

Full Length Research Article
Biofilm Detection in Multidrug-Resistant Klebsiella pneumoniae via Phenotypic and Genotypic Methods in Diverse Clinical Isolates
Taghreed Tahseen Omaran*, Saba Jasim Jawad Alzubaidy
Adv. life sci., vol. 12, no. 3, pp. 476-482, August 2025
*- Corresponding Author: Teghridt Omran (Email: pbiomsc.teghridtahseen@uodiyala.edu.iq)
Authors' Affiliations
[Date Received: 24/09/2024; Date Revised: 23/02/2025; Available Online: 31/10/2025]
Abstract![]()
Introduction
Methods
Results
Discussion
References
Abstract
Background: Klebsiella pneumoniae is a virulent pathogen that is resistant to several classes of antibiotics and has been responsible for severe hospital- and community-acquired infections. Physiologically found within the human gut, it can induce opportunistic infections, including pneumonia, urinary tract infection, bacteremia, and wound/burn infection. It is possible to isolate it from several clinical sources.
Methods: 190 samples were collected from different health centers of Diyala Governorate between September 2022 and January 2023. These health centers were Baquba Teaching Hospital, Al-Batoul Teaching Hospital, Consulting clinic, Burn and Wound wards, and Educational Laboratories.
Results: Biochemical tests and the VITEK® 2 compact system identified K. pneumoniae in 26.3% (n = 50) of isolates, with 34.0% (n = 17) being multidrug-resistant (MDR). MDR K. pneumoniae showed resistance to CTX (60%), MEM (48%), AMP (100%), AMC (68%), ATM (46%), CAZ (70%), IPM (40%), AK (38%), LEV (30%), CIP (38%), and SXT (60%). All 17 MDR isolates formed biofilms (100%) via the Microtiter Plate Method, with 76.48% (n = 13) being moderate and 23.52% (n = 4) strong producers. Molecular detection revealed 100% positivity for luxS and mrkD genes, and 41.17% (n = 7) for traT.
Conclusion: MDR K. pneumoniae with robust biofilm production, virulence genes, and high-level antimicrobial resistance creates significant infection control issues. Clonal hospital spread is indicated by the genetic similarity, and further epidemiologic studies are necessary to fully understand the strain behavior.
Keywords: MDR, Klebsiella pneumoniae, Virulence Factors Genes, Biofilm
Introduction![]()
Klebsiella pneumoniae is a Gram-negative bacterium that is further categorized under the Enterobacteriaceae family. It is a capsulated, non-motile, facultative anaerobe, lactose-fermenting organism [1,2]. Among all the types of Klebsiella, Klebsiella pneumoniae is of the utmost significance. It is a normal resident of the human intestine and can cause many persistent infections such as urinary tract infections, Bacteremia, Purulent Liver abscess, wound infection, burns, and diarrhea. Therefore, Isolation and study of this bacterium are essential, as infants, older adults, and immunocompromised individuals are highly susceptible. However, the bacterium is also responsible for a growing number of community-acquired infections [1,3]. The mucous surfaces of the digestive system and pharynx are usually colonized in humans by these bacteria, and they can show high degrees of virulence and antibiotic resistance, where it is multi-resistant, meaning that it is resistant to more than one type or more than one group of antibiotics, and it is called Multidrug Resistance (MDR) [4,5]. The Klebsiella pneumoniae bacteria, which are highly virulent organisms, have the ability to form biofilms that enable them to cause chronic infections. This biofilm protects the bacteria from being phagocytosed and from the humoral and cellular immune responses, thus leading to persistent inflammation [6]. Biofilm formation has been documented in K. pneumoniae in 1988 [7]. Klebsiella pneumoniae is capable of biofilm formation: a phenomenon whereby cells adhere to and aggregate with other cells with the help of a matrix of polysaccharides, proteins, and DNA. These biofilms are of clinical importance on catheters and implanted devices and are known to colonize bodily tracts and cause severe infections in immunocompromised patients [8]. These bacteria often colonize hospital patients, complicating treatment and contributing to healthcare-associated infections, and biofilms are multiple or Monomicrobial formations that cause long-term infections that are problematic to treat and remove from the body. Most infections occur in hospitals due to contamination of medical equipment such as catheters and ventilators, which are coated with cellular components hosted on-site [9]. Genes involved in biofilm formation include mrkD, mrkA, fimH, and fimA, which enable adhesion [10]. One of the biofilm genes is the luxS gene, which belongs to QS quorum-sensing genes, and facilitates the production of biofilm. The transfer of genetic material between bacterial cells thus increases the resistance of bacteria to antibiotics [11]. The traT gene is another biofilm-producing gene in MDR Klebsiella pneumoniae that helps in conjugation and complement inhibition [12].
This study aims to analyze the characteristics of K pneumoniae from varied clinical origins, in terms of appearance and genetic makeup, and explore the diversity of biofilm genes, such as luxS, mrkD, and traT, using molecular methods.
Methods![]()
Sample Collection and Identification
190 samples were collected from different health institutions in Diyala Governorate, including Baquba Teaching Hospital, Al-Batoul Teaching Hospital, the consulting clinic, Burn and Wound wards, and Educational Laboratories for the period from September 2022 to January 2023. These samples were distributed between 80 Urine samples for people suffering from urinary tract infections and 45 Sputum samples for people with Respiratory infections, and 28 Wound samples were collected from the Wound wards, in addition to 22 Burn samples. Also, 15 Blood samples were collected from inpatients in Baquba General Hospital. All these samples were cultured on MacConkey Agar medium and Blood Agar medium, and then the samples were incubated at a temperature of 37°C for 24 hours. Bacteria were visually identified on MacConkey agar as lactose fermenters, then transferred to EMB medium for differentiation. HiCrome Agar, a selective medium, was used for easier isolation of K. pneumoniae, which appears light violet on this medium.
Several biochemical tests were performed on the collected samples, and the tests included the oxidase test, catalase test, urease test, indole test, and methyl red test. For final confirmation, Biochemical tests are embedded in the VITEK 2 compact system (BioMérieux / USA).
Antimicrobial Susceptibility Test
Antibiotics used included: Meropenem (MEM), Ampicillin (AMP), Ceftazidime (CAZ), Amoxicillin + Clavulanic acid (AMC), Aztreonam (ATM), Cefotaxime (CTX), Amikacin (AK), Ciprofloxacin (CIP), Levofloxacin (LEV), Imipenem (IPM), Azithromycin (AZM), and Trimethoprim-sulfamethoxazole (SXT). Antimicrobial susceptibility testing was performed using the Kirby–Bauer disk diffusion method on Mueller–Hinton agar, in accordance with the Clinical and Laboratory Standards Institute (CLSI, 2020; M100) guidelines. The inhibition-zone diameters were measured and interpreted according to CLSI breakpoints.
Phenotypic Detection of biofilm
Using the method described by Lamichhane et al., [13], the microtiter plate technique was employed to assess biofilm formation:
- The bacterial isolates were incubated on Nutrient agar at 37°C for a 24-hour period.
- 2-4 colonies were transferred to the Nutrient broth medium supplemented with sucrose, and the turbidity was compared with the turbidity of the McFarland standard solution.
- In a micropipette, 200 μl of bacterial stock for all isolates was transferred to a 96-well polystyrene plate, three replicates of each isolate were made, and nutrient broth was added to several wells and left unvaccinated, and negative control wells were considered. After that, the plate was covered and incubated for 24 hours at 37°C.
- The cover was removed from the plate, and the contents of the wells were gently emptied from the liquid cultures, and the non-adhering cells were removed by washing the wells 2-4 times with distilled water.
- For fixing the cells on the wells, Methanol 200 μl was used for a period of 10 minutes.
- The plate was emptied of alcohol, and the cell membranes were then dyed by adding 200 μl of Crystal violet dye for 15 minutes.
- Distilled water was used two to three times to strip excess dye, and then 200 μl of 95% Ethanol was introduced.
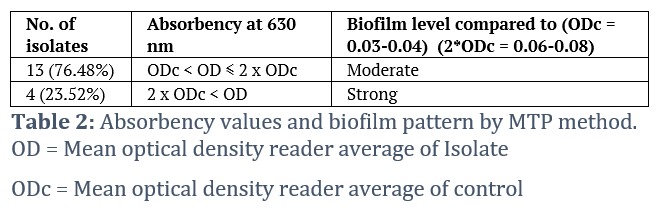
An ELISA reader measured relative absorption at 630 nm. Implant-associated wells were compared to controls, and the results were categorized according to the absorption strength: high, moderate, and non-biofilm forming. Absorbency classification is: OD ≤ ODc, without biofilm; ODc < OD ≤ 2ODc, moderate biofilm; 2ODc < OD, strong or high biofilm forming. "OD" is the mean optical density of the isolate; "ODc" is the mean optical density of the control.
Molecular study of Klebsiella pneumonia
DNA Extraction
DNA was extracted from bacterial cells growing on brain heart infusion broth, where these cells were grown on this medium 24 hours at a temperature of 37 °C, and the extraction process was carried out according to the ABIO pure Extraction protocol. DNA extract's concentration and purity were assessed by measuring absorbance via a QuantusTM Fluorometer.
PCR detection of virulence-associated genes
Biofilm genes were detected via PCR, using gene-specific primers, from 17 of 50 multidrug-resistant isolates. Lyophilized primers, sourced from Macrogen Company, were reconstituted in nuclease-free water to yield a 100 pmol/μl stock. Solved 10 pmol/μl working solutions were also made by taking 10 μl of the -20°C stored cold stock and diluting it with 90 μl nuclease-free water. Table 1 presents the primer sequences for genes employed in the study.
Results![]()
190 clinical samples were collected from 120 patients (63.15%) and non-inpatients (70 patients) (36.84%) from the health institutions of Diyala province, The samples included: Urine (80) samples, Sputum (45) samples, Wound swabs (28) samples, Burns swabs (22) samples and Blood samples (15) samples and the ages of patients ranged between (1-80) years, and these samples were plated on MacConkey agar and the medium of Blood Agar, where the results of the transplantation were that (121) samples by (63.70%) showed a clear bacterial growth on the culture medium and that (69) samples and by (36.31%) did not give any bacterial growth.
The results of bacterial culture on the medium of MacConkey according to the source of the sample, (Urine) out of a total of (80) samples appeared (57) positive for transplantation (71.3%), (Sputum) out of a total of (45) samples appeared (20) positive for transplantation by (44.4%), and (Wounds) out of a total of (28) samples appeared (19) positive for transplantation by (67.9%), (Burns) of a total of (22) samples appeared (15) positive for transplantation and by (68.2%), and (Blood) out of a total of (15) samples appeared (10) positive for transplantation by (66.6%).
The samples were distributed according to gender, 100 samples of females, where they were Urine 48 samples (60%), Sputum 25 samples (55.6%), Wounds 10 samples (35.7%), Burns 10 samples (45.5%), and Blood 7 samples (46.7%). As for males, 90 samples, among which there were Urine 32 samples (40%), Sputum 20 samples (44.4%), Wounds 18 samples (64.3%), Burns 12 samples (54.5%), and Blood 8 samples (53.3%).
Antibiotic Susceptibility Tests
Antimicrobial susceptibility testing was conducted for all 50 K. pneumoniae isolates obtained from various clinical sources. However, the resistance percentages presented below specifically correspond to the 17 multidrug-resistant (MDR) isolates identified among them, to maintain consistency with the data summarized in the Abstract. The sensitivity of K. pneumoniae isolates under study, which numbered 50, was studied, as they showed high resistance towards several antibiotics that are used in health institutions and are widely used to treat different types of infections. The inhibition zone diameters around the antibiotic discs were also measured, and the results were compared to the already established standard tables [14]. The results of the current study showed the sensitivity of K. pneumoniae isolates towards the group of β-lactam antibiotics, where the resistance to Ampicillin (AMP) was 100%, Amoxicillin + Clavulanic acid (AMC) 68%, Aztreonam (ATM) 46%, Imipenem (IPM) 40%, Ceftazidime (CAZ) 70%, Meropenem (MEM) 48%, and Cefotaxime (CTX) 60%. As for the percentage of isolates' resistance to Amikacin (AK), which belongs to the group of Aminoglycoside antibiotics, it was 38%, and the results of the resistance of K. pneumoniae to Quinolone antibiotics were 30% for Levofloxacin (LEV) and 38% for Ciprofloxacin (CIP). As for the Sulfonamide group, Trimethoprim-sulfamethoxazole (SXT) was 60%, and Azithromycin (AZM) was 40% [15]. The results of this study converge with the findings of El-Badawy et al., [16], where the resistance rate to Levofloxacin was 38.59% and to Ciprofloxacin was 44.73%, respectively.
Biofilm detection by Micro-titer plate
The Microtiter Plate Method detected biofilm production in all 17 resistant K. pneumoniae isolates. Bacterial biofilm counts were determined via a microtiter plate assay and ELISA reader, yielding numerical absorbance at 630 nm. All isolates, as per the findings of current research work, were biofilm-producing by 100%. The absorbance (OD) values of the control wells were 0.03-0.04, and the biofilm-producing isolates were distributed into moderate producers, where 13 isolates out of 17 isolates were 76.48%, and 4 isolates were strong biofilm-producing isolates (23.52%). The classification of biofilms was based on the absorption values of the wells in which the isolates were distributed after the rate of the three readings for each isolation was extracted and compared with the absorbance (OD) values of the control wells, as shown in Table 2.
The results of the current study are consistent with some local studies, Al-Rubyaie et al., [17], where the study indicated that all isolates of K. pneumoniae bacteria are 100% biofilm producers, but in contrast with the current study, a study by Al-Timimi et al., [18] found that among 50 isolates of K. pneumoniae bacteria, 46% were weak biofilm producers, 28% were moderate, 6% were strong, and 20% did not produce biofilms. Biofilm is an essential factor in the virulence of K. pneumoniae, which persists in infection due to its resistance to phagocytosis and immunity [6].
Molecular detection of biofilm genes of K. pneumoniae
All 17 isolates of K. pneumoniae (MDR) were subjected to molecular detection of some biofilm genes using the presets assigned to these genes and the polymerase chain reaction (PCR) technique; the genes detected are (luxS, traT, mrkD).
Detection of luxS gene
The results of the current study showed that all isolates were carriers of the luxS gene, the quorum-sensing gene (AI-2QS), as shown in Figure 1.
The results of the current study are consistent with the results of a local study conducted by Mohamed et al., [19]. All 17 isolates under study were 100% carriers of this gene, and these results are in agreement with the outcomes of Shadkam et al., [20]. K. pneumoniae forms biofilms on different surfaces, where cell binding depends on the production of exopolysaccharides and adhesive proteins of type III. There are limited studies describing the relationship between Quorum sensing systems QS and biofilm formation in K. pneumoniae bacteria and this system (QS) type II was found in clinical isolation multi-drug resistance (MDR) on a large scale as well as found that there is a relationship between the luxS gene and gene expression of LPS biosynthesis genes as well as the availability of nutrients and other environmental factors have an impact on the development of biofilms and the construction of polysaccharides and metabolic pathways and all these processes are coordinated within the network of Quorum sensing signals QS bacteria K. pneumoniae as well as gene characterization and other processes regulated by autoinducer-2 (AI-2) [21].
Detection of mrkD gene
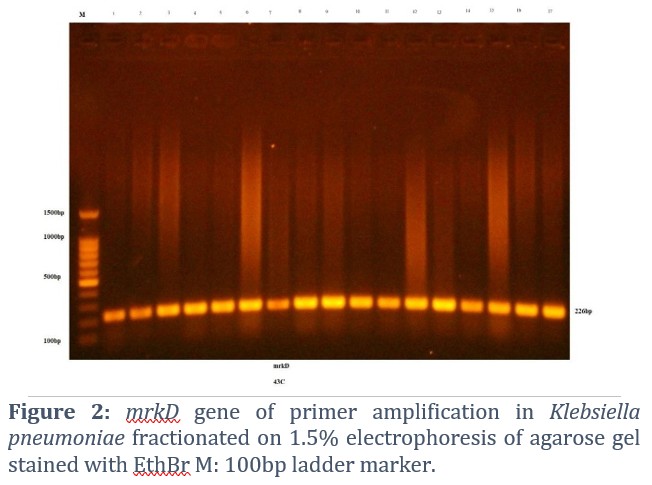
mrkD, a biofilm gene, was detected (Figure 2). Its specific primer revealed the gene's presence in 100% of K. pneumoniae bacterial isolates.
The outcomes of this study are in consensus with those of Al-Saady et al., [22], which showed the mrkD gene was present in 100% of the MDR K. pneumoniae isolates tested. The study of Compain et al., [23] showed that all 65 isolates of K. pneumoniae bacteria are carriers of this gene by 100%. A study by El Fertas-Aissani et al., [24] found mrkD in 96.3% of isolates, while current results align with Rastegar et al., [25], which showed 138/146 K. pneumoniae isolates, or 94.5%, had the mrkD gene.
Detection of traT gene
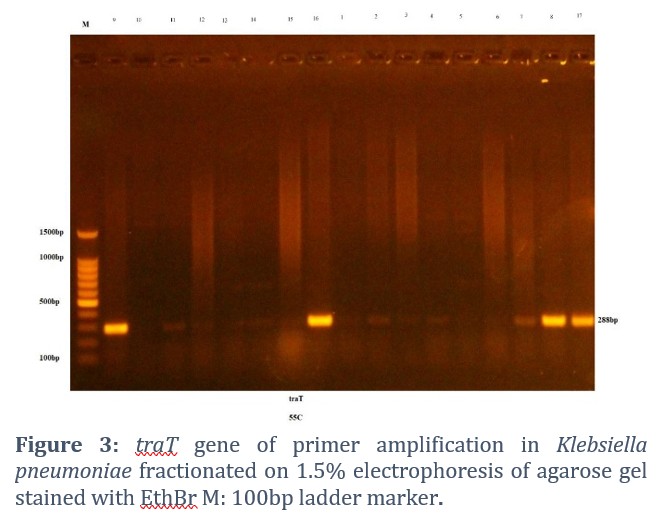
The outer membrane protein coding gene, traT gene, was the last biofilm gene detected in K. pneumoniae MDR isolates and is crucial for conjugation and complement inhibition [12]. The results of the PCR reaction of the gene traT using the primer assigned to it showed that out of 17 isolates of the bacteria K. pneumoniae, 7 isolates were carriers of this gene at a rate of 41.17%.
The current results are consistent with the results of Mirzaie et al., [26]. Where the presence of the traT gene in the isolates of the multi-drug-resistant K. pneumoniae bacteria MDR was 62%, it was found that 62 isolates out of 100 of the bacteria K. pneumoniae were carriers of this gene. The current results are inconsistent with those of El Fertas-Aissani et al., [24], where the results showed that one isolate out of 54 isolates of K. pneumoniae was a carrier of the traT gene at 1.8% (Figure 3).
Figures & Tables


This study demonstrates that MDR Klebsiella pneumoniae from Diyala hospitals combine extensive drug resistance with universal biofilm-forming capacity, amplifying their ability to persist and spread. Integrating genomic surveillance with strategies that disrupt biofilm formation could substantially reduce hospital transmission. Future research should evaluate anti-biofilm therapeutics and monitor genetic linkage between biofilm and resistance determinants.
The ability of bacteria to produce biofilm varies from one isolation to another due to several factors, such as the physical and chemical properties of K. pneumoniae, the physical interaction between components, the type of surface on which biofilms adhere, as well as temperature and pH [29].
The results of genetic detection of biofilm genes showed that all K. pneumoniae isolates under study carried the luxS gene and mrkD gene, while 7 isolates carried the traT gene.
In the current study, the results showed that the K. pneumoniae isolates exhibited resistance patterns commonly associated with β-lactamase-producing strains; however, specific phenotypic or genotypic tests for ESBL, MBL, and AmpC enzymes were not performed in this study, so these mechanisms should be verified in future research.
A high incidence of MDR K. pneumoniae is reported, which is resistant to many antimicrobials. All K. pneumoniae isolates were 100% biofilm producers and possessed virulence genes that made the treatment difficult, and the genes involved in biofilm formation can be transferred from one bacterium to another. The clonal dissemination of K. pneumoniae in all isolates was demonstrated by high genetic similarity in MDR strains. The luxS and mrkD genes were 100% molecularly detected through biofilm-producing genes. The traT gene was observed in 7 isolates, which means that measures should be taken. It is therefore important to conduct more epidemiological analysis of K. pneumoniae strains in Iraq.
Author Contributions
The authors isolated Klebsiella pneumoniae from various clinical sources from hospitalized and non-hospitalized patients and diagnosed them using traditional methods and diagnosis using VITEK2. The phenotypic detection of some virulence aspects was also carried out, the most significant of which is the production of biofilm. Genetic detection of biofilm genes (luxS, mrkD, traT) using their genetic primers.
The authors declare that there are no competing interests in this manuscript.![]()
References
- Bengoechea JA, Sa Pessoa J. Klebsiella pneumoniae infection biology: living to counteract host defenses. FEMS Microbiology Reviews, (2019); 43(2): 123-144.
- Ryan KJ, Ray CG (2014) Enterobacteriaceae. Sherris Medical Microbiology: An Introduction to Infectious Diseases. 4th ed: McGraw-Hill. pp. 343-372.
- Flaih O, Najeb L, Mohammad R. Molecular Detection of Serotypes K1 and K2 of Klebsiella pneumonia Isolated Form Wound and Burn Infections. Al-Anbar Journal of Veterinary Sciences, (2016); 9(1): 311-317.
- Joseph L, Merciecca T, Forestier C, Balestrino D, Miquel S. From Klebsiella pneumoniae colonization to dissemination: an overview of studies implementing murine models. Microorganisms, (2021); 9(6): 1282.
- Wang N, Zhan M, Liu J, Wang Y, Hou Y, et al. Prevalence of carbapenem-resistant Klebsiella pneumoniae infection in a Northern Province in China: clinical characteristics, drug resistance, and geographic distribution. Infection and Drug Resistance, (2022); 15(2022): 569-579.
- Jasim SA, Abdulrazzaq SA, Saleh RO. Virulence Factors of Klebsiella pneumoniae Isolates from Iraqi Patients. Systematic Reviews in Pharmacy, (2020); 11(6): 916.
- Lechevallier MW, Cawthon CD, Lee RG. Factors promoting survival of bacteria in chlorinated water supplies. Applied and environmental microbiology, (1988); 54(3): 649-654.
- Hall-Stoodley L, Costerton JW, Stoodley P. Bacterial biofilms: from the natural environment to infectious diseases. Nature reviews microbiology, (2004); 2(2): 95-108.
- Murphy CN, Clegg S. Klebsiella pneumoniae and type 3 fimbriae: nosocomial infection, regulation and biofilm formation. Future microbiology, (2012); 7(8): 991-1002.
- Wasfi R, Elkhatib WF, Ashour HM. Molecular typing and virulence analysis of multidrug resistant Klebsiella pneumoniae clinical isolates recovered from Egyptian hospitals. Scientific reports, (2016); 6(1): 38929.
- Trubenová B, Roizman D, Moter A, Rolff J, Regoes RR. Population genetics, biofilm recalcitrance, and antibiotic resistance evolution. Trends in microbiology, (2022); 30(9): 841-852.
- Kuş H, Arslan U, Türk Dağı H, Fındık D. Investigation of various virulence factors of Klebsiella pneumoniae strains isolated from nosocomial infections. Mikrobiyoloji Bulteni, (2017); 51(4): 329-339.
- Lamichhane K, Adhikari N, Bastola A, Devkota L, Bhandari P, et al. Biofilm-producing candida species causing oropharyngeal candidiasis in HIV patients attending Sukraraj Tropical and Infectious Diseases Hospital in Kathmandu, Nepal. HIV/AIDS-Research and Palliative Care, (2020); 12(2020): 211-220.
- CLSI. M100 Performance standards for antimicrobial susceptibility testing. 2020; 40(2020); 1-294. CLSI supplement
- Al-Zubaidi SJ (2020) Genetic diversity of the capsular polysaccharide in multidrug resistant Klebsiella pneumoniae and determiner the effect of Zinc Oxide nanoparticles on it. Iraq: University of Diyala.
- El-Badawy MF, Tawakol WM, El-Far SW, Maghrabi IA, Al-Ghamdi SA, et al. Molecular Identification of Aminoglycoside‐Modifying Enzymes and Plasmid‐Mediated Quinolone Resistance Genes among Klebsiella pneumoniae Clinical Isolates Recovered from Egyptian Patients. International journal of microbiology, (2017); 2017(1): 8050432.
- Al-Rubyaie NS (2021) Detection of antiseptic resistant genes in multidrug resistant Pseudomonas aeruginosa and Klebsiella pneumoniae from hospital environment. Iraq: Mustansiriyah University.
- Al-Timimi SNA (2021) Persistence and Filaments Formation in Klebsiella pneumoniae Clinical Isolates. Iraq: Mustansiriyah University.
- Mohamed IQ (2022) Molecular investigation of some biofilms and quorum sensing genes in Klebsiella pneumonia isolated from different clinical cases. Iraq: University of Diyala.
- Shadkam S, Goli HR, Mirzaei B, Gholami M, Ahanjan M. Correlation between antimicrobial resistance and biofilm formation capability among Klebsiella pneumoniae strains isolated from hospitalized patients in Iran. Annals of Clinical Microbiology and Antimicrobials, (2021); 20(2021): 1-7.
- Chen L, Wilksch JJ, Liu H, Zhang X, Torres VV, et al. Investigation of LuxS-mediated quorum sensing in Klebsiella pneumoniae. Journal of medical microbiology, (2020); 69(3): 402-413.
- Al-Saady OMF, NH Zaki. The effect of biosynthesized ag-nanoparticles on Klebsiella pneumoniae biofilm and some virulence genes. Chinese Journal of Medical Genetics, (2022); 32(4): 907-917.
- Compain F, Babosan A, Brisse S, Genel N, Audo J, et al. Multiplex PCR for detection of seven virulence factors and K1/K2 capsular serotypes of Klebsiella pneumoniae. Journal of clinical microbiology, (2014); 52(12): 4377-4380.
- El Fertas-Aissani R, Messai Y, Alouache S, Bakour R. Virulence profiles and antibiotic susceptibility patterns of Klebsiella pneumoniae strains isolated from different clinical specimens. Pathologie Biologie, (2013); 61(5): 209-216.
- Rastegar S, Moradi M, Kalantar-Neyestanaki D, Hosseini-Nave H. Virulence factors, capsular serotypes and antimicrobial resistance of hypervirulent Klebsiella pneumoniae and classical Klebsiella pneumoniae in Southeast Iran. Infection & chemotherapy, (2019); 51(2019): 345-352.
- Mirzaie A, Ranjbar R. Antibiotic resistance, virulence-associated genes analysis and molecular typing of Klebsiella pneumoniae strains recovered from clinical samples. AMB Express, (2021); 11(1): 122.
- Al-Ezzi AS, Shukr M (2019) The presence of genes blaTEM, blaSHV, blaCTX- and anthron in Escherichia coli bacteria isolated from urinary tract infections. Iraq: Diyala University.
- Abdelraheem WM, Abdelkader AE, Mohamed ES, Mohammed MS. Detection of biofilm formation and assessment of biofilm genes expression in different Pseudomonas aeruginosa clinical isolates. Meta Gene, (2020); 23(2020): 100646.
- Cherif-Antar A, Moussa–Boudjemâa B, Didouh N, Medjahdi K, Mayo B, et al. Diversity and biofilm-forming capability of bacteria recovered from stainless steel pipes of a milk-processing dairy plant. Dairy science & technology, (2016); 96(2016): 27-38.
This work is licensed under a Creative Commons Attribution-Non Commercial 4.0 International License. To read the copy of this license please visit: https://creativecommons.org/licenses/by-nc/4.0

