at 6 months, with partial improvement observed thereafter, although not a full recovery to baseline levels. However, patients treated solely with insulin had consistently lower eGFR (around 37 mL/min) compared to other groups throughout the 12-month observation period. These results align with a recent study that found a similar effect for dapagliflozin, which significantly reduces the risk of a composite sustained decline in eGFR by at least 50% among patients with CKD irrespective of their diabetic status [21]. Patients receiving dapagliflozin also had a reduced incidence of ESKD and death from cardiovascular and renal causes compared to those who received a placebo. Another study also indicated that SGLT-2 inhibitors cause an initial decline in eGFR during the first 2–4 weeks of treatment in patients with CKD [24]. Despite the early sharp decline in eGFR, the renal protective effect of SGLT-2 inhibitors gradually emerged and maintained stability over the following years.
The significant benefit of SGLT-2 inhibitors only became apparent by the second year of treatment. Additionally, Chertow et al., (2021) found that patients with stage 4 CKD had a lesser effect of dapagliflozin on eGFR than patients with stages 2 or 3 CKD [25].
The current findings also revealed a more significant impact on serum creatinine and BUN when insulin was administered without dapagliflozin. However, the combination therapy (dapagliflozin and insulin) was associated with long-term stabilization of both serum creatinine and BUN by the 12 months of the study, which were significantly greater compared to the group treated with insulin alone. This study is the first to explore the effect of dapagliflozin on serum creatinine and BUN during the first year of treatment, comparing those on insulin or other oral hypoglycemic drugs with or without dapagliflozin.
One of the major complications of T2DM is diabetic nephropathy. Therefore, the potential benefits of antidiabetic medications on kidney function have always been of research interest [26,27]. In animal models, dapagliflozin treatment showed improved diabetic nephropathy by improving glucose levels and reducing inflammation and oxidative stress [28,29]. These findings show promise in treating diabetic nephropathy; however, further studies are required to elucidate the exact mechanism of protection.
Previous studies have suggested that SGLT-2 inhibitors may provide advantages for kidney function via several mechanisms. These include lowering glomerular hyperfiltration, decreasing sodium reabsorption in the proximal tubules, reducing inflammatory and fibrotic reactions in the kidney, and decreasing urinary albumin creatinine ratio (UACR), all of which potentially slow down the progression of diabetic nephropathy [30-32]. Moreover, SGLT-2 inhibitors not only lower blood pressure and body weight but also reduce uric acid concentrations, providing additional benefits to the cardiovascular system [33]. The decreased serum uric acid concentration is likely due to the inhibition of sodium-conjugated uric acid reabsorption in the proximal renal tubules [34]. As for serum albumin, dapagliflozin elevates the serum albumin levels in patients treated with insulin or oral glucose-lowering drugs. This could be linked to the usual decrease in albuminuria associated with diabetic patients.
Numerous studies have investigated the effectiveness of dapagliflozin as a valuable medication that can be administered as a monotherapy or in conjunction with other antidiabetic drugs [35]. According to a recent study, the DAPA-CKD trial, dapagliflozin can reduce deleterious kidney and cardiovascular outcomes as well as overall mortality in patients with CKD, regardless of their diabetes status [20,36]. In addition, a different study examined whether the use of cardiovascular medications, such as diuretics, β-blockers, calcium channel blockers, antithrombotic agents, and lipid-lowering agents, influences the renal protective effects of dapagliflozin. The study found that the renal and cardiovascular benefits of dapagliflozin were consistent. This consistency was observed with an unchanged safety profile, regardless of the cardiovascular medications used [37].
Finally, all previous findings indicate that dapagliflozin provides advantages in T2DM patients with cardiovascular risk factors by managing elevated BUN levels and slowing down kidney dysfunction, yet the challenge is considerably escalated in patients with advanced CKD. The results also confirm the safety and effectiveness of dapagliflozin, whether used alone or in combination with cardiovascular drugs, demonstrating benefits on renal and cardiovascular outcomes in patients with mild to advanced CKD, both diabetic and non-diabetic, who are at a greater risk for adverse effects compared to individuals with normal or near-normal kidney function. However, a few studies have warned against the use of dapagliflozin, particularly in patients with moderate or severe kidney impairments and in patients at risk of volume depletion [34]. Moreover, dapagliflozin has been linked to a higher occurrence of genital and lower urinary tract infections. However, these infections are generally mild to moderate in severity and respond well to antimicrobial treatment [35]. In the current study, a higher prevalence of retinopathy, cataracts, and glaucoma was observed in the dapagliflozin-treated group compared to the control groups during the 12-month study period. However, since this was a retrospective analysis, these results should be interpreted as associative findings rather than causal effects. Therefore, clinicians should be cautious and closely monitor patients when prescribing dapagliflozin to avoid potential adverse effects.
In summary, although dapagliflozin may initially reduce HbA1C levels, the reduction was not sufficiently significant at any time point, and the long-term control varies among individuals. Treating T2DM patients with CKD using dapagliflozin for 12 months did not demonstrate a significant renal protective effect. Dapagliflozin alone does not appear to be a promising treatment for preventing or reducing kidney tissue damage, particularly in CKD cases. Continued research is still warranted to further explore the long-term effectiveness of dapagliflozin in controlling HbA1C levels and its role as a renal-protective agent over an extended duration.
Study limitations
It is essential to highlight that this study was retrospective and limited to King Abdulaziz Medical City in Riyadh, Saudi Arabia. Patients who received follow-up care at other hospitals were not included. Therefore, additional research that encompasses multiple regions is necessary to clarify the precise effect of Dapagliflozin on kidney function tests.
Acknowledgments
The authors are thankful for the support of the King Abdullah International Medical Research Center.
![]()
Author Contributions
Tariq M. Aldebasi, Abdullkarem M. Albekairy, and Mahmoud Mansour conceptualized and designed the study. Wesam Abdel-Razaq, Sham Alenazi, Ghada Al-Sanoni, Sarah Alwaily, Abeer Alzubaidi, and Yousef Al-Rajhi contributed to the methodology, data collection, analysis, and interpretation of the results. Wesam Abdel-Razaq and Mahmoud Mansour were responsible for writing, reviewing, and finalizing the manuscript.
All authors have reviewed and approved the final version of the manuscript for submission.
The authors declare no conflicts of interest.![]()
References
- Webster AC, Nagler EV, Morton RL, Masson P. Chronic kidney disease. The lancet, (2017); 389(10075): 1238-1252.
- Nasri H, Rafieian-Kopaei M. Diabetes mellitus and renal failure: Prevention and management. Journal of research in medical sciences, (2015); 20(11): 1112-1120.
- Robert AA, Al Dawish MA, Braham R, Musallam MA, Al Hayek AA, et al. Type 2 diabetes mellitus in Saudi Arabia: major challenges and possible solutions. Current diabetes reviews, (2017); 13(1): 59-64.
- Alshaya OA, Korayem GB, Alghwainm M, Alyami W, Alotaibi A, et al. The prevalence of cardiovascular diseases, chronic kidney disease, and obesity in patients with type 2 diabetes mellitus and the description of concurrent treatments: A two-center retrospective cross-sectional study in Saudi Arabia. Saudi Pharmaceutical Journal, (2024); 32(5): 102054.
- van den Brand JA. Diabetes mellitus as a cause of end-stage renal disease in Europe: signs of improvement. Clinical Kidney Journal, (2016); 9(3): 454-456.
- Ruggenenti P, Perna A, Gherardi G, Garini G, Zoccali C, et al. Renoprotective properties of ACE-inhibition in non-diabetic nephropathies with non-nephrotic proteinuria. The Lancet, (1999); 354(9176): 359-364.
- Brenner BM, Cooper ME, De Zeeuw D, Keane WF, Mitch WE, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. New England journal of medicine, (2001); 345(12): 861-869.
- Hou FF, Zhang X, Zhang GH, Xie D, Chen PY, et al. Efficacy and safety of benazepril for advanced chronic renal insufficiency. New England Journal of Medicine, (2006); 354(2): 131-140.
- Chatzimanouil MKT, Wilkens L, Anders H-J. Quantity and reporting quality of kidney research. Journal of the American Society of Nephrology, (2019); 30(1): 13-22.
- Wang H, Liu D, Zheng B, Yang Y, Qiao Y, et al. Emerging role of ferroptosis in diabetic kidney disease: molecular mechanisms and therapeutic opportunities. International Journal of Biological Sciences, (2023); 19(9): 2678.
- Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. New England Journal of Medicine, (2001); 345(12): 851-860.
- Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. New England Journal of Medicine, (2016); 375(4): 323-334.
- Hsia DS, Grove O, Cefalu WT. An update on sodium-glucose co-transporter-2 inhibitors for the treatment of diabetes mellitus. Current Opinion in Endocrinology, Diabetes and Obesity, (2017); 24(1): 73-79.
- Neal B, Perkovic V, Mahaffey KW, De Zeeuw D, Fulcher G, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. New England Journal of Medicine, (2017); 377(7): 644-657.
- Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. New England Journal of Medicine, (2019); 380(4): 347-357.
- Heerspink HJ, Kosiborod M, Inzucchi SE, Cherney DZ. Renoprotective effects of sodium-glucose cotransporter-2 inhibitors. Kidney international, (2018); 94(1): 26-39.
- Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJ, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. New England journal of medicine, (2019); 380(24): 2295-2306.
- Cherney DZ, Dekkers CC, Barbour SJ, Cattran D, Gafor AHA, et al. Effects of the SGLT2 inhibitor dapagliflozin on proteinuria in non-diabetic patients with chronic kidney disease (DIAMOND): a randomised, double-blind, crossover trial. The lancet Diabetes & endocrinology, (2020); 8(7): 582-593.
- Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. New england journal of medicine, (2015); 373(22): 2117-2128.
- Heerspink HJ, Stefansson BV, Chertow GM, Correa-Rotter R, Greene T, et al. Rationale and protocol of the Dapagliflozin And Prevention of Adverse outcomes in Chronic Kidney Disease (DAPA-CKD) randomized controlled trial. Nephrology Dialysis Transplantation, (2020); 35(2): 274-282.
- Heerspink HJ, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, et al. Dapagliflozin in patients with chronic kidney disease. New England Journal of Medicine, (2020); 383(15): 1436-1446.
- Nashar K, Khalil P. Clinical evaluation of dapagliflozin in the management of CKD: focus on patient selection and clinical perspectives. International Journal of Nephrology and Renovascular Disease, (2022); 289-308.
- Fioretto P, Del Prato S, Buse JB, Goldenberg R, Giorgino F, et al. Efficacy and safety of dapagliflozin in patients with type 2 diabetes and moderate renal impairment (chronic kidney disease stage 3A): The DERIVE Study. Diabetes, Obesity and Metabolism, (2018); 20(11): 2532-2540.
- Duo Y, Gao J, Yuan T, Zhao W. Effect of sodium‐glucose cotransporter 2 inhibitors on the rate of decline in kidney function: A systematic review and meta‐analysis. Journal of Diabetes, (2023); 15(1): 58-70.
- Chertow GM, Vart P, Jongs N, Toto RD, Gorriz JL, et al. Effects of dapagliflozin in stage 4 chronic kidney disease. Journal of the American Society of Nephrology, (2021); 32(9): 2352-2361.
- Filippatos TD, Elisaf MS. Combination drug treatment in obese diabetic patients. World Journal of Diabetes, (2010); 1(1): 8.
- Gosmanov AR, Wall BM, Gosmanova EO. Diagnosis and treatment of diabetic kidney disease. The American journal of the medical sciences, (2014); 347(5): 406-413.
- De Nicola L, Gabbai FB, Liberti ME, Sagliocca A, Conte G, et al. Sodium/glucose cotransporter 2 inhibitors and prevention of diabetic nephropathy: targeting the renal tubule in diabetes. American Journal of Kidney Diseases, (2014); 64(1): 16-24.
- Terami N, Ogawa D, Tachibana H, Hatanaka T, Wada J, et al. Long-term treatment with the sodium glucose cotransporter 2 inhibitor, dapagliflozin, ameliorates glucose homeostasis and diabetic nephropathy in db/db mice. PloS one, (2014); 9(6): e100777.
- Fioretto P, Zambon A, Rossato M, Busetto L, Vettor R. SGLT2 inhibitors and the diabetic kidney. Diabetes care, (2016); 39(Supplement_2): S165-S171.
- Heerspink HJ, Perkins BA, Fitchett DH, Husain M, Cherney DZ. Sodium glucose cotransporter 2 inhibitors in the treatment of diabetes mellitus: cardiovascular and kidney effects, potential mechanisms, and clinical applications. Circulation, (2016); 134(10): 752-772.
- de Albuquerque Rocha N, Neeland IJ, McCullough PA, Toto RD, McGuire DK. Effects of sodium glucose co-transporter 2 inhibitors on the kidney. Diabetes and Vascular Disease Research, (2018); 15(5): 375-386.
- Baker WL, Smyth LR, Riche DM, Bourret EM, Chamberlin KW, et al. Effects of sodium-glucose co-transporter 2 inhibitors on blood pressure: a systematic review and meta-analysis. Journal of the American Society of Hypertension, (2014); 8(4): 262-275.
- Ferrannini E, Ramos SJ, Salsali A, Tang W, List JF. Dapagliflozin monotherapy in type 2 diabetic patients with inadequate glycemic control by diet and exercise: a randomized, double-blind, placebo-controlled, phase 3 trial. Diabetes care, (2010); 33(10): 2217-2224.
- Filippatos TD, Liberopoulos EN, Elisaf MS. Dapagliflozin in patients with type 2 diabetes mellitus. Therapeutic advances in endocrinology and metabolism, (2015); 6(1): 29-41.
- Beernink JM, Persson F, Jongs N, Laverman GD, Chertow GM, et al. Efficacy of dapagliflozin by baseline diabetes medications: a prespecified analysis from the DAPA-CKD study. Diabetes care, (2023); 46(3): 602-607.
- Chertow GM, Correa‐Rotter R, Vart P, Jongs N, McMurray JJ, et al. Effects of Dapagliflozin in Chronic Kidney Disease, With and Without Other Cardiovascular Medications: DAPA‐CKD Trial. Journal of the American Heart Association, (2023); 12(9): e028739.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0