

Full Length Research Article
Assessment of Protein Klotho as Monitor in Diabetic Nephropathy
Sarah Sattar Jabbar1*, Sanad Baqer Mahmmad1,2
Adv. life sci., vol. 12, no. 3, pp. 471-475, August 2025
*- Corresponding Author: Sarah S. Jabbar (Email: sarahsattar@uotelafer.edu.iq)
Authors' Affiliations
2. Department of Chemistry, University of Baghdad, College of Science for Women, Al-Jadriya, Baghdad – Iraq
[Date Received: 28/10/2023; Date Revised: 11/12/2024; Available Online: 31/10/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Klotho is a protein found throughout the body with higher concentrations in the kidneys. Specifically, as a person ages, the levels of Klotho decline gradually, correlating with the natural decrease in kidney function. As we age, a decline in klotho leads to various age-related illnesses like chronic kidney disease, hypertension, cancer, diabetes, and heart disease. Klotho plays a role in regulating metabolism, including glucose and fatty acids, as well as aiding in bile acid production.
Methods: A total of 135 subjects were enrolled in this study, comprising 90 patients with type 2 diabetes mellitus (T2DM) and 45 healthy controls. The diabetic patients were divided into three subgroups based on the level of albuminuria: macroalbuminuria (n = 22), microalbuminuria (n = 23), and normoalbuminuria (n = 45). Serum Klotho levels were measured using the ELISA technique, along with other kidney function tests. The study was conducted at the Hospital of Telafer, Mosul, Iraq, from November 2021 to April 2022.
Result: Compared with controls, diabetic nephropathy (DN) patients had lower serum Klotho levels.
Conclusion: The diagnosis of DN with serum klotho can be promising, and lower serum klotho serves as a good biomarker.
Keywords: Diabetic nephropathy (DN), eGFR, Soluble alpha-Klotho, Albuminuria, Type 2 diabetes mellitus
Introduction![]()
Diabetes mellitus (T2DM), insulin resistance (IR), and irregular insulin secretion characterize its pathophysiology [1]. Most hormones exhibit altered plasma levels in advanced diabetes mellitus due to multiple interrelated metabolic factors [2]. Type-2 diabetes mellitus (DM) is regarded as a long-term impairment in glucose metabolism connected to insulin insufficiency or resistance [3]. Diabetes-related chronic hyperglycemia is linked to organ dysfunction and failure, particularly in the kidney, nerves, heart, and blood vessels [4]. A subgroup of metabolic illnesses recognized as hyperglycemia induced by pancreatic insulin secretion, insulin resistance, or both is classified as a metabolic disorder [5,6]. Diabetic kidney disease or chronic kidney disease (CKD) is a result of diabetic nephropathy (DN), a chronic microvascular consequence of hyperglycemia in diabetes patients. The pathophysiology of diabetic nephropathy (DN) is multifactorial, primarily associated with insulin resistance and chronic hyperglycemia.
Additionally, oxidative stress, inflammation, and altered lipid metabolism have all been linked to it [6,7]. Japanese researchers discovered the anti-aging capabilities of klotho protein in mice that spontaneously developed hypertension in 1997 [8]. The 130 kDa type I transmembrane protein is generated by one of two transcripts from the roughly 50 kb long Klotho genes; meanwhile, the other transcript produces a secreted protein weighing 70 kDa. These transmembrane Klotho proteins are found in the epithelial cells of choroid plexus found in the brain and distal convoluted tubules of the kidneys. The secretases cleave off part of the portion of transmembrane Klotho proteins, releasing them in cerebrospinal fluid, urine, and blood. The Klotho protein that has been cleaved is also referred to as soluble Klotho (sKlotho) or Klotho [9,10]. Previous studies have also explored the role of apoptosis in Klotho-mediated renal protection [11]. Its interest in regulating energy metabolism has recently come to light. Increasing the concentration of Klotho could protect renal endothelial cells [12,13]. This study aims to understand how klotho levels and DN are related, along with the clinical significance of klotho in the diagnosis of DN.
Methods![]()
This case-control study was carried out on patients in the Telafer Hospital from April 2021 to June 2022. The subjects in this study were 135 participants: 90 (53 males and 37 females) and 45 controls. The current study included 90 type 2 DM patients classified into three groups depending on their urine albuminuria levels. These three groups include 45 diabetic patients with normal albuminuria, 22 patients with macroalbuminuria, and 23 patients with microalbuminuria. Out of 135 participants, 45 were healthy persons, named as the control group. A consulting nephrologist performed a clinical examination of all individuals. This kit uses a dual-antibody biotin sandwich-based enzyme-linked immunosorbent assay (ELISA)
Statistical analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 17.0 for Windows (SPSS Inc., Chicago, IL, USA). Continuous/quantitative variables were described with means and standard deviations, while categorical/qualitative variables were described with numbers and percentages.
Results![]()
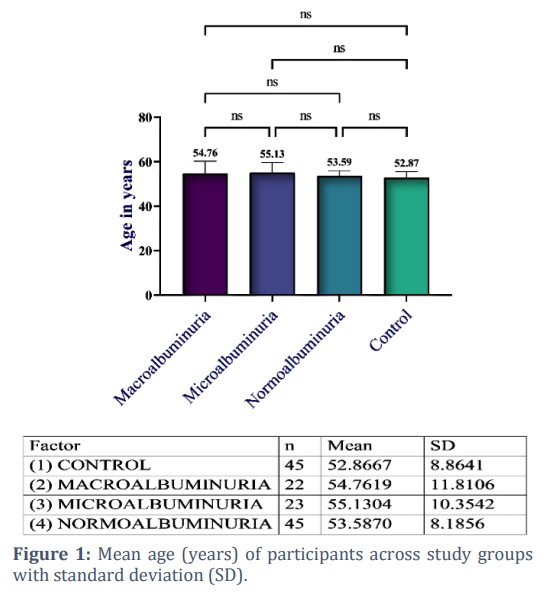
Among the 135 participants, 88 (65.2%) were male and 47 (34.8%) were female, with ages ranging from 32 to 73 years. The male was the most frequent gender within the Control group (n = 35, 25.9%), followed by the normoalbuminuric group (n = 26, 19.3%). There was no significant difference in gender distribution between the groups, χ²(3) = 6.66, p = 0.084. The age means ranged from 54.76 ± 11.53 to 55.13 ± 10.13 for macroalbuminuria and microalbuminuria, respectively. At the same time, the age for normoalbuminuria was 53.59 ± 8.10; for control, it was 52.87 ± 8.77. The variation in age among the groups was not significant, as indicated by the ANOVA statistics, F(3, 131) = 0.38, p = 0.767, which showed that the age discrepancies between the various levels of the group were all similar. Figure 1 depicts the means and 95% CI of means for each group.
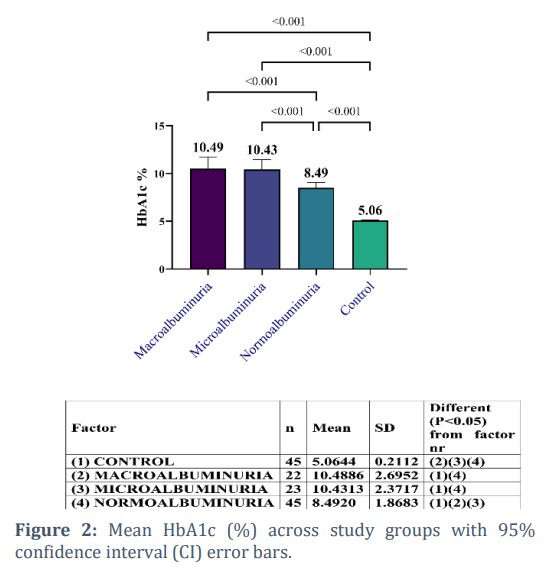
The average HbA1c of the macroalbuminuria group was 10.49 ± 2.70; the average HbA1c level of the microalbuminuria group was 10.43 ± 2.37, while the average HbA1c levels for Normoalbuminuria and Control were (8.49 ± 1.87) and (5.06 ± 0.21), respectively. The ANOVA results were significant: F(3, 131) = 14.95, p < 0.001. This means that at least one group had HbA1c levels that differed significantly from other groups. Multiple pairwise comparisons were made, and the results showed that the mean HbA1c for Macroalbuminuria (M = 10.49 ± 2.70) was significantly higher than for Normoalbuminuria p < 0.001 and Control p < 0.001. On the other
hand, the mean HbA1c for Microalbuminuria (M = 10.43 ± 2.37) was significantly higher than for both Normoalbuminuria (p < 0.001) and Control (p < 0.001). Lastly, the mean HbA1c (%) for Normoalbuminuria (8.49 ± 1.87) was significantly higher than for Controls (5.06 ± 0.21, p < 0.001). The means, standard deviations, and their comparisons are displayed in Figure 2.
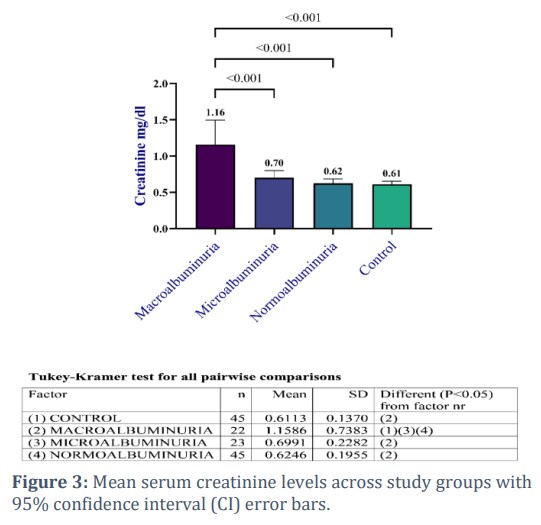
Serum creatinine (mg/dL) averaged 1.16 ± 0.74 in macroalbuminuria, 0.70 ± 0.23 in microalbuminuria, 0.62 ± 0.20 in normoalbuminuria, and 0.61 ± 0.14 in controls. The ANOVA results were significant, F(3, 131) = 14.95, p < 0.001, indicating significant differences in Creatinine among the groups. Multiple pairwise comparisons showed that the mean creatinine value for Macroalbuminuria (1.16 ± 0.74) was significantly greater than Microalbuminuria (M = 0.70 ± 0.23), where p is equal to 0.001, Normoalbuminuria (M = 0.62 ± 0.20), p = 0.001, and Control (M = 0.61 ± 0.14), p = 0.001; the means, standard deviations, and mean values comparisons are shown in Figure 3.
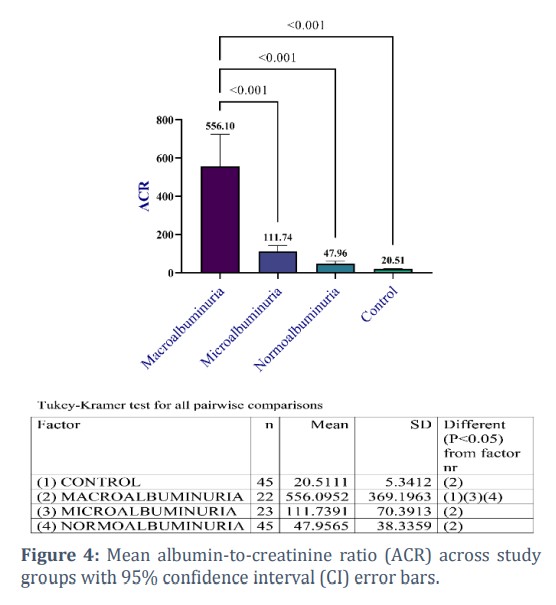
The albumin–creatinine ratio (ACR, mg/g creatinine) averaged 556.10 ± 369.20 in the macroalbuminuria group, 111.74 ± 70.39 in the microalbuminuria group, 47.96 ± 38.34 in the normoalbuminuria group, and 20.51 ± 5.34 in the control group. The ANOVA results showed a significant difference in ACR across the groups, F(3, 131) = 70.25, p < 0.001. The multiple pairwise comparisons showed that the mean of the ACR for macroalbuminuria (M = 556.10 ± 369.20) was significantly larger than for microalbuminuria (M = 111.74 ± 70.39), p < 0.001; it was also significantly larger than for normoalbuminuria (M = 47.96 ± 38.34), p < 0.001; it was also significantly larger than for control. The means, standard deviations, and compared mean values are shown in Figure 4.
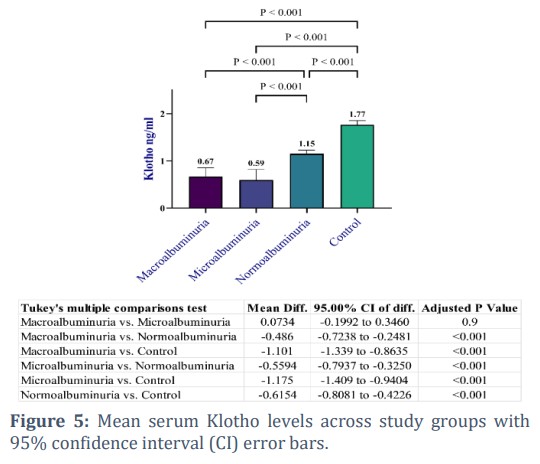
Multiple pairwise comparisons revealed statistically significant smaller Klotho mean values for Macroalbuminuria (M = 0.67, SD = 0.42) than Normoalbuminuria (M = 1.15, SD = 0.25), p < 0.001 and the Control (M = 1.77, SD = 0.29), p < 0.001, the latter two groups showed significantly higher Klotho mean compared to Microalbuminuria (M = 0.59, SD = 0.52). Also, the mean of klotho for Normoalbuminuria (M = 1.15, SD = 0.25) was significantly smaller than for Control (M = 1.77, SD = 0.29), p < 0.001. Figure 5 displays the results of ANOVA and means comparisons.
Figures & Tables
Mean HbA1c levels differed significantly between diabetic patients and controls (F(3, 131) = 67.83, p < 0.001). Within diabetes subgroups, there were significant differences between those with normoalbuminuria and those with microalbuminuria, whereas highly significant variations were present between the macroalbuminuria group and the normoalbuminuria and microalbuminuria groups. Inadequate glycemic management is a major risk factor for diabetic nephropathy development and progression. HbA1c levels in T2D patients are related to an increased risk of developing nephropathy, severe albuminuria, or ESKD [14]. There was no significant difference in the ages of different groups by using the ANOVA test compared with the control groups. This is in agreement with Sueud et al., [15], who showed no significant difference in mean age between both types of diabetes with DN. It was reported that the incidence of ESKD in type 2 diabetes increased with diabetes duration and age [16]. Moreover, intensive glycemic control limits the development of nephropathy to ESRD. The results of this study supported that there are certain mechanisms involved between glucose levels and incident albuminuria [17,18]. The main results showed the levels of Klotho and diabetic nephropathy correlation in diabetic persons; compared to people without DN, patients with DN have reduced quantities of sKlotho. Reduced levels of Klotho (Klotho is a protein linked to aging) are implicated in DM and the onset of kidney and blood vessel ailments associated with DM. Identifying low amounts of the Klotho protein at an early phase could aid in averting illnesses related to type 2 diabetes (DM) and halting their advancement [19].
This study demonstrated a significant inverse relationship between serum Klotho levels and diabetic nephropathy progression. The level of klotho was notably lower in stages of DN, suggesting that sKlotho may serve as an encouraging biomarker for DN detection.
Author Contributions
All authors contributed equally to study conception, data collection, analysis, and manuscript preparation.
No conflicts of interest are disclosed by the authors.![]()
References
- Sadiq C, Hussein R, Maulood I. Ghrelin and Leptin and their Relations with Insulin Resistance in Diabetes Mellitus Type 2 Patients. Baghdad Science Journal, (2022); 19(1): 1-33.
- Fadhel A, Al-Tameemi M, Alfarhani B. Biochemical Investigation in Blood Serum of Female Patients in Type-2 Diabetes. Journal of Global Pharma Technology, (2018); 10(10): 369-373.
- Mustafa S, Hasan B, Ibrahim N. ESTIMATION OF FERRITIN. ERYTHROPOIETIN IN OBESE IRAQI TYPE II DIABETIC PATIENTS. Biochemical and Cellular Archives, (2019); 19(2): 3307-3312.
- Ali K and Shaban S. Relation between Serum Leptin, Lipid Profiles and other biomarkers levels in patients with type 2 diabetic nephropathy. Baghdad Science Journal, (2010); 7(1): 678–686.
- Alwan L, Khaleel F, Hameed A, Al-Ghani R. Determination of Polymorphism Of Glutathione S Transferase (GST) In The Iraqi (Diabetic and Non-Diabetic) Acromegalic Patients, Biochemical & Cellular Archives, (2020); 20(2): 000-000.
- Guo J, Zheng H, Zhang W, Lou W, Xia C, et al. Accelerated kidney aging in diabetes mellitus. Oxidative Medicine and Cellular, (2020); 24(1): 000-000.
- Fineberg D, Jandeleit K, Cooper M. Diabetic nephropathy: diagnosis and treatment. Nature Reviews Endocrinology, (2013); 9(12): 713-723.
- Kuro O. Mutation of the mouse klotho gene leads to a syndrome resembling aging. Nature, (1997); 390(6659): 45-51.
- Xu Y, & Sun Z. Molecular basis of Klotho: from gene to function in aging. Endocrine reviews, (2015); 36(2): 174-193.
- Dalton G, Xie J, An S, Huang C. New insights into the mechanism of action of soluble klotho. Frontiers in endocrinology, (2017); 8(2017): 323.
- Kuro M. The Klotho proteins in health and disease. Nature Reviews Nephrology, (2019); 15(1): 27-44.
- Kim H, Nam B, Kim D, Kang M, Han J, et al. Circulating α-klotho levels in CKD and relationship to progression. American Journal of Kidney Diseases, (2013); 61(6): 899-909.
- Typiak M, Piwkowska A. Antiinflammatory actions of klotho: implications for therapy of diabetic nephropathy. International Journal of Molecular Sciences, (2021); 22(2): 000-956.
- Tziomalos K, Athyros V. Diabetic nephropathy: new risk factors and improvements in diagnosis. The review of diabetic studies: RDS, (2015); 12(12): 000-110.
- Sueud T, Hadi NR, Abdulameer R, Jamil DA, Al-Aubaidy HA. Assessing urinary levels of IL-18, NGAL and albumin creatinine ratio in patients with diabetic nephropathy. Diabetes & Metabolic Syndrome: Clinical Research & Reviews, (2019); 13(1): 0-56.
- Morton JI, Liew D, McDonald SP, Shaw JE, Magliano DJ. The association between age of onset of type 2 diabetes and the long-term risk of end-stage kidney disease: a national registry study. Diabetes Care, (2020); 43(8): 1788-1795.
- Kundu D, Roy A, Mandal T, Bandyopadhyay U, Ghosh E, et al. Relation of microalbuminuria to glycosylated hemoglobin and duration of type 2 diabetes. Nigerian journal of clinical practice, (2013); 16(2): 216-220.
- Bhaisare SD, Rao AK, Jog AS, Kolapkar HU. Clinical Study of Urine Albumin Creatinine Ratio as an Earlier Predictor of Diabetic Nephropathy. Journal of Evolution of Medical and Dental Sciences, (2020); 9(9): 598-603.
- Dokumacıoğlu E, Iskender H. Klotho Protein and Type 2 Diabetes Mellitus. Journal of Apitherapy and Nature, (2022); 5(2): 133-146.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0

